Chang-Long Tai, Mei-Ying Liu, Hsiao-Chi Yu, Chiang-Chuan Chiang, Hung Chiang, Jeng-Hung Suen, Shu-Min Kao, Yu-Hsiu Huang, Tina Jui-Ting Wu, Chia-Feng Yang, Fang-Chih Tsai, Ching-Yuang Lin, Jan-Gowth Chang, Hong-Duo Chen, Dau-Ming Niu
PII: S0009-8981(11)00584-5 DOI: doi:10.1016/j.cca.2011.10.023
Reference: CCA 12492
To appear in: Clinica Chimica Acta
Received date: 18 September 2011 Revised date: 18 October 2011 Accepted date: 18 October 2011
Please cite this article as: Tai Chang-Long, Liu Mei-Ying, Yu Hsiao-Chi, Chiang Chiang-Chuan, Chiang Hung, Suen Jeng-Hung, Kao Shu-Min, Huang Yu-Hsiu, Wu Tina Jui-Ting, Yang Chia-Feng, Tsai Fang-Chih, Lin Ching-Yuang, Chang Jan-Gowth, Chen Hong-Duo, Niu Dau-Ming, THE Use of High Resolution Melting Analysis to Detect Fabry Mutations in Heterozygous Females via Dry Bloodspots, Clinica Chimica Acta (2011), doi:
10.1016/j.cca.2011.10.023
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
ACCEPTED MANUSCRIPT
The Use of High Resolution Melting Analysis to Detect Fabry
Mutations in Heterozygous Females via Dry Bloodspots
Chang-Long Taia,b, Mei-Ying. Liua, Hsiao-Chi Yua, Chiang-Chuan Chiangc, Hung
Chiangd, Jeng-Hung Suend, Shu-Min Kaoc, Yu-Hsiu Huanga, Tina Jui-Ting Wua,
Chia-Feng Yanga, Fang-Chih Tsaia, Ching-Yuang Line, Jan-Gowth Changf, Hong-Duo
Chenb*, Dau-Ming Niua,g,* a
Department of Pediatrics, Taipei Veterans General Hospital, Taipei, Taiwan b
Department of Dermatology, No. 1 Hospital of China Medical University, Shenyang,
China c
Chinese Foundation of Health Neonatal Screening Center, Taipei, Taiwan d
Taipei Institute of Pathology,Institute of Clinical Medicine, Taipei, Taiwan e
College of Medicine,China Medical University, Clinical Immunology Center, China
Medical University Hospital, Taichung, Taiwan f
Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University,
Kaohsiung, Taiwan g
National Yang-Ming University, Taipei, Taiwan
Mei-Ying. Liu have equal contribution to first author.
ACCEPTED MANUSCRIPT
Hong-Duo Chen
Department of Dermatology, No.1 Hospital of China Medical University,
155N.Nanjing St, Shenyang 110001, China.
Phone: +86 24 8328 2642; Fax: +86 24 8328 2633
e-mail: [email protected]
Dau-Ming Niu
Institute of Clinical Medicine, National Yang-Ming University, No.155, Sec. 2,
Linong Street, Taipei 112, Taiwan
Phone: +886 2 7736 8485; Fax: +886 2 2876 7181
ACCEPTED MANUSCRIPT
Abstract
Background: As an X-linked genetic disorder, Fabry disease was first thought to
affect only males, and females were generally considered to be asymptomatic carriers.
However, recent research suggests that female carriers of Fabry disease may still
develop vital organ damage causing severe morbidity and mortality. In the previous
newborn screening, from 299,007 newborns, we identified a total of 20 different
Fabry mutations and 121 newborns with Fabry mutations. However, we found that
most female carriers are not detected by enzyme assays.
Methods: A streamlined method for high resolution melting (HRM) analysis was
designed to screen for GLA gene mutations using a same PCR and melting
programme. Primer sets were designed to cover the 7 exons and the Chinese common
intronic mutation, IVS4+919G>A of GLA gene.
Results: The HRM analysis was successful in identifying heterozygous and
hemizygous patients with the 20 surveyed mutations. We were also successful in
using this method to test dry blood spots of newborns afflicted with Fabry mutations
without having to determine DNA concentration before PCR amplification.
Conclusion: The results of this study show that HRM could a reliable and sensitive
ACCEPTED MANUSCRIPT
Keywords:
ACCEPTED MANUSCRIPT
1. Introduction
Fabry disease (MIM 301500) is an X-linked recessive lysosomal storage disorder
resulting from deficient α-galactosidase A (α-Gal A) activity. It has been estimated
that this disease affects 1 in ~50,000 males in the general population [1-2]. α-Gal A is
an enzyme involved in the metabolic breakdown of globotriaosylceramide (GL-3) and
deficient activity of this enzyme results in GL-3 accumulation in the walls of small
blood vessels, nerves, dorsal root ganglia, renal glomerular and tubular epithelial cells,
and cardiomyocytes. It is a complex multisystemic disorder characterized clinically
by peripheral neuropathic pains (chronic burning and acute episodes of severe pain),
gastrointestinal disturbances, characteristic skin lesions (angiokeratomata),
progressive renal impairment, cardiomyopathy, and early stroke [1].
During the past decade, several variants of Fabry disease have received attention
from doctors and researchers. Three primary variants have been identified,
respectively targeting the cardiac, renal, and neurological systems. Patients with the
cardiac variant lack the classic symptoms of Fabry disease, presenting hypertrophic
cardiomyopathy in the 5th-8th decades of life [3-6]. Previous studies reported that
1-4% of patients with left ventricular hypertrophy (LVH) or hypertrophic
cardiomyopathy (HCM) had undiagnosed Fabry disease [3-5]. Patients with the renal
ACCEPTED MANUSCRIPT
end-stage renal disease after 50 years of age. Screening of plasma α-Gal A activities
showed that the prevalence of Fabry disease in patients undergoing hemodialysis was
0.25-1% [7-9]. Patients with neurologic variant also lack the classic symptoms, but
develop cerebrovascular disease at around forty years of age. The prevalence of Fabry
disease in young patients (18-55 years old) with cryptogenic stroke was reported to be
as high as 4.9% in men and 2.4 % in women [10].
Recently, the authors conducted a study that revealed a surprisingly high
incidence of the cardiac variant GLA mutation IVS4+919G>A (~1 in 1,500-1,600
males) in the Taiwan Han Chinese population [11]. Via family studies of newborns
with the IVS4+919G>A mutation, the authors evaluated the clinical manifestations in
the adults older than 40 years with this mutation. We found that 47 out of 93 subjects
(51%) had left ventricular hypertrophy (LVH), including 28 males (28/39; 72%) and
19 females (19/54; 35%). We also found a positive correlation between disease-onset
rate and age of the patient (Figure 1). In additon, none of the 19 female subjects had α-Gal A enzyme activity less than 3.1 μmol/h/L (25% of the normal mean; 25% is our cutoff value of newborn screening). Very similar finding was observed for our female
patients who have classic type mutations and significant systemic involvement. Only
2 out of these 12 females had α-Gal A enzyme activity less than 3.1 μmol/h/L. We
ACCEPTED MANUSCRIPT
IVS4+919G>A mutation, who did not suffer from left ventricular hypertrophy and
found that around 89% of these females had enzyme activity greater than 25% of the
normal mean (figure 2). These findings showed that current newborn screening
techniques are insufficient in identifying female carriers of Fabry mutations.
Considering that most female carriers even with sufficient residual enzymatic activity
could still suffer from significant systematic disease, we aimed to develop a new
method of newborn screening for Fabry mutations that would be able to detect female
carriers.
High-Resolution Melting Analysis
It has long been noted that high-resolution melting (HRM) analysis provides a
simple, reliable and cost-effective method to identify sequence variants [12-15]. The
procedure is conducted firstly by a PCR amplification in the presence of an
appropriate DNA binding dye, followed by the formation of heteroduplex molecules,
and a final melting and analysis step. Through this study, we aimed to develop a
streamlined method for HRM analysis of the 7 exons (including the flanking intronic
sequences) and the Chinese common intronic mutation, IVS4+919G>A of GLA gene
using the same PCR and melting programme. We also successfully used this method
with dry blood spot extracts of the newborns with Fabry mutations without the
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
2. Materials and Methods
2.1 Subjects
From Jan 2008 to Dec 2010, a total of 299,007 (156,179 males) newborns were
screened for Fabry disease at our cooperative newborn screening centers (Taipei
Institute of Pathology and Chinese Foundation of Health). From this screening, we
identified 121 (106 males) newborns carrying Fabry mutations. Thereafter, we
identified 218 family members (including male and female subjects) carrying Fabry
mutations via the family study. A total of 20 different mutations, were identified in
these patients (figure 3). Aside from the c.274G>T mutation, which was only
identified in one heterozygous (female) patient, all other mutations were identified in
both male and female patients enrolled in the HRM analysis study. Thirteen
unaffected individuals were analyzed as normal controls in this study.
2.2 Methods
Genomic DNA samples were extracted from whole blood or dry blood spots using
MagCore HF16 Automatic DNA/RNA Purification system (RBC Bioscience Corp.,
Taiwan) with MagCore Tissue Genomic DNA Extraction Kit (RBC Bioscience Corp.,
Taiwan). DNA concentrations were determined using a Nanodrop spectrophotometer
(Infinigen, USA). The sequences of primer sets, annealing temperatures and fragments
ACCEPTED MANUSCRIPT
sets were designed using GenBank accession number NM_000169.2 as a reference
sequence. The primer sets were used to amplify the sequences of seven GLA exons and
the region including IVS4+919G>A. The PCR mixture used contained 1x Roche
LighCycler High Resolution Melting Master, 2 pmol of each primer and 6 ng of
genomic DNA for a total volume of 20-l. For the dry blood sample tests, 2 l of out
of 30 l extracts, which were extracted from 3 punched (5 mm in diameter) dried
blood spots, were substituted for the 6 ng of genomic DNA. The polymerase chain
reaction and HRM analyses were performed using a Roche LightCycler® 480 system.
The amplification was performed with an initial denaturation at 95C for 10 min,
followed by 45 cycles of denaturation at 95C for 10 s, annealing at 60C for 15 s and
extension at 72C for 12 s. To facilitate heteroduplex formation, all the PCR products
were heated to 95C for 1 min and cooled down to 40C. Melting curves were
generated by heating the samples from 65 to 95C at a ramp rate of 1C/s. The melting
curves were normalized by selecting linear regions of pre- and post-melting transition,
and defined as 100% and 0%. The melting curves were displayed as melting peaks.
Mutations were identified through a change in melting curve position, shape or
deviated melting curve shape.
All the sequence variations are described according to the guidelines for mutation
ACCEPTED MANUSCRIPT
(http://www.hgvs.org/mutnomen/) using the cDNA sequence NM_000169.2 as the
reference. PCR products of normal genotype are described as “c.[=]+[=]”, while
hemizygous PCR products are described as “c.[variation]” and heterozygous PCR
ACCEPTED MANUSCRIPT
3. Results
Initially we used the original sequence primers (total 8 primer sets, Table 1)
which had been used for sequencing in previous studies [11, 16-21], to cover all seven
exons of the GLA gene and the intronic IVS4+919G>A mutation. However, two
mutations, c.1172A>C and c.1194delA, both located at the 3’ region of exon 7, were
not identified in heterozygous or hemizygous patients (figure 4b). The IVS4+919G>A
mutation was not identified in hemizygous patients.
The amplicons of exon 7 and IVS4+919G>A mutation were the two largest
amplicons (352 and 446 bp) in these 8 original sequence primer sets (241 – 446 bp,
Table 1). Because the ideal amplicon length is less than 250 bp for HRM analysis, we
designed two new primer sets (exon7-1 and 7-2, table 1 and figure 4) to cover exon 7
and a new IVS4 primer set (IVS4-1) to cover the IVS4+919G>A mutation (table 1).
All new designed primer sets created smaller amplicons (220, 233 and 121 bp,
respectively). Thereafter, both the heterozygous and hemizygous patients of these
mutations could be identified by HRM analysis (Figure 4C, 6). The HRM curves of
the identified mutations (excluding IVS4+919G>A) are shown in figure 5.
The MagCore HF16 Automatic DNA/RNA Purification system was then used to
extract DNA samples from dry blood spots. We found that the DNA concentration
ACCEPTED MANUSCRIPT
acceptable concentrations (around 6 ng/ul) for HRM analysis. Therefore, this method
was successful in identifying the mutations from the dry blood spots of the newborns
without determining DNA concentration before the PCR amplification. In order to
examine the discrimination ability, we performed HRM analysis with 30 samples of
different genotypes. The results of 30 dry blood spot samples, including 13 normal, 7
hemizygous and 10 heterozygous individuals with IVS+919G>A mutation, in one
ACCEPTED MANUSCRIPT
4. Discussion
The results of our study have demonstrated that HRM is a reliable and sensitive
method for use in rapid screening of females or even males carrying known GLA
mutations in Taiwan. Recently, HRM analysis for detection of known and unknown
mutations has grown in popularity, as HRM analysis does not require post-PCR
manipulation of samples, unlike DNA sequencing technologies and conventional
gel-based or HPLC-based scanning methods [15]. The cost of the reagents used in this
study was less than $1 (U.S.) per sample per amplicon, making HRM a cost-effective
gene variation analysis technique. In addition to PCR, HRM analysis takes only 15
minutes, amplifying as high as 384 wells at one time for melting analysis. Therefore,
HRM has the potential to be an effective alternative method for Fabry newborn
screening, especially when considering the fact that current screening methods are not
reliable in females.
Although, in our study, all the hemizygous mutations could be easily identified in
our study, the detection rates of hemizygous mutations were only around 75% in
several studies [22-23]. In situation like this, it has been suggested that mixing the
normal male DNA with the hemizygous male DNA could produce artificial
heterozygotes, which would in turn increase the detection rate of hemizygous
ACCEPTED MANUSCRIPT
concentration of DNA to each male PCR tube and the fact that the current
high-throughput enzymatic method for identifying male Fabry patients is highly
reliable, make the HRM method to be the preferable choice only in identifying female
Fabry patients this time.
The interpretation of mutation analysis via HRM is a challenge owing to the
sensitivity of HRM profiles to variable concentrations of nucleic acids or salts [24-25].
It is therefore recommended that DNA samples that have been prepared using a
common extraction procedure be used for HRM. In our study, DNA was extracted
from dried blood spots via a steady automatic DNA extraction system, which ensured
the consistency of the DNA concentration (around 6 ng/ul). In addition, the isolation
reagents used to prepare DNA contain little salt, making the determination of DNA
concentration unnecessary for dry-blood spot analysis. Hence, the unique advantages
of HRM analysis in blood spot analysis may make HRM a possible choice for disease
screening in the near future.
Another important factor to consider in the usage of HRM screening is the
efficiency of any such screening operation. Each year, around 100,000 female
newborns are born in Taiwan. There are 3 newborn screening centers in Taiwan, based
respectively in the National Taiwan University Hospital, Taipei Institute of Pathology,
ACCEPTED MANUSCRIPT
working days and three newborn screening centers, there are around 167 female
babies to be screened for Fabry disease per center each day. Therefore, with the use of
an appropriate automated nucleic acid extraction system and high throughput melting
analyzer, each center could screen all 167 daily female newborns for the IVS4
mutation within 2 hours (including PCR) with one analyzer. Within 8 hours, each
center (with two melting analyzers) could easily screen for all exons of the GLA gene
and the Chinese common intronic IVS4 mutation. Therefore, we propose that, with an
appropriately designed system, HRM analysis could be used as a simple, rapid and
reliable method in female newborn screening for Fabry mutations. This method may
also be viable in the detection of heterozygous Fabry patients within female patient
populations suffering from HCM, renal impairment, or stroke.
A possible concern regarding HRM analysis, however, may still be its sensitivity.
2 mutations were missed in the initial screening using the original primer sets, raising
concerns that the method established so far is not sensitive enough to identify all
Fabry mutations, especially those located at exons 2 and 6 with their amplicons are
greater than 300bp. Therefore, it will be necessary to enlarge the sample size of Fabry
mutations in future studies through cooperation with other Fabry centers.
In conclusion, considering that a large percentage of Fabry female patients could
ACCEPTED MANUSCRIPT
for use as a rapid newborn screening technique for Fabry disease, particularly in
identifying female Fabry patients.
Abbreviations
GL3 globotriaosylceramide
LVH left ventricular hypertrophy
HCM hypertrophic cardiomyopathy
ACCEPTED MANUSCRIPT
References
[1] Desnick RJ, Ioannou YA, Eng CM, alpha-Galactosidase A deficiency: Fabry
disease. In: Scriver CR, Beaudet AL, Sly WS, et al., editors. The metabolic and
molecular bases of inherited disease. New-York: McGraw-Hill, 2001:
3733-3774.
[2] Meikle PJ, Hopwood JJ, Clague AE, Carey WF. Prevalence of lysosomal storage
disorders. JAMA 1999; 281:249-254.
[3] Monserrat L, Gimeno-Blanes JR, Marin F, et al. Prevalence of fabry disease in a
cohort of 508 unrelated patients with hypertrophic cardiomyopathy. J Am Coll
Cardiol 2007; 50:2399-2403.
[4] Nakao S, Takenaka T, Maeda M, et al. An atypical variant of Fabry's disease in
men with left ventricular hypertrophy. N Engl J Med 1995; 333:288-293.
[5] Sachdev B, Takenaka T, Teraguchi H, et al. Prevalence of Anderson-Fabry
disease in male patients with late onset hypertrophic cardiomyopathy. Circulation
2002; 105:1407-1411.
[6] von Scheidt W, Eng CM, Fitzmaurice TF, et al. An atypical variant of Fabry's
disease with manifestations confined to the myocardium. N Engl J Med 1991;
324:395-399.
ACCEPTED MANUSCRIPT
Anderson-Fabry disease among dialysis patients. J Am Soc Nephrol 2004;
15:1323-1329.
[8] Nakao S, Kodama C, Takenaka T, et al. Fabry disease: detection of undiagnosed
hemodialysis patients and identification of a "renal variant" phenotype. Kidney
Int 2003; 64:801-807.
[9] Tanaka M, Ohashi T, Kobayashi M, et al. Identification of Fabry's disease by the
screening of alpha-galactosidase A activity in male and female hemodialysis
patients. Clin Nephrol 2005; 64:281-287.
[10] Rolfs A, Bottcher T, Zschiesche M, et al. Prevalence of Fabry disease in patients
with cryptogenic stroke: a prospective study. Lancet 2005; 366:1794-1796.
[11] Lin HY, Chong KW, Hsu JH, et al. High incidence of the cardiac variant of Fabry
disease revealed by newborn screening in the Taiwan Chinese population. Circ
Cardiovasc Genet 2009; 2:450-456.
[12] Cho MH, Ciulla D, Klanderman BJ, Raby BA, Silverman EK. High-resolution
melting curve analysis of genomic and whole-genome amplified DNA. Clin
Chem 2008; 54:2055-2058.
[13] Erali M, Voelkerding KV, Wittwer CT. High resolution melting applications for
clinical laboratory medicine. Exp Mol Pathol 2008; 85:50-58.
ACCEPTED MANUSCRIPT
simple and efficient molecular diagnostics. Pharmacogenomics 2007; 8:597-608.
[15] Vossen RH, Aten E, Roos A, den Dunnen JT. High-resolution melting analysis
(HRMA): more than just sequence variant screening. Hum Mutat 2009;
30:860-866.
[16] Chen CH, Shyu PW, Wu SJ, Sheu SS, Desnick RJ, Hsiao KJ. Identification of a
novel point mutation (S65T) in alpha-galactosidase A gene in Chinese patients
with Fabry disease. Mutations in brief no. 169. Online. Hum Mutat 1998;
11:328-330.
[17] Lin HY, Chong KW, Hsu JH, Yu HC, Huang CH, Niu DM. Novel human
pathological mutations. Gene symbol: GLA. Disease: Fabry disease. Hum Genet
2010; 127:124.
[18] Lin HY, Huang CH, Yu HC, et al. Enzyme assay and clinical assessment in
subjects with a Chinese hotspot late-onset Fabry mutation (IVS4 + 919G-->A). J
Inherit Metab Dis 2010; 33:619-624.
[19] Lin HY, Niu DM, Chong KW, Hsu JH, Yu HC, Huang CH. Novel human
pathological mutations. Gene symbol: GLA. Disease: Fabry disease. Hum Genet
2010; 127:122-123.
[20] Niu DM, Lin HY, Chong KW, Hsu JH, Yu HC, Huang CH. Novel human
ACCEPTED MANUSCRIPT
2010; 127:122.
[21] Wu KH, Tzung TY, Ro LS, Hsiao KJ. A novel mutation (c. 1072_1074delGAG)
in the alpha-galactosidase gene of a Taiwanese family with Fabry disease. Acta
Derm Venereol 2004; 84:310-311.
[22] Wittwer CT. High-resolution DNA melting analysis: advancements and
limitations. Hum Mutat 2009; 30:857-859.
[23] Farrar JS, Reed GH, Wittwer CT, High Resolution Melting Curve Analysis for
Molecular Diagnostics. In: Patrinos GP, Ansorge WJ, editors. Molecular
Diagnostics. Burlington, MA, USA: Academic Press, 2009: 229-245.
[24] Gundry CN, Vandersteen JG, Reed GH, Pryor RJ, Chen J, Wittwer CT. Amplicon
melting analysis with labeled primers: a closed-tube method for differentiating
homozygotes and heterozygotes. Clin Chem 2003; 49:396-406.
[25] Seipp MT, Durtschi JD, Liew MA, et al. Unlabeled oligonucleotides as internal
temperature controls for genotyping by amplicon melting. J Mol Diagn 2007;
ACCEPTED MANUSCRIPT
Figure legend
Figure 1. Age-onset of patients with the IVS4+919G>A mutation
The age-onset of male and female patients with the IVS4+919G>A mutation were
showed in panel A and B, respectively. 72% percentage of male adults with
IVS4+919G>A mutation, who were older than 40 years old, had developed
hypertrophic cardiomyopathy. Disease onset rate is positively correlated with the age
of the patient. The disease onset rate of male Fabry patients increased from 50% to
64% and then to 87%, as the age progressed from forties to fifties and then to sixties
(figure 1a). The disease onset rate of female Fabry patients increased from 18% to
100%, as age progressed from forties to seventies. One woman at the age group of 80
did not show any sign of hypertrophic cardiomyopathy (figure 1b).
Figure 2. Residual α-galactosidase A activity of female adults carrying IVS4+919G>A
or classical mutations identified in Taiwan.
A: females with IVS4+919G>A mutation, but without HCM (n = 31); B: females with
IVS4+919G>A mutation and HCM (n = 16); C: females with classical mutations and
major organ involvement (n= 10). Activity is expressed as percentage of the mean of
ACCEPTED MANUSCRIPT
enzymatic activity of the normal control.
Figure 3. Schematic representation of the exon/intron organization of the GLA gene
with indication of positions of mutations identified in Taiwanese Chinese populations.
A total of 20 GLA mutations, identified in Taiwanese patients, including missense
(blue); nonsense (red), deletion (green) and splicing site mutations (black) were
examined in this study.
Figure 4. HRM analysis of exon 7 of the GLA gene.
The primer set 7 was first used in this HRM analysis. With this primer set, however,
two mutations, c.1172A>C and c.1194delA, both of which are located at the 3’
terminal of exon 7, were not identified in heterozygous or hemizygous patients (figure
3b). The amplicon of this primer set (352 bp) was larger than the ideal amplicon
length for HRM analysis (less than 250 bp). Therefore two primer sets (exon7-1 and
7-2) covering the entire exon 7 coding region sequence(table 1 and figure 3a) were
designed to replace primer set 7. The primer set “exon 7-1” covered the 5’ region of
exon 7 and was designed to amplify a fragment of 220 bp. The primer set, exon 7-2,
covered the 3’ region of exon 7 and was designed to amplify a fragment of 233 bp.
ACCEPTED MANUSCRIPT
c.1194delA mutations were easily identified (D).
Figure 5. HRM curves of the mutations which were identified at exons in this study.
Panels A through F show the normalized difference plots for each amplicon. (A) exon
1, containing the wild type and mutant c.157A>G; (B): exon 2, containing the wild
type and mutants c.274G>A, c.331G>T, c.332G>A and c.335G>A; (C) exon 3,
containing the wild type and mutants c.394G>A and c.427G>A; (D) exon 4,
containing the wild type and mutant c.612G>A; (E) exon 5, containing the wild type
and mutants c.656T>C and c.695T>C; (F) exon 6, containing the wild type and
mutants c.886A>T and c.902G>A. (G) exon 7-1, containing the wild type and mutants
c.1034C>G, c.1066C>T, c.1067G>A, c.1078G>T and c.1087C>T. Notably, the
hemizygous c.1034C>G mutation could be distinguished from the wild-type sequence
when analyzed alone (Figure H); however, this discrimination disappeared when the
samples were analyzed with all other mutations. The HRM curves of exon 7-2 are
shown in figure (figure 3c).
Figure 6. An example of simultaneous screening for the IVS4+919G>A mutation in
30 samples
ACCEPTED MANUSCRIPT
IVS4+919G>A, in larger sample amount at the same run, 30 samples with the wild
type (n = 13), heterozygous (n = 10) and hemizygous (n = 7) IVS4+919G>A mutation
were simultaneously screened by HRM analysis. The hemizygous IVS4+919G>A
samples (genotype: A) could be distinguished from wild type sample (genotype: G/G)
by their Tm variations, while heterozygous samples (genotype: G/A) have a different
melting curve shape (A). Thus, individuals with the different genotypes of
IVS4+919G>A were clearly distinguishable from the wild type. Samples with the
IVS4+919G>A hemizygous genotype are marked in green, heterozygous are in red
and wild-type samples are in blue. (A): Normalized melting curve. (B): Difference
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT
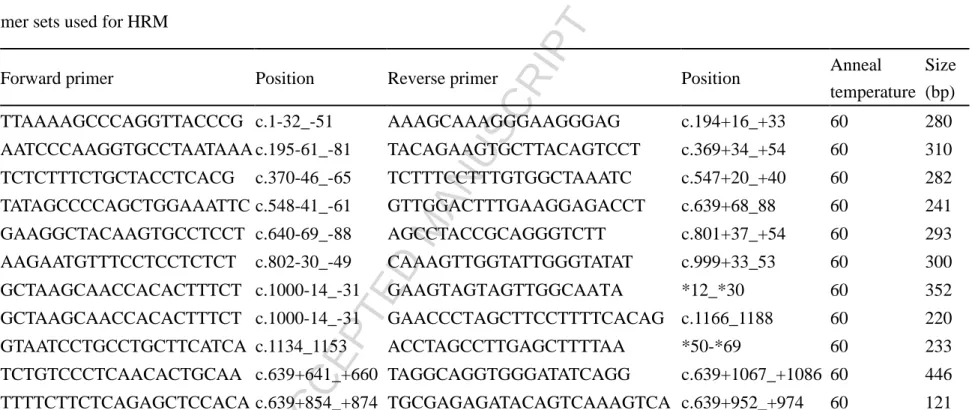
Table 1 Primer sets used for HRM
Amplicon Forward primer Position Reverse primer Position Anneal
temperature Size (bp)
Exon 1 TTAAAAGCCCAGGTTACCCG c.1-32_-51 AAAGCAAAGGGAAGGGAG c.194+16_+33 60 280
Exon 2 AATCCCAAGGTGCCTAATAAA c.195-61_-81 TACAGAAGTGCTTACAGTCCT c.369+34_+54 60 310
Exon 3 TCTCTTTCTGCTACCTCACG c.370-46_-65 TCTTTCCTTTGTGGCTAAATC c.547+20_+40 60 282
Exon 4 TATAGCCCCAGCTGGAAATTC c.548-41_-61 GTTGGACTTTGAAGGAGACCT c.639+68_88 60 241
Exon 5 GAAGGCTACAAGTGCCTCCT c.640-69_-88 AGCCTACCGCAGGGTCTT c.801+37_+54 60 293
Exon 6 AAGAATGTTTCCTCCTCTCT c.802-30_-49 CAAAGTTGGTATTGGGTATAT c.999+33_53 60 300
Exon 7a GCTAAGCAACCACACTTTCT c.1000-14_-31 GAAGTAGTAGTTGGCAATA *12_*30 60 352
Exon 7-1 GCTAAGCAACCACACTTTCT c.1000-14_-31 GAACCCTAGCTTCCTTTTCACAG c.1166_1188 60 220
Exon 7-2 GTAATCCTGCCTGCTTCATCA c.1134_1153 ACCTAGCCTTGAGCTTTTAA *50-*69 60 233
IVS4 a TCTGTCCCTCAACACTGCAA c.639+641_+660 TAGGCAGGTGGGATATCAGG c.639+1067_+1086 60 446
IVS4-1 TTTTCTTCTCAGAGCTCCACA c.639+854_+874 TGCGAGAGATACAGTCAAAGTCA c.639+952_+974 60 121
a
ACCEPTED MANUSCRIPT
Hightlights
> We developed method for HRM analysis of GLA gene using a same PCR/
melting programme.
>All Fabry mutations in heterozygous or hemizygous patients can be identified
with HRM.
>We also develop this HRM method in dry blood spots of newborns with Fabry