行政院國家科學委員會專題研究計畫 成果報告
九二一地震對健康影響之世代研究
計畫類別: 個別型計畫 計畫編號: NSC93-2320-B-002-081- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學公共衛生學院職業醫學與工業衛生研究所 計畫主持人: 詹長權 計畫參與人員: 袁韻涵 王彥雯 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 25 日
Chinese and English abstract Chinese abstract 背景:地震不但會造成外傷及死亡,對災民生理健康、心理狀態、生活型態 與週遭環境均會造成不同程度的影響。然而災難公共衛生學上仍有三個重要 問題需待澄清:包括地震後心理上有疾病或創傷的居民其長期之健康影響; 地震後生活品質改變與生理值變化的關係;地震對母親在心理及生理方面影 響是否容易造成新生兒低出生體重。 目的:本研究主要目的在透過世代追蹤研究的方式來評估921 地震災區心理 受創居民之健康狀況及公務人員世代在生活品質與生理變化上之關係;並且 評估地震前後南投縣新生兒低出生體重之變化。 方法:我們以南投縣政府於2001 年社區複合式篩檢活動所收集的居民作為 921 地震後心理上有疾病或創傷的研究對象,透過該活動所收集的中國人健 康量表(Chinese Health Questionnaire, CHQ)和體檢結果,聯結健保檔就醫資 料,得到5,390 人以進行長期健康追蹤。其次,透過過去兩年研究建立的南 投縣公務員世代,連結「台灣簡明版世界衛生組織生活品質問卷」 (WHOQOL-BREF)與社區複合式篩檢結果,共 553 人來評估生活品質與 生理在地震後的關聯性。最後,以問卷調查新生兒低出生體重之相關危險因 子及家中地震受災情況,利用1,593 名於 1998 年 9 月至 2004 年 8 月間出生 之新生兒作為新生兒世代,透過1997 年到 2003 年南投縣出生兒的登記資料 名來分析新生兒地震後低出生體重的趨勢。我們利用邏吉斯迴歸模式 (Logistic Regression Model)進行調整干擾因子後,評估生理與心理健康兩者 的相關性,比較生活品質與生理指標表現之間的關聯,以及新生兒低出生體 重和地震影響之關係。
道疾病,關節炎以及糖尿病與心理健康有關,而生活品質與生理指標兩者間 並沒有統計上的顯著相關。此外地震經歷與新生兒低出生體重沒有統計上的 顯著相關。
關鍵詞:地震,生活品質,健康影響,世代研究,災難
English Abstract
Backgrounds: Earthquakes not only caused traumas and deaths but also changed
seismic victims’ physiological health, mental health, lifestyle and environment. However, three key disaster public heath issues remain to be clarified including the association between acute psychological effects and long-term physiological effects, the relationship between quality of life and psychological health, the effects of maternal psychological impact and child low-birth weight.
Objective: This study evaluated the health effects of the 921 earthquake
including psychological and physical health effects, quality of life and infant low-birth weight by following the cohorts of adults and children in the disaster areas.
Method: We followed an adult cohort of 5,390 residents in Nantou County’s
community-based integrated screening programs to study their psychological impacts on disease-screened outcomes by linking the data from National Health Insurance Research Database. The Chinese Health Questionnaire (CHQ) had been used to collect the 1999 Taiwan Earthquake’s impact on these residents’ psychological health in 2001. We also used the public employee cohort with 553 persons established between 2000 and 2003 to investigate the relationship between WHOQOL and physiological index of chronic diseases. We examined
trends in the changes of low-birth weight for a birth cohort of 1,593 children born in Nantou County between 1998 and 2004. We used logistic regressive models to analyze collected data.
Results:The results showed that the people suffering from ischemic heart disease, cerebrovascular disease, chronic respiratory tract disease, diabetes and arthropathy were associated with mental health. There was no significant different risk of people with abnormal reports of biochemical tests by changing WHOQOL-BREF scores, and no statistical significant between earthquake experience and low-birth weight after adjusting relative risk factors.
Introduction
A powerful earthquake of 7.3 on the Richter scale struck central Taiwan at 1:47 a.m. on September 21, 1999, followed by thousands of aftershocks in the following five days. Nantou County, where the epicenter was located, was the most seismically damaged area. The earthquake caused 916 seismic deaths or missing persons and about 28,322 completely collapsed homes and 29,270 half-collapsed homes by Nantou government’s statistical data.
Earthquakes not only caused traumas and deaths but also changed seismic victims’ physiological health, mental health, lifestyle and environment. Previous epidemiological studies explored the short and long-term physiological health effects of earthquakes [1-5]. And several studies focused on the psychological well being of seismic victims [6-11]. According those, we knew that earthquake would cause sudden deaths or cardiovascular diseases [5], and increasing incidence of hypertension, diabetes, and arthropathy [4]. After one year of earthquake, the patients’ blood sugar control was worse than two year before and the control of patients’ blood sugar was associated with mental health and seismic damages [11].
It has been shown that survivors after a natural disaster such as an earthquake were more susceptible to post-traumatic stress disorders (PTSD), depression, insomnia, anxiety, and substance abuse than the subjects that were not afflicted by the disaster [12-18]. Previous study in Taiwan explored the prevalence of PTSD in the disaster area was quite large. Among 525 seismic victims screened by CHQ-12, the percentage of CHQ≥3 was about 89.9% [18].
Among the past studies about how earthquake affects people’s life quality, Wang et al. reported that the people with PTSD had lower quality of life (QOL) than the people
with no PTSD in north china [19]; experienced lower initial exposure but then received less post-disaster help reported poorer QOL and psychological well-being. [20]; the paper investigated by he 28-item Taiwanese-adapted brief version of the World Health Organization's quality of life questionnaire (WHOQOL-BREF) [21] in Taiwan reported that 268 subjects had lower QOL in physical capacity, psychological well-being, and environment 12 months after the earthquake than at the assessment prior to the earthquake [22].
The past studies revealed the long term health effects of earthquake. Trevisan M et al. discovered that the observed short-term increase in serum lipids and heart rate was not present long-term (7 years after the quake) in Italy [23]; higher resting heart rates were observed for individuals who reported financial loss, increased distance from family/friends, or decreased visiting as a result of relocation after the quakes [24]; participants who reported suffering from damage due to the 1980 quake showed on the average significantly increased serum uric acid after 7 years [25]. The highest numbers of deaths from all causes and from heart disease were observed within the first 6 months following the earthquake, and there was also the relation of damage and loss to newly reported hypertension, diabetes mellitus, and arthritis. The author suggested that the people sustaining such losses should be closely monitored for increased long term morbidity [26].
In the past studies about how the earthquake affects the pregnancy results, it pointed out that earthquake affects the pregnancy by act on hypothalamic-pituitary-adrenal (HPA) axis [27] [28]. There were two studies in Taiwan. Chang collected 171 women in a town near the epicenter during March to August in 2000 [29], and used a
Post-Earthquake Questionnaire, Chinese Health Questionnaire (CHQ-12) and
the level of the earthquake affected on the women mental states. The results of this study revealed that among the 115 pregnancies with known perinatal outcome, there were nine (7.8%) low-birth weight neonates, defined as birth weight < or = 2500 g, which higher than the prevalence of low-birth weight in Taiwan (2.8%~6.8%).
Moreover, in the paper of 「Association Between the 921 Earthquake and Pregnancy Outcome」written by Ching-Ting Huang of Collage of Public Health of National Taiwan University [30], it showed that there was no association between earthquake and pregnancy outcome such as preterm delivery and low-birth weight by analyzing the database of 1996-2000 from Ministry of Interior Department in Taiwan.
This study examines three hypotheses. Firstly, previous studies about health effects of earthquakes focused on seismic traumas and deaths, and the short-term physiological health or mental health effects of earthquakes. Nevertheless, the study about the association between physiological health and mental health effects was quite rare. Thus, this study by using seismic victims’ data of the chronic diseases, and mental health scores (CHQ-12 and SPAN) to illustrate the correlation between physiological health and mental health. Second, from past studies, earthquake causes the variation of quality of life and biochemical indicators. Therefore it is necessary to investigate the relationship between QOL and biochemical indicators to clarify weather we could discover the health problem of victims in Nantou County promptly and easily by using quality of life questionnaire. Finally, although the relationship between
earthquake and the low-birth weight of infants had been investigated, the past studies restricted by the limitation of data collection, it didn’t adjust some risk factor of low-birth weight, such as medical history, pregnancy experience, smoking condition of mother, etc. the major risk factor of low-birth weight including the heredity, constitution of mother, demographic characteristics, mentality, nutrition, ill during
pregnancy, and exposure to toxicants [31], and the most important risk factors of low-birth weight in developing country are smoking condition, nutrition and the weight before pregnancy. Thus, this study examines the relationship between earthquake and the low-birth weight of infants through adjusting the risk factor of low-birth weight.
Method and Material
.Evaluating the correlation between physiological health and mental health
Participants
After the 1999 Taiwan earthquake happened, we conducted a longitudinal survey to follow-up residents in Nantou County. The number of total participants was 5930, and they were divided into two cohorts; one was 273 public employees who had either worked in the county government or one of the 13 town governments, and the other was 5117 general residents who were not public employees.
Data collection
In our survey, the cases who suffered from a chronic disease between 21/03/1999 and 20/03/2002 were obtained from the National Health Insurance Research Database. The chronic diseases included diabetes (ICD-9 codes 250), ischemic heart disease (ICD-9 codes 410-414), essential hypertension (ICD-9 codes 401), cerebrovascular disease (ICD-9 codes 430-438), chronic respiratory tract disease (ICD-9 codes 490-493), atherosclerosis (ICD-9 codes 440), hyperlipidaemia (ICD-9 codes 2720-2721), and arthropathy (ICD-9 codes 710-719). If a person suffered from diabetes before 30 years old, then we deleted him or her in order to exclude cases with
congenital diabetes.
The participants’ individual characteristics were collected from Nantou Community-based Integrated Screening (NCIS) database during 25/04/2001 to 01/07/2001, and 16/03/2002 to 28/08/2002. The individual characteristics included socio-demographic characteristics (gender, age, education, marital status, religion and occupation), health behaviors (smoking, drinking, eating betelquids, exercise and diet habits) and personal and family health history.
Moreover, we obtained individual mental health data from Tsaotun Psychiatric Center Department of Health (TTPC). TTPC developed a post-earthquake stress and mental health survey for all residents in Nantou disaster area during 25/04/2001 to 21/10/2001 and 16/03/2002 to 26/09/2002. In this survey, the questionnaire included three parts: the participants’ socio-demographic characteristics, 12-item versions of the Chinese Health Questionnaire (CHQ-12), and SPAN. The CHQ is a self-administered screening instrument used to identify non-psychotic psychiatric disorders in community settings. Its reliability and validation had been verified [32-35]. The SPAN is a brief four-item, patient rated, written screening instrument for post-traumatic stress disorder (PTSD) [36].
Statistical analysis
We first compared the differences between two cohorts and understood the frequency distribution of socio-demographic characteristics, health behaviors, mental health score, and prevalence of chronic disease.
Then, we used logistic regression model to estimate odds ratio and its 95% confidence intervals of the chronic disease prevalence between general residents and public
employees every six months during 01/01/1999 to 20/03/2002 by adjusting gender, age, smoking, drinking, betelquids, and exercise habit and let public employees’ odds=1. In addition, we checked goodness-of-fit of all models and done regression diagnostics including residual analysis, influence analysis, checking for multicollinearity and detection of separation.
Moreover, we set up another two kinds of logistic regression models to evaluate the association between chronic diseases and mental health. These models were constructed with gender, age, smoking, drinking, betelquids, exercise habit, cohort, CHQ score, SPAN score, and the time of attending TTPC’s survey as covariates. One used total participants’ data and the other only used general residents’ data. In addition, we checked goodness-of-fit of all models and done regression diagnostics including residual analysis, influence analysis, checking for multicollinearity and detection of separation.
.Evaluating the relationship between QOL and biochemical indicators
Participants
After the 1999 Taiwan earthquake happened, we conducted a cross-sectional survey for public employees who had either worked in the county government or one of the 13 town governments in Nantou County.
Data collection
The participants’ individual characteristics were collected from Nantou Community-based Integrated Screening (NCIS) database during 25/04/2001 to 01/07/2001, and 16/03/2002 to 28/08/2002. The individual characteristics included
socio-demographic characteristics (gender, age, education, marital status, religion and occupation), health behaviors (smoking, drinking, eating betelquids, exercise and diet habit) and personal and family health history.
Self-reported questionnaires were sent out to all Nantou County public employees during 30/07/2002 to 09/08/2002 and 26/03/2003 to 02/05/2003. The questionnaire included three major parts: the participants’ socio-demographic characteristics, experiences in the earthquake, and quality of life. The demographic data collected in the questionnaire included the age, gender, marital status, education, and religion of our participants. Six earthquake experience measures in our questionnaire included house damages, evacuation, financial loss, financial hardship, bereavement, and disruption of water supply. And the participants’ quality of life was measured by the Taiwan version of WHOQOL-BREF, whose reliability and validity have been verified previously (Yao, et al., 2002). There were 28 items that measured the physical, psychological, social and environmental domains of health (The WHOQOL Group, 1998). The Taiwan version included two cultural-specific items, “face” (being respected) in the social domain, and “food” in the environmental domain (Yao, et al., 2002). The standardized domain scores were between 0 and 100. Higher scores represent higher quality of life in each domain. WHOQOL-BREF has been used in previous post-earthquake health studies (Wang, et al., 2000a; Wang, et al., 2000b; Lin, 2002).
Statistical analysis
We first understood the distribution of socio-demographic characteristics, health behaviors, earthquake experience, biochemical indicators, and WHOQOL-BREF scores.
Then, we used logistic regression model to evaluate the association between biochemical indicators and WHOQOL-BREF scores and estimate odds ratio and its 95% confidence intervals. These models were constructed with gender, age, smoking, drinking, betelquids, financial loss, financial hardship, bereavement, house damages, and WHOQOL-BREF scores as covariates. In addition, we checked goodness-of-fit of all models and done regression diagnostics including residual analysis, influence analysis, checking for multicollinearity and detection of separation.
.Evaluating the relationship between earthquake and low-birth weight
Participants
After the 1999 Taiwan earthquake happened, we conducted a longitudinal survey of mother residing in the 13 towns of Nantou County.
Data collection
We conducted questionnaire to collect the information of the mothers of zero to three year old infants during September to December in 2003, which was 2,661 copies, and zero to one year old infants during July to October in 2004, which was 2,012 copies. The total number of the questionnaire was 4,673. The information consisted of the demographic data including the mother’s ID, name, birth, blood, height and weight, and the infant’s ID, name and birth. In addition, we collected the smoking and environmental tobacco exposure conditions during their pregnancy in this
questionnaire. All the questionnaire was conducted by training personnel of every Township (Country) Public Health Center when the mother took the infants to the Township (Country) Public Health Center for vaccine. Besides, we combined the Nantou Community-based Integrated Screening (NCIS) database during 25/04/2001
to 01/07/2001, and 16/03/2002 to 28/08/2002 to compensate the missing data of the height, weight and smoking condition in questionnaire by infants’ ID numbers. To acquire the data of the infants, we used a computerized birth certificate registry database of 1997-2003 from Ministry of Interior Department in Taiwan. From the database, we obtained the ID of the mother and infants, the weight of infants, and some potential risk factor of infant low birth weight, including the sex, parity of the infants.
Study population
We linked the questionnaire information to the database of Ministry of Interior Department in Taiwan by the infants’ ID numbers. After excluding the incomplete cases and cases with no valid value, the number of total cases is 1593, and they were divided into six groups. First, we defined the infant whose birth was before September 21, 1999 as non-exposure group. Then, the infants whose birthday were between September 21, 1999 and July 20, 2000 (that is, subject whose pregnancy period
passed through September 21, 1999), were considered as exposure group 1. Moreover, considering the long term effect of the earthquake, we divided the remained infants by 10 months as interval, resulting in other four groups: the one whose birthday were between July 21, 2000 and May 20, 2001, whose birthday were between May 21, 2001 and March 20, 2002, whose birthday were between March 21, 2002 and January 20, 2003 and the birthday were between January 21, 2000 and December 31, 2003 (as exposure group 2, exposure group 3, exposure group 4 and exposure group 5).
Statistic analysis
Among the six groups, descriptive statistics of all numeric variables, including means, standard deviations, together with the proportions of all categorical variables were
calculated. Six independent group means were compared by means of ANOVA for independent groups when the variables indicated normal distribution, otherwise Kruskal Wallis Test was performed. Differences between group proportions were examined by χ2test.
The confounding variables about low birth weight are sex, parity, fetal number, smoking condition during pregnancy, BMI, and accouchement age. To adjust these confounders, logistic regression model was built and possible predictors were examined. We calculate odds ratio and construct 95% confidence interval. Statistical significance was assigned to p-values < 0.05.
Results
.Evaluating the correlation between physiological health and mental health
Table 1 summarizes the characteristics of participants. The percentage of male public employees is about 40% and is more than male general residents. Public employees are younger than general residents and have smaller age variation. Public employees have more positive health behavior but the number of those who take exercise regularly is smaller. Moreover, the public employees’ mental health scores are both smaller than general residents’.
Table1. Frequency distributions of socio-demographic characteristics, health behaviors, and mental health scores among 5390 public employees and general residents in Nantou County, Taiwan.
Public employees N ( % ) General residents N ( % ) Total N ( % ) Gender Male 111 (41) 1862 (36) 1973 (37) Female 162 (59) 3255 (64) 3417 (63) Smoke No 234 (86) 3970 (78) 4204 (78) Give up 33 (12) 317 ( 6) 350 ( 6) Yes 6 ( 2) 830 (16) 836 (16) Drink No 239 (88) 3766 (74) 4005 (74) Give up 23 ( 8) 249 ( 5) 272 ( 5) Yes 11 ( 4) 1102 (22) 1113 (21) Betelquids No 261 (95) 4455 (87) 4716 (88) Give up 10 ( 4) 282 ( 6) 292 ( 5) Yes 2 ( 1) 380 ( 7) 382 ( 7) Take exercise No 165 (60) 2568 (50) 2733 (51) Yes 108 (40) 2549 (50) 2657 (49) Age mean(SD) 47.0 (9.9) 54.9 (15. 5) 54.5 (15.3) Chinese Health Questionnaire (CHQ)
mean(SD) 1.7 (2.4) 2.5 (3.1) 2.4 (3.0) SPAN
mean(SD) 2.3 (2.2) 3.0 (2.5) 2.9 (2.5)
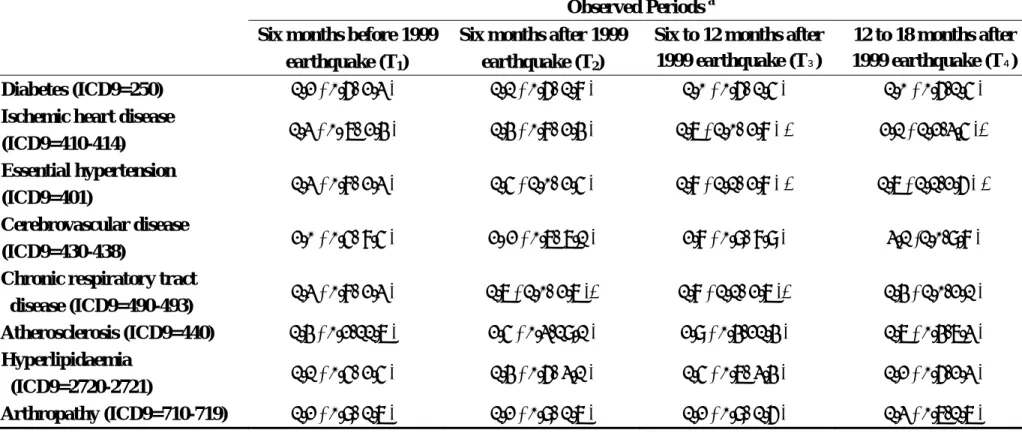
Table 2 shows that the prevalence of chronic diseases is not significantly different between public employees and general residents before earthquake happened. In half-year of post-earthquake, general residents’ risk of developing chronic respiratory tract disease is about 1.7 times as public employees’ but their risks of other diseases are not significantly different. After half-year to one year of post-earthquake, general
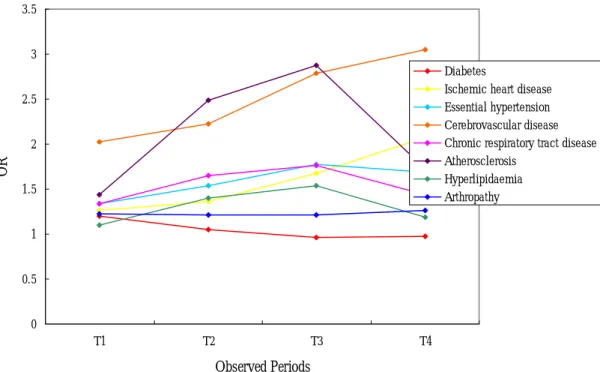
residents’ risk of developing ischemic heart disease, essential hypertension and chronic respiratory tract disease is about 1.7, 1.8 and 1.8 times as public employees’, but their risks of other diseases are not significantly different. After one year to one and half-year of post-earthquake, general residents’ risk of developing ischemic heart disease and essential hypertension is about 2.1 and 1.7 times as public employees’, but their risks of other diseases are not significantly different. As time goes by, we can find the OR of ischemic heart disease, cerebrovascular disease, and arthropathy increase, and the OR of diabetes decreases a little. Before one year of post-earthquake, the OR of essential hypertension, chronic respiratory tract disease, atherosclerosis, and hyperlipidaemia increase with time but decrease afterwards. (Figure 1)
Table 2. Logistic regression adjusted odds ratio (OR) and 95% confidence intervals of chronic disease prevalence of 4 observed periods during
1999.03.21 to 2001.03.21 between 273 public employees and 5117 general residents in Nantou County, Taiwan.
Observed Periods a
Six months before 1999 earthquake (T1)
Six months after 1999 earthquake (T2)
Six to 12 months after 1999 earthquake (T3)
12 to 18 months after 1999 earthquake (T4)
Diabetes (ICD9=250) 1.2 ( 0.6- 2.3 ) 1.1 ( 0.6- 1.8 ) 1.0 ( 0.6- 1.5 ) 1.0 ( 0.6-1.5 ) Ischemic heart disease
(ICD9=410-414) 1.3 ( 0. 7- 2.4 ) 1.4 ( 0.8- 2.4 ) 1.7 ( 1.0- 2.8 ) * 2.1 ( 1.2-3.5 )* Essential hypertension
(ICD9=401) 1.3 ( 0.8- 2.3 ) 1.5 ( 1.0- 2.5 ) 1.8 ( 1.1- 2.8 ) * 1.7 ( 1.1-2.6 ) * Cerebrovascular disease
(ICD9=430-438) 2.0 ( 0.5- 8.5 ) 2. 2 ( 0.7- 7.1 ) 2.8 ( 0.9- 8.9 ) 3.1 (1.0-9.8 ) Chronic respiratory tract
disease (ICD9=490-493) 1.3 ( 0.8- 2.3 ) 1.7 ( 1.0- 2.7 )* 1.8 ( 1.1- 2.7 )* 1.4 ( 1.0-2.1 ) Atherosclerosis (ICD9=440) 1.4 ( 0.2-11.7 ) 2.5 ( 0.3-19.1 ) 2.9 ( 0.4-21.4 ) 1.7 ( 0.4-7.3 ) Hyperlipidaemia (ICD9=2720-2721) 1.1 ( 0.5- 2.5 ) 1.4 ( 0.6- 3.1 ) 1.5 ( 0.7- 3.4 ) 1.2 ( 0.6-2.3 ) Arthropathy (ICD9=710-719) 1.2 ( 0.9- 1.7 ) 1.2 ( 0.9- 1.7 ) 1.2 ( 0.9- 1.6 ) 1.3 ( 0.7-1.7 ) a T1: 1999.03.21~1999.09.20, T2: 1999.09.21~2000.03.20, T3: 2000.03.21~2000.09.20, T4: 2000.09.21~2001.03.20. * P-value<0.05
0 0.5 1 1.5 2 2.5 3 3.5 T1 T2 T3 T4 Observed Periods OR Diabetes
Ischemic heart disease Essential hypertension Cerebrovascular disease Chronic respiratory tract disease Atherosclerosis
Hyperlipidaemia Arthropathy
Figure 1. Logistic regression adjusted odds ratio (OR) of chronic disease prevalence of 4 observed periods during 1999.03.21 to 2001.03.21 between 273 public employees and 5117 general residents in Nantou County, Taiwan.
After adjusting relative risk factor of chronic diseases, the results of total participants’ OR of chronic diseases are similar to general residents’ in table 3 and 4. The risk of people suffering from ischemic heart disease, cerebrovascular disease, and chronic respiratory tract disease increase about 1.07, 1.03, and 1.04 times every one CHQ score. The risk of people suffering from diabetes, and arthropathy increase about 1.06, and 1.04 times every one SPAN score. We don’t find significantly different risk of people suffering from other chronic disease by changing mental health scores.
The goodness-of-fit of all logistic regression models are passable because the percentages of concordant pairs, discordant pairs, and tied pairs of all models are between 70% to 80%, 20% to 30%, and less than 3%. And we don’t find any big problem in our models by regression diagnostics including residual analysis, influence
analysis (plotting graphs of ∆ versus ˆP with symbols proportional to Bχp2 ∆ and checking |DFBETASjk| ), checking for multicollinearity (calculating correlation matrix
of ˆβ and VIF), and detection of separation.
Table 3. Logistic regression adjusted odds ratio (OR) and 95% confidence intervals of chronic disease prevalence on mental health score, CHQ-12 and SPAN, during 2000.09.21 to 2001.03.21 among 5390 public employees and general residents in Nantou County, Taiwan.
Mental Health Score
CHQ-12 SPAN
Diabetes (ICD9=250) 0.99 ( 0.96-1.02 ) 1.06 ( 1.02-1.09 )* Ischemic heart disease (ICD9=410-414) 1.07 ( 1.04-1.09 )* 1.02 ( 0.99-1.05 ) Essential hypertension (ICD9=401) 1.03 ( 1.01-1.06 )* 1.01 ( 0.98-1.04 ) Cerebrovascular disease (ICD9=430-438) 1.03 ( 0.99-1.07 ) 1.03 ( 0.98-1.08 ) Chronic respiratory tract disease
(ICD9=490-493) 1.04 ( 1.01-1.06 )* 1.01 ( 0.98-1.04 ) Atherosclerosis (ICD9=440) 0.98 ( 0.92-1.04 ) 1.07 ( 0.99-1.15 ) Hyperlipidaemia (ICD9=2720-2721) 0.99 ( 0.95-1.03 ) 1.05 ( 1.00-1.08 ) Arthropathy (ICD9=710-719) 1.02 ( 1.00-1.04 ) 1.04 ( 1.01-1.07 )*
Table 4. Logistic regression adjusted odds ratio (OR) and 95% confidence intervals of chronic disease prevalence on mental health score, CHQ-12 and SPAN, during 2000.09.21 to 2001.03.21 among 5117 general residents in Nantou County, Taiwan
Mental Health Score
CHQ-12 SPAN
Diabetes (ICD9=250) 0.99 ( 0.96-1.02 ) 1.06 ( 1.02-1.09 )* Ischemic heart disease (ICD9=410-414) 1.06 ( 1.03-1.09 )* 1.02 ( 0.99-1.05 ) Essential hypertension (ICD9=401) 1.03 ( 1.00-1.05 )* 1.01 ( 0.98-1.04 ) Cerebrovascular disease (ICD9=430-438) 1.02 ( 0.99-1.06 ) 1.03 ( 0.98-1.08 ) chronic respiratory tract disease
(ICD9=490-493) 1.04 ( 1.01-1.06 )* 1.01 ( 0.99-1.05 ) Atherosclerosis (ICD9=440) 0.98 ( 0.92-1.05 ) 1.07 ( 0.99-1.15 ) Hyperlipidaemia (ICD9=2720-2721) 0.99 ( 0.95-1.03 ) 1.05 ( 1.00-1.10 )* Arthropathy (ICD9=710-719) 1.02 ( 1.00-1.04 ) 1.04 ( 1.01-1.07 )* * P-value<0.05
.Evaluating the relationship between QOL and biochemical indicators
As shown in table 5, among the 553 public employees in our study, about 62% were female, and their average age was 44.1 years old with SD 9.7. Out of the 553 participants, 84.8% were married, and 10.7%, 12.7%, 3.6% had smoking, drinking and eating-betelquids habits. They had financial loss more than 499K, financial hardship, bereavement, or house damages about 33.3%, 19.2%, 28.7%, and 18.3%. Their mean (+SD) scores in the physical, psychological, social and environmental domains of quality of life were 62.0 (+13.6), 56.2 (+14.7), 59.7 (+14.0), and 52.9 (+14.1) respectively.
Table 5. Description of socio-demographic characteristics, health behaviors, earthquake experience and WHOQOL-BREF scores among public employees in Nantou County, Taiwan.
N ( % ) mean (SD)
Gender Age
Male 210 (38.0) 44.1 (9.7)
Female 343 (62.0) Physical domain
Marital status 62.0 (13.6)
not married 83 (15.2) Psychological domain
married 464 (84.8) 56.2 (14.7)
Smoke Social domain
No 491 (89.3) 59.7 (14.0)
Yes 59 (10.7) Environment domain
Drink 52.9 (14.1) No 479 (87.3) Yes 70 (12.7) Betelquids No 530 (96.4) Yes 20 ( 3.6) Financial loss ≦499K 369 (66.7) ≧500K 184 (33.3) Financial hardship No 447 (80.8) Yes 106 (19.2) Bereavement No 394 (71.3) Yes 159 (28.7) House damages No 452 (81.7) Yes 101 (18.3)
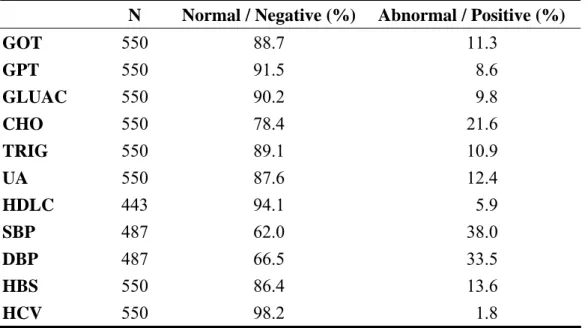
The results of biochemical tests were shown in table6. We divided the outcomes of biochemical tests in to two groups: normal and abnormal, according to the standard suggested by National Taiwan University Hospital. We found most of public employees were normal. About 11.3%, 8.6%, 9.8%, 21.6%, 10.9%, 12.4%, 5.9%,
38.0%, and 33.5% were abnormal on GOT, GPT, GLUAC, CHO, TRIG, UA, HDLC, SBP, and DBP. 13.6% and 1.8% were positive on HBS and HCV.
Table 6. Frequency distributions of reports of biochemical tests among public
employees in Nantou County, Taiwan.
N Normal / Negative (%) Abnormal / Positive (%)
GOT 550 88.7 11.3 GPT 550 91.5 8.6 GLUAC 550 90.2 9.8 CHO 550 78.4 21.6 TRIG 550 89.1 10.9 UA 550 87.6 12.4 HDLC 443 94.1 5.9 SBP 487 62.0 38.0 DBP 487 66.5 33.5 HBS 550 86.4 13.6 HCV 550 98.2 1.8
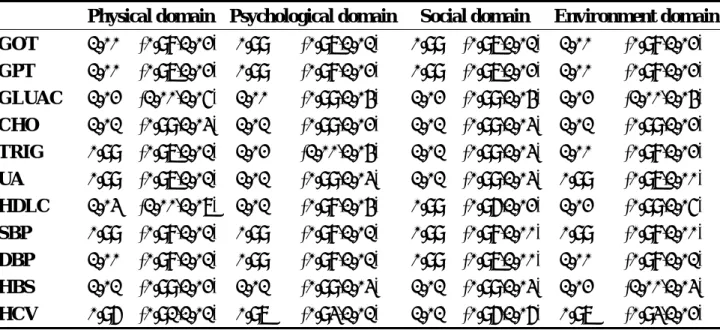
After adjusting gender, age, smoking, drinking, betelquids, financial loss, financial hardship, bereavement, and house damages, the results of participants’ OR of abnormal reports of biochemical tests are shown in table 7. The risk of people with abnormal reports of biochemical tests increased between 0.96 and 1.03 times every one WHOQOL-BREF score. We didn’t find significantly different risk of people with abnormal reports of biochemical tests by changing WHOQOL-BREF scores.
Table 7. Logistic regression adjusted odds ratio (OR) and 95% confidence intervals of reports of biochemical tests on WHOQOL-BREF among public employees in Nantou County, Taiwan.
Physical domain Psychological domain Social domain Environment domain GOT 1.00 (0.98,1.02) 0.99 (0.97,1.01) 0.99 (0.97,1.01) 1.00 (0.98,1.02) GPT 1.00 (0.97,1.02) 0.99 (0.98,1.02) 0.99 (0.97,1.02) 1.00 (0.98,1.02) GLUAC 1.02 (1.00,1.05) 1.00 (0.99,1.04) 1.02 (0.99,1.04) 1.02 (1.00,1.04) CHO 1.01 (0.99,1.03) 1.01 (0.99,1.02) 1.01 (0.99,1.03) 1.01 (0.99,1.02) TRIG 0.99 (0.97,1.01) 1.02 (1.00,1.04) 1.01 (0.99,1.03) 1.00 (0.98,1.02) UA 0.99 (0.97,1.01) 1.01 (0.99,1.03) 1.01 (0.99,1.03) 0.99 (0.97,1.00) HDLC 1.03 (1.00,1.07) 1.01 (0.98,1.04) 0.99 (0.96,1.02) 1.02 (0.99,1.05) SBP 0.99 (0.98,1.01) 0.99 (0.98,1.01) 0.99 (0.98,1.00) 0.99 (0.98,1.00) DBP 1.00 (0.98,1.01) 0.99 (0.98,1.01) 0.99 (0.97,1.00) 1.00 (0.98,1.01) HBS 1.01 (0.99,1.02) 1.01 (0.99,1.03) 1.01 (0.99,1.03) 1.02 (1.00,1.03) HCV 0.96 (0.91,1.01) 0.97 (0.93,1.01) 1.01 (0.96,1.06) 0.97 (0.93,1.02)
.Evaluating the relationship between earthquake and low-birth weight
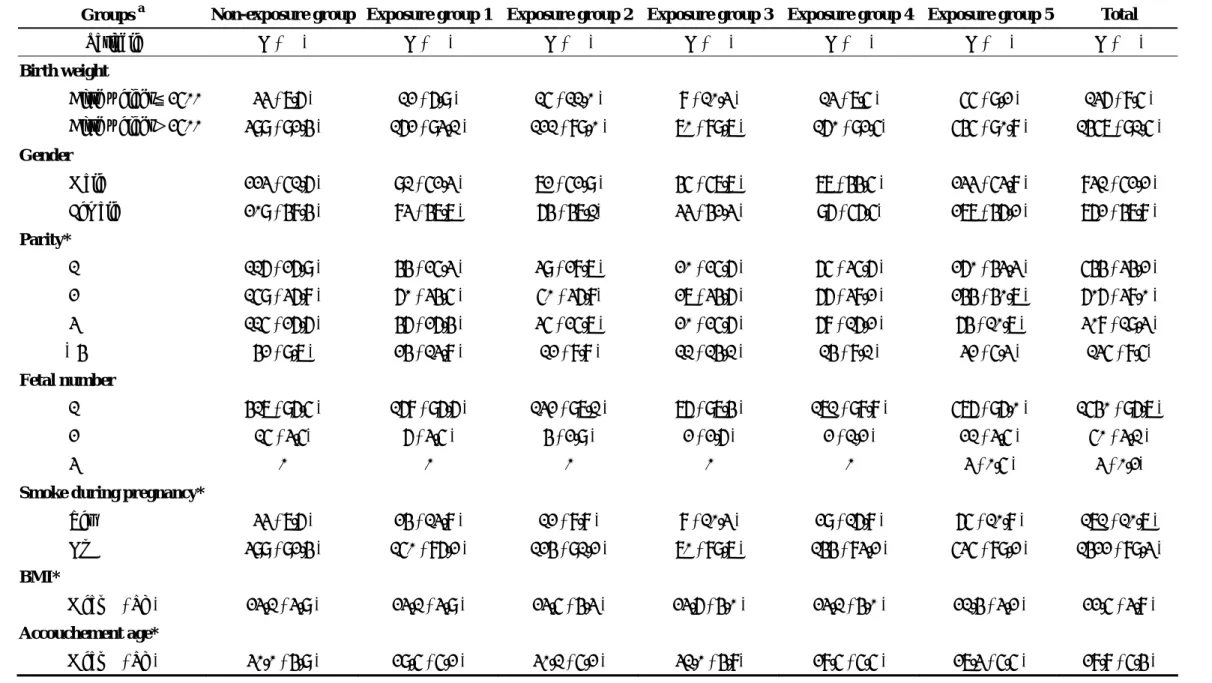
A total number of 1593 infants were included in this study. The characteristics of infants, including the frequencies of different birth weigh, fetal gender, parity, fetal number, maternal smoking condition, BMI and accouchement age, are showed in Table 8. Among the 1593 subjects, there were 432 (27.1%) subjects in non-exposure group, 174 (10.9%) in exposure group 1, 136 (8.5%) in exposure group 2, 78 (4.9%) in exposure group 3, 173 (10.9%) in exposure group 4 and 600 (37.7%) in exposure group 5. The prevalence of low-birth weight among the six groups was between 6.9%- 11.0%, and there was no significant difference between the six groups. The mean BMI and accouchement age of 1593 patients was 22.54 ±3.78 and 28.83 ± 5.38, respectively. As presented in Table 8, we found some variables are significantly different between different birth cohorts, including parity, smoking condition during pregnancy, BMI, and accouchement age.
Table 8. Descriptive statistics of all variables among the six groups of infants born between 1997 and 2003 in Nantou County.
Groups a Non-exposure group Exposure group 1 Exposure group 2 Exposure group 3 Exposure group 4 Exposure group 5 Total
Variable N ( % ) N ( % ) N ( % ) N ( % ) N ( % ) N ( % ) N ( % ) Birth weight Birth weight≦2500 33 ( 7.6 ) 12 ( 6.9 ) 15 ( 11.0 ) 8 ( 10.3 ) 13 ( 7.5 ) 55 ( 9.2 ) 136 ( 8.5 ) Birth weight>2500 399 ( 92.4 ) 162 ( 93.1 ) 121 ( 89.0 ) 70 ( 89.7 ) 160 ( 92.5) 545 ( 90.8 ) 1457 ( 91.5 ) Gender Male 223 ( 51.6 ) 91 ( 52.3 ) 72 ( 52.9 ) 45 ( 57.7 ) 77 ( 44.5 ) 233 ( 53.8 ) 831 ( 52.2 ) Female 209 ( 48.4 ) 83 ( 47.7 ) 64 ( 47.1) 33 ( 42.3 ) 96 ( 56.5) 277 ( 46.2 ) 762 ( 47.8 ) Parity* 1 116 ( 26.9 ) 44 ( 25.3 ) 39 ( 28.7 ) 20 ( 25.6 ) 65 ( 35.6 ) 260 ( 43.3 ) 544 ( 34.2 ) 2 159 ( 36.8 ) 60 ( 34.5 ) 50 ( 36.8) 27 ( 34.6 ) 66 ( 38.2 ) 244 ( 40.7 ) 606 ( 38.0 ) 3 115 ( 26.6 ) 46 ( 26.4 ) 35 ( 25.7 ) 20 ( 25.6 ) 68 ( 16.2 ) 64 ( 10.7 ) 308 ( 19.3 ) ≥4 42 ( 9.7 ) 24 ( 13.8 ) 12 ( 8.8 ) 11 ( 14.1 ) 14 ( 8.1 ) 32 ( 5.3 ) 135 ( 8.5) Fetal number 1 417 ( 96.5 ) 168 ( 96.6 ) 132 ( 97.1 ) 76 ( 97.4 ) 171 ( 98.8 ) 576 ( 96.0 ) 1540 ( 96.7 ) 2 15 ( 3.5) 6 ( 3.5 ) 4 ( 2.9 ) 2 ( 2.6 ) 2 ( 1.2 ) 21 ( 3.5 ) 50 ( 3.1 ) 3 0 0 0 0 0 3 ( 0.5 ) 3 ( 0.2)
Smoke during pregnancy*
Yes 33 ( 7.6 ) 24 ( 13.8 ) 12 ( 8.8 ) 8 ( 10.3 ) 29 ( 16.8 ) 65 ( 10.8 ) 171 ( 10.7 ) No 399 ( 92.4 ) 150 ( 86.2 ) 124 ( 91.2 ) 70 ( 89.7 ) 144 ( 83.2 ) 535 ( 89.2 ) 1422 ( 89.3 ) BMI* Mean ( Sd ) 23.1 ( 3.9 ) 23.1 ( 3.9 ) 23.5 ( 4.3 ) 23.6 ( 4.0 ) 23.1 ( 4.0 ) 21.4 ( 3.2 ) 22.5 ( 3.8 ) Accouchement age* Mean ( Sd ) 30.0 ( 4.9 ) 29.5 ( 5.2 ) 30.1 ( 5.2 ) 31.0 ( 4.8) 28.5 ( 5.5 ) 27.3 ( 5.5 ) 28.8 ( 5.4 )
a Non-exposure group: subject whose birthday is before September 21 ,1999;
Exposure group 1: subject whose birthday is between September 21 ,1999 and July 20, 2000. (subjects whose pregnancy period passed through September 21 ,1999). Exposure group 2: subject whose birthday is between July 21, 2000 and May 20, 2001 Exposure group 3: subject whose birthday is between May 21, 2001 and March 20, 2002 Exposure group 4: subject whose birthday is between March 21, 2002 and January 20, 2003 Exposure group 5: subject whose birthday is between January 21, 2000 and December 31, 2003 * p<0.05
The low birth weight data set in Table 8 presents six factors associated with low-birth weight: exposing earthquake or not (six groups), fetal gender (female and male), parity (four categories), and mother’s accouchement age, smoking condition (yes or no), and BMI. We fit a logistic regression model using all these to predict whether the infant’s birth weight was lower than 2500g (y =1). Table 9 shows the results of
logistic regression adjusted these factors.
Table.9. Logistic regression adjusted odds ratio (OR) and 95% confidence intervals of low birth weight in Nantou County, Taiwan
Odds Ratio 95% Confidence Intervel
Smoking condition (Y vs. N ) 1.16 0.67 2.00 Accouchement age 0.98 0.95 1.02 BMI 1.01 0.96 1.06 Fetal gender (F vs. M) 1.10 0.78 1.57 Parity (≥ 4 vs. 1) 1.04 0.53 2.03 (3 vs. 1) 0.86 0.51 1.45 (2 vs. 1) 0.74 0.49 1.13 Exposure group (group 1 vs. group 0) 0.87 0.44 1.73 (group 2 vs. group 0) 1.50 0.79 2.85 (group 3 vs. group 0) 1.39 0.61 3.14 (group 4 vs. group 0) 0.93 0.47 1.82 (group 5 vs. group 0) 1.17 0.73 1.87
The odds ratio is 1.16 for smoking during pregnancy versus non-smoking during pregnancy, 1.10 for female infant versus male infant, 0.983 for a unit increase of maternal age, and 1.010 for a unit increase of BMI. As regards fetal parity, the odds ratio is 1.04 for fetal number≥ 4 versus fetal number=1, 0.86 for fetal number=3 versus fetal number=1, 0.74 for fetal number=2 versus fetal number=1. in the case of earthquake exposure group, the non-exposure group defined as baseline data, the odds
ration is 0.87 for exposure group 1 versus non-exposure group, 1.50 for exposure group 2 versus non-exposure group, 1.39 for exposure group 3 versus non-exposure group, 0.93 for exposure group 4 versus non-exposure group and 1.17 for exposure group 5 versus non-exposure group. As presents in Table 9, all 95% confidence interval of odds ratios contain 1. Therefore, all six variables are not statistically significant in low birth weight.
Discussion
Combining the studies of the three years, we could obtain the conclusions as following:
1. The incidence rate of ischemic heart disease among public employee increased in the two years after earthquake (2000-2001), and decreased in 2002; the incidence rate of diabetes in 2000 higher than the baseline before earthquake, and decreased after one year. The incidence rate of essential hypertension and respiratory tract disease were lower than the baseline before earthquake.
2. After the long term analysis of data from Bureau of National Health Insurance between 1999 and 2002, there were no increments of clinic visits numberfor the ischemic heart disease, hypertension, diabetes and respiratory disease. However, there were increments of clinic visit for the ischemic heart disease and diabetes after three years letter of earthquake; clinic visits of respiratory disease increased within one year letter of earthquake but there was no statistic difference after one year.
3. Clinic visits for diabetes and respiratory disease was higher among public employees with financial difficulty. Public employees with housing damage were determined with the higher clinic visits for ischemic heart disease and respiratory
disease. Clinic visits for ischemic heart disease, diabetes and respiratory disease were higher among public employees with bereavement.
4. After comparing the prevalence of chronic diseases between public employee and general population, we found general residents’ risk of developing chronic respiratory tract disease is about 1.7 times as public employees’ in half-year of post-earthquake. After half-year to one year of post-earthquake, general residents’ risk of developing ischemic heart disease, essential hypertension and chronic respiratory tract disease is about 1.7, 1.8 and 1.8 times as public employees’. After one year to one and half-year of post-earthquake, general residents’ risk of developing ischemic heart disease and essential hypertension is about 2.1 and 1.7 times as public employees’.
5. In evaluating the correlation between physiological health and mental health, the risk of people suffering from ischemic heart disease, cerebrovascular disease, and chronic respiratory tract disease increase about 1.07, 1.03, and 1.04 times every one CHQ score. The risk of people suffering from diabetes, and arthropathy increase about 1.06, and 1.04 times every one SPAN score.
6.Among 3 categories of public employees, teachers had the highest scores of WHOQOL, followed by public servants, and policemen and firefighters.Financial loss and financial difficulty were two main components associated with public employees’ quality of life after the earthquake. Marital and educational status had positive effects toward quality of life; married public employees and the one with college or university or above had higher quality of life. Furthermore, female had higher quality of life in social domain then male, and the old had higher quality of life in environmental domain.
7. Significant improvement of quality of life in four domains among public employees had been observed in 2002 by comparing the quality of life surveys held in 2000, especially in environmental domain. The public employee with financial difficulty significantly decreased then the one with no financial difficulty in physical,
psychological and environmental domains; the public employee with financial loss significantly decreased then the one with no financial loss in physical domain. Age, gender, occupation, religious belief, marital and educational status and life style had different effects among the four domains of quality of life.
8. The survey of health situation done in 2001 and 2002 showed that the residents with completely or partially collapsed house-damage had higher SBP, DBP, UA but lower HDLC then general victims in 2001, and higher DBP, UA, GOT but lower HDLC in 2002. Among the 3 categories of earthquake survivors, residents with completely or partially collapsed house-damage had the worst health situation and highest proportion of cigarette smoking, alcohol drinking, and betel quid chewing. 9. Dividing the outcomes of biochemical tests into normal and abnormal showed that about 11.3%, 8.6%, 9.8%, 21.6%, 10.9%, 12.4%, 5.9%, 38.0%, and 33.5% were abnormal on GOT, GPT, GLUAC, CHO, TRIG, UA, HDLC, SBP, and DBP. 13.6% and 1.8% were positive on HBS and HCV. The result of evaluating the relationship between QOL and biochemical indicators revealed that there was no significant different risk of people with abnormal reports of biochemical tests by changing WHOQOL-BREF scores.
10. Among the six groups of 1593 infants in the study, the prevalence rate of low-birth weight was between 6.9%- 11.0% and the sexual ratio near to one. The major parity of infants was below two and the most fetal number was one. There was about 10%
mother smoking during pregnancy, and the mean BMI and accouchement age of the mothers of 1593 subjects was 22.54 ±3.78 and 28.83 ± 5.38.
11. After adjusting risk factor including exposing earthquake or not, fetal gender, parity, mother’s accouchement age smoking condition and BMI, we found that there was no statistical significant between earthquake experience and low-birth weight. To summarize, our study showed that the 921 earthquake caused the short term health effects including the increments in the incidence rate of ischemic heart disease and diabetes, and worsen the ischemic heart disease, diabetes and respiratory disease, increasing the clinic visits. In the long term effects of earthquake, it continued affecting the patients with ischemic heart disease and diabetes, causing high clinic visits after three years letter of earthquake. Furthermore, general residents’ risk of chronic respiratory, ischemic heart disease and essential hypertension were higher then public employee in half-year of post-earthquake, half to one year and one to one and half-year. The risk of ischemic heart disease, cerebrovascular disease, chronic respiratory tract disease, diabetes and arthropathy were affected by mental health score. In the part of quality of life among public employee, we found that the manpower and sources supplied by government or non-governmental circles truly improved the quality of life of public employee. Besides, according to survey of health situation, the residents with completely or partially collapsed house-damage had worse health situation then housing or general population, and they had higher frequency of unhealthy behaviors then other two populations, such as smoking, drinking or betelquids. However, we couldn’t find that there was any relationship between abnormal reports of biochemical tests and WHOQOL=BREF scores. As regards if earthquake experience contributed to the low-birth weight, the result of our study showed that earthquake was not statistically significant in low-birth weight after
adjusting other risk factor of low-birth weight. Therefore, there are some suggestions as below:
1. It is necessary to continue tracing and monitoring the patients with diabetes and ischemic heart disease to identify the long term effects toward this population.
2. In consideration of lower risk of Ischemic heart disease, essential hypertension and chronic respiratory tract disease among public employee, stable employment and income are important factors toward the chronic disease prevalence and need to be provided to the victims.
3. The risk of suffering chronic disease could be decreased by providing the program about improving the mental health.
4. In order to improve the quality of life among the residents with completely or partially collapsed house-damage, there should provide more financial supplements. 5. To improve the health situation of the population with heavy damage, there must be more comprehensive program about medical treatment and health promotion.
Reference
1. Trevisan M, Jossa F, Farinaro E, Krogh V, Panico S, Giumetti D, Mancini M. Earthquake and coronary heart disease risk factors: A longitudinal study. Am J of Epidemiol 1992; 135: 632-637.
2. Trevisan M, O'Leary E, Farinaro E, Jossa F, Galasso R, Celentano E, Scottoni A, Fusco G, Panico S. Short- and long-term association between uric acid and a natural disaster. Psychosom Med 1997; 59: 109-113.
3. Armenian HK, Melkonian AK, Hovanesian AP. Long term mortality and morbidity related to degree of damage following the 1988 earthquake in Armenia. Am J of Epidemiol 1998; 148: 1077-1084.
4. Bland SH, Farinaro E, Krogh V, Jossa F, Scottoni A, Trevisan M. Long term relations between earthquake experiences and coronary heart disease risk factors. Am J Epidemiol 2000; 151: 1086-1090.
5. Leor J, Poole K, Kloner RA. Sudden cardiac death triggered by an earthquake. N Engl J Med 1996; 334: 413-419.
6. Goenjian AK, Najarian LM, Pynoos RS, Steinberg AM, Manoukian G, Tavosian A, Fairbanks LA. Posttraumatic stress disorder in elderly and younger adults after the 1988 earthquake in Armenia. Am J Psychiatr 1994; 151: 895-901.
7. Carr VJ, Lewin TJ, Webster RA, Hazell PL, Kenardy JA, Carter GL. Psychosocial sequelae of the 1989 Newcastle earthquake: I. Community disaster experiences and psychological morbidity 6 months post-disaster. Psychol Med 1995; 25: 539-555.
8. Sharan P, Chaudhary G, Kavathekar SA, Saxena S. Preliminary report of psychiatric disorders in survivors of a severe earthquake. Am J Psychiatr 1996; 153: 556-558.
9. Bland SH, O'Leary ES, Farinaro E, Jossa F, Krogh V, Violanti JM, Trevisan M. Social network disturbances and psychological distress following earthquake evacuation. J of Nerv Ment Dis 1997; 185: 188-194.
10. Armenian HK, Morikawa M, Melkonian AK, Hovanesian AP, Haroutunian N, Saigh PA, Akiskal K, Akiskal HS. Loss as a determinant of PTSD in a cohort of adult survivors of the 1988 earthquake in Armenia: implications for policy. Acta Psychiatr Scand 2000; 102: 58-64.
11. Inui A, Kitaoka H, Majima M, Takamiya S, Uemoto M, Yonenaga C, Honda M, Shirakawa K, Ueno N, Amano K, Morita S, Kawara A, Yokono K, Kasuga M, Taniguchi H. Effect of the Kobe earthquake on stress and glycemic control in patients with diabetes mellitus. Arch Intern Med 1998; 158: 274-277.
12. Freedy JR, Saladin ME, Kilpatrick DG, Resnick HS, Saunders BE. Understanding acute psychological distress following natural disaster. J Trauma Stress 1994; 7: 257-273.
13. Murphy SA. Status of natural disaster victims' health and recovery 1 and 3 years later. Res Nurs Health 1986; 9: 331-340.
14. Lima BR, Pai S, Toledo V, Caris L, Haro JM, Lozano J, et al. Emotional distress in disaster victims: a follow-up study. J Nerv Ment Dis 1993; 181: 388-393. 15. Warheit GJ, Zimmerman RS, Khoury EL, Vega WA, Gil AG. Disaster related
stresses, depressive signs and symptoms, and suicidal ideation among a multi-racial/ ethnic sample of adolescents: a longitudinal analysis. J Child Psychol Psychiatry 1996; 37: 435-444.
16. Logue JN, Melick ME, Hansen H. Research issues and directions in the epidemiology of health effects of disasters. Epidemiol Rev 1981; 3: 140-162. 17. Center for Mental Health Services. Disaster response recovery: a handbook for
mental health professionals. Rockville, Md.: Substance Abuse and Mental Health Services Administration 1994: 2-3.
18. Chen CC, Yeh TL, Yang YK, Chen SJ, Lee IH, Fu LS, Yeh CY, Hsu HC, Tsai WL, Cheng LY, Si TC. Psychiatric morbidity and post-traumatic symptoms among survivors in the early stage following the 1999 earthquake in Taiwan. Psychiatry Research 2001; 105: 13-22.
19. Wang X, Gao L, Shinfuku N, Zhang H, Zhao C, Zhen Y. Longitudinal study of earthquake-related PTSD in a randomly selected community in north China. Psychatry 2000; 157:1260-1266.
20. Wang X, Gao L, Zhang H, Zhao C, Zhen Y, Shinfuku N. Post-earthquake quality of life psychological well-being: Longitudinal evaluation in a rural community sample in northern China. Psychatry and Clinical Neurosciences 2000;
54:427-433.
21. 台灣版世界衛生組織生活品質問卷發展小組:台灣版世界衛生組織生活 品質問卷之發展及使用手冊(第一版)。1999。
22. Lin MR, Huang W, Huang C, Hwang HF, Tsai LW. The impact of the
Chi-Chi earthquake on quality of life among elderly survivors in Taiwan – A before and after study. Quality of Life Research 2002; 11:379-388.
23. Trevisan m, Jossa F, Farinaro E, et al. Earthquake and coronary heart disease risk factors: A longitudinal study. American Journal of Epidemiology 1992;
135:632-637.
24. Bland SH, Farinaro E, Krogh V, Jossa F, Scottoni A, Trevisan M. Long term relations between earthquake experiences and coronary heart disease risk factors.
American Journal of Epidemiology 2000;151:1086-1090.
25. Trevisan M, O’Leary E, Farinaro, et al. Short- and long-term association between uric acid and a natural disaster. Psychosomatic Medicine 1997;59:109-113.
26. Armenian HK, Melkonian A, Hovanesian AP. Long term mortality and morbidity related to degree of damage following the 1988 earthquake in Armenia.
American Journal of Epidemiology 1998;148:1077-1084.
27. Austin MP, Leader L. Maternal Stress and obstetric and infant outcomes: epidemiological findings and neuroendocrine mechanisms. Australian & New Zealand Journal of Obstetrics & Gynaecology 2000; 40:331-337. 28. Chang HL. Chang TC. Lin TY. Kuo SS. Psychiatric morbidity and
pregnancy outcome in a disaster area of Taiwan 921 earthquake. [Journal Article] Psychiatry & Clinical Neurosciences 2002; 56(2):139-44.
29. 黃昌鼎:一、九二一地震與懷孕結果相關性之探討。二、台灣地區死產 危險因子分析,台灣大學公共衛生學院職業醫學與工業衛生研究所碩士 論文。2003。
30. Kramer MS. Determinants of low birth weight: methodological assessment and meta-analysis. [Review] [286 refs] Bulletin of the World Health Organization 1987; 65(5):663-737
31. King EH. Logsdon DA. Schroeder SR. Risk factors for developmental delay among infants and toddlers. Children's Health Care 1992; 21(1):39-52.
32. Chong MY, Wilkinson G.. Validation of 30- and 12-item versions of the Chinese Health Questionnaire (CHQ) in patients admitted for general health screening. Psychol Med 1989; 19: 495-505.
33. Lee CS, Yang YC. Screening for Psychiatric Morbidity Using Chinese Health Questionnaire. Taiwanese J Psychiatry 1997; 11: 368-377.
34. Cheng TA, Wu JT, Chong MY, Williams P. Internal consistency and factor structure of the Chinese Health Questionnaire. Acta Psychiatr Scand 1990; 82: 304-308.
35. Cheng TA, Williams P. The design and development of a screening questionnaire (CHQ) for use in community studies of mental disorders in Taiwan. Psychol Med 1986; 16: 415-422.
36. Meltzer-Brody S, Churchill E, Davidson JR. Derivation of the SPAN, a brief diagnostic screening test for post-traumatic stress disorder. Psychiatry Res. 1999 Oct 18;88(1):63-70.