Association between Serum Levels of Thyroid Measures and the Acrylamide Metabolite N-Acetyl-S-(propionamide)-cysteine in Adolescents and Young Adults
Chien-Yu Lin,1,2Yu-Chuan Chen,3 Guang-Wen Lien,3 Lain-Yu Lin,4Li-Li Wen, 5 Chien-Chang Liao,6, Kuo-Liong Chien,7 Fung-Chang Sung,8 Pau-Chung Chen,3,9,10 ** and Ta-Chen Su4 *
1Department of Internal Medicine, En Chu Kong Hospital, New Taipei City 237, Taiwan
2School of Medicine, Fu Jen Catholic University, New Taipei City 242, Taiwan 3Institute of Occupational Medicine and Industrial Hygiene, College of Public Health,
National Taiwan University, Taipei 10002, Taiwan
4Department of Internal Medicine and Cardiovascular Center, National Taiwan University Hospital, Taipei 10002, Taiwan
5Department of Clinical Laboratory, En Chu Kong Hospital, New Taipei City 237, Taiwan
6Health Policy Research Center, Taipei Medical University, Taipei, Taiwan 7Institute of Epidemiology and Preventive Medicine, College of Public Health,
National Taiwan University, Taipei 10002, Taiwan
8Institute of Environmental Health, College of Public Health, China Medical University, Taichung 404, Taiwan
9Department of Public Health, College of Public Health, National Taiwan University, Taipei 10002, Taiwan.
10Department of Environmental and Occupational Medicine, National Taiwan
University College of Medicine and National Taiwan University Hospital, Taipei 10002, Taiwan
*Corresponding author: Ta-Chen Su, MD, PhD
Department of Internal Medicine and Cardiovascular Center, National Taiwan University Hospital, Taipei 10002, Taiwan
Telephone: +886-2-23123456 ext 66719, Fax: +886-2-23712361 Email: [email protected] **Co-corresponding author: Pau-Chung Chen, MD, PhD Telephone: +886-2-3322-8088, Fax: +886-2-358-2402 Email: [email protected]
Abstract
Acrylamide is present in mainstream cigarette smoke and in some foods prepared at high temperatures. Animal studies have shown that acrylamide exposure altered thyroid function; however, it is not known if this also occurs in humans. We recruited 793 subjects (mean age, 21.3 years, range, 12–30 years) from a population-based sample of Taiwanese adolescents and young adults to determine if urinary levels of the acrylamide metabolite N-acetyl-S-(propionamide)-cysteine (AAMA) and the 6 serum thyroid measures are associated. The mean (SD) AAMA were 76.54 (76.42) µg/L. In linear regression analyses, a 1-unit increase in natural log AAMA was significantly associated with a decrease in serum free thyroxine (T4) (ng/dL) (β = -0.041, SE = 0.013, p = 0.001) after controlling for covariates. Subpopulation analyses showed AAMA and free T4 were significantly associated with females, age 20–30 years, body mass index < 24, non-current smokers, and subjects without alcohol consumption. In conclusion, higher urinary AAMA concentrations were associated with decreased levels of free T4 in this cohort. Further studies are warranted to determine if there is a causal relationship between acrylamide exposure and thyroid function test.
Key words: Acrylamide; N-Acetyl-S-(propionamide)-cysteine (AAMA); thyroid function; free thyroxine
List of abbreviations
AAMA: N-acetyl-S-(2-carbamoylethyl)-cysteine BMI: Body mass index
LOD: Limit of detection
NTUH: National Taiwan University Hospital NTD: New Taiwan Dollars
Introduction
Since the 1970s, acrylamide has been used as industrial material for the production of polyacrylamide which is widely used to synthesize polymers for industrial applications such as soil conditioning, wastewater treatment, research applications, cosmetic, papers and textile industries (1). Besides the industrial and laboratory uses, acrylamide may be absorbed from mainstream cigarette smoke, where it is present at concentrations of 1.1–2.34 μg per cigarette (2). A 2002 study reported that acrylamide was also present in foods processed at high temperatures (above 120°C) (3). In the case of high-temperature processed carbohydrate-rich foods, the formation of acrylamide in the diet is associated with high-temperature cooking processes for certain carbohydrate-rich foods, especially when asparagine reacts with sugars (4-6). These findings attracted worldwide interest because Acrylamide is probably carcinogenic to humans by the International Agency on Research of Cancer (7). In 2002, the World Health Organization reported an average dietary intake of acrylamide of 0.3–0.8 μg/kg BW/day, based on data from multiple studies (8). It is reported that exposure to acrylamide at 200 μg /kg bw/day places humans at risk for neurotoxicity, while 300 μg /kg bw/day puts humans at carcinogenic risk (9, 10).
In humans, acrylamide is detoxified by phase I and phase II metabolic pathways. In the phase I pathway, the cytochrome P450 enzyme CYP2E1 transforms acrylamide
to the epoxy derivative glycidamide (11). In the phase II pathway, the major route of metabolism, acrylamide is conjugated with glutathione to form mercapturic acids (12, 13), and N-acetyl-S-(2-carbamoylethyl)-cysteine (AAMA) is the major mercapturic acid in urine. In one study, 51.7% of the total acrylamide dose was recovered as urinary AAMA within 46 h of exposure, and AAMA was shown to have a half-life of 11 h (14). AAMA has also been proposed to be a non-invasive biomarker for
acrylamide exposure (11, 15-17).
The biological consequences of acrylamide exposure have chiefly centered on neurotoxicity ever since this effect was observed in humans occupationally exposed to this compound. Subsequently, experimental exposure of rodents to acrylamide has also revealed developmental, reproductive toxicity, genotoxicity and carcinogenicity (18). Acrylamide carcinogenicity studies in rats have reported increases in combined benign and malignant tumors of the thyroid, mammary tissues, and tunica vaginalis of the testis, as well as sporadic findings of other tumors.(10, 19). Recently, it was suggested that these tumors may be caused, at least in part, by effects of acrylamide on hormones (20, 21). Although acrylamide can cause genotoxic damage in vitro and in vivo (18, 22), there are indications that genotoxicity alone cannot explain the specific tumor patterns seen in rats (20, 21, 23).
formation of thyroid tumors in male and female F344 rats are alteration of a signal transduction pathway, leading to persistent stimulation of cell proliferation in thyroid follicular cells and eventual progression to follicular cell adenomas. The results of longer-term acrylamide administration appear to be a prolonged and modest disruption in thyroid–pituitary homeostasis, although the evidence is not consistent (24-26).
In humans, 3 prospective epidemiologic studies demonstrated a positive association between dietary acrylamide exposure and risk of cancer. Positive associations were observed for endometrial, ovarian (27), and renal cell (28) cancer and for postmenopausal estrogen-receptor-positive breast cancer (29). However, the information about the association between dietary acrylamide and the risk of thyroid cancer in humans is limited. In occupational studies, nonstatistically significant increased risks have been observed for occupational exposure to acrylamide (30, 31) , but the number of cases was small. Dietary acrylamide intake and the risk of head-neck and thyroid cancers had been evaluated in one prospective study. The authors did not observe a positive association between dietary acrylamide intake and the risk of thyroid cancers (32). However, there is no previous study investigate about how acrylamide might exert its effect on thyroid hormone levels in humans.
etiology of thyroid tumor and alter thyroid hormone homeostasis in animal studies. To investigate whether acrylamide may impact circulating levels of thyroid hormones in humans, we designed a cross-sectional study in Taiwanese adolescents and young adults based on a nationwide mass urine-screening program. We measured urinary AAMA as a marker of acrylamide exposure and 6 thyroid function tests as markers of thyroid function.
Material and methods
Study population and data collection
The study population was composed of students who participated in the 1992–2000 mass urine-screening program in Taiwan (33). Detailed information on the study subjects has been published elsewhere (34-36). For the current study, we selected 878 subjects who lived in the Taipei area and whose urine samples were available for further analysis. The subjects were interviewed and given cardiovascular health check-ups at the National Taiwan University Hospital (NTUH) between 2006 and 2008. The study was approved by the Research Ethics Committee, NTUH. Written informed consent was obtained from each participant or from the parents of children and adolescents when they enrolled in the follow-up study. Of the 878 subjects, 78 subjects were eliminated whose urine creatinine levels were below 0.3 g/L or above 3 g/L, which are the World Health Organization recommended guidelines for
acceptable variability of creatinine levels in urine specimens (37).Individuals with a reported history of thyroid disease were excluded to avoid the influence of medications on thyroid measure (n = 7). Finally, 793 participants were enrolled in the study.
Measurement of urinary AAMA
procedure modified from Huang et al (13). Briefly, 70 µL of 400 ng/mL N-acetyl-S-(2-carbamoylethyl-d4)-L-cysteine in acetonitrile (C/D/N Isotopes Inc, Pointe-Claire,
Quebec, Canada) was added to 70 µL of the urine sample in a polypropylene
centrifuge tube and vortexed for 30 s. The sample was then centrifuged at 14,000 rpm (14,462 × g) for 5 min in a benchtop centrifuge (Beckman Microfuge 16, Fullerton, CA, USA). An aliquot (70 µL) of the supernatant was transferred to a fresh tube, mixed with 70 µL of Milli-Q water (Billerica, MA, USA), vortexed for 30 s, and centrifuged as above. The supernatant (∼120 µL) was removed and filtered through a 0.22-µm PVDF syringe filter into a 2.0-mL autosampler vial. Ten calibration standard solutions (between 0.5 and 1000 ng/mL) were prepared in 70 µL of artificial urine (Ward’s Natural Science, Rochester, NY, USA) and subjected to the same sample preparation procedure.
The separation and detection of AAMA was performed on a Waters ACQUITY UHPLC system (Waters Corporation, Milford, MA, USA) coupled with a Waters Quattro Premier XE triple-quadrupole mass spectrometer. The instrument was operated in multiple reaction monitoring (MRM) mode with negative electrospray ionization. The following transitions were monitored: AAMA 232.8→104 and 58.1, and d4-AAMA 237.1→108. Samples were injected in 4 μL onto an ACQUITY UHPLC BEH HILIC column (2.1 mm × 50 mm, 1.7 µm) maintained at 25°C. The
mobile phase consisted of 0.1% formic acid (pH = 3.6) and acetonitrile (LC/MS grade; J.T. Baker), and separation was achieved with the following conditions: hold at 99% acetonitrile for 1.0 min, decrease to 70% acetonitrile over 0.2 min, hold at 70% acetonitrile for 2.0 min, and return to 99% acetonitrile over 0.1 min. The total run time was 3.3 min and the flow rate was maintained constantly at 0.5 mL/min through the run. The recoveries of sample preparations of AAMA spiked three different levels (5, 100, and 1000 µg/L) into artificial urine ranged between 85.0 to 93.2% with relative standard deviations between 4.6 and 11.7%. Intra- and inter-day calibration bias was less than 22.5% and intra- and inter-day calibration of relative standard deviations were within 1.55-15.4% for all the concentrations. The limit of detection (LOD) for AAMA was 0.33 ng/mL and 97.9 % of urine samples were at or above the LOD. For concentrations below the detection limits, a value of half the LOD was used.
Serum thyroid measures
The thyroid panel, including measures of free and total triiodothyronine (T3) and thyroxine (T4), thyroid stimulating hormone (TSH), and thyroxine-binding globulin (TBG), was measured in serum and analyzed using various immunoenzymatic assays. The normal range of thyroid measures are as follows: TSH: 0.4-4.0 μIU/mL; free T4:
0.89-1.76 ng/dL; total T4: 4.5-12.5 μg/dL; free T3: 1.8-4.2 pg/mL; total T3: 84-172 ng/dL; TBG: 14-31 μg/mL. Subclinical hyperthyroidism was defined as TSH < 0.4 μIU/mL while subclinical hypothyroidism was defined as TSH > 4.0 mIU/L. We used subclinical hypo and hyperthyroidism since participants with a reported history of thyroid disease were excluded from the study.
Covariate
We considered age, gender, alcohol consumption, smoking status as potential confounders of thyroid function. Sociodemographic information such as age, gender was recorded during the interview. Alcohol intake was determined using a
questionnaire and categorized as current alcohol consumers or non-consumers. Smoking status was subdivided into non-current smoker, <10 cigarettes/day, 10–19 cigarettes/day, and ≥20 cigarettes/day. Hypo- and hyperthyroidism can affect blood pressure (38, 39) and thyroid function may influence BMI and glucose homeostasis (40). We assumed that BMI, glucose, and blood pressure are not confounders and adjusting for these covariates may result in over-adjustment.
Statistical analysis
SPSS for Windows (version 16.0; SPSS Inc., Chicago, IL) was used for all statistical analyses. Urinary AAMA concentrations were corrected for urine creatinine
and expressed as µg/g creatinine. The concentration of AAMA was described by exponential mean and SD calculated from natural log AAMA in different subgroups and tested by Student’s two-tailed t-test and one-way analysis of variance (ANOVA). Analysis of covariance (ANCOVA) was used to examine the AAMA levels in
different subgroups after adjusting for gender and age. The association between AAMA and thyroid measures was tested using linear regression models. Potential confounders were adjusted in the models: model 1 was adjusted for age and gender, and model 2 was adjusted for age, gender, smoking and drinking status. To be considered significant, an association was required to achieve statistical significance in both models. Due to significant deviation from the normal distribution, the natural log-transformation was performed for TSH. To evaluate dose response effects across the population, the AAMA were also stratified across the population in tertiles in linear regression models. In logistic regression, we used the model 2 as confounders to test exposures to AAMA related to the odds ratio of subclinical hyperthyroid (TSH below normal range) and subclinical hypothyroid (TSH above normal range). For further investigation of AAMA and free T4 associations in the total subject population and in subpopulations, multiple linear regression analyses of free T4 with a unit increase in natural log AAMA were performed. The potential confounders adjusted in the model were gender, age, smoking and drinking status. All tests were two-sided,
and statistical significance was defined as P < 0.05.
Results
The study sample consisted of 297 males and 496 females. The mean age (range) was 21.3 (12–30) years. The mean (SD) AAMA before and after corrected for urine creatinine were 76.54 (76.42) µg/L and 52.78 (53.18) µg/g creatinine, respectively. The basic demographics of the sample population are provided in Table 1. The mean AAMA levels were not different between age, gender, household income, or BMI. AAMA levels were higher in the active smokers.
A summary of the association between the natural log AAMA and thyroid measures after adjustment in the 2 models is given in Table 2. A 1-unit increase in natural log AAMA was significantly associated with a decrease in serum free T4 concentration in both models (β = -0.041, SE = 0.013, p = 0.001 in the final model). There was no association between mean AAMA levels and other thyroid measures. The association between tertiles of urine concentrations of AAMA and free T4 after adjusting for other potential covariates is listed in Table 3. When AAMA was entered into the full regression models (controlling age, gender, smoking and drinking status), free T4 decreased significantly with increasing levels of AMMA (P for trend 0.027).
Among the 793 (496 females, 297 males) study subjects, 33 (29 women, 4 men) were subclinical hypothyroid (TSH above normal range) and 19 (13 women, 6 men) were
subclinical hyperthyroid (TSH below normal range). Associations between thyroid diseases and unit increases in natural log-transformed AAMA in logistic regression models are shown in Table 4. No differences were found between exposure to acrylamide and the odds ratio of being subclinical hypothyroid/hyperthyroid in logistic regression.
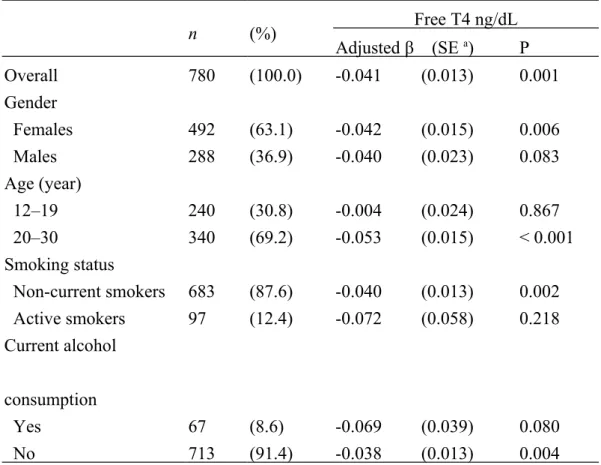
Table 5 shows multiple linear regression coefficients (SE) of free T4 with a 1-unit increase in natural log AAMA, for the total study population and different subpopulations. After controlling for potential confounders (gender, age, smoking, and drinking status), the association between free T4 and AAMA was significant in the following groups: females, age 20–30 years, BMI <24 kg/m2, non-current
smokers, and subjects who did not consume alcohol.
Discussion
In this cross-sectional study, we found that urinary AAMA concentration was negatively associated with free T4 in a Taiwanese population of adolescents and young adults. Since urinary AAMA has been served as a biomarker of acrylamide exposures for the general populations from tobacco smoke or the consumption of high-temperature processed foods (11, 15-17) and there is no other chemical or protein can release AAMA through urine, we suggest that daily low-dose acrylamide exposure might be associated with decreased free T4 in this study population. To our knowledge, this is the first report to link urine acrylamide metabolite and thyroid
measures in humans. In this study, urinary AAMA concentrations were slightly higher than those previously found in studies of different age groups, even though the
fraction of smokers was not higher (11, 16, 17, 41, 42). This may have been due to greater consumption of acrylamide-rich foods; however, we did not obtain
information on the food consumption in this study.
There has been a great deal of progress in the last few years in understanding the toxicology and distribution of acrylamide in animals and in humans. However, the effects of acrylamide on thyroid homeostasis were only mentioned in animal studies. In rats, both of the available chronic oral exposure studies for acrylamide reported statistically significant increased incidences of thyroid follicular cell adenomas, or combined adenomas and carcinomas, at the highest dose levels of 2–3 mg/kg-day (10, 19). Chemicals that alter thyroid hormone synthesis or metabolism leading to a decrease in thyroid hormone levels and a rise in TSH from the pituitary which may induce thyroid follicular cell hyperplasia that may progress to neoplasia (43). These findings have led to several investigations of effects of acrylamide on hypothalamus-pituitary-thyroid axis endpoints. One study found exposure of female F344 rats to 2 or 15 mg/kg-day for 2 or 7 days decreased thyroid colloid and increased follicular cell height. Both of these changes indicate release of thyroid hormones, which appears to occur at 7 days (26). In an unpublished study, male or female F344 rats were exposed
to acrylamide in drinking water for 14 or 28 days at dose levels ranging from about 1 to 25 mg/kg-day. A significant decrease in T3 and T4 in high dose males is reported with a nonsignificant increase in TSH at 28 days (25). Another study examined a number of endpoints indicative of disruption of the hypothalamus-pituitary-thyroid axis in male F344 rats (70 days of age) exposed for 14 days to acrylamide in drinking water delivering nominal doses of 0, 2.5, 10, or 50 mg/kg-day acrylamide exposure caused a significant decrease in serum T4 only at the high dose, but had no effect on serum T3or TSH (24). Thus, the results of longer-term acrylamide administration appear to be a prolonged and modest disruption in thyroid–pituitary homeostasis.
However, these animal studies were carried out with acrylamide doses several fold higher than human dietary doses, which make extrapolation to human dietary doses problematic. In addition, other differences need to be considered when
analyzing thyroid functions in humans and rodents. The first difference is the lack of thyroid-binding globulin in rodents. The second difference is that the half -life for the thyroid hormone, T4 is shorter in rodents than in humans (12 h versus 5–9 days), and TSH levels are 25 times higher in rodents than humans. This makes care must be taken in any extrapolation from these rodents (44).
In our study, we found decreased serum free T4 without the concomitant increase in TSH that would be expected through feedback stimulation. One possible
explanation is thyroid resistance, a syndrome of reduced end-organ responsiveness to thyroid hormone. The common causes of the syndrome including mutations of the β form of the thyroid hormone receptor, thyroid hormone cell transporter defect and thyroid hormone metabolism defect (45). However, it is not clear acrylamide may interfere in which step of hypothalmic-pituitary-thyroid axis. The possible site of action for acrylamide may be in the liver with an enhanced catabolism of thyroid hormone. Some minimal evidence exists that an increased catabolism of thyroid hormones might be occurring in the liver (9). Second, acrylamide is known to interfere with microtubule function. Thus, a possibility exists that acrylamide in the thyroid may lead to the loss of integrity of microfilaments and microtubules in thyroid follicular development (20). Third, acrylamide might affect thyroid responses via perturbation of endocrine signaling as a secondary consequence of neurotoxicity or altered neurotransmitter levels in the hypothalamus. This hypothesis was directly tested by one study as described above and found that gene expression or
neurotransmitter changes in the hypothalamus did not suggest any related activity, but that gene expression changes in the pituitary and thyroid might be related (24). Although acrylamide is a known neurotoxicant, sufficient data on its specific toxicity to the hypothalamus are not available.
to 2nd and 3rd tertiles. However, the pairwise comparisons between 2nd and 3rd tertiles were insignificant. The non-monotonic relation is a common finding for other endocrine-active chemicals (46), for which high doses inhibit the low-dose response system while initiating a wide array of other adverse effects via different response mechanisms (47). The possible explanation is that the dose–response effects of acrylamide on FT4 may not be a linear relationship in humans. Acrylamide exerts the maximal effects at a low dose already and no further consistent or potentially relevant clinical changes occur at an even higher level.
Neither the extent of interindividual variability in acrylamide metabolism nor human variability in response to acrylamide has been well characterized. Factors that could contribute to a range of human response to acrylamide include variations in cytochrome P450, epoxide hydrolase, or glutathione transferase activity or due to other factors including exposure to other chemicals that induce or inhibit enzyme levels, nutritional status, alcohol consumption, or the presence of underlying disease that could alter metabolism of acrylamide or antioxidant protection systems (20). In our study, the association between AAMA and free T4 was more evident in female subjects and age group 20-30, but there was no significant difference in urinary AAMA concentrations between these groups. No data are available regarding gender and age-related differences in sensitivity to acrylamide in humans. However, we can’t
conclude the association between AAMA and free T4 in female subjects because the study group of male gender is smaller and the P value is borderline (p=0.08). The association between AAMA and free T4 is evident in young adults but the
mechanisms are not known.
We also found an association between AAMA and free T4 in non-current smokers, and subjects who did not consume alcohol, despite the higher concentration of AAMA in the active smoker group. Light to moderate alcohol consumption was found to be a significant predictor of thyroid volume enlargement and was a significant predictor of low FT4 (48). This may result from either damage to the thyroid gland or changes in the HPT axis at the pituitary level caused by chronic drinking (49). Cigarette smoke contains chemicals that are thought to influence thyroid functions, leading to abnormalities of the thyroid gland. Smokers face an increased risk of Graves' disease, and other thyroid-related problems. The longer a person has smoked, the greater the risk for thyroid disease (50). It is possible that acrylamide exposure may have a lesser effect on thyroid than does tobacco smoke, and alcohol intake, although the trends within these subpopulations were too small to be statistically significant. Alternatively, it is possible that the association between acrylamide, tobacco smoke, and alcohol is due to an opposite synergistic effect.
not permit causal inference. Second, we didn’t have acrylamide exposure data in this study. Third, when foods are heat processed, the sugars and lipids react with the proteins they contain via the Maillard and related reactions to form a wide range of products. Reaction products include advanced glycation/lipoxidation endproducts, acrylamide and heterocyclic amines, all of which may impact on human health and disease. Furthermore, some Maillard reaction products affect the growth of colonic bacteria and thermally-induced modification of dietary protein can affect allergenicity (51). A correlation between two measured parameters doesn't necessary mean that a found association means that the other parameter is causative. Fourth, our study population was composed of adolescents and young adults, and therefore, we cannot infer that the same associations will hold in older adults. Fifth, we did not obtain information about amino acid intake, which is known to affect glutathione homeostasis and may be relevant to detoxification (52). Finally, a common
physiology could influence urinary AAMA levels and 8-OHdG, rather than exposure affecting outcome.
Conclusion
In this cross-sectional study, we present the first report of a relationship between urine acrylamide metabolite and serum free T4 in a Taiwanese population of
smoking has become a worldwide concern, further longitudinal clinical and in vitro studies are urgently warranted to elucidate the putative causal relationship.
Acknowledgments
This study was supported by grants from National Health Research Institute of Taiwan (NHRI-EX97-9721PC~10021PC and NHRI-EX95-9531PI~9731PI) and from National Science Council of Taiwan (102-2314-B-385 -002). No funding organization or sponsor played any part in the design or conduct of the study; in the analysis or interpretation of the data; or in the preparation, review, or approval of the manuscript.
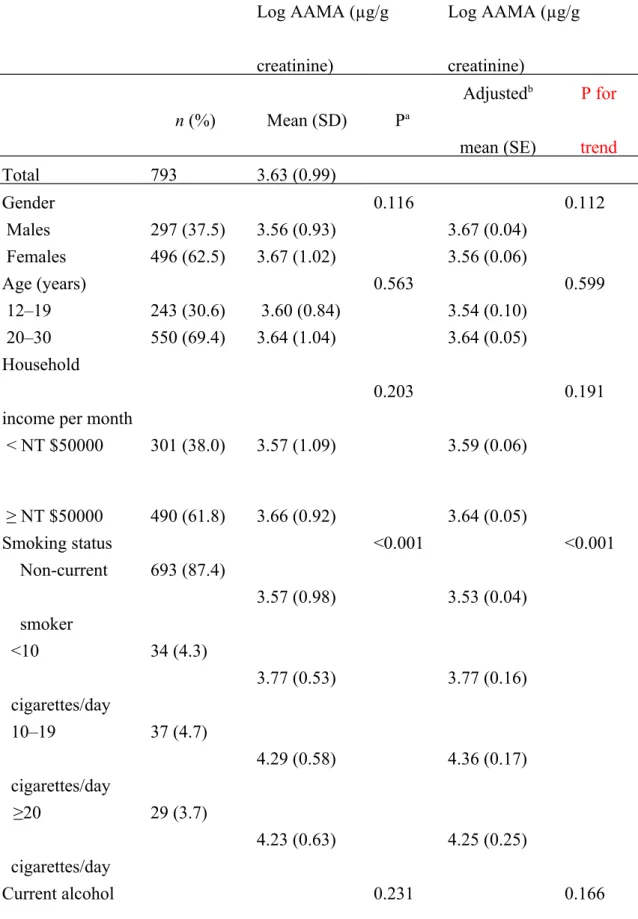
Table 1. Basic demographics of the sample subjects and log-transformed mean (SD) and gender- and age-adjusted mean (SE) urinary AAMA concentrations
Log AAMA (µg/g creatinine) Log AAMA (µg/g creatinine) n (%) Mean (SD) Pa Adjustedb mean (SE) P for trend Total 793 3.63 (0.99) Gender 0.116 0.112 Males 297 (37.5) 3.56 (0.93) 3.67 (0.04) Females 496 (62.5) 3.67 (1.02) 3.56 (0.06) Age (years) 0.563 0.599 12–19 243 (30.6) 3.60 (0.84) 3.54 (0.10) 20–30 550 (69.4) 3.64 (1.04) 3.64 (0.05) Household income per month
0.203 0.191 < NT $50000 301 (38.0) 3.57 (1.09) 3.59 (0.06) ≥ NT $50000 490 (61.8) 3.66 (0.92) 3.64 (0.05) Smoking status <0.001 <0.001 Non-current smoker 693 (87.4) 3.57 (0.98) 3.53 (0.04) <10 cigarettes/day 34 (4.3) 3.77 (0.53) 3.77 (0.16) 10–19 cigarettes/day 37 (4.7) 4.29 (0.58) 4.36 (0.17) ≥20 cigarettes/day 29 (3.7) 4.23 (0.63) 4.25 (0.25) Current alcohol 0.231 0.166
consumption Yes 69 (8.7) 3.76 (1.07) 3.72 (0.12) No 724 (91.3) 3.62 (0.98) 3.59 (0.04) BMI (kg/m2) 0.502 0.703 <24 618 (77.9) 3.64 (1.00) 3.62 (0.04) ≥24 175 (22.1) 3.58 (0.96) 3.59 (0.08)
a P values determined by t-test or ANOVA; b adjusted for gender and age AAMA: N-acetyl-S-(2-carbamoylethyl)-cysteine; BMI: body mass index
Table 2. Linear regression coefficients (standard error) of thyroid measures and 1-unit increase in natural log AAMA in different subpopulations
Model 1a Model 2b
Adjusted β (SEc) P Adjusted β (SEc) P
Total T4 μg/dL -0.070 (0.063) 0.272 -0.069 (0.065) 0.289 Free T4 ng/dL -0.038 (0.012) 0.002 -0.041 (0.013) 0.001 Total T3 ng/dL 0.204 (0.811) 0.802 0.202 (0.835) 0.809 Free T3 pg/mL -0.022 (0.027) 0.410 -0.034 (0.027) 0.217 Natural log TSH μIU/mL -0.048 (0.025) 0.062 -0.050 (0.042) 0.058 TBGμg/mL 0.073 (0.124) 0.557 0.046 (0.128) 0.717
a Model 1 was adjusted for gender and age; b model 2 was adjusted for gender, age, smoking and drinking status; c SE, standard error;
AAMA: N-acetyl-S-(2-carbamoylethyl)-cysteine; TBG: thyroxine-binding globulin *P<0.05 **P<0.01
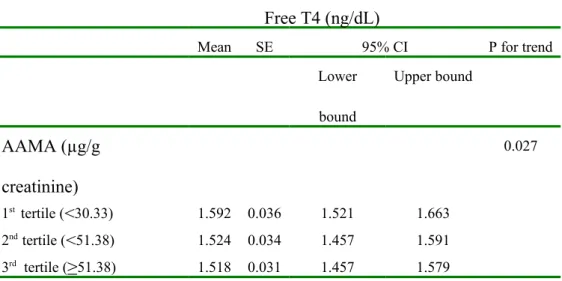
Table 3. Mean and Standard Error of free T4 (ng/dL) Across Tertiles of AAMA in Linear Regression Models.
Free T4 (ng/dL)
Mean SE 95% CI P for trend Lower bound Upper bound AAMA (µg/g creatinine) 0.027 1st tertile (<30.33) 1.592 0.036 1.521 1.663 2nd tertile (<51.38) 1.524 0.034 1.457 1.591 3rd tertile (≥51.38) 1.518 0.031 1.457 1.579
Adjusted for age, gender, smoking status and drinking status AAMA: N-acetyl-S-(2-carbamoylethyl)-cysteine
Table 4. Associations between subclinical thyroid diseases and unit increase in natural log-transformed AAMA in logistic regression models in different subpopulations.
Total Female Male
OR (95% CI) OR (95% CI) OR (95% CI) Subclinical hypothyroidism 0.90(0.64-1.26) 0.93 (0.63-1.37) 0.88(0.42-1.83) Subclinical hyperthyroidism 1.16(0.66-2.04) 1.19(0.63-2.23) 1.08(0.31-3.78) Adjusted for age, gender, smoking status and drinking status
Subclinical hyperthyroidism was defined as TSH < 0.4 mIU/L Subclinical hypothyroidism was defined as TSH > 4.0 mIU/L *P<0.05
Table 5. Linear regression coefficients between AAMA and free T4 in study subpopulations n (%) Free T4 ng/dL Adjusted β (SE a) P Overall 780 (100.0) -0.041 (0.013) 0.001 Gender Females 492 (63.1) -0.042 (0.015) 0.006 Males 288 (36.9) -0.040 (0.023) 0.083 Age (year) 12–19 240 (30.8) -0.004 (0.024) 0.867 20–30 340 (69.2) -0.053 (0.015) < 0.001 Smoking status Non-current smokers 683 (87.6) -0.040 (0.013) 0.002 Active smokers 97 (12.4) -0.072 (0.058) 0.218 Current alcohol consumption Yes 67 (8.6) -0.069 (0.039) 0.080 No 713 (91.4) -0.038 (0.013) 0.004
1. Kuklenyik Z, Needham LL, Calafat AM. Measurement of 18 perfluorinated organic acids and amides in human serum using on-line solid-phase extraction. Analytical chemistry 2005;77(18):6085-91.
2. Smith CJ, Perfetti TA, Rumple MA, et al. "IARC group 2A Carcinogens" reported in cigarette mainstream smoke. Food Chem Toxicol 2000;38(4):371-83.
3. Tareke E, Rydberg P, Karlsson P, et al. Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J Agric Food Chem 2002;50(17):4998-5006. 4. Mottram DS, Wedzicha BL, Dodson AT. Acrylamide is formed in the
Maillard reaction. Nature 2002;419(6906):448-9.
5. Sharp D. Acrylamide in food. Lancet 2003;361(9355):361-2.
6. Stadler RH, Blank I, Varga N, et al. Acrylamide from Maillard reaction products. Nature 2002;419(6906):449-50.
7. IARC monographs on the evaluation of the carcinogenic risk of chemicals to humans. Some industrial chemicals -acrylamide. 1994, (Cancer) IIAfRo 8. Consultation of the health implications of acrylamide in food. WHO (World
Health Organisation), 2002,
9. Burek JD, Albee RR, Beyer JE, et al. Subchronic toxicity of acrylamide administered to rats in the drinking water followed by up to 144 days of recovery. Journal of environmental pathology and toxicology 1980;4(5-6):157-82.
10. Friedman MA, Dulak LH, Stedham MA. A lifetime oncogenicity study in rats with acrylamide. Fundamental and applied toxicology : official journal of the Society of Toxicology 1995;27(1):95-105.
11. Boettcher MI, Schettgen T, Kutting B, et al. Mercapturic acids of acrylamide and glycidamide as biomarkers of the internal exposure to acrylamide in the general population. Mutat Res 2005;580(1-2):167-76.
12. Fennell TR, Sumner SC, Snyder RW, et al. Metabolism and hemoglobin adduct formation of acrylamide in humans. Toxicol Sci 2005;85(1):447-59. 13. Huang YF, Wu KY, Liou SH, et al. Biological monitoring for occupational
acrylamide exposure from acrylamide production workers. Int Arch Occup Environ Health 2011;84(3):303-13.
14. Hartmann EC, Boettcher MI, Bolt HM, et al. N-Acetyl-S-(1-carbamoyl-2-hydroxy-ethyl)-L-cysteine (iso-GAMA) a further product of human
metabolism of acrylamide: comparison with the simultaneously excreted other mercaptuic acids. Arch Toxicol 2009;83(7):731-4.
15. Huang CC, Li CM, Wu CF, et al. Analysis of urinary
exposure in smokers. Environ Res 2007;104(3):346-51.
16. Urban M, Kavvadias D, Riedel K, et al. Urinary mercapturic acids and a hemoglobin adduct for the dosimetry of acrylamide exposure in smokers and nonsmokers. Inhal Toxicol 2006;18(10):831-9.
17. Heudorf U, Hartmann E, Angerer J. Acrylamide in children--exposure assessment via urinary acrylamide metabolites as biomarkers. Int J Hyg Environ Health 2009;212(2):135-41.
18. Shipp A, Lawrence G, Gentry R, et al. Acrylamide: review of toxicity data and dose-response analyses for cancer and noncancer effects. Critical reviews in toxicology 2006;36(6-7):481-608.
19. Johnson KA, Gorzinski SJ, Bodner KM, et al. Chronic toxicity and oncogenicity study on acrylamide incorporated in the drinking water of Fischer 344 rats. Toxicology and applied pharmacology 1986;85(2):154-68. 20. Dourson M, Hertzberg R, Allen B, et al. Evidence-based dose-response
assessment for thyroid tumorigenesis from acrylamide. Regulatory toxicology and pharmacology : RTP 2008;52(3):264-89.
21. Haber LT, Maier A, Kroner OL, et al. Evaluation of human relevance and mode of action for tunica vaginalis mesotheliomas resulting from oral exposure to acrylamide. Regulatory toxicology and pharmacology : RTP 2009;53(2):134-49.
22. Besaratinia A, Pfeifer GP. A review of mechanisms of acrylamide carcinogenicity. Carcinogenesis 2007;28(3):519-28.
23. Segerback D, Calleman CJ, Schroeder JL, et al. Formation of N-7-(2-carbamoyl-2-hydroxyethyl)guanine in DNA of the mouse and the rat
following intraperitoneal administration of [14C]acrylamide. Carcinogenesis 1995;16(5):1161-5.
24. Bowyer JF, Latendresse JR, Delongchamp RR, et al. The effects of subchronic acrylamide exposure on gene expression, neurochemistry, hormones, and histopathology in the hypothalamus-pituitary-thyroid axis of male Fischer 344 rats. Toxicology and applied pharmacology 2008;230(2):208-15.
25. Friedman MAD, L. H.; Keefe, R. T. . Effect of acrylamide on rat hormone levels in a 28-day drinking water study 1999.
26. Khan MA, Davis CA, Foley GL, et al. Changes in thyroid gland morphology after acute acrylamide exposure. Toxicological sciences : an official journal of the Society of Toxicology 1999;47(2):151-7.
27. Hogervorst JG, Schouten LJ, Konings EJ, et al. A prospective study of dietary acrylamide intake and the risk of endometrial, ovarian, and breast cancer. Cancer epidemiology, biomarkers & prevention : a publication of the
American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 2007;16(11):2304-13.
28. Hogervorst JG, Schouten LJ, Konings EJ, et al. Dietary acrylamide intake and the risk of renal cell, bladder, and prostate cancer. The American journal of clinical nutrition 2008;87(5):1428-38.
29. Olesen PT, Olsen A, Frandsen H, et al. Acrylamide exposure and incidence of breast cancer among postmenopausal women in the Danish Diet, Cancer and Health Study. International journal of cancer Journal international du cancer 2008;122(9):2094-100.
30. Marsh GM, Youk AO, Buchanich JM, et al. Mortality patterns among workers exposed to acrylamide: updated follow up. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine 2007;49(1):82-95.
31. Swaen GM, Haidar S, Burns CJ, et al. Mortality study update of acrylamide workers. Occupational and environmental medicine 2007;64(6):396-401. 32. Schouten LJ, Hogervorst JG, Konings EJ, et al. Dietary acrylamide intake and
the risk of head-neck and thyroid cancers: results from the Netherlands Cohort Study. American journal of epidemiology 2009;170(7):873-84.
33. Wei JN, Sung FC, Lin CC, et al. National surveillance for type 2 diabetes mellitus in Taiwanese children. JAMA : the journal of the American Medical Association 2003;290(10):1345-50.
34. Lin CY, Wen LL, Lin LY, et al. Associations between Levels of Serum Perfluorinated Chemicals and Adiponectin in a Young Hypertension Cohort in Taiwan. Environ Sci Technol 2011.
35. Lin CY, Lin LY, Wen TW, et al. Association between levels of serum perfluorooctane sulfate and carotid artery intima-media thickness in adolescents and young adults. International journal of cardiology 2013. 36. Lin CY, Wen LL, Lin LY, et al. The associations between serum
perfluorinated chemicals and thyroid function in adolescents and young adults. Journal of hazardous materials 2013;244-245:637-44.
37. Biological Monitoring of Chemical Exposure in the Workplace. 1996, ((WHO) WHO
38. Prisant LM, Gujral JS, Mulloy AL. Hyperthyroidism: a secondary cause of isolated systolic hypertension. Journal of clinical hypertension 2006;8(8):596-9.
39. Luboshitzky R, Aviv A, Herer P, et al. Risk factors for cardiovascular disease in women with subclinical hypothyroidism. Thyroid : official journal of the American Thyroid Association 2002;12(5):421-5.
40. Knudsen N, Laurberg P, Rasmussen LB, et al. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. The Journal of clinical endocrinology and metabolism 2005;90(7):4019-24.
41. Bjellaas T, Janak K, Lundanes E, et al. Determination and quantification of urinary metabolites after dietary exposure to acrylamide. Xenobiotica 2005;35(10-11):1003-18.
42. Hartmann EC, Boettcher MI, Schettgen T, et al. Hemoglobin adducts and mercapturic acid excretion of acrylamide and glycidamide in one study population. J Agric Food Chem 2008;56(15):6061-8.
43. Williams ED. Mechanisms and pathogenesis of thyroid cancer in animals and man. Mutation research 1995;333(1-2):123-9.
44. Meek ME, Bucher JR, Cohen SM, et al. A framework for human relevance analysis of information on carcinogenic modes of action. Critical reviews in toxicology 2003;33(6):591-653.
45. Refetoff S, Dumitrescu AM. Syndromes of reduced sensitivity to thyroid hormone: genetic defects in hormone receptors, cell transporters and deiodination. Best Pract Res Clin Endocrinol Metab 2007;21(2):277-305. 46. vom Saal FS, Myers JP. Bisphenol A and risk of metabolic disorders. Jama
2008;300(11):1353-5.
47. Welshons WV, Nagel SC, vom Saal FS. Large effects from small exposures. III. Endocrine mechanisms mediating effects of bisphenol A at levels of human exposure. Endocrinology 2006;147(6 Suppl):S56-69.
48. Valeix P, Faure P, Bertrais S, et al. Effects of light to moderate alcohol consumption on thyroid volume and thyroid function. Clinical endocrinology 2008;68(6):988-95.
49. Leggio L, Ferrulli A, Cardone S, et al. Relationship between the
hypothalamic-pituitary-thyroid axis and alcohol craving in alcohol-dependent patients: a longitudinal study. Alcohol Clin Exp Res 2008;32(12):2047-53. 50. Utiger RD. Effects of smoking on thyroid function. European journal of
endocrinology / European Federation of Endocrine Societies 1998;138(4):368-9.
51. Jenny A. Dietary Maillard reaction products: implications for human health and disease. Czech Journal of Food Sciences 2009;27:S66-S9.
52. Wu G, Fang YZ, Yang S, et al. Glutathione metabolism and its implications for health. The Journal of nutrition 2004;134(3):489-92.