Page 1
Title: Can FESSCombined with Submucosal Resection (SMR)/Septoplasty Reduce Revision Rate?
Chan-Chi Chang, MD1,Chih-JaanTai, MD1,2, Teik-Ying Ng, MD1, Yung-An Tsou, MD1,2, Ming-Hsui Tsai, MD1,2
1Departments of Otolaryngology, China Medical University Hospital 2College of Medicine, China Medical University
Corresponding author: Chih-Jaan Tai
Department of Otolaryngology, China Medical University Hospital, Taichung, Taiwan No. 2 Yuh-Der Road, Taichung 404, Taiwan
Tel: 886-4-22052121 ext. 4436 Fax: 886-4-22034174 E-mail: [email protected] 1 1 2 3 4 5 6 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
ABSTRACT
Objectives: Our study was designed to ascertain the outcomes of FESS combined with SMR/septoplasty in reducing FESS revision rates.
Study Design: retrospective population-based study Setting: Academic tertiary medical center
Subjects and Methods: By using the Taiwan Longitudinal Health Insurance Database, we obtained the patients underwent FESS for chronic rhinosinusitis. These patients were divided into two groups: the control group (FESS alone) and the study group (FESS combined with SMR). The primary outcome was the revision operative rate.
Results: In total, 4,484 patients who had undergone FESS were recruited into this study. The number of patients who underwent revision FESS was 528 (11.78%). In our sample, 80.45% of patients received FESS alone, whereas 19.54% of the patients underwent concurrent SMR/septoplasty during FESS. There are more female patients and older patients in the control group than in the study group. The revision rates of these two groups were significantly different (12.36% vs 9.36%, respectively; p = 0.016). Moreover, logistic regression analysis came out that patients in the control group had a higher revision rates than those in the study group. Male patients and younger patients were found to have higher revision rates. In addition, patients with asthma or allergic rhinitis had higher revision rates compared with those patients without these two co-morbidities.
Conclusions: This study showed an association between FESS combined with concurrent SMR/septoplasty and less incidence of revision rate of FESS. Patients with asthma or allergic rhinitis have an increased risk of requiring more revision surgeries after FESS. 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
Page 3
Key words:revision FESS,septoplasty, SMR, deviated nasal septum, asthma, allergic rhinitis 7 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69
1. Introduction
Chronic rhinosinusitis (CRS) is a disease characterized by the inflammation of the paranasal sinus mucosa for a duration of at least 12 consecutive weeks.1 Data from the
2007 Medical Expenditure Panel Survey medical conditions file and linked to the consolidated expenditures file of the United States showed that CRS is one of the most frequently diagnosed chronic diseases, affecting 4.9% ± 0.2% of the population. Because of this high prevalence rate, the overall expenditure for CRS has been recognized as a socioeconomic burden in the United States. The estimated direct cost was $8.6 billion.2
Nasal obstruction is one of the most common reasons for nasal surgery. Deviated nasal septum is the most common cause of nasal obstruction.3 In England and Wales, over 23,500 people were
diagnosed with deviated nasal septum in 2008-2009.4,5 Septal surgery
is one of the most common procedures in ENT practice, with more than 20,000 submucosal resections (SMRs) and septoplasties performed in England and Wales in 2008-2009.6,7 However, the benefits of this form
of surgery have been questioned.8
Functional endoscopic sinus surgery (FESS) has been the most common surgery for rhinosinusitis for those with failed maximal medical treatments. Published success rates for FESS range from 76% to 98%.9 Common failure factors associated with FESS include
inappropriate surgical technique, poor operative field or visualization, and inadequate postoperative care. Initially, limited septoplasty was recognized as a type of SMR and was primarily used only when the deviation of the septum limited the ability of the surgeon to accomplish his or her surgical goals.10 A prospective, multicenter study
70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92
Page 5
revealed that concurrent SMR was performed in 27% of ESS procedures for medically refractory CRS.11
From the available published articles, there are no clear answers for whether concurrent SMR improves the outcomes of FESS or the revision rates of FESS. Our study was designed to ascertain the outcomes of FESS combined with SMR/septoplasty in reducing FESS revision rates
2. Materials and Methods
2.1 Data source
The National Health Insurance (NHI) program in Taiwan, launched in 1995, has successfully provided universal and quality healthcare to patients at affordable costs and provides coverage to 99.6% of Taiwan’s 23 million residents.12 The National Health
Insurance Research Database (NHIRD) contains the medical claim history for the entire insured population, allowing us to compare the postoperative outcomes of our two patient groups.
The Taiwan National Health Research Institute established and manages the NHIRD, which includes the reimbursement claim data for the Taiwan NHI program. All personal identification information was encrypted before being released to the public to protect patient privacy.
By using the Taiwan Longitudinal Health Insurance Database 2000 from the NHIRD, we obtained a dataset containing all reimbursement claims data from 1989 to 2010 for one million subjects randomly selected from the entire insured population of 23 million. This random sample was representative of the entire insured population. The
13 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115
International Codes of Diseases 9th Revision, Clinical Modification (ICD-9-CM) was used to identify the diagnoses of disease and surgical procedures. This study used administrative data with all personal identifications encrypted. This study was approved by the institutional review board of the China Medical University Hospital, Taichung, Taiwan. The institutional review board approval number is CMUH102-REC2-070.
2.2. Study subjects
Our study used a population-based retrospective approach. We identified 4,484 patients with FESS for chronic rhinosinusitis during the period of 1989-2010. Patients who had undergone previous septoplasty or septomeatoplasty were excluded. In order to avoid confounding our sampling, we had excluded that the patients underwent SMR at revision FESS. These patients were divided into two groups: the control group (FESS alone) and the study group (FESS combined with SMR). The index date for each patient was defined by the date that the patient received the surgery. The primary outcome was the revision operative rate. Minimal period of three months between when the patient was operated and when the revision operation happened was allotted to determine recurrence.
2.3. Statistical analysis
We used a chi-square test for category variables and Fisher’s exact test for continuous variables to assess the differences in baseline demographic characteristics between the control and study groups. A logistic regression was used to predict the outcomes of the independent variables. A p value < 0.05 was considered to indicate statistical significance; all tests were two-tailed. All statistical analyses were performed with the statistical package SAS for Windows (Version 9.1, SAS Institute Inc., Cary, NC, USA). 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135 136 137 138
Page 7
3. Results
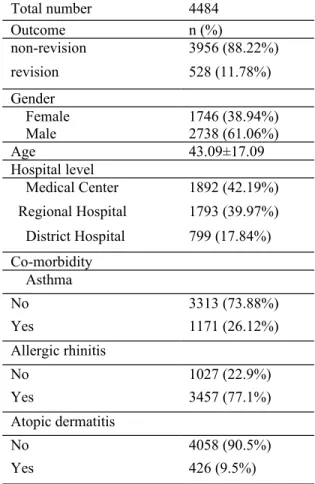
In total, 4,484 patients, with mean age of 43.09, who had undergone FESS were recruited into this study (2,738 were male and 1,746 were female). The number of patients who had undergone revision FESS was 528 (11.78%). There were 1,892 patients (42.19%) who had received surgeries in a medical center, 1,793 (39.97%) in a regional hospital, and 799 (17.84%) in a district hospital. Of these patients, 1,171 (26.12%) had asthma, 3,457 (77.1%) had allergic rhinitis (77.1%), and 426 (9.5%) had atopic dermatitis (Table 1).
3,608 Patients (80.46%) received FESS alone were in control group, whereas 876 patients (19.54%) underwent concurrent SMR/septoplasty during FESS were in study group. 2,149 cases (67.24%) and 589 cases (59.56%) were male in the control group and study group, respectively. The mean ages of the patients were 43.89 and 39.79 years old in the control and study groups. Regarding the co-morbidities, 964 patients (26.71%) in the control group and 207 patients (23.63%) in the study group had asthma, 2,765 patients (76.64%) in the control group and 692 patients (79.0%) in the study group patients had allergic rhinitis, and 343 patients (9.51%) in the control group and 83 patients (9.47%) in the study group had atopic dermatitis. There were no significant differences between these two groups regarding hospital level and co-morbidities (Table 2).
The revision patients were 446 (12.36%) and 82 (9.36%) in the control and study groups. The revision rates of these two groups were significantly different (p = 0.016) (Table 3). 19 139 140 141 142 143 144 145 146 147 148 149 150 151 152 153 154 155 156 157 158 159 160
Moreover, a logistic regression analysis found that patients in the control group had a higher revision rate than those in the study group (Odds Ratio = 1.404, p = 0.008). Regarding gender, male patients had higher revision rates than female patients (Odds ratio= 1.211, p = 0.0499). Older patients had less revision rate than younger patients (Odds Ratio = 0.993, p = 0.078). There was no significance difference between the hospital levels. In addition, patients with asthma or allergic rhinitis had higher revision rates compared with those patients without these two co-morbidities (Odds Ratio = 1.441, p = 0.000, and Odds Ratio = 1.629, p = 0.000, respectively), but patients with atopic dermatitis had no significant findings between study and control groups (Table 4).
4. Discussions
The predisposing factors of sinusitis are multitudinous, including anatomic abnormalities, air pollution, cigarette smoking, allergy or genetic factors. Anatomic abnormalities were once recognized as a significantfactor in the pathogenesis of rhinosinusitis. Septal deviation has been among those anomalies examined in multiple studies, and conflicting results have been reported. Some reports have described a correlation between septal deviation and the presence of rhinosinusitis, and an approximately equal number of reports have not found any such correlation. Most of these studies were rather small or examined this association indirectly, such as by investigating the role of a concha bullosa in rhinosinusitis.
Primary FESS failure is most often associated with re-obstruction in the area of the ostiomeatal complex. The cause of revision FESS can be divided into systemic and local factors. The local factors focus on various anatomic 161 162 163 164 165 166 167 168 169 170 171 172 173 174 175 176 177 178 179 180 181 182 183
Page 9
problems. According to previous studies, a severely deviated nasal septum is one of the most common causes of revision endoscopic sinus surgery.13,14 The most common anatomic factors associated with primary surgery failure have been the lateralization of the middle turbinate (78%), incomplete anterior ethmoidectomy (64%), scarred frontal recess (50%), incomplete posterior ethmoidectomy (41%), and middle meatal antrostomy stenosis (39%). In addition, retained aggernasi and retained uncinate process were identified in 49% and 37% of patients, respectively. Other factors such as persistent sphenoid disease and sphenoid ostium stenosis were less frequent.9
Septal deviation is a common anatomical variation. Its role in the pathogenesis of chronic rhinosinusitis remains unclear.15 The prevalence of septal deviation increases with
age. In infants, the prevalence of bilateral nasal septal deviation is 27% and that of unilateral deviation is 31%. The prevalence of septal deviation in adults is 79%.16 Of
patients about to undergo septoplasty, 27% showed sinus abnormality in plain radiology assessment.9 In addition, sinus pathology was found in 50% of 150 patients who had
rhinomanometrically proven nasal septal deformity and obstruction.17
Some studies have suggested that a deviation of the nasal septum may interfere with proper airflow, potentially predisposing one to sinus disease.18,19 However, Yousem concluded that the most critical factor in the development of sinusitis may be an intrinsic defect in mucociliary clearance. Anatomical narrowing or tortuous passageways may further compound the problem.20 The association demonstrated herein still suggests that
septal deviation may play a role in rhinosinusitis. Interestingly, Bayiz found that septoplasty alone can be adequate for the treatment of CRS with septal deviation.21
Three possible mechanisms may explain the pathophysiology of how septal deviation 25 184 185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202 203 204 205 206
may cause chronic rhinosinusitis. First, the stenosis of the ostiomeatal complex due to either the anatomical configuration or edematous mucosa may cause the obstruction and stagnation of secretions, which may subsequently become infected or perpetuate infection.22 The second potential mechanism involves aerodynamics: septal deviation
leads to an increase in nasal airflow velocity, which may cause mucosal desiccation and diminished mucociliary function.23,24 Third, changes in maxillary sinus pressure and
ventilation in theregion of the ostiomeatal complex due to septal deviations may cause chronic rhinosinusitis.25 Decreased antral pressure is correlated with posterior septal
deviations.
Regarding the angle of deviation, a higher incidence and severity of sinus disease were associated with an increased severity in septal deviation in the region of the ostiomeatal complex.20,26,27 Elahi reported that patients with increasing degrees of nasal
septal deviations were associated with higher incidences of osteo-meatal complex obstruction. The incidence and severity of sinus disease increased with the severity of septal deviation.28 In a review study, septal deviation was not only found to be strongly
associated with rhinosinusitis, but the study also found a statistically association between the degree of septal deviations and rhinosinusitis, especially in patients with a septal deviation angle greater than 10 degrees.29
However, not all reports supported the relationship between DNS and sinusitis. In one study, 500 consecutive patients underwent CT scanning of their paranasal sinuses for possible chronic sinus disease. Harar did not find any significant difference between chronic rhinosinusitis and septal deviation.30 Additionally, Yasan claimed that a mild to
moderate degree of deviated nasal septum was not a risk factor for chronic sinus disease. 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223 224 225 226 227 228 229
Page 11
Only the gross deviation of the nasal septum is a risk factor for the development of CRS.31 Collet reviewed published literature and concluded that a definite role cannot be
attributed to the nasal septum, either as the pathogenesis of chronic sinusitis or as a contributing factor. No relationship could be proven between septal surgery combined with sinus surgery and chronic sinusitis. A postoperative prognosis for the subjective comfort of patients has been demonstrated. Thus, performing septoplasty only aims to relieve complaints of nasal obstruction or improve surgical access to the ethmoid sinus.15 Due to the recent appreciation that the pathogenesis of rhinosinusitis is likely multifactorial, it is appropriate to re-examine its possible anatomic etiologies. A systematic analysis of septal deviation and rhinosinusitis was therefore performed to better define this association and describe the possible etiologic mechanisms.29
To optimize nasal patency and improve surgical access, SMR or septoplasty is commonly performed during FESS.32 So far, there have been limited publications
reporting the outcomes of concurrent SMR for FESS. Our results showed that patients who received FESS alone had higher revision rates than patients who received FESS combined with SMR. Concurrent SMR during FESS had better outcomes in our dataset. These findings may have been observed because concurrent SMR can provide better surgical field, reduce postoperative narrowing or synechiae of middle meatus, expand nasal space for sinus drainage and ventilation, and increase the convenience of postoperative care.
In our results, higher revision rate was revealed in the male patients. This finding may attribute to higher smoking rate of male in Taiwan, which is a critical factor in the
31 230 231 232 233 234 235 236 237 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252
recurrence of rhinosinusitis. On the other hand, decreased revision rate can be found in the older patients (Odds Ratio = 0.993, p = 0.078). This phenomenon may be associated with the age distribution of atopic diseases.
Epidemiologic, genetic, immunologic, and clinical studies show a close relationship between rhinosinusitis and atopic diseases (allergic rhinitis, asthma, and atopic dermatitis) 33. In our study population, there was 26.12% had asthma, 77.1% had allergic
rhinitis, and 9.5% had atopic dermatitis.
The distribution of atopic diseases between these two groups didn’t have significant difference (p=0.0682, 0.1481, 0.9771). Results from logistic regression showed patients with co-morbidities of asthma or allergic rhinitis had higher revision rate (Odds ratio=1.441 and 1.629). These results divulged if patients had rhinosinusitis with co-morbidity of atopic diseases (asthma or allergic rhinitis), concurrent SMR/septoplasty during FESS might be considered. Patients also need to be informed preoperatively for higher recurrence rates and closer postoperative follow-up.
There are some limitations in our study. First, because this study was a population-based retrospective cohort study from NHIRD, coding errors or over-diagnosis problems, including patients with/without nasal polyps or deviated nasal septum may occur due to the declaration of National Health Insurance (NHI). Second, the samples were from a claim database, clinical information such as preoperative patient’s stage and severity were not available. Presumably septoplasty would be used on more difficult cases to access the frontal recesses better. If the severity of disease could be controlled between the two study groups, a difference or an even greater change in the outcome of interest could be presented. Third, it might be different outcomes between the distributions of 253 254 255 256 257 258 259 260 261 262 263 264 265 266 267 268 269 270 271 272 273 274 275
Page 13
surgeons (rhinologists or those who that perform FESS intermittently). Thus, this would be an experience or surgeon ‘s ability confounder. The fourth limitation is patient selection bias. Some endoscopic sinus surgeries that were performed to treat non-CRS sinonasal problems, such as sinonasal tumor, were also included in this study.
5. Conclusions
This study showed an association between FESS combined with concurrent SMR/septoplasty and less incidence of revision rate of FESS. To reduce the possibility of failed FESS, concurrent SMR should be considered in primary FESS. Patients with asthma or allergic rhinitis may also require more revision surgeries after FESS.
37 276 277 278 279 280 281 282 283 284 285
References:
1. Benninger MS, Ferguson BJ, Hadley JA, et al. Adult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngology--head and
neck surgery 2003;129:S1-32.
2. Neil Bhattacharyya. Incremental Health Care Utilization and Expenditures for Chronic Rhinosinusitis in the United States. Annals of Otology. Rhinology &Laryngology 2011;120(7):423-7.
3. Benson V, Marano MA. Current estimates from the National Health Interview Survey, 1995. Vital and health statistics Series 10, Data from the National Health Survey 1998:1-428.
4. Mantovani M, Minetti A, Torretta S, et al. The velo-uvulo-pharyngeal lift or "roman blinds" technique for treatment of snoring: a preliminary report. Acta
otorhinolaryngologica Italica 2012;32:48-53.
5. Lindberg E, Theorell-Haglow J, Svensson M, et al. Sleep apnea and glucose metabolism: a long-term follow-up in a community-based sample. Chest 2012;142:935-42.
6. D'Elia E, Vanoli E, La Rovere MT, et al. Adaptive servo ventilation reduces central sleep apnea in chronic heart failure patients: beneficial effects on autonomic modulation of heart rate. Journal of cardiovascular medicine 2013;14:296-300.
7. Stow NW, Sale PJ, Lee D, et al. Simultaneous tonsillectomy and nasal surgery in adult obstructive sleep apnea: a pilot study. Otolaryngology--head and neck surgery 2012;147:387-91. 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307
Page 15
8. Roblin DG, Eccles R. What, if any, is the value of septal surgery? Clinical
otolaryngology and allied sciences 2002;27:77-80.
9. Musy PY, Kountakis SE. Anatomic findings in patients undergoing revision endoscopic sinus surgery. American journal of otolaryngology 2004;25:418-22.
10. Cantrell H. Limited septoplasty for endoscopic sinus surgery. Otolaryngology--head
and neck surgery 1997;116:274-7.
11. Smith TL, Litvack JR, Hwang PH, et al. Determinants of outcomes of sinus surgery: a multi-institutional prospective cohort study. Otolaryngology--head and neck
surgery2010;142:55-63.
12. Faria AC, da Silva-Junior SN, Garcia LV, et al. Volumetric analysis of the pharynx in patients with obstructive sleep apnea (OSA) treated with maxillomandibular advancement (MMA). Sleep & breathing 2013;17:395-401.
13. Moses RL, Cornetta A, Atkins JP, Jr., et al. Revision endoscopic sinus surgery: the Thomas Jefferson University experience. Ear, nose, & throat journal 1998;77:190, 93-5, 99-202.
14. Khalil HS, Eweiss AZ, Clifton N. Radiological findings in patients undergoing revision endoscopic sinus surgery: a retrospective case series study. BMC Ear Nose
Throat Disord 2011;11:4.
15. Collet S, Bertrand B, Cornu S, et al. Is septal deviation a risk factor for chronic sinusitis? Review of literature. Acta oto-rhino-laryngologica Belgica 2001;55:299-304. 16. Gray LP. Deviated nasal septum. Incidence and etiology. The Annals of otology,
rhinology & laryngology Supplement 1978;87:3-20. 43 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329
17. Matschke RG, Fiebach A. [Septum deviation and concomitant sinusitis]. Hno 1985;33:541-4.
18. Stallman JS, Lobo JN, Som PM. The incidence of concha bullosa and its relationship to nasal septal deviation and paranasal sinus disease. AJNR American
journal of neuroradiology 2004;25:1613-8.
19. Bolger WE, Butzin CA, Parsons DS. Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. The Laryngoscope 1991;101:56-64.
20. Yousem DM, Kennedy DW, Rosenberg S. Ostiomeatal complex risk factors for sinusitis: CT evaluation. The Journal of otolaryngology 1991;20:419-24.
21. Bayiz U, Dursun E, Islam A, et al. Is septoplasty alone adequate for the treatment of chronic rhinosinusitis with septal deviation? American journal of rhinology 2005;19:612-6.
22. Stammberger H, Posawetz W. Functional endoscopic sinus surgery. Concept, indications and results of the Messerklinger technique. European archives of
oto-rhino-laryngology 1990;247:63-76.
23. Blaugrund SM. Nasal obstruction. The nasal septum and concha bullosa.
Otolaryngologic clinics of North America 1989;22:291-306.
24. Danese M, Duvoisin B, Agrifoglio A, et al. [Influence of naso-sinusal anatomic variants on recurrent, persistent or chronic sinusitis. X-ray computed tomographic evaluation in 112 patients]. Journal de radiologie 1997;78:651-7.
25. Bachert C. [Experimental studies of the effect of nasal respiratory obstruction on ventilation of the maxillary sinus]. Laryngologie, Rhinologie, Otologie 1986;65:250-5. 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350 351 352
Page 17
26. Calhoun KH, Waggenspack GA, Simpson CB, et al. CT evaluation of the paranasal sinuses in symptomatic and asymptomatic populations. Otolaryngology--head and neck
surgery 1991;104:480-3.
27. Elahi MM, Frenkiel S. Septal deviation and chronic sinus disease. American journal
of rhinology 2000;14:175-9.
28. Elahi MM, Frenkiel S, Fageeh N. Paraseptal structural changes and chronic sinus disease in relation to the deviated septum. The Journal of otolaryngology 1997;26:236-40.
29. Orlandi RR. A systematic analysis of septal deviation associated with rhinosinusitis.
The Laryngoscope 2010;120:1687-95.
30. Harar RP, Chadha NK, Rogers G. The role of septal deviation in adult chronic rhinosinusitis: a study of 500 patients. Rhinology 2004;42:126-30.
31. Yasan H, Dogru H, Baykal B, et al. What is the relationship between chronic sinus disease and isolated nasal septal deviation? Otolaryngology--head and neck surgery 2005;133:190-3.
32. Rudmik L, Mace J, Ferguson BJ, et al. Concurrent septoplasty during endoscopic sinus surgery for chronic rhinosinusitis: does it confound outcomes assessment? The
Laryngoscope 2011;121:2679-83.
33. Tan RA, Corren J. The relationship of rhinitis and asthma, sinusitis, food allergy, and eczema. Immunology and allergy clinics of North America 2011; 31:481-491.
49 353 354 355 356 357 358 359 360 361 362 363 364 365 366 367 368 369 370 371 372 373 374 375
Total number 4484 Outcome n (%) non-revision 3956 (88.22%) revision 528 (11.78%) Gender Female 1746 (38.94%) Male 2738 (61.06%) Age 43.09±17.09 Hospital level Medical Center 1892 (42.19%) Regional Hospital 1793 (39.97%) District Hospital 799 (17.84%) Co-morbidity Asthma No 3313 (73.88%) Yes 1171 (26.12%) Allergic rhinitis No 1027 (22.9%) Yes 3457 (77.1%) Atopic dermatitis No 4058 (90.5%) Yes 426 (9.5%) Abbreviations: n=number
Table 2.Demographic data of all patients (Control group versus Study group ) Control group (FESS) Study group (FESS with
SMR) Total number n % n % 3608 80.46 876 19.54 Gender n % n % χ2 Female 1459 40.44 287 32.76 17.1432 Male 2149 59.56 589 67.24 P< 0.0001
Age Mean SD Mean SD t test=6.86
P value < 0.0001
43.89 17.36 39.79 15.50
Hospital level n % n % fisher
Medical Center 1577 43.71 315 35.96 P = 0.9105 Regional Hospital 1370 37.97 423 48.17 377 378 379 380 381
Page 19 Co-morbidity n % n % χ2 Asthma 3.3259 P = 0.0682 No 2644 73.28 669 76.37 Yes 964 26.72 207 23.63 Allergic rhinitis 2.0919 P = 0.1481 No 843 23.36 184 21.00 Yes 2765 76.64 692 79.00 Atopic dermatitis 0.0008 P = 0.9771 No 3265 90.49 793 90.53 Yes 343 9.51 83 9.47
Abbreviations: n=number, SD: standard deviation
Table 3. Revision rate (Control group versus Study group )
Outcome (revision FESS)
χ2
No revision % Revision %
Control group (FESS) 3162 87.64 446 12.36 5.8238
Study group (FESS with SMR) 794 90.64 82 9.36 P = 0.0158
55 382 383 384 385 386 387 388 389 390 391 392 393 394 395 396 397 398
Table 4. Logistic regression of outcome(revision FESS)
Odds Ratio 95% CI P value
Group
Control group (FESS) 1.404 (1.092-1.804) 0.0081
Study group (FESS with SMR) (ref.)
Gender Male 1.211 (1.000-1.467) 0.0499 Female (ref.) Age 0.993 (0.987-0.998) 0.0078 Hospital level Medical Center 1.129 (0.920-1.386) 0.2460
Regional Hospital (ref.)
District Hospital 1.179 (0.913-1.524) 0.2068 Asthma No (ref.) Yes 1.441 (1.177-1.765) 0.0004 Allergic rhinitis No (ref.) Yes 1.629 (1.265-2.097) 0.0002 Atopic dermatitis No (ref.) Yes 0.955 (0.699-1.305) 0.7743
Abbreviations: CI: confidence interval, ref: reference group 400 401 402 403 404 405 406 407 408 409 410