j o u r n a l h o m e p a g e : w w w . i n t l . e l s e v i e r h e a l t h . c o m / j o u r n a l s / i j m i
Development and evaluation of a patient-oriented
education system for diabetes management
Ting-I Lee
a, Yu-Ting Yeh
b, Chien-Tsai Liu
c,∗, Ping-Ling Chen
daTaipei Medical University, Wanfang Hospital, Taipei, Taiwan
bGraduate Institute of Medical Sciences, Taipei Medical University, Taipei, Taiwan
cGraduate Institute of Medical Informatics, Taipei Medical University, 250 Wu-Xing Street, Taipei, Taiwan dCollege of Nursing, Taipei Medical University, Taipei, Taiwan
a r t i c l e
i n f o
Article history:
Received 7 February 2005 Received in revised form 10 March 2006 Accepted 8 May 2006 Keywords: Internet Diabetes mellitus Disease management Patient education
a b s t r a c t
Purpose: To develop and evaluate a Web-based, patient-orientated diabetic education
man-agement (POEM) system.
Methods: The POEM system has been developed to extend hospital patient education by
integrating patients’ medical care data into their education program components and pre-senting them on the Web. Since most patients are concerned about their medical care data, the POEM system can provide the incentives for patients to continuously and persistently log in and learn the required knowledge and skills, improving their clinical outcomes. A quasi-experimental method that uses control groups and pretests was used to evaluate the outcomes of the system intervention. We recruited patients with type-2 diabetes and alter-natively assigned them to intervention and control groups. We compared laboratory test results including fasting blood glucose, HbA1c, total cholesterol, triglyceride (TG), and HDL between the two groups from the first visit through each follow-up visit. The study period progressed from September 2003 to May 2004 at the Metabolism Center of a medical teaching hospital in Taipei.
Results: In this study, we recruited 274 participants: 134 (57% males and 43% females)
in the intervention group and 140 (46% males and 54% females) in the control group. The patients’ laboratory test results from the first visit for fasting blood glucose, HbA1c, total cholesterol level, TG, and HDL in the intervention and control groups were respec-tively 187.54± 77.10 and 189.99 ± 73.49 mg/dl, 9.03 ± 2.79% and 8.95 ± 2.23%, 193.29 ± 47.93 and 202.52± 58.45 mg/dl, 152.48 ± 70.85 and 157.37 ± 74.88 mg/dl, and 44.97 ± 12.09 and 45.32± 12.08 mg/dl. There were three follow-up visits during the study period. We collected laboratory test results of the two groups through each of the following visits and analyzed them using ANCOVA. We discovered a significant difference in fasting blood glucose lev-els between intervention and control group as early as the first follow-up. At the second follow-up, both fasting blood glucose and HBA1c levels were significantly different between intervention and control group. At the third follow-up, there was a significant difference in fasting blood glucose, HBA1c, and total cholesterol between intervention and control group. We also monitored the number of logins for the patients in the intervention group during the follow-up period. The result showed the patients had consistently logged into the POEM system (about 8.5± 3.7 logins per person per month after 3 months enrollment). Thus, the patients in the intervention group had better control of their fasting blood glucose, HbA1c
∗Corresponding author. Tel.: +886 2 23776730x202; fax: +886 2 27339049.
E-mail address:[email protected](C.-T. Liu).
1386-5056/$ – see front matter © 2006 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijmedinf.2006.05.030
656
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 ( 2 0 0 7 ) 655–663and total cholesterol levels than those in the control group due to the assistance of the system.
Conclusions: The POEM system can help patients control their glucose, HbA1c and total
cholesterol levels to manage their diabetes, providing an easy and inexpensive way to extend hospital-based patient education services for community-based continuous patient education.
© 2006 Elsevier Ireland Ltd. All rights reserved.
1.
Introduction
Diabetes is an irreversible disease requiring lifetime care and rehabilitation. Persistent monitoring and control of blood sugar levels are effective treatments[1–4], whereas consistent patient education to improve their ability in administering self-care is also effective, lowering the risks of developing com-plications[3,5–10]. In Taiwan, traditional patient education as well as follow-ups requires patients to return to the hospitals where they received their medical care. In order to encour-age patient participation, most education activities operate in conjunction with follow-up clinics[11–13].
As the Internet becomes more widespread, the general public is beginning to seek medical information and support online[13–16]. There are currently many Web sites providing general information on diabetes, its treatments, and knowl-edge and skills of self-management[17,18]. However, most patients require more specific information regarding their individual disease conditions. Therefore, it is hardly possible for them to obtain appropriate and adequate education from the Internet without the help of clinical professionals[19–21]. In recent years, many researchers have used computer pro-grams and Web interfaces [22–28] to provide frequent and responsive interactions between patients and their physicians online. The online services can motivate patients to utilize the systems more enthusiastically, leading to the better manage-ment of their diabetes conditions.
Patient education is usually an important component in routine medical services. After being evaluated and receiving instructions from their doctors at a hospital visit, a patient can receive an individual tutorial along with education mate-rials (such as goals to achieve, and knowledge and skills for self-management) based on the development of their disease conditions. To extend this highly individualized patient educa-tion for a lasting effect, such tutorials and educaeduca-tion materials should be presented on the Web so patients can easily access the information after having left the hospital.
A high percentage of the population in Taiwan use the Internet (about 61%)[29]; thus, dissemination of health care information through it is becoming increasingly popular. An Internet questionnaire survey on information provided by medical care services most concerned by patients showed that the top two were: completeness of their medical care data and comprehensive explanations for their prescribed medicines
[30]. Based on these needs, we have developed a patient-oriented education management (POEM) system for extending the routine patient education service[31].
In the system, we collect diabetic patients’ medical care data along with their education materials at each hospital visit and organize them into educational folders, then present the
structured folders on the Web. This paper is organized into six sections presenting: a brief description of the POEM system in Section2; the method for evaluation of the system in Section3; the results shown and discussed in Sections4 and 5; followed by conclusions in Section6.
2.
System description
The POEM system, as shown inFig. 1, consists of the follow-ing major components: Web browsers for patients; a patient-oriented medical care data organizer (POMDO) for consolidat-ing an individual’s medical care data in a hospital; a Web server as repository and service provider for patients’ medical care information and education materials.
The POMDO is used to retrieve a patient’s medical care data from hospital information systems at each visit and orga-nize them into a folder for that visit. The medical care data currently include a patient’s demographical data, medication data (prescription orders), laboratory test results, date of visit, and date of next follow-up visit. The consolidated data are then transferred to the Web server via file transfer protocol (FTP) on a daily basis.
The Web server consists of: account management, doc-ument management, patient-oriented profile (POP) manage-ment, and alert and reminder control. The account manager handles user names and passwords, controlling their access right. There are two types of users: patients and educators. Patients can only access their own folders consisting of med-ical care data and education materials; educators can access any patient’s medical data along with previously given edu-cation materials while also being able to compose eduedu-cation materials for a specific patient.
The education materials include a wide range of knowledge and skills that diabetic patients may need to know for manage-ment of their conditions such as: a set of printed or handwrit-ten sheets, lecture notes, instructions, books or manuals; or they can be videos of class lectures or demonstration pictures for insulin injections. Currently, the knowledge and skills are classified into 13 components (Fig. 2, checkboxes of window A, from top to bottom): foot-care; instructions for daily care; self-monitoring of blood glucose; instructions for low blood glucose level; instructions for high blood glucose level; knowledge of diabetes; insulin injection; diet; exercise; diabetic medication; instructions for using glucose meters; diabetes complications; other goals and notes. Each component is constituted of a set of predefined instructions and materials.
These materials are created by doctors and patient edu-cators based on predefined education program components, then transformed into electronic formats. Written notes or printed sheets are digitalized into MicrosoftTM word format
Fig. 1 – The framework of a patient-oriented education management system.
(.doc) or AdobeTM portable document format (.pdf); lecture
notes into PowerPointTM format (.ppt); static images or
pic-tures into Joint Photographic Experts Group format (.jpg); videos into Moving Picture Experts Group format (.mpg). The
document manager organizes these materials and presents them in a tree structure for visualization (Fig. 2, window B). Thus, it can help an educator assign the appropriate educa-tion materials for diabetic patients based on their physician’s
658
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 ( 2 0 0 7 ) 655–663Fig. 3 – Web interfaces for presentation of medical care data and education materials through POP management.
recommendations. To describe individual goals and other notes, an editing window (Fig. 2, window C) appears for the educator to write remarks if the “other goals and notes” category is selected.
The POP manager organizes education materials, medica-tion data and laboratory test results from each patient visit into separate patient education folders in the order of visit. Patients have their own separate folders, presented on their Web page. (Fig. 3, window A). Three columns (marked by squares A–C) on this page are: education materials, laboratory test results, and medication data. After selecting the date of a hospital visit and clicking “laboratory test results”, the results of the laboratory tests performed at that visit are displayed in a pop-up window (Fig. 3, window B). Each record contains the details of the test including: name, test value, normal range and comments. Thus, patients can easily access and review their clinical data and education materials online.
The alert and reminder control mechanism persistently monitors a patient’s laboratory test results performed in the hospital, and sends e-mails to alert educators for further investigation when the results are out of a predefined normal range. In an emergency where a patient must return for treat-ment, there is an interface to help educators write and send messages to the patient. Reminders will also automatically be sent to patients one week before their follow-up appointment in forms of both email and cellphone SMS (short message service).
At each visit, the doctor evaluates and determines the patient’s education need and the components that should be
given, marking them on a referral sheet if needed. The referred patients then take the referral sheet to a patient educator to receive their education program. The patient educator chooses the appropriate set of education materials, and provides a detailed description on them for the patient based on the referral sheet. These materials, along with the medical data indicated above, are collected and integrated into the POEM system, which can then be presented on the Web where the patients can access the information after having left the hos-pital. The POEM system has been developed and installed for use since September 2003 at Taipei Medical University Wan-fang Hospital (TMUWFH). The Website ishttp://dmc.tw/.
3.
Evaluation method
3.1. Study design
A quasi-experimental study that uses control groups and pretests was used to evaluate the outcomes of the system intervention. The target population of this study was the patients with type-2 diabetes who visited the Metabolism Cen-ter at TMUWFH. In addition, the patients must meet the fol-lowing conditions:
• Did not have any severe complications that would affect the patients’ ability to follow physician’s orders, for example, blindness, stroke, or amputation;
• Had a normal level of consciousness and the ability to read or communicate with spoken language in order for patient educators to carry out education;
• Signed an agreement of consent to participate in the study; • Have accessibility to the Internet by patient or family
members.
The qualified patients were alternatively assigned to the intervention or control group based on the order of their visits. According to the statistics of TMUWFH outpatient services, an average of 120 diabetic patients visited the Metabolism Center per day in the past year. Thus, we expected to recruit 150 patients in each group in one month. The study period was from the beginning of September 2003 to the end of May 2004.
3.2. Intervention
Patients in both groups were treated based on the same treatment guidelines and traditional patient education pro-grams, and were required to return for follow-ups every three months. Additionally, each patient in the intervention group was assigned a username and password to log into the POEM system, and received training (could be in the presence of family members) on accessing the Internet, using the POEM system, and reading their cell phone messages.
The improvement of diabetes conditions between the inter-vention and control group was evaluated through labora-tory test results including fasting blood glucose, HbA1c, total cholesterol, triglyceride (TG), and HDL, by comparing the first visit (baseline) with each follow-up visit. In addition to the laboratory test results, we collected the visit date, next follow-up date, education materials received, and medication data (orders) from both groups of patients at each visit to the hos-pital. In order to establish the baseline, only patients with
valid results on fasting blood glucose, HbA1c, total cholesterol, TG, and HDL tests from the first visit were included. However, if patients failed to return for one or more follow-up or had invalid test results from a follow-up visit; their results were excluded for those particular tests.
3.3. Data collection and analysis
We recruited the participants from patients visiting the Metabolism Center at TMUWFH in September 2003. Two hun-dred and eighty-eight qualified patients were recruited and alternatively assigned to the control or intervention group, resulting in each group with 144 patients. Fourteen patients were excluded due to one or more invalid test results from their first visit, lowering the total number of participants to 274: 134 in the intervention group and 140 in the control group. During the study period we collected the patients’ laboratory test results of their first (December 2003), second (March 2004) and third (June 2004) follow-up visit. The number of partici-pants included for each laboratory test were: 216 (108 in both group) for fasting blood glucose; 210 (102 in the intervention group; 108 in the control group) for HbA1c; 216 (107 in the inter-vention group; 109 in the control group) for total cholesterol; 211 (105 in the intervention group; 106 in the control group) for TG; 206 (104 in the intervention group; 102 in the control group) for HDL.
Statistical analysis was performed with SPSS (version 11.0); all results are expressed as means± S.D. (standard deviation). The significance of difference between the intervention and control group from the baseline to the first, second and third follow-up visit was evaluated by ANCOVA (analysis of covari-ance), which controls the effects of different baseline values
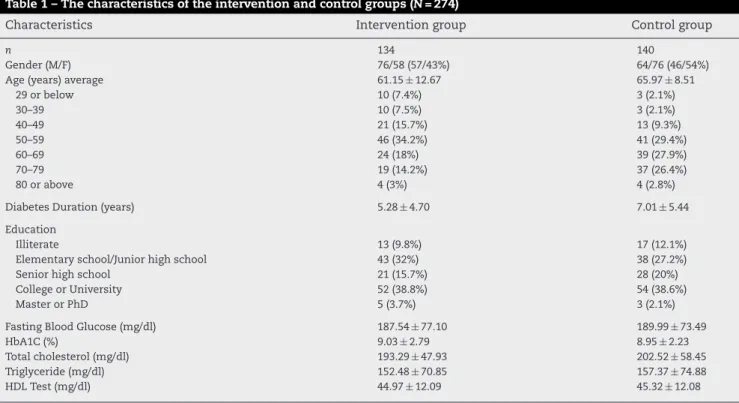
Table 1 – The characteristics of the intervention and control groups (N = 274)
Characteristics Intervention group Control group
n 134 140
Gender (M/F) 76/58 (57/43%) 64/76 (46/54%)
Age (years) average 61.15± 12.67 65.97± 8.51
29 or below 10 (7.4%) 3 (2.1%) 30–39 10 (7.5%) 3 (2.1%) 40–49 21 (15.7%) 13 (9.3%) 50–59 46 (34.2%) 41 (29.4%) 60–69 24 (18%) 39 (27.9%) 70–79 19 (14.2%) 37 (26.4%) 80 or above 4 (3%) 4 (2.8%)
Diabetes Duration (years) 5.28± 4.70 7.01± 5.44
Education
Illiterate 13 (9.8%) 17 (12.1%)
Elementary school/Junior high school 43 (32%) 38 (27.2%)
Senior high school 21 (15.7%) 28 (20%)
College or University 52 (38.8%) 54 (38.6%)
Master or PhD 5 (3.7%) 3 (2.1%)
Fasting Blood Glucose (mg/dl) 187.54± 77.10 189.99± 73.49
HbA1C (%) 9.03± 2.79 8.95± 2.23
Total cholesterol (mg/dl) 193.29± 47.93 202.52± 58.45
Triglyceride (mg/dl) 152.48± 70.85 157.37± 74.88
HDL Test (mg/dl) 44.97± 12.09 45.32± 12.08
660
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 ( 2 0 0 7 ) 655–663on the outcomes of interest. A P-value of 0.05 was considered to be statistically significant.
4.
Results
4.1. The characteristics of participants
The total number of participants in this study was 274: 134 (57% males and 43% females) in the intervention group and 140 (46% males and 54% females) in the control group. Their characteristics are shown in Table 1. The age and dura-tions of diabetes of the intervention and control group were 61.2± 12.7 and 66.0 ± 8.5 years and 5.28 ± 4.70 and 7.01 ± 5.44 years, respectively.
The patients with a college or university degree were the majority: 38.8% in the intervention group and 38.6% in the control group; those with elementary school or junior high school education were the second largest percentage: 32% in the intervention group and 27.2% in the control group; there were about 10% in both groups who are illiter-ate. The patients’ laboratory test results from the first visit for fasting blood glucose; HbA1c; total cholesterol level; TG; HDL in the intervention and control groups were respec-tively: 187.54± 77.10 and 189.99 ± 73.49 mg/dl; 9.03 ± 2.79% and 8.95± 2.23%; 193.29 ± 47.93 and 202.52 ± 58.45 mg/dl; 152.48± 70.85 and 157.37 ± 74.88 mg/dl; 44.97 ± 12.09 and 45.32± 12.08 mg/dl.
4.2. The results of laboratory tests during the
follow-up period
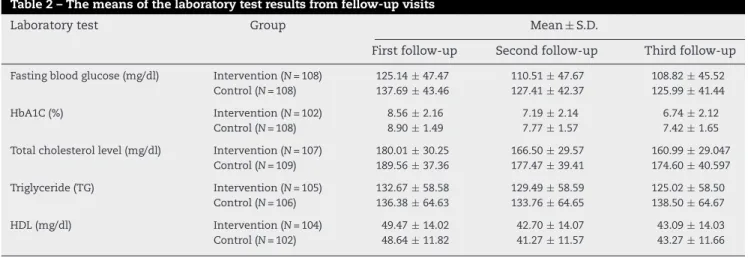
There were three follow-up visits during the study period. The patients’ fasting blood glucose, HbA1c, total cholesterol, TG, and HDL test results are shown inTable 2. After performing ANCOVA on the test results, as shown in Table 3, we dis-covered a significant difference (F = 5.079, P = 0.025) in fasting blood glucose levels between intervention and control group as early as the first follow-up. The differences from the first visit to the second follow-up were significant in fasting blood glucose (F = 9.735, P = 0.002) and HbA1c (F = 8.459, P = 0.004); the differences from the first to the third follow-up were sig-nificant in fasting blood glucose (F = 10.857, P = 0.001), HbA1c (F = 10.784, P = 0.001) and total cholesterol (F = 6.378, P = 0.012). FromTable 2we can see that the patients in the interven-tion group had better control of their fasting blood glucose, HbA1c and total cholesterol levels than those in the control group.
4.3. Analysis of user logins
During the follow-up period, we also monitored the number of logins for the patients in the intervention group (Fig. 4). In the first three months there was an average of 9.6± 2.9 logins per patient per month, then it slowly decreased in the fol-lowing 3 months to 8.5± 3.7, staying there with only slight
Table 2 – The means of the laboratory test results from fellow-up visits
Laboratory test Group Mean± S.D.
First follow-up Second follow-up Third follow-up Fasting blood glucose (mg/dl) Intervention (N = 108) 125.14± 47.47 110.51± 47.67 108.82± 45.52
Control (N = 108) 137.69± 43.46 127.41± 42.37 125.99± 41.44
HbA1C (%) Intervention (N = 102) 8.56± 2.16 7.19± 2.14 6.74± 2.12
Control (N = 108) 8.90± 1.49 7.77± 1.57 7.42± 1.65
Total cholesterol level (mg/dl) Intervention (N = 107) 180.01± 30.25 166.50± 29.57 160.99± 29.047 Control (N = 109) 189.56± 37.36 177.47± 39.41 174.60± 40.597 Triglyceride (TG) Intervention (N = 105) 132.67± 58.58 129.49± 58.59 125.02± 58.50
Control (N = 106) 136.38± 64.63 133.76± 64.65 138.50± 64.67
HDL (mg/dl) Intervention (N = 104) 49.47± 14.02 42.70± 14.07 43.09± 14.03
Control (N = 102) 48.64± 11.82 41.27± 11.57 43.27± 11.66
Table 3 – ANCOVA on laboratory test results between the intervention and control groups from the first visit through the follow-up visits
Laboratory test First follow-up visit Second follow-up visit Third follow-up visit (Mean)2 F Significance (Mean)2 F Significance (Mean)2 F Significance Fasting blood glucose 7554.77 5.079 0.025* 14120.5 9.735 0.002* 14634.04 10.857 0.001*
HbA1C 7.23 3.248 0.073 19.96 8.459 0.004* 26.386 10.784 0.001*
Total cholesterol level 2087.34 2.630 0.106 3144.73 3.688 0.056 5791.855 6.378 0.012* Triglyceride (TG) 108.49 0.041 0.840 215.67 0.080 0.777 6633.393 2.473 0.117
HDL 60.28 0.909 0.341 60.28 0.909 0.341 62.829 0.947 0.332
Fig. 4 – The trend of user logins during the follow-up period.
fluctuations afterwards. It can be seen that the patients in the intervention group had consistently used the POEM sys-tem, and had better control of their fasting blood glucose, HbA1c and total cholesterol level than those in the control group.
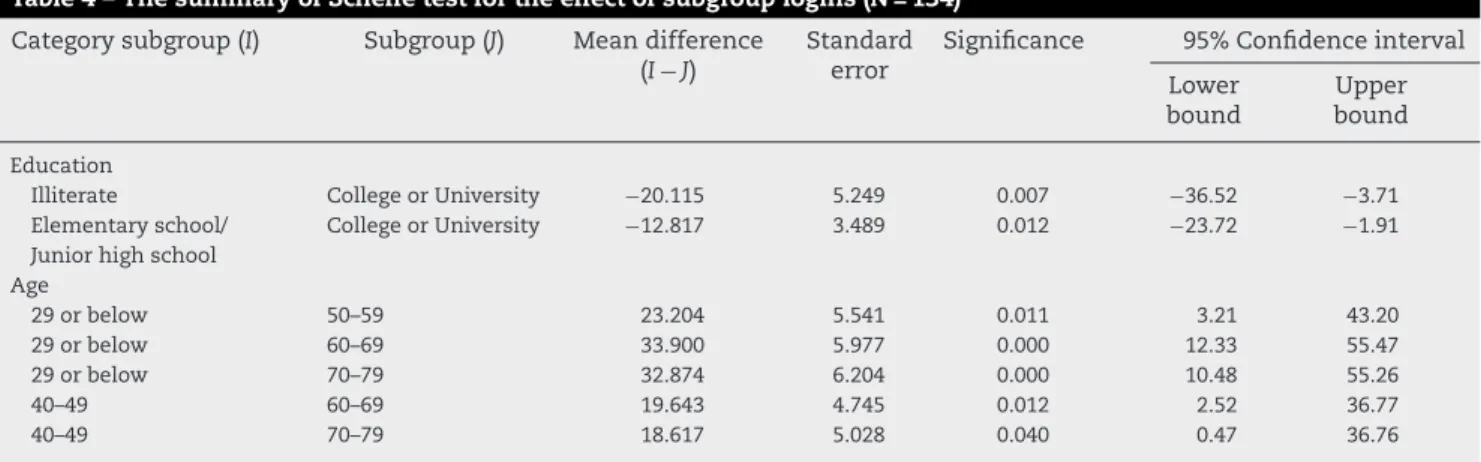
To analyze the effects of education background and age on the use of the system, we performed ANOVA to test the significance between subgroups in each education back-ground and age category. The results showed that different subgroups in categories “education backgrounds” (degree of freedom, d.f. = 4, F = 6.005, P < 0.01) and “age” (d.f. = 6, F = 7.813,
P < 0.01) had significant effects on the use of the system. The
summary of the effects of age and education background on the number of logins is shown inTable 4. For the “Edu-cation background” category, the differences mainly came from the subgroups “Illiterate” to “College or university” (P = 0.007) and “Elementary school/Junior high school” to “College or university” (P = 0.012). Meaning the number of logins of subgroup “College or university” was larger than that of “Illiterate” or “Elementary school/Junior high school”. Similarly, for the age category the significant differences were mainly contributed by the subgroups “29 or below” and “40–49”. The patients in the subgroup “29 or below” logged in the POEM system more frequently than those in the “50–59”, “60–69” and “70–79” subgroups; those in the “40–49” sub-group more frequently than those in the “60–69” and “70–79” subgroups.
5.
Discussion
Diabetes mellitus is a complex chronic metabolic dis-ease. Without appropriate treatment, complications such as cerebrovascular and coronary heart disease, nephropathy, retinopathy, and gangrenous foot often occur[1,2]. Persistent and continued patient education can effectively help patients control blood glucose and HbA1c levels and delay the occur-rence of associated complications[7,10,11,32]. In our approach we collect and integrate a diabetic patient’s medical care data and education materials for each hospital visit, and then present the information on the Web so that the patients can access the information after having left the hospital.
Since the medical care data are closely relevant to patients’ health conditions and the education materials assigned specifically to meet their needs, patients can therefore be motivated to review education materials while accessing medical care information. Our study has demonstrated that patients could be motivated to use the POEM system, conse-quently managing their diabetes conditions better. The results have been consistent with those reported for other Web-based diabetes management systems that provide frequent and responsive interactions between patients and their physi-cians through emails or web interfaces[22–28,33–35].
To maximize active participation, we provided not only medical care data as incentives, but also reminders for follow-up returns through email and cell phone SMS messages. From the login numbers, we can see that this multifaceted interven-tion has kept patients consistently involved with the POEM system. Active participation is one of the main forces lead-ing to better outcome of self-management for patients with chronic diseases[36]. Therefore, the POEM system can be an efficacious delivery system for patient education, and can also help patients manage their diabetes conditions.
Under the current health insurance system in Taiwan
[37], the reimbursement policy is mainly based on the fee for services. Thus, most hospitals place their focus on treatment and therapy rather than patient education; these programs must therefore be designed carefully in order to minimize overall cost. Our approach extends routine hospital patient education services, and provides an easy and inexpensive way for continuous effect. This approach can be particularly useful for the hospitals in communities with a high
percent-Table 4 – The summary of Scheffe test for the effect of subgroup logins (N = 134)
Category subgroup (I) Subgroup (J) Mean difference (I− J)
Standard error
Significance 95% Confidence interval Lower
bound
Upper bound Education
Illiterate College or University −20.115 5.249 0.007 −36.52 −3.71
Elementary school/ Junior high school
College or University −12.817 3.489 0.012 −23.72 −1.91 Age 29 or below 50–59 23.204 5.541 0.011 3.21 43.20 29 or below 60–69 33.900 5.977 0.000 12.33 55.47 29 or below 70–79 32.874 6.204 0.000 10.48 55.26 40–49 60–69 19.643 4.745 0.012 2.52 36.77 40–49 70–79 18.617 5.028 0.040 0.47 36.76
662
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 ( 2 0 0 7 ) 655–663Summary points
What was known before the study
• Persistent monitoring, control of blood sugar level, and consistent education for patients to enhance their abil-ity in administering self-care are effective treatments for diabetes.
• Computer programs and Web interfaces have been used to provide frequent and responsive interactions between patients and their physicians online. These online services can help patients manage their dia-betes conditions better.
• Little was known on the methods of motivating patients to constantly use the online services and actively participate in self-management.
What this study has added to the body of knowledge
• In our work (the POEM system), we integrated patients’ clinical data into their education program compo-nents and presented the data on the Web. Since most patients are concerned about their medical data, the system provides this as incentive for them to contin-uously and persistently log in, learning the required knowledge and skills after having left hospitals. This is supported by the trend of user logins during the follow-up period: the number of logins reached a sta-ble amount after three months enrollment. We can see that the system has kept patients consistently involved.
• Our study has demonstrated that the POEM system is able to help patients control their blood glucose, HbA1c, and HDL levels better. This system can be an efficacious delivery system for patient education and self-management.
• Since the POEM system extends routine hospital patient education services while providing an easy and inexpensive way for continuous patient education, it can easily be adopted to support continuous patient education services with little additional effort. This approach can be particularly useful for the hospitals in communities with a high percentage of Internet users.
age of Internet users. With little additional effort, the POEM system can be easily adopted to support continuous patient education services.
Although our study showed the improvement of labora-tory test results, there were many unaccounted factors that could have influenced the clinical outcomes. In this study we did not record the courses and the Web pages browsed by a patient; thus, we could not justify which components (educa-tional materials, medical care data, or reminders) contributed most to the improvement. There are also problems in our user interfaces such as lack of consideration for illiterate persons. System security for management of user accounts and logins need to be reinforced so that the patients and their family
members can have different rights to access sensitive data. Further studies should be conducted after enhancement of functionality and tracking mechanisms of the POEM system.
6.
Conclusion
We take advantage of Web technology to extend hospital patient education services by integrating patients’ medical care data into their education program components and pre-senting them on the Web. Since most patients are concerned about their medical care data, the POEM system can provide the incentives to motivate patients to continuously and per-sistently log in and learn their required knowledge and skills, prolonging the effect of patient education after they have left the hospitals. The evaluation results showed that the POEM system was able to help patients control their blood glucose, HbA1c, and HDL levels better. The POEM system can not only support hospital routine patient education service, but can also provide an easy and inexpensive way for extension of patient education, increasing the likeability to be adopted by hospitals. Since there were many unaccounted factors that could have influenced on clinical outcomes, we could not justify which components (educational materials, medi-cal care data or reminders) contributed to the improvement in our approach; further studies should be conducted on these aspects.
Acknowledgments
This research was partially supported by the grants from the National Science Council (NSC92-2516-S-038-002) and the Taipei Medical University Wan-Fang Hospital (93TMU-WFH-25).
r e f e r e n c e s
[1] Diabetes Control and Complications Trial Research Group, The effect of intensive treatment of diabetes on the development and progression of long term complications in insulin-dependent diabetes mellitus, N. Engl. J. Med. 329 (1993) 977–986.
[2] United Kingdom Prospective Diabetes Study (UKPDS) Group, Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33), Lancet 352 (1998) 837–853.
[3] M. Berger, I. M ¨uhlhauser, Diabetes care and patient-oriented outcomes, J. Am. Med. Assoc. 281 (18) (1999) 1676–1678. [4] American Diabetes Association Position Statement,
Standards of medical care for patients with diabetes mellitus, Diab. Care 26 (2003) S33–S50.
[5] N.N. Abourizk, P.J. O’Connor, B.F. Crabtree, J.D. Schnatz, An outpatient model of integrated diabetes treatment and education: functional, metabolic, and knowledge outcomes, Diab. Educ. 20 (5) (1994) 416–421.
[6] S. Clement, Diabetes self-management education, Diab. Care 18 (1995) 1204–1214.
[7] R. Deichmann, E. Castello, R. Horswell, K.E. Friday, Improvement in diabetic care as measured by HbA1C after a physician education project, Diab. Care 39 (1999) 444–447.
[8] J.D. West, K.L. Goldberg, Diabetes self-care knowledge among outpatients at a Veterans Affairs medical center, Am. J. Health Syst. Pharm. 59 (2002) 849–852.
[9] K.A. Peterson, M. Hughes, Readiness to change and clinical success in a diabetes educational program, J. Am. Board Fam. Pract. 15 (4) (2002) 266–271.
[10] F. Snoek, A.P. Visser (Eds.), Improving quality of life in diabetes education: how effective is education, Patient Educ. Counsel. 51 (2003) 1–3 (editorial).
[11] T.R. Pieber, A. Holler, A. Siebenhofer, G.A. Brunner, B. Semlitsch, S. Schattenberg, H. Zapotoczky, W. Rainer, G.J. Krejs, Evaluation of a structured teaching and treatment programme for type 2 diabetes in general practice in a rural area of Austria, Diab. Med. 12 (1995) 349–354.
[12] C.M. Renders, E.H. Wagner, G.D. Valk, J.T. Eijk van, Interventions to improve the management of diabetes in primary care, output, and community settings, Diab. Care 34 (10) (2001) 1821–1832.
[13] C.T. Liu, Y.T. Yeh, I.J. Chiang, H.Y. Chen, T.I. Lee, W.T. Chiu, Development and evaluation of an integrated
pharmaceutical education system, Int. J. Med. Inform. 73 (4) (2004) 383–389.
[14] J.J. Cimino, S.A. Socratous, P.D. Clayton, Internet as clinical information system: Application development using the World Wide Web, J. Am. Med. Inform. Assoc. 2 (1995) 273–284. [15] R. Peters, R. Sikorski, The cardiology beat: an Internet
education for patients and health professionals, J. Am. Med. Assoc. 278 (6) (1997) 451–452.
[16] A.R. Jadad, A. Gagliardi, Rating health information on the Internet: navigating to knowledge or to Babel? J. Am. Med. Assoc. 279 (1998) 611–614.
[17] J.F. Zrebiec, A.M. Jacobbson, What attracts patients with diabetes to an Internet support group: a 21-month longitudinal website study, Diab. Med. 18 (2001) 154–158. [18] M.I. Kim, P.W. Ladenson, Diabetes on the Internet: resources
for patients, J. Clin. Endocrinol. Metab. 87 (8) (2002) 3523–3526.
[19] P.A. Thakurdesai, P.L. Kole, R.P. Pareek, Evaluation of the quality and contents of diabetes mellitus patient education on Internet, Patient Educ. Counsel. 53 (2004) 309–313. [20] P. Impicciatore, C. Pandolfini, N. Casella, M. Bonati,
Reliability of health information for the public on the World Wide Web: systematic survey of advice on managing fever in children at home, Br. Med. J. 314 (1997) 1875–1879.
[21] P. Wilson, How to find the good and avoid the bad or ugly: a short guide to tools for rating quality of health information on the Internet, Br. Med. J. 324 (2002) 598–602.
[22] H.G. McKay, J.R. Seeley, D. King, R.E. Glasgow, E.G. Eakin, The diabetes network Internet-based physical activity
intervention, Diab. Care 24 (8) (2001) 1328–1334. [23] S. Plougmann, O.K. Hejlesen, D.A. Cavan, DiasNet—a
diabetes advisory system for communication and education via the internet, Int. J. Med. Inform. 64 (2001) 319–330.
[24] J.B. Meigs, H. Chueh, E. Cagliero, M.J. Barry, A. Dubey, D.E. Singer, P. Murphy-Sheehy, D.M. Nathan, C. Gildesgame, A controlled trail of web-based diabetes disease management, Diab. Care 26 (3) (2003) 750–757.
[25] R.E. Glasgow, S.M. Boles, H.G. McKay, E.G. Feil, M. Barrera Jr., The D-Net diabetes self-management program: long-term implementation, outcomes, and generalization results, Prev. Med. 36 (2003) 410–419.
[26] O. Ferrer-Roca, K.F. Burbano, A. C ´ardenas, P. Pulido, A. Diaz-Cardama, Web-based diabetes control, J. Telemed. Telecare 10 (2004) 277–281.
[27] H. Kwon, J. Cho, H. Kim, B. Song, S. Ko, J. Lee, S. Kim, S. Chang, H. Kim, B. Cha, K. Lee, H. Son, W. Lee, K. Yoon, Establishment of blood glucose monitoring system using the Internet, Diab. Care 27 (2004) 478–483.
[28] S.E. Davis Kirsch, F.M. Lewis, Using the World Wide Web in health-related intervention research, a review of controlled trials, CIN: Comput. Inform. Nursing 22 (1) (2004) 8–18. [29] Internet World Stats, Internet Usage and population
statistics in Asia, July 2005,http://www. internetworldstats.com/stats3.htm.
[30] Taiwan Health Reform Foundation: What information was the most concerned by patients about their medical care services, an Internet questionnaire survey, an Internet report October 2001, fromhttp://www.thrf.org.tw/. [31] Y.T. Yeh, T.I. Lee, C.Y. Hsu, A.J. Long, Y.C. Li, C.T. Liu, A
Framework for integrating information of clinical care into patient education for diabetes, J. Taiwan Assoc. Med. Inform. 14 (1) (2005) 15–24.
[32] P. Richard, B.Y. Nilsson, U. Rosenqvist, The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus, New Engl. J. Med. 329 (5) (1993) 304–309.
[33] D. Tate, R. Wing, R. Winett, Using Internet technology to deliver a behavioral weight loss program, J. Am. Med. Assoc. 285 (9) (2001) 1172–1177.
[34] M. Zabinski, M. Pung, D. Wilfley, et al., Reducing risk factors for eating disorders: targeting at-risk women with a computerized psychoeducational program, Int. J. Eat. Disord. 29 (4) (2001) 401–408.
[35] R. Bellazzi, M. Arcelloni, G. Bensa, H. Blankenfeld, E. Brugu ´es, et al., Management of patients with diabetes through information technology: tools for monitoring and control of the patients’ metabolic behavior, Diab. Technol. Ther. 6 (5) (2004) 567–578.
[36] L. Lenert, R.F. Mu ˜noz, J. stoddard, K. Delucchi, A. Bansod, S. Skoczen, E.J. P ´erez-stable, Design and pilot evaluation of an internet smoking cessation program, J. Am. Med. Inform. Assoc. 10 (1) (2003) 16–20.
[37] Bureau of National Health Insurance in Taiwan
(http://www.nhi.gov.tw/), The reimbursement standard for National Health Insurance services, June 2004, Taipei, Taiwan.