CASE REPORT
Alcohol drinking triggers acute myocardial infarction in
a case of hypertrophic obstructive cardiomyopathy
阻塞性肥厚心肌症病患喝酒誘發急性心肌梗塞d病例報告
Po-Chao Hsu
a, Chih-Sheng Chu
a,b, Tsung-Hsien Lin
a,b, Ho-Ming Su
a,b,
Hsueh-Wei Yen
a,b, Wen-Ter Lai
a,b, Sheng-Hsiung Sheu
a,b,*
許栢超a, 朱志生a, 林宗憲a,b,蘇河名a,b,顏學偉a,b, 賴文德a,b,許勝雄a,b,*
a
Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
b
Department of Internal Medicine, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Received 1 March 2010; accepted 9 August 2010 Available online 21 March 2011
KEYWORDS Acute myocardial infarction; Alcohol ingestion; Hypertrophic obstructive cardiomyopathy 關鍵詞 急性心肌梗塞; 喝酒; 阻塞性肥厚心肌症
Abstract Alcohol ingestionerelated increased left ventricular outflow tract (LVOT) pressure gradient in hypertrophic obstructive cardiomyopathy (HOCM) has been reported in the litera-ture; however, acute myocardial infarction (AMI) after alcohol drinking in this patient group is rarely reported. Herein, we report a 68-year-old man with chronic alcoholism suffering from AMI after alcohol drinking. Electrocardiography revealed complete left bundle branch block, and chest X-ray showed acute pulmonary edema. Intubation was done for respiratory failure and intra-aortic balloon pump was also inserted for unstable hemodynamics. However, emer-gent coronary angiography revealed normal coronary arteries. HOCM was diagnosed by a high pressure gradient over LVOT and systolic anterior motion of mitral valve by echocardiography. This patient became stable under intensive care and medical treatment. This case reminds physicians that alcohol ingestion might cause AMI in HOCM patients because of increased LVOT pressure gradient and decreased coronary perfusion despite normal coronary arteries. 摘 摘要要 在阻塞性肥厚心肌症病患因為喝酒造成左心室流出道壓力差上升已經有文獻報告過。然而, 喝酒後發生急性心肌梗塞在阻塞性肥厚心肌症族群則很少被報導。我們在此報告一位68歲有慢性 酒精中毒的男性病患在喝酒後發生急性心肌梗塞。心電圖上顯示是完全性左側支束傳導阻滯以及 胸部X光片顯示為急性肺水腫。這個病患因為呼吸衰竭被插管,也由於血行動力學不穩定被放置 了主動脈內氣球幫浦。然而緊急心導管的結果發現其冠狀動脈並無異常。阻塞性肥厚心肌症是在
* Corresponding author. Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Tzyou 1st
Road, Kaohsiung 80708, Taiwan.
E-mail address:[email protected](S.-H. Sheu).
a v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
j o u r n a l h o m e p a g e : h t t p : / / w w w . k j m s - o n l i n e . c o m
Kaohsiung Journal of Medical Sciences (2011) 27, 195e198
1607-551X/$36 Copyrightª 2011, Elsevier Taiwan LLC. All rights reserved. doi:10.1016/j.kjms.2010.08.003
左心室造影時發現在左心室流出道有較高的壓力差並且在超音波上發現僧帽瓣有收縮期的前移運 動。這個病患最後在加護病房照護以及藥物治療下逐漸穩定。這個案例告訴我們,儘管是在冠狀 動脈正常的情況下,喝酒可能會使有阻塞性肥厚心肌症的病患發生急性心肌梗塞,其原因可能是 由於上升左心室流出道的壓力差並造成冠狀動脈的灌流量減少所導致。
Copyrightª 2011, Elsevier Taiwan LLC. All rights reserved.
Introduction
Hypertrophic cardiomyopathy (HCM) is characterized by hypertrophy of the left ventricle without any obvious cause. It is also a genetic disease of the cardiac sarcomere with autosomal dominant pattern of inheritance. About one-third of patients with HCM have a LVOT pressure gradient at rest, and a similar fraction develops pressure gradient with provocation. According to the literature, alcohol ingestion could increase the LVOT pressure gradient and is considered to have harmful effects in patients of hypertrophic obstructive cardiomyopathy (HOCM) [1]. However, acute myocardial infarction (AMI) after alcohol drinking in this patient group has rarely been reported. Herein, we report a case of a man with chronic alcoholism suffering from AMI after alcohol drinking with normal coronary angiography.
Case presentation
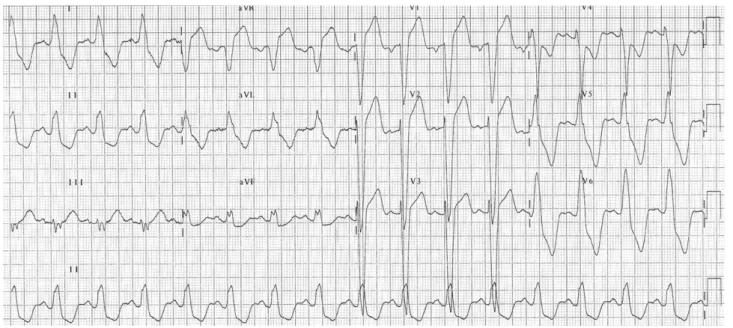
A 68-year-old man suffered from sudden-onset chest tight-ness, dyspnea, cold sweating, and nausea sensation after drinking several bottles of beer with his friends and was brought to our emergency department for help. It was a case of chronic alcoholism and denied heart disease, such as coronary artery disease, myocardial infarction, valvular heart disease, and cardiomyopathy before. After emer-gency department arrival, vital signs were as follows: pulse rate was 96 beats/min and blood pressure was 85/40 mmHg. Initial electrocardiogram (ECG) revealed complete left bundle branch block (CLBBB) (Fig. 1), and chest X-ray
showed acute pulmonary edema. Because of shock status and subsequent respiratory failure, vasopressor was given and intubation was done for unstable hemodynamics. Laboratory workup revealed the following: creatinine kinase (CK), 58 U/L; CKMB, 8.3 U/L; troponin I, 0.06 ng/mL; and C-reactive protein, 4.85 mg/L. Emergent percutaneous coronary intervention was suggested under the impression of AMI and intra-aortic balloon pump was also inserted for hemodynamic support. However, coronary angiography showed normal coronary arteries, and left ventriculography revealed no obvious wall motion defect. In addition, we also found a high pressure gradient (70 mmHg) of LVOT while pulling back from the left ventricle (Fig. 2A). Then, the patient was transferred to our cardiac care unit (CCU) for further intensive care.
In our CCU, bedside echocardiography revealed asym-metric left ventricular hypertrophy (Fig. 2B). Systolic anterior motion of mitral valve (Fig. 2C) and high pressure gradient (63 mmHg) of LVOT were noted by M-mode and Doppler echocardiography, which confirmed HOCM in this case. Laboratory data follow-up also showed progressive elevation of cardiac enzymes (peak cardiac enzymes: CK, 714 U/L; CKMB, 137.9 U/L; troponin I, 12.23 ng/mL) and abnormal lipid profile (total cholesterol, 256 mg/dL; low-density-lipoprotein cholesterol, 146.6 mg/dL). Because pulmonary edema and hemodynamics improved during CCU stay, we successfully removed intra-aortic balloon pump and vasopressor, and further weaned the patient off the ventilator. Medications, such as nondihydropyridine calcium channel blocker and statin, were also added for HOCM and dyslipidemia treatment. This patient was finally discharged
Figure 1. Initial electrocardiogram revealed complete left bundle branch block.
in stable condition, and ECG follow-up at outpatient visit showed only left ventricular hypertrophy and narrow QRS pattern (Fig. 3).
Discussion
AMI is a life-threatening emergency. Early reperfusion therapy is the standard treatment strategy for ST elevation myocardial infarction (including new-onset CLBBB) and benefits this condition. The 12-lead ECG is an important diagnostic tool for AMI because it enables physicians to localize the infarct-related coronary artery and to optimize treatment strategy. However, other conditions may mimic the ECG signs of AMI, such as pericarditis, Prinzmetal’s angina, cardioversion, hyperkalemia, and so on. HCM is also a possible cause of AMI, and most cases in the literature reveal normal coronary arteries or only nonsignificant lesions[2e6]. ECG findings in these cases showed a wide variety of abnormalities, including ST-segment depression, T-wave inversion, or even ST-segment elevation. Our case
showed CLBBB as an initial ECG finding, which was not reported in the literature. Despite there being no previous ECG to compare if this was a new-onset finding, ECG follow-up after recovery showed only left ventricular hypertrophy and narrow QRS pattern, which confirmed our thoughts. Cardiac enzymes also revealed serial change in our case. All these findings proved myocardial infarction despite normal coronary angiography.
There are some mechanisms to explain the relationships between myocardial injury and HCM, such as diminished coronary perfusion[2,3], recurrent episode of atrial fibril-lation[4], diminutive coronary artery[6], coronary artery spasm, septal perforator artery compression, myocardial bridging, and so on. However, alcohol ingestion was considered to be the initial trigger mechanism in our patient. Despite there still being few reports mentioning the relationship between alcohol ingestion and myocardial infarction[7], to our knowledge, our case is the first report of alcohol-triggered AMI in a patient with HOCM. The possible mechanism might be as follows: alcohol ingestion is associated with decreasing systolic blood pressure and Figure 2. (A) High pressure gradient (70 mmHg) of left ventricular outflow tract was found while pulling back from left ventricle. Bedside echocardiography revealed (B) asymmetric left ventricular hypertrophy and (C) systolic anterior motion of mitral valve by M-Mode (C).
increasing systolic anterior motion in the literature [1], which might increase pressure gradient of LVOT and further cause diminished coronary perfusion and myocardial injury. This rare case not only reminds us that alcohol ingestion might aggravate myocardial injury in patients of HCM, but also informs us that both alcohol and HCM are the two possible causes of AMI with normal coronary arteries.
References
[1] Paz R, Jortner R, Tunick PA, Sclarovsky S, Eilat B, Perez JL, et al. The effect of the ingestion of ethanol on obstruction of the left ventricular outflow tract in hypertrophic cardiomyop-athy. N Engl J Med 1996;335:938e41.
[2] Lin CS, Chen CH, Ding PY. Apical hypertrophic cardiomyopathy mimicking acute myocardial infarction. Int J Cardiol 1998;64: 305e7.
[3] Sato Y, Matsumoto N, Matsuo S, Yoda S, Kunimoto S, Saito S. Mid-ventricular hypertrophic obstructive cardiomyopathy pre-senting with acute myocardial infarction. Tex Heart Inst J 2007; 34:475e8.
[4] Limongelli G, Calabro’ P, Pacileo G, Santoro G, Calabro’ R. Myocardial infarction in a young athlete with non-obstructive hypertrophic cardiomyopathy and normal coronary arteries. Int J Cardiol 2007;115:e71e3.
[5] Di Bella G, Bramanti O, Russo MS, Migliorato A, Anfuso C, Minutoli F, et al. Hypertrophic cardiomyopathy mimicking acute myocardial infarction: diagnostic role of cardiac magnetic resonance. Int J Cardiol 2008;125:e34e6.
[6] Patane` S, Marte F, Di Bella G, Chiribiri A. Acute myocardial infarction with diminutive right coronary artery and obstructive hypertrophic cardiomyopathy without significant coronary stenoses. Int J Cardiol 2009;135:e73e5.
[7] Murphy JC, Campbell NP, McKeown PP. Alcohol induced myocardial infarction in two young brothers. Int J Cardiol 2008; 127:e145e7.
Figure 3. Electrocardiographic follow-up at outpatient visit showed only left ventricular hypertrophy and narrow QRS pattern.