Responsiveness of the Michigan Hand Outcomes
Questionnaire and the Disabilities of the Arm, Shoulder,
and Hand Questionnaire in Patients With Hand Injury
Yi-Shiung Horng, MD, Ming-Chuan Lin, MD, Chi-Tzu Feng, BS, Chi-Hung Huang, BS, Hsin-Chi Wu, MD, Jung-Der Wang, MD
Purpose To compare responsiveness of the Michigan Hand Outcomes Questionnaire (MHQ) with that of the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire in patients with hand injuries. We postulated that the MHQ may be more sensitive to functional changes in the hands, whereas the DASH questionnaire would have a closer association with days of disability.
Methods Patients with hand injuries were consecutively recruited from 2 community hospi-tals. Each patient was asked to complete out the MHQ, the DASH questionnaire, the satisfaction with their health-related quality of life (Sat-HRQOL) measure, and Chinese Health Questionnaire (CHQ), which is a measure of psychological stressors. Disability days were defined as the duration of restricted activities of daily living during the previous 4 weeks. Patients repeated the same questionnaires between 2 and 9 months after enrollment (average: 4 mo).
Results A total of 105 patients with hand injuries were recruited, and 50 of the 105 patients returned for the second evaluation. There were no statistical differences between responders and nonresponders for age, gender, disability days, the MHQ, the DASH questionnaire, the CHQ, or the Sat-HRQOL. Responsiveness was evaluated by effect sizes and standardized response means: Those for the MHQ were 0.84 and 1.05, and those for the DASH were 0.67 and 0.86, respectively. A mixed model analysis for repeated measurements of the 50 participants showed a significant influence of psychological factors (CHQ) for both the Sat-HRQOL and disability days. After adjustment for the effects of age, gender, and the CHQ, there was an increment of one Sat-HRQOL unit for an MHQ score increment of 3.2, whereas the score decrement for the DASH questionnaire was 3.3 units.
Conclusions The MHQ might be slightly more sensitive to functional changes, but the DASH questionnaire seemed more correlated with disability days. Psychological factors are the strongest determinants of the HRQOL and disability. (J Hand Surg 2010;35A:430–436. Copyright © 2010 by the American Society for Surgery of the Hand. All rights reserved.) Key words Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, hand injury, Michigan Hand Outcomes Questionnaire (MHQ), responsiveness.
From the Department of Physical Medicine and Rehabilitation, Buddhist Tzu Chi General Hospital, Taipei Branch, Taipei, Taiwan; Department of Medicine, Tzu Chi University, Hualien, Taiwan; Department of PhysicalMedicineandRehabilitation,EnChuKongHospital,Taipei,Taiwan;InstituteofOccupationMed-icine and Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan; and the Departments of Internal Medicine and Environmental and Occupational Medicine, National Taiwan University Hospital, Taipei, Taiwan.
Received for publication April 6, 2009; accepted in revised form November 18, 2009.
Supported by a grant from Tzu Chi General Hospital, Taipei Branch (TCRD-TPE-95-20), and partially supported by a grant from the National Science Council, Executive Yuan, Taiwan (95WFA0101282).
No benefits in any form have been received or will be received related directly or indirectly to the subject of this article.
The authors thank Jing-Hsiang Hwang, PhD, the statistician at Academia Sinica, for his invaluable assistance with the statistical methods and results.
Corresponding author: Jung-Der Wang, MD, Institute of Occupation Medicine and Industrial Hy-giene, College of Public Health, National Taiwan University, Taipei 100, Taiwan; e-mail:
0363-5023/10/35A03-0012$36.00/0 doi:10.1016/j.jhsa.2009.11.016
E
ARLY LITERATURE FOCUSED on developingstan-dardized methods for measuring impairment in dexterity, strength, and range of motion.1Recent literature has placed a greater emphasis on the impacts of patient-reported outcomes and the ability to function in daily life, although this kind of assessment can be challenging.2– 4Among the many instruments that have
been developed for the assessment of the disability status of the hands and upper extremities, two of the most well-known and frequently used tools are the Michigan Hand Outcomes Questionnaire (MHQ) and the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire. The MHQ is a questionnaire comprising a total of 37 hand-specific questions,5,6 whereas the DASH questionnaire features a 30-item scale relating to the upper extremities.7,8 Both have been validated in the evaluation of impairments, ac-tivity limitations, and participation restrictions to normal daily living activity.
It is both theoretically and clinically important to gain a complete understanding of the responsiveness and minimal important difference (MID) of these 2 measurement tools. Responsiveness refers to the ability of an instrument to detect clinically important changes over time and may thus be considered as an aspect of validity.9 Minimal important difference refers to the
smallest difference in a score that would be perceived by patients as being important, irrespective of whether it is beneficial or harmful, and which would, as a result, lead the treating clinician to consider a change in the patient’s current course of treatment.10,11
Although an in-depth investigation has already been performed regarding the comparative responsiveness of the MHQ and the DASH questionnaire after surgery on patients with carpal tunnel syndrome,12we could find no similar studies that have been conducted on patients with hand injuries. Because it has often been shown that the responsiveness of various outcome measures is pop-ulation-specific, we postulated that the MHQ may be more sensitive to functional changes in the hands, whereas the DASH questionnaire would have a closer association with disability days.
MATERIALS AND METHODS Data collection
The sample cohort for this study consisted of patients with hand injuries consecutively recruited from 2 com-munity hospitals. The patients were recruited 1 month or more after the occurrence of injury, when they were referred to receive rehabilitation therapy. The majority of the injuries were ruptures of flexor/extensor tendons
and fractures of hands, and about half of the injuries were work-related.
All of the subjects were invited to participate in the study on an entirely voluntary basis with prior informed consent having been obtained from each of the patients. Approval to carry out this study was provided by the institutional review board.
Each patient was asked to complete a set of ques-tionnaires, including the MHQ, the DASH question-naire, and the Chinese Health Questionnaire (CHQ), with the demographic data of the patients (including age, gender, and working status) also being recorded along with their medical histories. Disability days were defined as the duration of restricted activities of daily living during the previous 4 weeks due to hand injury.13,14 The patients were asked to rate their satisfaction with their health-related quality of life (Sat-HRQOL) using a visual analog scale.14,15 All participants received occupational therapy, and the length of rehabilitation varied according to the severity of the injury. The patients were followed up with the same questionnaire to evaluate changes in their disability status and HRQOL. The average fol-low-up time was 5 months⫾ 3 (range, 2 to 9 mo).
Michigan Hand Outcomes Questionnaire
The MHQ is a questionnaire composed of a total of 37 questions specifically related to the hand that are cate-gorized under the following six domains: (1) overall hand functioning; (2) activity of daily living; (3) pain; (4) work performance; (5) aesthetics; and (6) patient satisfaction with hand functioning.5,6
Each of the categories of the MHQ is subdivided into right- and left-hand–specific questions, with the excep-tions of the pain and the work performance categories. Activities of daily living are also divided into right- and left-hand–specific questions, in addition to a set of questions on bilateral task performance.
Disabilities of the Arm, Shoulder, and Hand questionnaire The DASH questionnaire is a 30-item scale that rel-ates to the upper extremities and is scored as a percent-age (where 0 indicates no problems). The majority of the questions are concerned with functional activities requiring use of the upper extremities, and the remain-ing questions include the followremain-ing: 2 items specifically relating to pain, 3 questions relating to other symptoms, 1 question that addresses social life, 1 directly related to work, 1 related to sleeping, and 1 that aims to determine the patients’ perceptions of their own capabilities.7,8
Satisfaction with health-related quality of life
The patients were asked to rate their Sat-HRQOL, a single measure of overall satisfaction in this domain, using a visual analog scale as the external criterion with scores ranging from 0 to 100; a score of 0 indicates the lowest level of satisfaction with health-related quality of life, and a score of 100 indicates the highest possible level of satisfaction.14,15
Chinese Health Questionnaire
The CHQ is a validated questionnaire for psychological illness that was derived from a Chinese translation of the General Health Questionnaire, with the addition of specially designed, culturally relevant items.16 The 4 categories of questions in the CHQ cover the assess-ment of (1) anxiety and depression; (2) the respondent’s concern over sleep disturbances; (3) somatic symptoms/ concerns; and (4) interpersonal difficulties.
The scoring method applied in this study involves a 0/1 alternative, with the total score for all items ranging between 0 and 12. This reflects a simple, nonweighted sum of the items, as endorsed by the respondent, with a higher (lower) score representing a greater (lesser) de-gree of emotional distress.16
Responsiveness
The responsiveness of each questionnaire is evaluated in this study using 2 different approaches, the first of which is a distribution-based methodology: This is per-formed by calculating the effect size (the mean change divided by the standard deviation [SD] of the baseline value), as well as the standardized response mean (SRM; the mean change divided by the SD of the change).9
The second approach, an anchor-based methodol-ogy, evaluates responsiveness by selecting the Sat-HRQOL and the number of disability days as the ex-ternal criteria.
Data and statistical analysis
Analysis of the data was performed for the following aspects: (1) responsiveness, including effect size and standardized response mean; (2) Pearson correlations between the scores of the MHQ, the DASH question-naire, the CHQ, the Sat-HRQOL, and the number of disability days; (3) the 95% confidence interval (CI) of the effect size and standardized response means, esti-mated by bootstrap methods; and (4) anchor-based methodology with the Sat-HRQOL and the number of disability days as the external criteria. Mixed effects models were constructed for repeated measurements of
the Sat-HRQOL instrument and disability days at initial and follow-up clinic visits; we also included age, gen-der, the CHQ, the DASH questionnaire, or the MHQ as fixed effects and appropriately adjusted the models. RESULTS
Initial-stage data
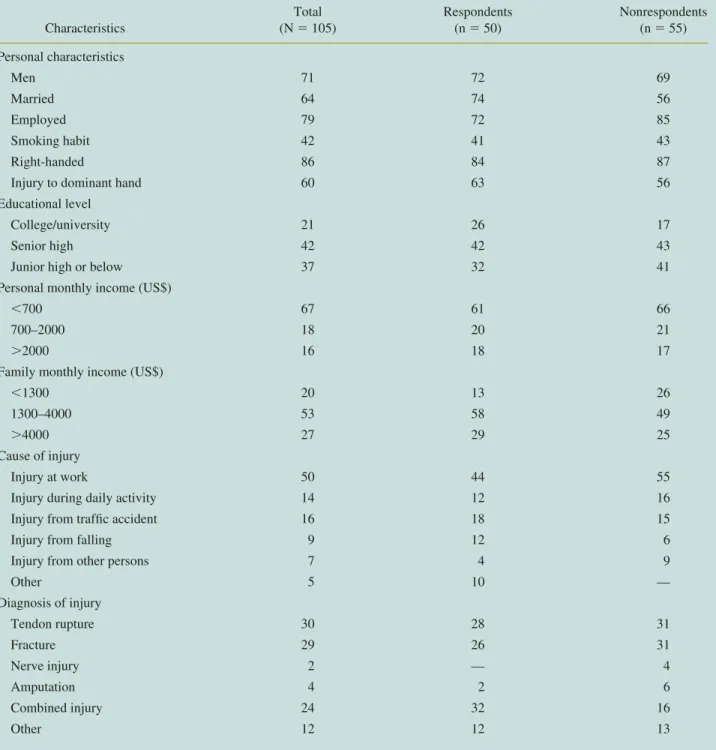
A total of 105 hand injury patients (74 men and 31 women) were recruited and completed the question-naire from the Departments of Physical Medicine and Rehabilitation in 2 community hospitals between 2004 and 2007. Fifty of the original 105 participants (36 men and 14 women) responded to the follow-up question-naire. Detailed demographic information on the sub-jects is provided inTable 1.
The mean age of the 50 participants in this study was 42 years⫾ 14, with 37 of 50 being married and 30 of 50 having sustained injuries to the dominant hand. Twenty-two of these patients’ injuries were directly attributable to their work. The mean number of disabil-ity days during the previous 4 weeks was 14 days⫾ 13, and the mean CHQ was 7.4⫾ 3.4.
Follow-up data
At the follow-up stage, the mean number of disability days during the previous 4 weeks was 6 days⫾ 12, and the mean CHQ was 6.7 ⫾ 3.7. Using t-test and chi-square analyses, we found no statistical differences between responders and nonresponders for age, gender, education level, dominant hand injury, disability days, the MHQ, the DASH questionnaire, the CHQ, or the Sat-HRQOL (as summarized inTable 1).
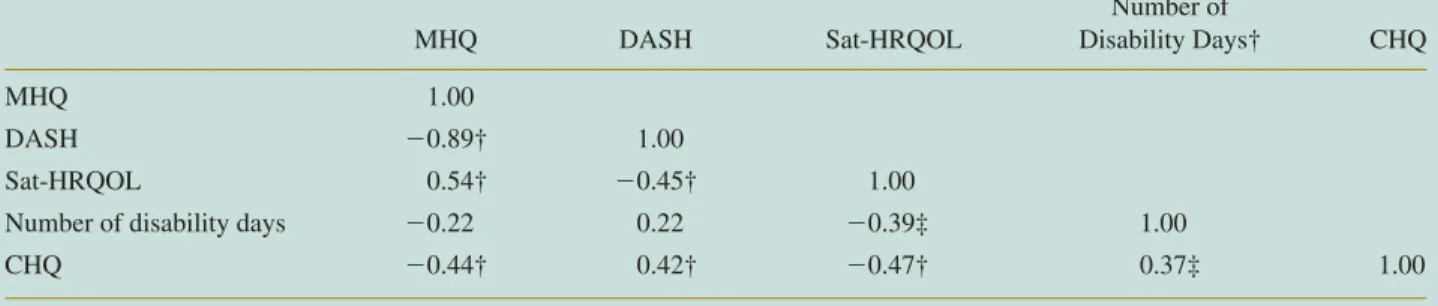
There were significant correlations among the MHQ, the DASH questionnaire, the CHQ, and the Sat-HRQOL, as summarized in Table 2. Among those, strong associations were discernible between the MHQ and the DASH questionnaire (r⫽ ⫺0.89, p ⬍ .01).
A comparison of the health status of the respondents at the initial and follow-up stages showed statistically significant improvements in the MHQ, DASH, and Sat-HRQOL scores (p⬍ .05). As shown inTable 3, the effect size for the MHQ was 0.84 (confidence interval [CI] 0.61, 1.18), and that for the DASH questionnaire was 0.67 (CI 0.41, 1.08); furthermore, the standardized response mean for the MHQ was 1.05 (CI 0.78, 1.42), and that for the DASH questionnaire was 0.86 (CI 0.60, 1.20).
The mixed model analyses, adjusted for the effects of age, gender, and the CHQ on the changes in the Sat-HRQOL, revealed coefficients of 0.31 for the MHQ and⫺0.30 for the DASH questionnaire (models I and II
inTable 4). Namely, an increase of 1 unit of the MHQ resulted in an elevation of 0.31 unit of the Sat-HRQOL, whereas that of the DASH corresponded with a de-crease of 0.30 unit. In other words, an MHQ score increment of 3.2 reduced the satisfaction of the HRQOL by 1, whereas the same effect was obtained for the DASH questionnaire with a score decrement of 3.3, indicating a similar magnitude of change in satisfaction with the quality of life for 1 unit change of these 2
instruments. In these 2 models, the CHQ was also a significant predictor for the HRQOL (p⬍ .01).
We also used a mixed model analysis to determine whether the scores of both instruments correlated with the number of disability days. However, the results revealed that only the CHQ (p⬍ .05) and the DASH (p⬍ .01) questionnaire were significant predictors for the number of disability days, whereas the MHQ was not (models III and IV inTable 4).
TABLE 1. Frequency Distribution (Percentages) of Demographic and Clinical Data for Hand Injury Patients Characteristics Total (N⫽ 105) Respondents (n⫽ 50) Nonrespondents (n⫽ 55) Personal characteristics Men 71 72 69 Married 64 74 56 Employed 79 72 85 Smoking habit 42 41 43 Right-handed 86 84 87
Injury to dominant hand 60 63 56
Educational level
College/university 21 26 17
Senior high 42 42 43
Junior high or below 37 32 41
Personal monthly income (US$)
⬍700 67 61 66
700–2000 18 20 21
⬎2000 16 18 17
Family monthly income (US$)
⬍1300 20 13 26
1300–4000 53 58 49
⬎4000 27 29 25
Cause of injury
Injury at work 50 44 55
Injury during daily activity 14 12 16
Injury from traffic accident 16 18 15
Injury from falling 9 12 6
Injury from other persons 7 4 9
Other 5 10 — Diagnosis of injury Tendon rupture 30 28 31 Fracture 29 26 31 Nerve injury 2 — 4 Amputation 4 2 6 Combined injury 24 32 16 Other 12 12 13
DISCUSSION
The results of this study reveal that the standardized response mean, at 1.05, and the effect size, at 0.84, of the MHQ are both larger than those for the DASH questionnaire (standardized response mean, 0.86; effect size, 0.67). This means that the MHQ may be better able to reflect the changes in scores. Similar findings were reported in a study that examined these 2 instru-ments in the setting of carpal tunnel syndrome.12We
hypothesize that the increased responsiveness of the MHQ arises because (1) the MHQ is specific to the hand, whereas the DASH questionnaire is a general arm instrument; and (2) the MHQ assesses at least 4 sepa-rate domains for each hand, whereas the DASH ques-tionnaire does not.
However, the previous study found that the pain domain seemed to be the most responsive for the
MHQ,12but as shown inTable 3, our study found that work performance appeared to be the most responsive. Such a divergence may be attributable to the rapid improvement in pain and numbness after surgery for carpal tunnel syndrome, whereas comprehensive im-provements in hand functioning, as opposed to changes in sensation, would be experienced by patients with hand injuries after rehabilitation.
In this study, 30 of the 50 participants had high psychological stress (CHQ score⬎5). This implies that patients with hand injuries suffer more frequently from emotional distress than do Chinese high school students (67 of 471 subjects; CHQ score⬎5).17We also found that both the MHQ and the DASH questionnaire had moderate correlations with the CHQ (Table 2), and the mixed model analysis revealed that the CHQ was a significant predictor for both the Sat-HRQOL and the TABLE 2. Correlation Matrix Between the MHQ, the DASH Questionnaire, the Sat-HRQOL, the CHQ, and the Number of Disability Days Among Hand Injury Patients*
MHQ DASH Sat-HRQOL Number of Disability Days† CHQ MHQ 1.00 DASH ⫺0.89† 1.00 Sat-HRQOL 0.54† ⫺0.45† 1.00
Number of disability days ⫺0.22 0.22 ⫺0.39‡ 1.00
CHQ ⫺0.44† 0.42† ⫺0.47† 0.37‡ 1.00
*Total sample number⫽ 50. †Significance at the .01 level. ‡Significance at the .05 level (2-tailed).
TABLE 3. Responsiveness of the MHQ and the DASH Questionnaire Among Hand Injury Patients Returning for Re-evaluation*
Variables
Initial Score Follow-Up Score Observed Change
Effect Size
Standardized Response Mean Mean (1) SD Mean (2) SD Mean (2) – (1) SD
DASH† 31.0 19.1 18.3 18.8 ⫺12.7 14.7 0.67 0.86
MHQ† 47.4 18.7 63.2 21.1 15.8 15.0 0.84 1.05
Function† 44.6 24.8 58.8 25.0 14.4 21.2 0.59 0.68
Activities of daily living (ADL)† 52.1 29.0 72.2 24.2 20.1 24.5 0.69 0.82
Work† 34.3 27.3 57.6 28.7 23.3 23.8 0.85 0.98
Pain 38.1 22.6 29.0 22.7 ⫺9.1 24.2 0.40 0.38
Aesthetics† 53.4 20.2 63.3 22.9 9.9 23.9 0.49 0.41
Satisfaction† 38.4 24.5 54.4 26.6 16.1 20.5 0.66 0.78
*Total sample number⫽ 50.
number of disability days (Table 4). These results imply that psychological factors not only play an important role when patients rate their subjective HRQOL but that they also influence the subject’s self-evaluation of the extent of his or her disability. Thus, the future care of patients with upper extremity injuries must also take into account their psychological health in addition to function improvement.
There is still a general lack of consensus on any gold standard for the effective estimation of responsiveness and MID for patient-reported outcomes.11 The stan-dardized response mean may be a more statistically efficient index of responsiveness than effect size, as it takes into account the variability in change over time by applying the pooled variances of mean differences.18 Nevertheless, a statistically significant divergence in the scores has no direct link with clinical importance, as there is no intuitive meaning of the standard deviation units.19Anchor-based methods may have better corre-lations with clinical changes. Because the Sat-HRQOL and the number of disability days are generally consid-ered as clinically important by patients and health care professionals, we adopted the Sat-HRQOL and the number of disability days as the anchor.
The results of the mixed model analyses revealed that the magnitude of change in the Sat-HRQOL for a single unit change in the MHQ is 0.31 unit, whereas that for a single unit change in the DASH questionnaire is⫺0.30 unit. As all 3 instruments have a scale of 0 to 100, the minimal differences in the DASH question-naire and the MHQ may indicate a similar magnitude of change for a unit of subjective score change, with about 3 score units linked to 1 unit of satisfaction in the quality of life. The MHQ and the DASH questionnaire may have similar linkages to the HRQOL as a result of the following: (1) the strong correlation between the MHQ and the DASH questionnaire; and (2) moderate
correlation among the MHQ, the DASH questionnaire, the CHQ, and the Sat-HRQOL. Some patients with hand injuries might have activity restrictions not only to their hand and wrist but also to their elbow and shoulder because of long-term immobilization. The strong cor-relation suggests that the DASH, a more function-oriented instrument, may be a good alternative for eval-uating patients with hand injury.
However, the number of disability days might not directly reflect the severity of hand disability. As found in a prior study conducted with patients with chronic musculoskeletal pain, depression and anxiety could have adverse effects on pain severity, functional limi-tations, disability days, and HRQOL.20 The disability days are largely explained by psychosocial factors and environmental support, especially for those disabled from work.
Thus, compared with the MHQ, the DASH question-naire appears to have better correlation with the changes in disability days; it is also shorter in length and there-fore probably easier to handle in terms of the total amount of time required to complete and score the questionnaire. However, it would appear that the MHQ is slightly more sensitive to clinical changes, particu-larly if the focus is solely on hand functioning. Because it contains 6 domains, it can be scored individually, thereby helping clinicians to more easily detect a pa-tient’s major problems.
Because both instruments are shown to be relatively responsive to patients with carpal tunnel syndrome,12 this study consecutively recruited patients with many different types of hand injuries, as summarized inTable 1. Although the follow-up time has a wide range, the responsiveness of the MHQ and the DASH question-naire were evaluated simultaneously for each patient, and we only inquired about the number of disability days for the past 4 weeks. We directly analyzed the TABLE 4. Multiple Regression Coefficients (ˆ ⴞ Standard Error of ˆ) Based on Construction of a Mixed Model for the Sat-HRQOL and Disability Days for 50 Follow-Up Patients
Predictors
Sat-HRQOL Disability Days
Model I Model II Model III Model IV
ˆ ⫾ SE ˆ ˆ ⫾ SE ˆ ˆ ⫾ SE ˆ ˆ ⫾ SE ˆ
MHQ 0.31⫾ 0.06* ⫺0.05 ⫾ 0.07
DASH ⫺0.30 ⫾ 0.07* 0.18⫾ 0.07†
CHQ ⫺0.77 ⫾ 0.35† ⫺0.82 ⫾ 0.36† 1.09⫾ 0.39* 0.92⫾ 0.36†
Akaike’s information criterion (AIC) 731.6 755.1 664.5 674.4
SE, standard error.
correlation coefficient between the number of disability days and the duration of follow-up, which showed ⫺0.22 (p ⫽ .22). The negative sign of the correlation coefficient implies that the patients with a longer period of follow-up did not seem to show a larger number of disability days, or no association between these 2 vari-ables on this sample. The diversified diagnoses pro-vided us with a broader range of evaluation for patients with many types of injuries, but our results may differ from those of studies focusing on 1 specific type of injury, due to the heterogeneity of patients, or may be less likely to demonstrate responsiveness to disability days.
The patients in this study were recruited from the Departments of Physical Medicine and Rehabilitation in 2 community hospitals, and given that only 50 of the 105 participants responded to the follow-up question-naire, we should remain cautious in any attempts to generalize our findings to other establishments as they may not be appropriate for clinics under widely differ-ent settings. However, as there were no significant differences between the respondent and nonrespon-dent groups in the results for the MHQ, the DASH questionnaire, or the disability days, it appears that our conclusions may also be applicable to those patients who did not return for follow-up.
The results revealed that the MHQ might be slightly more sensitive to functional changes, but the DASH questionnaire seemed more correlated with disability days. Psychological factors are the strongest determi-nants of HRQOL and disability days. Using anchor-based methodology, we have demonstrated that an MHQ score increment of 3.2 units would increase sat-isfaction with the HRQOL by 1 unit, whereas that for the DASH questionnaire would correspond with a dec-rement of 3.3 units.
REFERENCES
1. Courtney TK, Webster BS. Disabling occupational morbidity in the United States: an alternative way of seeing the Bureau of Labor Statistics data. J Occup Environ Med 1999;41:60 – 69.
2. Harlan LC, Harlan WR, Parsons PE. The economic impact of inju-ries: a major source of medical costs. Am J Public Health 1990;80: 453– 459.
3. Blair SJ, McCormick E, Bear-Lehman J, Fess EE, Rader E. Function
of impairment of the upper extremity. Clin Orthop Relat Res 1987;221:42–58.
4. Ultee J, van Neck JW, Jaquet JB, Hovius SER. Difficulties in conducting a prospective outcome study. Hand Clin 2003;19:457– 462.
5. Chung KC, Pillsbury MS, Walters MR, Hayward RA. Reliability and validity testing of the Michigan Hand Outcomes Questionnaire (MHQ). J Hand Surg 1998;23A:575–587.
6. Chung KC, Arbor A, Wei FC. An outcome study of thumb recon-struction using microvascular toe transfer. J Hand Surg 2000;25A: 651– 658.
7. Hudak PL, Amadio PC, Bombardier C, the Upper Extremity Col-laborative Group. Development of an upper extremity outcome mea-sure: the DASH (Disabilities of the Arm, Shoulder and Hand). Am J Ind Med 1996;29:602– 608.
8. Liang HW, Wang HK, Yao G, Horng YS, Hou SM. Psychometric evaluation of the Taiwan version of the Disability of the Arm, Shoulder, and Hand (DASH) questionnaire. J Formos Med Assoc 2004;103:773–779.
9. Hays RD, Hadorn D. Responsiveness to change: an aspect of valid-ity, not a separate dimension. Qual Life Res 1991;1:73–75. 10. U.S. Food Drug Administration. Guidance for industry.
Patient-reported outcome measures: use in medical product development to support labeling claims. Available at: http://www.fda.gov/cder/ guidance/5460dft.pdf, 06/14/2006. Accessed on April 14, 2007. 11. Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for
determining responsiveness and minimally important differences for patient-reported outcome. J Clin Epidemiol 2008;61:102–109. 12. Kotsis SV, Chung KC. Responsiveness of the Michigan Hand
Out-comes Questionnaire and the Disabilities of the Arm, Shoulder and Hand questionnaire in carpal tunnel surgery. J Hand Surg 2005;30A: 81– 86.
13. Patrick DL, Deyo RA, Atlas SJ, Singer DE, Chapin A, Keller RB. Assessing health-related quality of life in patients with sciatica. Spine 1995;20:1899 –1909.
14. Horng YS, Hwang YH, Wu HC, Liang HW, Jang Y, Twu FC, et al. Predicting health-related quality of life in patients with low back pain. Spine 2005;30:551–555.
15. Hsiung PC, Fang CT, Chang YY, Chen MY, Wang JD. Comparison of WHOQOL-BREF and SF-36 in patients with HIV infection. Qual Life Res 2005;14:141–150.
16. Cheng TA, Williams P. The design and development of a screening questionnaire (CHQ) for use in community studies of mental disor-ders in Taiwan. Psychol Med 1986;16:415– 422.
17. Cho CY, Hwang IS, Chen CC. The association between psycho-logical distress and musculoskeletal symptoms experienced by Chinese high school students. J Orthop Sports Phys Ther 2003; 33:344 –353.
18. Hevey D, McGee HM. The effect size statistic. J Health Psychol 1998;3:163–170.
19. Copay AG, Subach BR, Glassman SD, Polly DW, Schuler TC. Understanding the minimum clinically important difference: a re-view of concepts and methods. Spine J 2007;7:541–546.
20. Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Associa-tion of depression and anxiety alone and in combinaAssocia-tion with chronic musculoskeletal pain in primary care patients. Psychosom Med 2008;70:890 – 897.