High Prevalence and Low Awareness of CKD in Taiwan: A Study on the Relationship Between Serum Creatinine and Awareness From
a Nationally Representative Survey
Chih-Cheng Hsu, MD, DrPH, Shang-Jyh Hwang, MD, Chi-Pang Wen, MD, DrPH, Hsing-Yi Chang, DrPH, MPH, Ted Chen, PhD, MPH, Ruei-Shiang Shiu, MA,
Shiow-Shiun Horng, MD, Yu-Kang Chang, MA, and Wu-Chang Yang, MD
● Background: The burden of chronic kidney disease (CKD) is a global challenge. Empirical evidence of low CKD awareness rates in developed countries speaks for an urgent need to strengthen strategies for CKD identification and prevention. The aim of this study is to estimate the awareness rate of CKD in Taiwan to promote early detection of CKD in this country. Methods: Data from a nationally representative survey were used for analysis. The study included 6,001 subjects. The simplified Modification of Diet in Renal Disease equation was used to define glomerular filtration rate (GFR) and CKD stages according to criteria of the US National Kidney Foundation.
Descriptive methods were used to analyze data. Results: The prevalence of CKD stages 3 to 5 in Taiwan is 6.9%
(95% confidence interval, 4.4 to 9.4). Awareness rates for CKD in Taiwan are low: 8.0% for individuals with stage 3, 25.0% for those with stage 4, and 71.4% for those with stage 5. Awareness rate is related closely to serum creatinine level: those with creatinine levels greater than 1.6 mg/dL (>141mol/L) are more likely to be informed of having a kidney disease. Conclusion: The high prevalence and low awareness of CKD in Taiwan explicitly show the need to advocate more strongly for CKD prevention and education for both physicians and the populace. Establishment of a mandated automatic GFR reporting system may be the first priority we need to accomplish in Taiwan to improve kidney well-being. Am J Kidney Dis 48:727-738.
© 2006 by the National Kidney Foundation, Inc.
INDEX WORDS: Chronic kidney disease (CKD); CKD awareness; serum creatinine; Taiwan.
T
HE INCREASING PREVALENCE of end- stage renal disease (ESRD) is a global challenge. In the United States, it is claimed that chronic renal diseases are the nation’s ninth leading cause of death,1and it was estimated that health care for patients with ESRD will cost$28.3 billion annually by 2010.2 In the United Kingdom, the annual incidence of ESRD has doubled during the past decade.3 In Taiwan, chronic renal diseases have been the eighth lead- ing cause of death since 1997.4 Dialysis alone consumes about 7.21% of Taiwan’s annual bud- get for national health insurance, with only a small proportion (0.15%) of the population need- ing treatment.5 Both the incidence and preva- lence of ESRD in Taiwan are among the highest in the world.6 The epidemiological pattern of ESRD in Taiwan, although not worse than in other developed countries, has adverse impacts not only on the population’s health, but also as a financial burden on the nation.
Among many reasons contributing to the high prevalence and incidence of ESRD in Taiwan, the high prevalence of chronic kidney disease (CKD) may be one of the most important factors.
Yang et al7reported that the point prevalence of CKD stages 3 to 5 in Taiwan was 6.43%, which was much greater than that in the United States
(the prevalence of CKD stages 3 to 4 in the United States was 3.83% to 4.39%, estimated by the National Health and Nutrition Examination Survey [NHANES III] data8). In the face of the high prevalence of CKD, 1 effective strategy for
From the Center for Health Policy Research and Develop- ment, National Health Research Institutes, Zhunan; Depart- ment of Medicine, Division of Nephrology, Kaohsiung Medi- cal University Hospital and College of Medicine, Kaohsiung;
Department of Health, Division of Adult and Elderly Health, Bureau of Health Promotion, Taichung; Department of Medi- cine, Division of Nephrology, Taipei Veterans General Hos- pital and National Yang-Ming University School of Medi- cine, Taipei, Taiwan, ROC; and Department of Community Health Science, School of Public Health and Tropical Medi- cine, Tulane University, New Orleans, LA.
Received March 24, 2006; accepted in revised form July 10, 2006.
Originally published online as doi:10.1053/j.ajkd.2006.07.018 on October 3, 2006.
Support: This work was supported by the National Health Research Institutes’ research grant (HD-PP-14). Potential conflicts of interest: None.
Address reprint requests to Wu-Chang Yang, MD, Divi- sion of Nephrology, Department of Medicine, Taipei Veter- ans General Hospital, 201 Shih-Pai Rd, Sec 2, Taipei, Taiwan 11217. E-mail: wcyang@vghtpe.gov.tw
© 2006 by the National Kidney Foundation, Inc.
0272-6386/06/4805-0005$32.00/0 doi:10.1053/j.ajkd.2006.07.018
American Journal of Kidney Diseases, Vol 48, No 5 (November), 2006: pp 727-738 727
Taiwan to lighten the burden of ESRD would be to prevent those with CKD from progressing to ESRD. Recognizing the importance of CKD prevention, the US National Kidney Foundation also strongly recommends that people at risk for CKD (such as those with diabetes, hypertension, or family history of CKD) be screened and provided with an individualized risk-reduction plan.9 However, it seems that worldwide, the task to make both health providers and popu- lace pay enough attention to increase CKD identification and awareness has not been ac- complished.
According to several studies10,11 from the United States, low awareness among CKD pa- tients is common in American society. Nickolas et al12 thus warned the medical community of possible failure with regard to the mechanism to identify patients with CKD and educate patients with CKD to be aware of their kidney disease. To our knowledge, there are few published reports, especially from outside the United States, of CKD identification and/or awareness. The pur- poses of this report are to estimate the CKD awareness rate in Taiwan and propose an unde- manding approach to possibly facilitate CKD identification and increase CKD awareness.
METHODS Subjects
In 2001, the National Health Research Insti- tutes and Bureau of Health Promotion in Taiwan conducted the National Health Interview Survey (NHIS) to assess health behaviors, quality of life (evaluated by using the Medical Outcomes Study 36-Item Short-Form Health Survey [SF-36] ques- tionnaire13), and medical utilization for noninsti- tutionalized civilians in Taiwan. Detailed sam- pling methods of the NHIS are described in another report.14 Basically, the NHIS was con- ducted using a multistage stratified systematic sampling scheme. The researchers first divided 359 townships/districts of Taiwan into 7 strata according to their geographic location and de- gree of urbanization. Townships or districts (first- stage primary sampling units) in each stratum were selected by using the method of probability proportional to sizes. In each selected township/
district, the second-stage sampling units, lins (the smallest administration unit in Taiwan), also were selected by using the same method of probability
proportional to sizes. In total, 1,648 lins were selected. Four households were assigned ran- domly from each selected lin. All members in selected households were interviewed. Alto- gether, 6,592 households (26,658 individuals) were sampled from the entire Taiwan area.
In 2002, another project, the Taiwanese Sur- vey on Blood Sugar, Blood Lipids and Blood Pressure (TW3H), was initiated to estimate the prevalence of hypertension and diabetes, as well as lipid profiles, for people in Taiwan. Participants in the TW3H were drawn from a subsample of the 2001 NHIS. Because implementing a biomar- ker screening for all NHIS participants was not affordable, one half of the NHIS chosen town- ships/districts were randomly selected for the TW3H. When the townships/districts were deter- mined, all original NHIS-selected lins, house- holds, and individuals within the selected town- ships/districts were included in the TW3H. The finalized study population of the TW3H was 10,292 individuals. Of these subjects, who came from 3,296 households in 824 lins, 7,578 (73.6%) completed TW3H interviews and 6,600 (64.1%) permitted blood pressure and other biomarker measurements. Residents in military services, medical facilities, boarding schools, job training centers, dormitories, and prisons and residents of mountainous areas and offshore islands were excluded from the TW3H. The major reason for nonparticipation in the TW3H was declining to undergo biomarker measurement, by 1,775 indi- viduals. Other reasons for nonparticipation in- cluded the following: army service (n⫽ 157), living or studying overseas (n ⫽ 378), death (n⫽ 24), and inability to make contact (n ⫽ 7).
Differences in sex were not statistically signifi- cant between those completing the TW3H and nonparticipants. Because the incidence and preva- lence of CKD are very low for people younger than 20 years, we selected those who were not younger than 20 years as our study subjects.
Subjects met the following inclusion criteria:
(1) 20 years or older, (2) previously inter- viewed for the NHIS conducted in 2001, and (3) provided informed consent for biomarker measurements. Total number of study subjects was 6,001. We also linked participants’ medical utilization data from the National Health Insur- ance archives (2002) for those (n⫽ 5,409) who
signed informed consent to allow researchers to do so.
Data Collection
To ensure study quality, all interviews in the NHIS and TW3H were conducted by well- trained and experienced interviewers under a standardized protocol and close supervision. De- mographic data for participants were based on self-reports during household interviews in the NHIS. Arterial blood pressure was measured by using a mercury sphygmomanometer after study subjects sat for at least 15 minutes. Systolic blood pressure was recorded as the first percep- tion of successive sounds. Diastolic blood pres- sure was marked at the complete disappearance of sound (Korotkoff phase V). Blood pressure was measured twice, with an interval of 5 min- utes between each measurement. The mean of these 2 measurements was recorded.
Venous blood after overnight fasting for at least 12 hours was collected to measure biomark- ers. All blood samples were kept well frozen at
⫺20°C and transported by express delivery to a central laboratory for analysis. Hemoglobin A1c was checked by using high-performance liquid chromatography (TOSOH G7; Fisher Scientific International Inc, Hampton, NH). Fasting plasma glucose, triglycerides, total cholesterol, blood urea nitrogen, and creatinine (Cr) were measured by using an automatic analyzer (VITROS750;
Johnson & Johnson, New Brunswick, NJ). Low- density lipoprotein cholesterol and high-density lipoprotein cholesterol were measured by means of electrophoresis assay (HELENA REP; Helena Laboratories, Beaumont, TX). To ensure laboratory quality, interassay coefficient of variation was cal- culated in the data collection period. High and low coefficient of variation values for specific biomark- ers were as follows: 1.03% to 1.58% (5.75⫾ 0.06 and 2.15⫾ 0.03 mg/dL) for Cr; 1.43% to 1.99%
(45.9⫾ 0.66 and 14.8 ⫾ 0.29 mg/dL) for blood urea nitrogen; 0.61% to 1.32% (261.60⫾ 1.60 and 79.30 ⫾ 1.05 mg/dL) for fasting glucose;
0.83% to 0.93% (184.00 ⫾ 1.71 and 89.00 ⫾ 0.74 mg/dL) for triglycerides; 0.95% to 1.03%
(262.00⫾ 2.49 and 129.00 ⫾ 1.33 mg/dL) for total cholesterol; 2.31% to 2.85% (138.90 ⫾ 3.21 and 66.60⫾ 1.90 mg/dL) for low-density lipoprotein cholesterol; and 2.26% to 2.52%
(56.10 ⫾ 1.27 and 24.30 ⫾ 0.61 mg/dL) for high-density lipoprotein cholesterol.
Variable Definitions and Statistical Analysis Late CKD. The simplified Modification of Diet in Renal Disease (MDRD) equation15was used to estimate glomerular filtration rate (GFR).
Based on clinical practice guidelines recom- mended by the Kidney Disease Outcomes Qual- ity Initiative (KDOQI) of the Nation Kidney Foundation,16we classified those with GFR less than 60 mL/min/1.73 m2(⬍1.00 mL/s/1.73 m2) as persons with CKD. Those with GFR of 30 to 59 mL/min/1.73 m2(0.50 to 0.98 mL/s/1.73 m2) were categorized as CKD stage 3 (389 subjects);
GFR of 15 to 29 mL/min/1.73 m2 (0.25 to 0.48 mL/s/1.73 m2), as CKD stage 4 (16 sub- jects); and GFR less than 15 mL/min/1.73 m2 (⬍0.25 mL/s/1.73 m2), as CKD stage 5 (7 sub- jects). We subdivided the group with CKD stage 3 into CKD stage 3A for those with GFR of 45 to 59 mL/min/1.73 m2(0.75 to 0.98 mL/s/1.73 m2) and CKD stage 3B for those with GFR of 30 to 44 mL/min/1.73 m2(0.50 to 0.73 mL/s/1.73 m2).
CKD awareness. Those who self-reported they had been told by a physician or health care professional that they had weak or failing kid- neys are defined as persons being aware of hav- ing kidney problems.
Persons who have diabetes. Study subjects are defined as having diabetes if they self-reported that they had been told by a doctor or health care professional that they had diabetes, were adminis- tered hypoglycemic agents to control blood glu- cose levels, or their fasting blood glucose level was greater than 126 mg/dL (⬎7.0 mmol/L).
Persons who have hypertension. Study sub- jects are defined as having hypertension if they self-reported that they had been told by a physi- cian or health care professional that they had hypertension, were administered antihyperten- sive agents to control blood pressure, or had blood pressure greater than 140/90 mm Hg.
Prevalence (number of events divided by total observations) is used to describe the percentage of study subjects with CKD and percentage of subjects with CKD being aware of having kidney disease. The NHIS sampling design resulted in an equal probability sample.14Comparisons be- tween the sample and population data indicated that the sample was representative of the nation.
AWARENESS OF CHRONIC KIDNEY DISEASE IN TAIWAN 729
Estimation of design effects also showed they were close to 1. Therefore, this set of data can be treated as samples from a simple random sample, and we do not have to adjust a design effect in prevalence estimation. Chi-square and t-tests were used to analyze categorical and continuous vari- ables, respectively. Statistical analyses were per- formed using SAS 8.01 (SAS Institute Inc, Cary, NC). All reported P are 2 sided; P less than 0.05 is considered statistically significant.
RESULTS
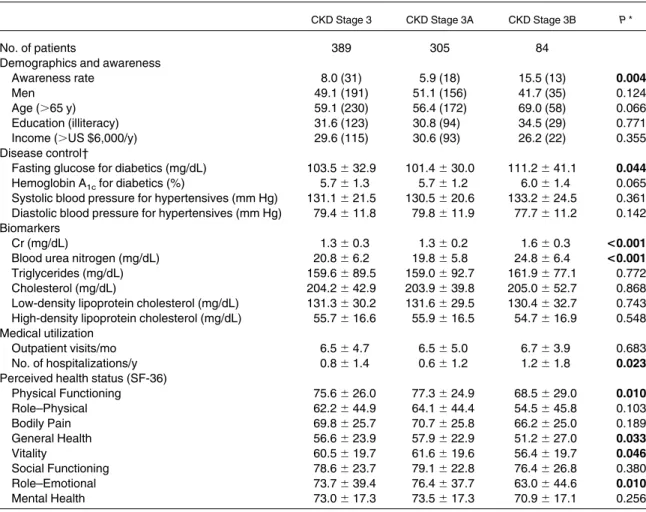
Table 1lists demographic characteristics, bio- chemical profiles, medical utilization, and per- ceived health status of study subjects with stage 3 CKD. There is no sex discrepancy; however, most subjects (⬃60%) were older than 65 years.
About one third of subjects with CKD in this study were illiterate and had no personal income.
About 8% of subjects in this group had been told by health professionals they had a certain kidney
Table 1. Characteristics of Study Subjects With Stage 3 CKD and Differences Between Subgroups With CKD Stages 3A and 3B
CKD Stage 3 CKD Stage 3A CKD Stage 3B P *
No. of patients 389 305 84
Demographics and awareness
Awareness rate 8.0 (31) 5.9 (18) 15.5 (13) 0.004
Men 49.1 (191) 51.1 (156) 41.7 (35) 0.124
Age (⬎65 y) 59.1 (230) 56.4 (172) 69.0 (58) 0.066
Education (illiteracy) 31.6 (123) 30.8 (94) 34.5 (29) 0.771
Income (⬎US $6,000/y) 29.6 (115) 30.6 (93) 26.2 (22) 0.355
Disease control†
Fasting glucose for diabetics (mg/dL) 103.5⫾ 32.9 101.4⫾ 30.0 111.2⫾ 41.1 0.044
Hemoglobin A1cfor diabetics (%) 5.7⫾ 1.3 5.7⫾ 1.2 6.0⫾ 1.4 0.065
Systolic blood pressure for hypertensives (mm Hg) 131.1⫾ 21.5 130.5⫾ 20.6 133.2⫾ 24.5 0.361 Diastolic blood pressure for hypertensives (mm Hg) 79.4⫾ 11.8 79.8⫾ 11.9 77.7⫾ 11.2 0.142 Biomarkers
Cr (mg/dL) 1.3⫾ 0.3 1.3⫾ 0.2 1.6⫾ 0.3 <0.001
Blood urea nitrogen (mg/dL) 20.8⫾ 6.2 19.8⫾ 5.8 24.8⫾ 6.4 <0.001
Triglycerides (mg/dL) 159.6⫾ 89.5 159.0⫾ 92.7 161.9⫾ 77.1 0.772
Cholesterol (mg/dL) 204.2⫾ 42.9 203.9⫾ 39.8 205.0⫾ 52.7 0.868
Low-density lipoprotein cholesterol (mg/dL) 131.3⫾ 30.2 131.6⫾ 29.5 130.4⫾ 32.7 0.743 High-density lipoprotein cholesterol (mg/dL) 55.7⫾ 16.6 55.9⫾ 16.5 54.7⫾ 16.9 0.548 Medical utilization
Outpatient visits/mo 6.5⫾ 4.7 6.5⫾ 5.0 6.7⫾ 3.9 0.683
No. of hospitalizations/y 0.8⫾ 1.4 0.6⫾ 1.2 1.2⫾ 1.8 0.023
Perceived health status (SF-36)
Physical Functioning 75.6⫾ 26.0 77.3⫾ 24.9 68.5⫾ 29.0 0.010
Role–Physical 62.2⫾ 44.9 64.1⫾ 44.4 54.5⫾ 45.8 0.103
Bodily Pain 69.8⫾ 25.7 70.7⫾ 25.8 66.2⫾ 25.0 0.189
General Health 56.6⫾ 23.9 57.9⫾ 22.9 51.2⫾ 27.0 0.033
Vitality 60.5⫾ 19.7 61.6⫾ 19.6 56.4⫾ 19.7 0.046
Social Functioning 78.6⫾ 23.7 79.1⫾ 22.8 76.4⫾ 26.8 0.380
Role–Emotional 73.7⫾ 39.4 76.4⫾ 37.7 63.0⫾ 44.6 0.010
Mental Health 73.0⫾ 17.3 73.5⫾ 17.3 70.9⫾ 17.1 0.256
NOTE. Results expressed as percent (number) or mean⫾ SD. CKD stage 3A, GFR between 45 and 59 mL/min/1.73 m2; CKD stage 3B, GFR is between 30 and 44 mL/min/1.73 m2. Values given in bold identify statistically significant differences.
To convert fasting glucose in mg/dL to mmol/L, multiply by 0.056; Cr in mg/dL tomol/L, multiply by 88.4; blood urea nitrogen in mg/dL to mmol/L, multiply by 0.357; triglycerides in mg/dL to mmol/L, multiply by 0.0113; cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol in mg/dL to mmol/L, multiply by 0.02586.
*P indicates the chance to reject null hypotheses that no difference in demographics or other indicators between people with GFRs of 30 to 44 mL/min/1.73 m2and 45 to 60 mL/min/1.73 m2, by using chi-square tests (for categorical data) or t-tests (for continuous data).
†Indicators for disease control: patients with hemoglobin A1cfor those with diabetes (n⫽ 75) and measurements of systolic and diastolic blood pressure for those with hypertension (n⫽ 198).
disease. Table 1 also lists differences between those with CKD stage 3A (GFR, 45 to 59 mL/min/
1.73 m2[0.75 to 0.98 mL/s/1.73 m2]) and CKD stage 3B (GFR, 30 to 44 mL/min/1.73 m2[0.50 to 0.73 mL/s/1.73 m2]). Compared with subjects with CKD stage 3A, those with CKD stage 3B had significantly greater levels of blood Cr (P⬍ 0.001) and urea nitrogen (P⬍ 0.001), twice the annual number of hospitalizations (1.2 versus 0.6; P⫽ 0.023), and lower SF-36 scores, espe- cially in the dimensions of Physical Functioning (P⫽ 0.010), General Health (P ⫽ 0.033), Vital- ity (P ⫽ 0.046), and Role–Emotional (P ⫽ 0.010). Those with CKD stage 3B also tended to have poorer diabetic control (P ⫽ 0.044) and were more likely to be informed about their renal illness (P⫽ 0.004).
Figure 1 shows prevalences of late CKD in Taiwan and the United States (data were adopted
from NHANES III, estimated by Coresh et al8).
Overall, about 6.9% (95% confidence interval [CI], 4.4 to 9.4) of the population in Taiwan has late CKD (stages 3 to 5). The prevalence of late CKD increases when people get old. Persons older than 60 years particularly are at greater risk for deteriorating renal function. Prevalences of stage 3 CKD are 3.4% (95% CI, 0 to 7.4), 21.1%
(95% CI, 14.4 to 27.8), and 31.0% (95% CI, 23.6 to 38.4) for Taiwanese aged 40 to 59, 60 to 69, and 70 plus years, respectively. Compared with the prevalence in the United States, the preva- lence of CKD in Taiwan is significantly greater for those aged 60 to 69 years.
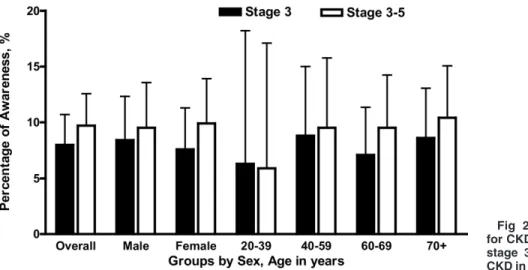
As shown inFig 2, only 9.7% (95% CI, 6.8 to 12.6) of subjects with late CKD were aware of having CKD. The low CKD awareness rates were observed across different sex and age groups.
Fig 1. Comparison of prevalences of stage 3 CKD between Taiwan and the United States by sex and age groups (US data estimated by NHANES III8).
Fig 2. Awareness rates for CKD among people with stage 3 and stages 3 to 5 CKD in Taiwan.
AWARENESS OF CHRONIC KIDNEY DISEASE IN TAIWAN 731
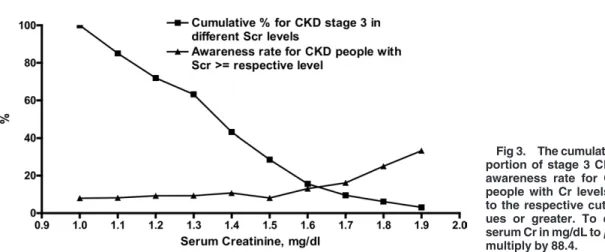
Figure 3 shows cumulative proportion and awareness rates for subjects with stage 3 CKD at different serum Cr cutoff levels. Awareness rates remained at approximately 10% or less until serum Cr level reached 1.6 mg/dL (141mol/L).
After passing this critical point, awareness rates increased to a peak at approximately 33.3%
when serum Cr level was 1.9 mg/dL or greater (ⱖ168mol/L). Conversely, the cumulative pro- portion of stage 3 CKD was 15.7% for those with Cr levels of 1.6 mg/dL or greater (ⱖ141mol/
L). The 50th percentile of Cr level for subjects with stage 3 CKD was 1.35 mg/dL (119mol/
L), which means that less than 50% of subjects with stage 3 CKD would have a Cr level greater than 1.4 mg/dL (⬎124mol/L), the point fre- quently used by clinicians to decide impaired renal function.
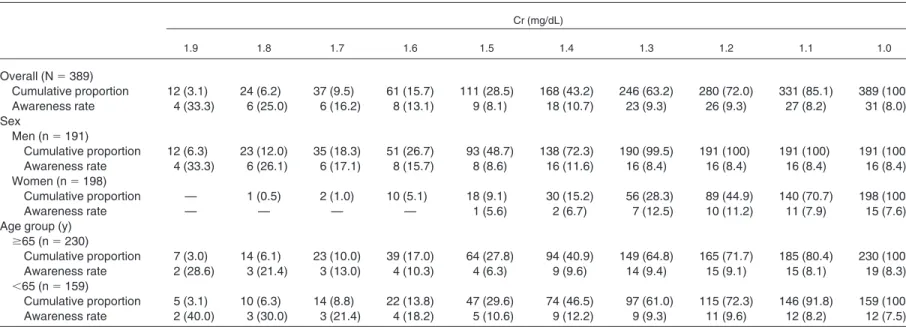
More detailed information about cumulative proportion and awareness rates of stage 3 CKD is listed in Table 2. In the same CKD category (stage 3), Cr levels in women generally were less than those in men (48.7% of men with stage 3 CKD had Cr levelsⱖ 1.5 mg/dL [ⱖ133mol/
L], but 55.1% of women with stage 3 CKD had Cr levels⬍ 1.2 mg/dL [⬍106mol/L]). Gener- ally speaking, women with stage 3 CKD tended to be less likely than their male counterparts to learn about their kidney disease. Compared with people older than 65 years, younger people had greater awareness rates when Cr levels were greater than 1.4 mg/dL (⬎124mol/L).
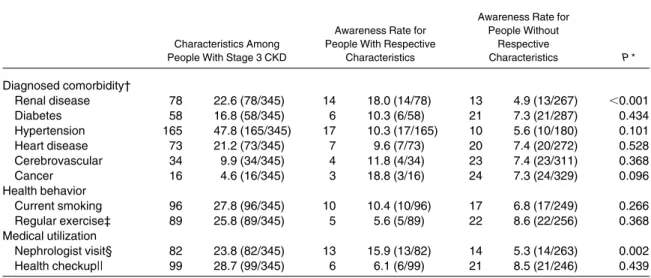
Table 3 lists characteristics of subjects with stage 3 CKD and compares awareness rates between those with and without certain comor- bidities and health behaviors. The most frequent
comorbidity found in subjects with stage 3 CKD was hypertension (47.8%). Only 22.6% of sub- jects with stage 3 CKD had renal disease diag- nosed in the previous year. About one fourth of subjects with stage 3 CKD had visited nephrolo- gists in the previous year. Current smokers or regular exercisers accounted for about one fourth of subjects with stage 3 CKD (27.8% and 25.8%, respectively). Those with renal disease diag- nosed and those who visited nephrologists in the previous year were significantly more likely to know about their kidney disease than those who had not (P⬍ 0.001 and P ⫽ 0.002, respectively).
Conversely, comorbidities and health behaviors generally did not impact on CKD awareness rates.
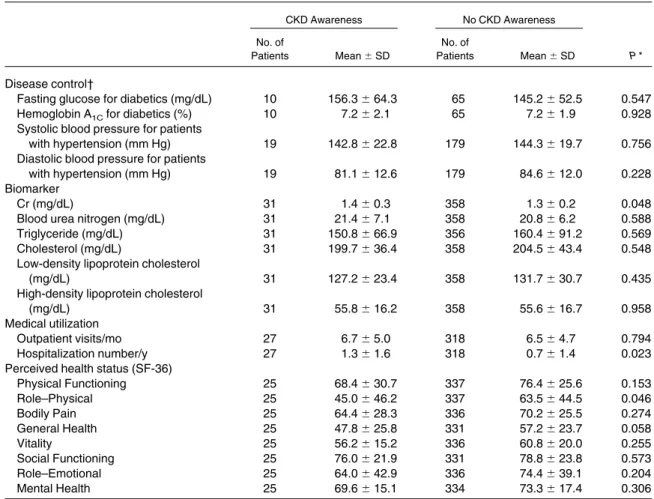
A comparison between awareness and un- awareness groups in stage 3 CKD samples is listed inTable 4. Serum Cr levels of the aware- ness group were significantly greater than those of the unawareness group (1.4 mg/dL [124mol/L]
versus 1.3 mg/dL [115 mol/L]; P ⫽ 0.048).
Although statistically not significant, CKD aware- ness may result in better lipid control for people with CKD (including total cholesterol, low- density lipoprotein cholesterol, and triglyceride levels) and better blood pressure control for those who have CKD and hypertension. Those who are aware of their renal problems also had greater hospitalization rates (annual admission numbers per person, 1.3 versus 0.7; P⫽ 0.023) and lower perceived health status (SF-36 scores generally were lower in the awareness group, especially in the dimensions of Role–Physical [45.0 versus 63.5; P⫽ 0.046] and General Health [47.8 versus 57.2; P⫽ 0.058]).
Fig 3. The cumulative pro- portion of stage 3 CKD and awareness rate for CKD in people with Cr levels equal to the respective cutoff val- ues or greater. To convert serum Cr in mg/dL tomol/L, multiply by 88.4.
Table 2. Cumulative Proportion of Stage 3 CKD and Awareness Rate for People With CKD Who Had Cr Levels Equal to Respective Cutoff Value or Greater by Sex and Age Group
Cr (mg/dL)
1.9 1.8 1.7 1.6 1.5 1.4 1.3 1.2 1.1 1.0
Overall (N⫽ 389)
Cumulative proportion 12 (3.1) 24 (6.2) 37 (9.5) 61 (15.7) 111 (28.5) 168 (43.2) 246 (63.2) 280 (72.0) 331 (85.1) 389 (100)
Awareness rate 4 (33.3) 6 (25.0) 6 (16.2) 8 (13.1) 9 (8.1) 18 (10.7) 23 (9.3) 26 (9.3) 27 (8.2) 31 (8.0)
Sex
Men (n⫽ 191)
Cumulative proportion 12 (6.3) 23 (12.0) 35 (18.3) 51 (26.7) 93 (48.7) 138 (72.3) 190 (99.5) 191 (100) 191 (100) 191 (100)
Awareness rate 4 (33.3) 6 (26.1) 6 (17.1) 8 (15.7) 8 (8.6) 16 (11.6) 16 (8.4) 16 (8.4) 16 (8.4) 16 (8.4)
Women (n⫽ 198)
Cumulative proportion — 1 (0.5) 2 (1.0) 10 (5.1) 18 (9.1) 30 (15.2) 56 (28.3) 89 (44.9) 140 (70.7) 198 (100)
Awareness rate — — — — 1 (5.6) 2 (6.7) 7 (12.5) 10 (11.2) 11 (7.9) 15 (7.6)
Age group (y) ⱖ65 (n ⫽ 230)
Cumulative proportion 7 (3.0) 14 (6.1) 23 (10.0) 39 (17.0) 64 (27.8) 94 (40.9) 149 (64.8) 165 (71.7) 185 (80.4) 230 (100)
Awareness rate 2 (28.6) 3 (21.4) 3 (13.0) 4 (10.3) 4 (6.3) 9 (9.6) 14 (9.4) 15 (9.1) 15 (8.1) 19 (8.3)
⬍65 (n ⫽ 159)
Cumulative proportion 5 (3.1) 10 (6.3) 14 (8.8) 22 (13.8) 47 (29.6) 74 (46.5) 97 (61.0) 115 (72.3) 146 (91.8) 159 (100)
Awareness rate 2 (40.0) 3 (30.0) 3 (21.4) 4 (18.2) 5 (10.6) 9 (12.2) 9 (9.3) 11 (9.6) 12 (8.2) 12 (7.5)
NOTE. N⫽ 389. Values expressed as number (percent). Cumulative proportion is cumulative frequency divided by total number in a specific group (overall, different sex or age groups). Awareness rate is the cumulative number for people with CKD being aware of their kidney problems divided by the cumulative frequency in the specific Cr cutoff points. To convert Cr in mg/dL tomol/L, multiply by 88.4.
AWARENESSOFCHRONICKIDNEYDISEASEINTAIWAN733
DISCUSSION
Taiwan and the United States are the 2 coun- tries in the world that have the greatest incidence and prevalence of ESRD.6The high prevalence of CKD may contribute significantly to the high incidence and prevalence of ESRD in Taiwan.
The prevalence pattern also indicates that per- sons older than 60 years in Taiwan should be the target population for renal function screening to make diagnoses and give treatments early enough to prevent CKD complications.
This study shows that CKD awareness rates in Taiwan are low: 8.0% (95% CI, 5.3 to 10.7) for people with stage 3, 25.0% (95% CI, 3.8 to 46.2) for people with stage 4, and 71.4% (95% CI, 37.9 to 100) for people with stage 5 (data for stages 4 and 5 are not shown). Although this study may not be able to ensure accurate awareness rates in the advanced CKD (stages 4 and 5) population because of its small sample size, the awareness rate for people with stage 3 is much less than that
in their American counterparts (Nickolas et al12 estimated 22.0% for stage 3). Inadequacy of CKD diagnosis and low CKD awareness also are mentioned frequently in the literature,17-20 but such a low CKD detection rate justifies immediate scrutiny, response, and action in a country with a high CKD prevalence, such as Taiwan.
Why is the CKD awareness rate in Taiwan so low? Physicians apparently have to take major responsibility for this. It is not convincing that physicians in Taiwan generally are familiar with CKD guidelines (KDOQI)16to identify patients when only 22.6% of subjects with stage 3 CKD in our study population had kidney-related dis- eases (International Classification of Diseases, Ninth Revision, codes 250.4, 403 to 404, or 580 to 599) diagnosed in their National Health Insur- ance records (Table 3).
As also listed in Table 3, a total of 99 study subjects with stage 3 CKD had undergone peri-
Table 3. Awareness and Characteristics of People With Stage 3 CKD Who Agreed to Disclose Their National Health Insurance Records
Characteristics Among People With Stage 3 CKD
Awareness Rate for People With Respective
Characteristics
Awareness Rate for People Without
Respective
Characteristics P * Diagnosed comorbidity†
Renal disease 78 22.6 (78/345) 14 18.0 (14/78) 13 4.9 (13/267) ⬍0.001
Diabetes 58 16.8 (58/345) 6 10.3 (6/58) 21 7.3 (21/287) 0.434
Hypertension 165 47.8 (165/345) 17 10.3 (17/165) 10 5.6 (10/180) 0.101
Heart disease 73 21.2 (73/345) 7 9.6 (7/73) 20 7.4 (20/272) 0.528
Cerebrovascular 34 9.9 (34/345) 4 11.8 (4/34) 23 7.4 (23/311) 0.368
Cancer 16 4.6 (16/345) 3 18.8 (3/16) 24 7.3 (24/329) 0.096
Health behavior
Current smoking 96 27.8 (96/345) 10 10.4 (10/96) 17 6.8 (17/249) 0.266
Regular exercise‡ 89 25.8 (89/345) 5 5.6 (5/89) 22 8.6 (22/256) 0.368
Medical utilization
Nephrologist visit§ 82 23.8 (82/345) 13 15.9 (13/82) 14 5.3 (14/263) 0.002
Health checkup|| 99 28.7 (99/345) 6 6.1 (6/99) 21 8.5 (21/246) 0.439
NOTE. n⫽ 345. Values expressed as number (second, fourth, sixth columns) and percent (third, fifth, seventh columns).
*P indicates the chance to reject the hypothesis that no difference in awareness rates exists for people with or without certain characteristics by using chi-square tests.
†Definition of diagnosed comorbidity: for those signing an informed consent form to release their medical utilization records, we assume they have the respective comorbidity if they had a diagnosis of the following diseases in the 2002 National Health Insurance Archives: renal disease (International Classification of Diseases, Ninth Revision [ICD-9], 250.4, 403 to 404, 580 to 599), diabetes (ICD-9, 250, 357.2, 362.0, 366.41), hypertension (ICD-9, 362.11, 401 to 405, 437.2), heart disease (ICD-9, 398, 402, 410 to 411, 428), cerebrovascular accident (ICD-9, 342, 430 to 437), and cancer (ICD-9, 140 to 208, 230 to 234).
‡Those who exercised at least 3 times a week, 30 minutes per time, and continued to do so for at least 3 months.
§Those who have visited (at least 1 visit) nephrologists’ clinics in 2002 (data retrieved from the 2002 National Health Insurance Archives).
||Those who had a health checkup (including renal function evaluation) during the previous year.
odical health checkups (including renal function evaluation through serum Cr level) in the previ- ous year, but only 6.1% were informed of having renal problems. People undergoing periodical health checkups usually have to visit a primary care physician for physical examination and lab- oratory interpretation, but the low awareness rate indicates that primary care physicians may not be able to identify patients with stage 3 CKD based on the laboratory report in hand.
Furthermore, also listed in Table 3, CKD awareness rates in high-risk groups with chronic morbidities (eg, diabetes, hypertension, cardio- vascular or cerebrovascular diseases) are not at a satisfactory level, although awareness rates are
greater than in patients without these chronic diseases. Patients with these chronic morbidities usually are cared for by respective specialists on a regular basis, but these patients are not knowl- edgeable about their kidney condition, even when GFR deteriorated to less than 60 mL/min/1.73 m2 (⬍1.0 mL/s), indicating that specialists in Taiwan also may not pay enough attention to their pa- tients’ renal function.
Physicians (including primary care physicians and specialists other than nephrologists) usually use serum Cr as the biomarker to evaluate renal function. It is easy and simple; however, GFR, the most reliable indicator to reflect kidney func- tion, is not determined by serum Cr level alone.
Table 4. Comparison of Glucose Levels, Blood Pressure, Lipid Control, Medical Utilization, and SF-36 Scores Between the CKD Awareness and Unawareness Groups
CKD Awareness No CKD Awareness
P * No. of
Patients Mean⫾ SD
No. of
Patients Mean⫾ SD Disease control†
Fasting glucose for diabetics (mg/dL) 10 156.3⫾ 64.3 65 145.2⫾ 52.5 0.547
Hemoglobin A1Cfor diabetics (%) 10 7.2⫾ 2.1 65 7.2⫾ 1.9 0.928
Systolic blood pressure for patients
with hypertension (mm Hg) 19 142.8⫾ 22.8 179 144.3⫾ 19.7 0.756
Diastolic blood pressure for patients
with hypertension (mm Hg) 19 81.1⫾ 12.6 179 84.6⫾ 12.0 0.228
Biomarker
Cr (mg/dL) 31 1.4⫾ 0.3 358 1.3⫾ 0.2 0.048
Blood urea nitrogen (mg/dL) 31 21.4⫾ 7.1 358 20.8⫾ 6.2 0.588
Triglyceride (mg/dL) 31 150.8⫾ 66.9 356 160.4⫾ 91.2 0.569
Cholesterol (mg/dL) 31 199.7⫾ 36.4 358 204.5⫾ 43.4 0.548
Low-density lipoprotein cholesterol
(mg/dL) 31 127.2⫾ 23.4 358 131.7⫾ 30.7 0.435
High-density lipoprotein cholesterol
(mg/dL) 31 55.8⫾ 16.2 358 55.6⫾ 16.7 0.958
Medical utilization
Outpatient visits/mo 27 6.7⫾ 5.0 318 6.5⫾ 4.7 0.794
Hospitalization number/y 27 1.3⫾ 1.6 318 0.7⫾ 1.4 0.023
Perceived health status (SF-36)
Physical Functioning 25 68.4⫾ 30.7 337 76.4⫾ 25.6 0.153
Role–Physical 25 45.0⫾ 46.2 337 63.5⫾ 44.5 0.046
Bodily Pain 25 64.4⫾ 28.3 336 70.2⫾ 25.5 0.274
General Health 25 47.8⫾ 25.8 331 57.2⫾ 23.7 0.058
Vitality 25 56.2⫾ 15.2 336 60.8⫾ 20.0 0.255
Social Functioning 25 76.0⫾ 21.9 331 78.8⫾ 23.8 0.573
Role–Emotional 25 64.0⫾ 42.9 336 74.4⫾ 39.1 0.204
Mental Health 25 69.6⫾ 15.1 334 73.3⫾ 17.4 0.306
NOTE. To convert fasting glucose in mg/dL to mmol/L, multiply by 0.056; Cr in mg/dL tomol/L, multiply by 88.4; blood urea nitrogen in mg/dL to mmol/L, multiply by 0.357; triglycerides in mg/dL to mmol/L, multiply by 0.0113; cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol in mg/dL to mmol/L, multiply by 0.02586.
*P indicates the chance to reject null hypotheses in chi-square tests (for categorical data) or t-tests (for continuous data).
†Indicators for disease control: hemoglobin A1cfor those with diabetes and systolic and diastolic blood pressure for those with hypertension.
AWARENESS OF CHRONIC KIDNEY DISEASE IN TAIWAN 735
To improve accuracy, equations frequently used in estimating GFR (eg, MDRD15,21 and Cock- croft-Gault22 formulae) are formulated with Cr level and other biomarkers, such as blood urea nitrogen and albumin levels, as well as several important parameters, such as age, sex, and race.
Therefore, using Cr level alone to estimate renal function often could cause underdiagnosis of CKD, especially in women and the elderly.23As shown inFig 3 andTable 2, overall awareness rates generally are not greater than 10% until Cr level reaches 1.6 mg/dL (141mol/L), but the cumulative proportion of CKD greater than this level (those with Cr⬎ 1.6 mg/dL [⬎141mol/L]) is less than 20%, indicating that most people with stage 3 CKD will be told they have normal renal function if their Cr level is less than 1.6 mg/dL (⬍141 mol/L). As listed in Table 2, more than 90% of females with stage 3 CKD have a Cr level less than 1.5 mg/dL (⬍133
mol/L). The gap in Cr levels between males and females also was described in other stud- ies.8,23If physicians do not incorporate sex as a variable to adjust their reading of serum Cr value, the natural disparity of Cr values between men and women could easily make physicians overlook initial renal impairment in women. This sex discrepancy at least partially explains why CKD awareness rates for women usually are lower than for men.
Cr level, which is lacking in good correspon- dence to GFR, as shown in this study, deserves a new interpretation. Otherwise, CKD diagnosis will be delayed and CKD awareness cannot be improved. First, continuing education for pri- mary care physicians and physicians in other specialties should emphasize the importance of CKD and how to unravel the meanings of Cr levels. Second, to minimize physicians’ uninten- tional negligence, the authors advocate that pa- thology laboratories be required to report GFR and Cr level simultaneously. Reporting GFR is not an unachievable task for regular pathology laboratories. For example, using the simplified MDRD formula,21 laboratories have to collect only 3 basic profiles from patients (age, sex, and race [black or not]) to convey GFR information, which is superior to Cr level alone in helping physicians determine a patient’s renal condition.
Recognizing the importance of GFR information in helping clinical decision making, Coresh et al8
of the Johns Hopkins Medical Institutes (Balti- more, MD), the US National Kidney Founda- tion,9and the Australasian Creatinine Consensus Working Group24also strongly advocated setting up a mandated laboratory system for automatic reporting of GFR to detect CKD at an early stage. Akbari et al25 of the Ottawa Health Re- search Institute also showed clear evidence that automatic laboratory reporting of GFR com- bined with a CKD-related educational program for family physicians can significantly increase the CKD detection rate in the primary care set- ting (the rate increased from 22.4% to 85.1%).
Advocacy for increasing CKD awareness is important and beneficial to both physicians and patients because it can remind physicians to prescribe available remedies to prevent CKD complications26and also may encourage patients to adopt healthier lifestyles or strategies condu- cive to slowing disease progression.27,28 Our study shows (Table 4) that CKD awareness gen- erally is associated with worse perceived physi- cal, mental, and social health status, especially for the Role–Physical and General Health dimen- sions of the SF-36. Thus, health providers should learn how to empathetically deliver understand- able explanations and provide available preven- tion strategies to patients. However, this study also shows that the awareness group seems not yet ready to adopt healthy lifestyles (eg, preva- lences of smoking and regular exercise were not significantly different between the awareness and unawareness groups; data not shown). It is obvi- ous that patient education related to CKD preven- tion, treatment, and self-care should be strength- ened to improve CKD prognosis in Taiwan.
Several limitations are found generically in this study. Because this is a cross-sectional inter- view study, we cannot ensure that all identified subjects with CKD had persistently impaired renal function for at least 3 months (KDOQI definition9). By conducting only a 1-time screen- ing, we may have overestimated late CKD preva- lence in Taiwan. The association between 2 vari- ables in this cross-sectional survey cannot be inferred to be a causal relationship, and recall biases cannot be prevented.
Because of small sample size (n⫽ 23; 0.4% of total samples) in the advanced-CKD group (stages 4 or 5), we could not reliably conduct statistical analysis for this group. Thus, in this study, we
focus on delineating characteristics of subjects with stage 3 CKD.
The NHIS and TW3H screening projects were not conducted for the purpose of a CKD survey;
therefore, the original screening test did not include checking for proteinuria or microalbumin- uria. Without data from these urinary function tests, we cannot specify the diagnosis of early CKD (stages 1 and 2).16 Using the simplified MDRD formula to calculate GFR and then esti- mate CKD prevalence may cause bias because this equation was developed by using only pa- tients with CKD.29Zuo et al30recently reported that the Cockcroft-Gault equation24 could be relatively useful in the Chinese population, but the self-reported weight and height collected in this study may induce more bias. The prevalence of CKD stage 3 in Taiwan would be as high as 15.3% (data not shown) by applying the Cock- croft-Gault equation to estimate GFR. We may need more epidemiological studies to validate such a high prevalence. In addition, the aware- ness rate is even lower (5.0%; data not shown) if we use the Cockcroft-Gault equation to identify patients with CKD stage 3. To minimize measure- ment errors, we decided to use the simplified MDRD formula to calculate GFR in this study.
Moreover, the question “Have you ever been told by a doctor or health care professional of weak or failing kidneys?” by which we defined CKD awareness in this study was not checked for its validity in Taiwan. However, because the same question was used in the NHANES to estimate CKD awareness for the US popula- tion,8,12 we believe this question is acceptable and also comparable across nations. Finally, we may have slightly underestimated the awareness rate in this study because the awareness question was asked in the NHIS survey (conducted in late 2001), about 6 months ahead of biomarker screen- ing in the TW3H project (conducted in early 2002). Therefore, some subjects might have been free of CKD (and thus legitimately unaware of having kidney disease) during the NHIS inter- view, but their renal function might have been impaired when serum Cr was checked. However, we do not think 6 months is long enough to have significantly distorted the results.
The high CKD prevalence, but low awareness rate, among people with CKD is a warning call for the Taiwan Medical Society to revise and
reinforce CKD prevention policies, which should at least include effective screening strategies for high-risk groups, patient education programs to attach importance to effects of CKD on health, health providers’ reorientation to draw their pro- active attention to CKD identification and care, and, last, but not least, service mandates to require pathology laboratories to report GFR (eg, by using the simplified MDRD formula) when- ever they are to report the serum Cr level.
ACKNOWLEDGMENT
The authors thank Dr Kung-Yee Liang, the acting presi- dent of the National Health Research Institutes in Taiwan, for his inspiring encouragement and visionary comments on the study.
REFERENCES
1. Arias E, Anderson RN, Kung HC, et al: Deaths: Final data for 2001. Natl Vital Stat Rep 52:1-115, 2003
2. Xue JL, Ma JZ, Louis TA, et al: Forecast of the number of patients with end-stage renal disease in the United States to the year 2010. J Am Soc Nephrol 12:2753-2758, 2001
3. The Renal Association: UK Renal Registry. The Sixth Annual Report, 2003. Available at:http://www.renalreg.com/
Report 2003/Cover3_Frames.htm.Accessed May 29, 2006 4. Department of Health: Health and Viral Statistics Re- public of China 2002. Taiwan, ROC, Department of Health, 2002
5. Department of Health: National Health Insurance An- nual Statistical Report. Taiwan, ROC, Department of Health, 2003
6. US Renal Data System: USRDS 2005 Annual Data Report. Available at: http://www.usrds.org/2005/pdf/02_
incid_prev_05.pdf.Accessed June 15, 2006
7. Yang WC, Hwang SC, Ng YY, et al: A huge burden of stage III-V chronic kidney disease in Taiwan: A national prevalence estimate from TW3H QC monitoring. National Kidney Foundation 2005 Spring Clinical Meetings, Washing- ton, DC, 2005 (abstr 262)
8. Coresh J, Byrd-Holt D, Astor BC, et al: Chronic kidney disease awareness, prevalence, and trends among US adults, 1999 to 2000. J Am Soc Nephrol 16:180-188, 2005
9. National Kidney Foundation: K/DOQI Clinical Prac- tice Guidelines for Chronic Kidney Disease: Evaluation, classification, and stratification. Am J Kidney Dis 39:S1- S266, 2002 (suppl 1)
10. St Peter WL, Schoolwerth AC, McGowan T, et al:
Chronic kidney disease: Issues and establishing programs and clinics for improved patient outcomes. Am J Kidney Dis 41:903-924, 2003
11. Levin A: Identification of patients and risk factors in chronic kidney disease—Evaluating risk factors and thera- peutic strategies. Nephrol Dial Transplant 16:S57-S60, 2001 (suppl 7)
12. Nickolas TL, Frisch GD, Opotowsky AR, et al: Aware- ness of kidney disease in the US population: Findings from the National Health and Nutrition Examination Survey
AWARENESS OF CHRONIC KIDNEY DISEASE IN TAIWAN 737
(NHANES) 1999 to 2000. Am J Kidney Dis 44:185-197, 2004
13. Steward A, Ware J: Measuring Functioning and Well- Being: The Medical Outcomes Study Approach. Durham, NC, Duke University, 1992
14. Shih YT, Hung YT, Chang HY, et al: The design, contents, operation and the characteristics of the respondents of the 2001 National Health Interview Survey in Taiwan.
Taiwan J Public Health 22:419-430, 2003
15. Levey AS, Bosch JP, Lewis JB, et al: A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130:461- 470, 1999
16. Levey AS, Coresh J, Balk E, et al: National Kidney Foundation practice guidelines for chronic kidney disease:
Evaluation, classification, and stratification. Ann Intern Med 139:137-147, 2003
17. Obrador GT, Ruthazer R, Arora P, et al: Prevalence of and factors associated with suboptimal care before initiation of dialysis in the United States. J Am Soc Nephrol 10:1793- 1800, 1999
18. Kausz AT, Khan SS, Abichandani R, et al: Manage- ment of patients with chronic renal insufficiency in the northeastern United States. J Am Soc Nephrol 12:1501- 1507, 2001
19. Duncan L, Heathcote J, Djurdjev O, et al: Screening for renal disease using serum creatinine: Who are we miss- ing? Nephrol Dial Transplant 16:1042-1046, 2001
20. Nissenson AR, Collins AJ, Hurley J, et al: Opportuni- ties for improving the care of patients with chronic renal insufficiency: Current practice patterns. J Am Soc Nephrol 12:1713-1720, 2001
21. Levey AS, Greene T, Kusek JW, et al: A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol 11:155A, 2000 (abstr A0828) 22. Cockcroft DW, Gault MH: Prediction of creatinine clearance from serum creatinine. Nephron 16:31-41, 1976
23. Perrone RD, Madias NE, Levey AS: Serum creatinine as an index of renal function: New insights into old con- cepts. Clin Chem 38:1933-1953, 1992
24. Mathew TH: Chronic kidney disease and automatic reporting of estimated glomerular filtration rate: A position statement. Med J Aust 183:138-141, 2005
25. Akbari A, Swedko PJ, Clark HD, et al: Detection of chronic kidney disease with laboratory reporting of esti- mated glomerular filtration rate and an educational program.
Arch Intern Med 164:1788-1792, 2004
26. Snively CS, Gutierrez C: Chronic kidney disease:
Prevention and treatment of common complications. Am Fam Physician 70:1921-1928, 2004
27. Thomas LK, Sargent RG, Michels PC, et al: Identifi- cation of the factors associated with compliance to therapeu- tic diets in older adults with end stage renal disease. J Ren Nutr 11:80-89, 2001
28. Milas NC, Nowalk MP, Akpele L, et al: Factors associated with adherence to the dietary protein intervention in the Modification of Diet in Renal Disease Study. J Am Diet Assoc 95:1295-1300, 1995
29. Rule AD, Gussak HM, Pond GR, et al: Measured and estimated GFR in healthy potential kidney donors. Am J Kidney Dis 43:112-119, 2004
30. Zuo L, Ma YC, Zhou YH, et al: Application of GFR-estimating equations in Chinese patients with chronic kidney disease. Am J Kidney Dis 45:463-472, 2005