Open Access
Research article
Triple negative breast carcinoma is a prognostic factor in
Taiwanese women
Che Lin
1, Su-Yu Chien
2, Li-Sheng Chen
1, Shou-Jen Kuo
1, Tsai-Wang Chang*
3and Dar-Ren Chen*
1Address: 1Comprehensive Breast Cancer Center, Changhua Christian Hospital, Changhua, Taiwan, 2Department of Pharmacology, Changhua
Christian Hospital, Changhua, Taiwan and 3Department of General Surgery, National Cheng Kung University Hospital, Tainan, Taiwan
Email: Che Lin - [email protected]; Su-Yu Chien - [email protected]; Li-Sheng Chen - [email protected]; Shou-Jen Kuo - [email protected]; Tsai-Wang Chang* - [email protected]; Dar-Ren Chen* - [email protected] * Corresponding authors
Abstract
Background: Currently, there is a debate as to whether triple negative breast carcinoma (TNBC) has a worse prognosis than non-TNBC. Our aim was to determine whether TNBC is a prognostic factor for survival.
Methods: We identified 1,048 Taiwanese breast carcinoma patients, of whom 167 (15.9%) had TNBC. Data used for analysis were derived from our cancer registry database for women with breast cancer who were diagnosed between 2002 January and 2006 December.
Results: In the Kaplan-Meier analysis, tumor subgroup (TNBC vs. non-TNBC) was a prognosis factor related to 5-year overall survival. In the univariate analysis, tumor subgroup (TNBC vs. non-TNBC) was a significant factor related to 5-year overall survival, in addition to age, tumor size, lymph node, metastasis, grade, stage, estrogen receptor status, progesterone receptor status, and HER2 overexpression status. In the multivariate analysis, tumor subgroup was not a significant factor related to 5-year disease-free survival (DFS). In node-positive patients, tumor subgroup was a significant factor related to 5-year overall survival, in addition to age, tumor size, metastasis, and grade. In node-negative patients, tumor subgroup was not a significant factor related to 5-year disease-free survival and 5-year overall survival.
Conclusion: Our results indicated that TNBC patients in Taiwan have worse 5-year overall survival than non-TNBC patients. Notably, in node-positive patients, TNBC played a prognostic role in 5-year overall survival.
Background
Many oncologists think breast cancer is a clinically heter-ogeneous disease with different responses to treatment and outcomes [1,2]. Sixty to 80% of tumors are positive for the estrogen receptor (ER) and/or progesterone (PgR), and 20% to 40% have her2/neu (HER2) gene
over-expres-sion [1]. Interestingly, some recent data suggested that tri-ple negative breast carcinomas (TNBC), ER-negative, PgR-negative and HER2-PgR-negative exhibited different clinical outcomes [3,4]. However, there is uncertainty about the appropriate survival role for TNBC. Information on the TNBC subtype is still limited and confusing in adjuvant
Published: 18 June 2009
BMC Cancer 2009, 9:192 doi:10.1186/1471-2407-9-192
Received: 31 October 2008 Accepted: 18 June 2009 This article is available from: http://www.biomedcentral.com/1471-2407/9/192
© 2009 Lin et al; licensee BioMed Central Ltd.
chemotherapies [4-15]. Liedtke revealed that patients with TNBC have increased pathologic complete response rates (pCR) compared with non-TNBC patients, and those with pCR have excellent survival [3]. Liedtke also demon-strated that patients with residual disease after neoadju-vant chemotherapy have significantly worse survival if they have TNBC compared with non-TNBC, particularly in the first 3 years. Because these studies were done in the other countries, their findings might not apply to Taiwan. In this study, we sought to determine the risk associated with TNBC in Taiwan.
Therefore, the aim of this study was to determine the prog-nostic significance of TNBC with respect to disease-free survival (DFS) and overall survival in a group of homoge-neously-treated Taiwanese breast carcinoma patients.
Methods
Patients were identified from the databases of the cancer registry at Changhua Christian Hospital, which is located in central Taiwan. Data collection for cancer in this medi-cal center began in 1986 and continued until 2009. The well-trained case managers used the registry software and collected uniform information about all patients with breast cancer who had been examined at least once as out-patients or inout-patients in the daily clinical service. This study was approved by the institutional review board of Changhua Christian Hospital (IRB number: 080325). The baseline data included demographic characteristics (e.g., age), tumor characteristics (e.g., tumor size, positivity of lymph node, metastasis, grade, pathologic stage, ER/PgR/ HER2 information and histology). Patients with ductal carcinoma in situ only were excluded. The data underwent a variety of editing checks and procedures, so as to omit duplicate records. The quality of the cancer registry data-base was reviewed and approved by the committee, which consisted of radiologists, oncologists, pathologists, sur-geons and epidemiologists with special expertise in breast cancer.
Tumor size was determined on the basis of pathological reports from the Changhua Christian Hospital. The Bloom-Richardson grading system was used for tumor grading. This grading scheme is based on three morpho-logic features: degree of tumor tubule formation, tumor mitotic activity, and nuclear pleomorphism of tumor cells. Seven possible scores are condensed into three Bloom-Richardson grades: I, II, or III. Staging in this study was presented by the American Joint Committee on Can-cer stage group.
Immunohistochemistry (IHC) analysis was performed on formalin-fixed, paraffin-embedded breast cancer tissue. The ER and PgR analysis was based on a IHC assay, in which a report of 10% or greater of cells that had nuclear
staining for ER was considered a positive result as well as PgR. IHC was performed with anti-ER (NeoMarkers, clone: SP1, dilution: 1:200, Fermont, California) and anti-PgR antibody (NeoMarkers, clone:SP2, dilution: 1:250, Fermont, California) by an autostaining system (Ventana Medical Systems, Tucson, Arizona).
Breast cancer tumors were classified as HER2-positive if they demonstrated HER2 gene amplification using the flu-orescence in-situ hybridization method, or were scored as 3+ by an IHC method. HER2 IHC only used cell mem-brane localization to interpret (Dako, Carpinteria, Cali-fornia). The intensity of the membrane staining was defined by a semiquantitative score (0 to 3+). Tumor staining was compared to staining of normal breast epi-thelium from the same patient as a negative control. For clinical purposes, 3+ staining, defined as uniform and intense membrane staining in more than 30% of invasive breast cancer cells, was considered overexpression. No staining or weak incomplete membrane staining was con-sidered a negative result.
Data used for analysis were derived from the cancer regis-try database of women with breast cancer who were diag-nosed between 2002 January and 2006 December. Data for analysis started from 2002, because there was a lack of information on HER2 in patients before 2002. DFS was defined as freedom from breast cancer recurrence or breast death. Overall survival was defined as freedom from breast cancer death or other causes of death.
Postoperative adjuvant therapy has been performed based on the recommendation of NCCN or St. Gallen guidelines with anthracycline-based regimens (in this study mostly FEC therapy: 5-FU 500 mg/m2, epirubicin 75–90 mg/m2, cyclophosphamide 500 mg/m2) as chemotherapy. Tax-anes (paclitaxel, docetaxel) were added to follow FEC therapy in few high risk patients.
The patient group included 1,048 females with an average age of 51.8 years (standard deviation [SD] = 11.9 years). Data are expressed as mean ± SD for continuous variables. Independent t tests were used for the comparison of con-tinuous variables. Categorical variables were normally tested by the χ2 test when appropriate. All p values are two-tailed; a p value of less than 0.05 was considered to indicate statistical significance.
Results
Eighty-two (7.8%) patients died for cancer-related rea-sons during their follow-up, up to 31, December 2007. Five (0.48%) patients died for non-cancer-related rea-sons. The average follow-up time was approximately 40 months. One hundred and sixty-seven patients (15.9%)
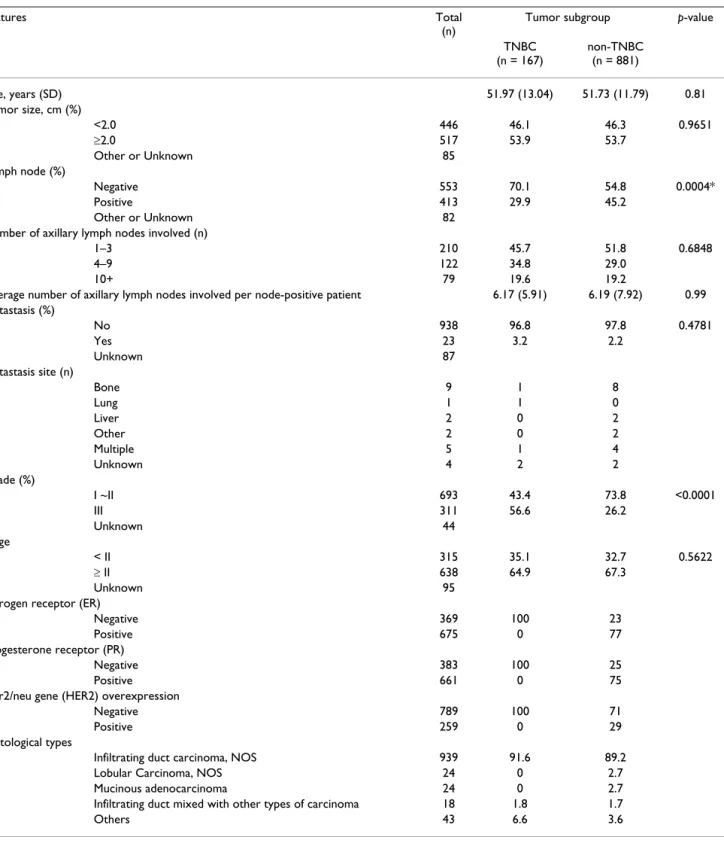
had TNBC and the remaining 881 patients (84.1%) were defined as non-TNBC. There was no distributional differ-ence of adverse prognostic factors between the two groups, except lymph node, and grade (Table 1). Sev-enty-one cases with recurrence of breast cancer were con-sidered as the events.
Table 1: Descriptive statistics of women with breast cancer according to tumor subgroup
Features Total
(n)
Tumor subgroup p-value
TNBC (n = 167) non-TNBC (n = 881) Age, years (SD) 51.97 (13.04) 51.73 (11.79) 0.81 Tumor size, cm (%) <2.0 446 46.1 46.3 0.9651 ≥2.0 517 53.9 53.7 Other or Unknown 85 Lymph node (%) Negative 553 70.1 54.8 0.0004* Positive 413 29.9 45.2 Other or Unknown 82
Number of axillary lymph nodes involved (n)
1–3 210 45.7 51.8 0.6848
4–9 122 34.8 29.0
10+ 79 19.6 19.2
Average number of axillary lymph nodes involved per node-positive patient 6.17 (5.91) 6.19 (7.92) 0.99 Metastasis (%) No 938 96.8 97.8 0.4781 Yes 23 3.2 2.2 Unknown 87 Metastasis site (n) Bone 9 1 8 Lung 1 1 0 Liver 2 0 2 Other 2 0 2 Multiple 5 1 4 Unknown 4 2 2 Grade (%) I ~II 693 43.4 73.8 <0.0001 III 311 56.6 26.2 Unknown 44 Stage < II 315 35.1 32.7 0.5622 ≥ II 638 64.9 67.3 Unknown 95
Estrogen receptor (ER)
Negative 369 100 23
Positive 675 0 77
Progesterone receptor (PR)
Negative 383 100 25
Positive 661 0 75
Her2/neu gene (HER2) overexpression
Negative 789 100 71
Positive 259 0 29
Histological types
Infiltrating duct carcinoma, NOS 939 91.6 89.2
Lobular Carcinoma, NOS 24 0 2.7
Mucinous adenocarcinoma 24 0 2.7
Infiltrating duct mixed with other types of carcinoma 18 1.8 1.7
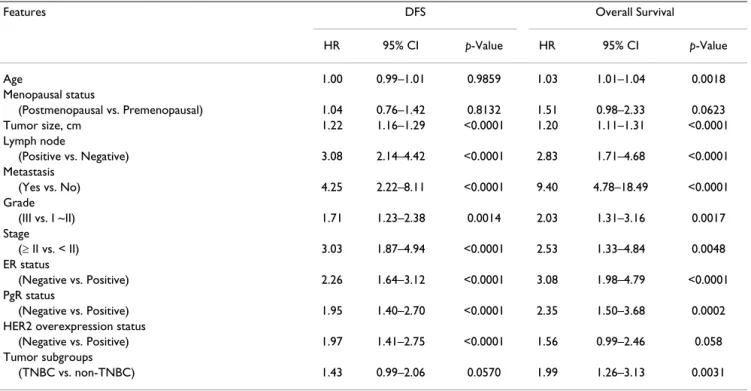
The univariate analysis for prognostic factors associated with 5-year DFS revealed that the tumor group, whether TNBC or non-TNBC, as well as age and menopausal sta-tus, was not statistically significant (Table 2). The univar-iate analysis for prognostic factors assocunivar-iated with 5-year overall survival revealed that the tumor group as TNBC or non-TNBC was statistically significant, in addition to age, tumor size, lymph node, metastasis, grade, stage, ER sta-tus, and PgR status (Table 2).
The multivariate analysis for prognostic factors associated with 5-year DFS revealed that the tumor group as TNBC or non-TNBC was not statistically significant. The multivari-ate analysis for prognostic factors associmultivari-ated with 5-year overall survival revealed that the tumor group as TNBC or non-TNBC was not statistically significant (Table 3). Survival curves are shown in the figures. Figure 1 reveals that TNBC tends to display a worse 5-year overall survival (p = 0.0026) than non-TNBC, using by log-rank analysis. ER-positive and/or PgR-positive and HER2-negative patients had the best clinical outcome, with a 5-year DFS of 80%; ER-negative, PgR-negative and HER2-positive patients (HER2-positive subtype) showed the worst out-come with a 5-year DFS of 45% (Figure 2A). TNBC has rel-atively poor prognosis. Figure 3A shows ER-positive and/ or PgR-positive and HER2-negative patients had the best clinical outcome, with a 5-year overall survival of 91%, and the HER2-positive subtype showed the worst out-come, with a 5-year overall survival of 59%.
To investigate the lymph node factor, we analyzed node-positive and node-negative patients individually. For node-positive patients, Figure 2B demonstrates that TNBC breast carcinoma tends to show a worse 5-year DFS, by log-rank analysis, and that ER-positive and/or PgR-posi-tive and HER2-negaPgR-posi-tive patients have the best 5-year DFS (p = 0.0088). For node-negative patients, Figure 2C reveals that the four subgroups do not show a 5-year DFS difference, using log-rank analysis (p = 0.0720).
For node-positive patients, Figure 3B points out that TNBC breast carcinoma patients tend to have the worst 5-year overall survival, by log-rank analysis, and that ER-positive and/or PgR-ER-positive and HER2-negative patients have the best 5-year overall survival (p < 0.0001). For node-negative patients, Figure 3C indicates that the four subgroups do not show a 5-year overall survival differ-ence, by log-rank analysis (p = 0.8620).
Discussion
We present the results of the largest Taiwanese study to date that thoroughly investigates the clinical phenotype of TNBC with regard to DFS and overall survival.
Traditionally, breast carcinomas have been classified as hormone receptor-positive or negative. Recently, newer approaches to breast carcinoma classification using gene-expression profiles and IHC biomarkers have identified at least four subtypes [10]. These subtypes are, luminal A (ER-positive and/or PgR-positive and HER2-negative),
Table 2: Prognostic factors for 5-year disease-free survival (DFS) and overall survival in univariate Cox regression analysis
Features DFS Overall Survival
HR 95% CI p-Value HR 95% CI p-Value Age 1.00 0.99–1.01 0.9859 1.03 1.01–1.04 0.0018 Menopausal status (Postmenopausal vs. Premenopausal) 1.04 0.76–1.42 0.8132 1.51 0.98–2.33 0.0623 Tumor size, cm 1.22 1.16–1.29 <0.0001 1.20 1.11–1.31 <0.0001 Lymph node (Positive vs. Negative) 3.08 2.14–4.42 <0.0001 2.83 1.71–4.68 <0.0001 Metastasis (Yes vs. No) 4.25 2.22–8.11 <0.0001 9.40 4.78–18.49 <0.0001 Grade (III vs. I ~II) 1.71 1.23–2.38 0.0014 2.03 1.31–3.16 0.0017 Stage (≥ II vs. < II) 3.03 1.87–4.94 <0.0001 2.53 1.33–4.84 0.0048 ER status (Negative vs. Positive) 2.26 1.64–3.12 <0.0001 3.08 1.98–4.79 <0.0001 PgR status (Negative vs. Positive) 1.95 1.40–2.70 <0.0001 2.35 1.50–3.68 0.0002
HER2 overexpression status
(Negative vs. Positive) 1.97 1.41–2.75 <0.0001 1.56 0.99–2.46 0.058
Tumor subgroups
luminal B (ER-positive and/or PgR-positive and HER2-positive), basal-like (ER-negative, PgR-negative and HER2-negative; mostly TNBC) and HER2-positive (ER-negative, negative and HER2-positive). ER- and PgR-negative tumors are generally thought to have a poor prognosis because of a deficiency of hormone therapy strategies. HER2-negative tumors lack the benefit of HER2-targeted therapy and are thought to imply a worse prognosis, as well [10]; however, few TNBC data have been reported among non-Western populations. Our data showed that TNBC in Taiwan may have a different mean-ing than in Western countries.
Table 1 revealed TNBC subgroup had higher rates of node-negative cases, in agreement with comparable studies [4,12,16,17]. Some series had different results from ours [3,6,7,10,13,14,18,19].
Our univariate Cox regression analysis demonstrated that tumor size, lymph node status, metastasis, grade, stage, ER status, PgR status, and HER2 status except tumor TNBC subgroup were the prognostic factors for 5-year DFS, in contrast to comparable series [4,6,17]. There were discrep-ant findings between the outcomes of DFS and overall sur-vival in our data. In CALGB 9344 trial, taxanes demonstrated a statistically significant improvement in DFS but not overall survival. It may interpret the discrep-ancy. In this study the chemotherapy regimen of most patients was FEC therapy. Due to Taiwan national health insurance policy, using FEC followed by Taxanes was only allowed in node-positive and ER negative breast cancer women. In Taiwan node-positive TNBC patients were allowed to receive Taxanes which improved DFS but not overall survival. Furthermore, Yin et al showed 85.1% of their patients were administered adjuvant chemotherapy
Table 3: Prognostic factors for 5-year DFS and overall survival in multivariate Cox regression analysis
Features DFS Overall Survival
HR 95%CI p-Value HR 95%CI p-Value
Age 1.00 0.98–1.01 0.9058 1.04 1.01–1.06 0.0013 Tumor size, cm 1.19 1.10–1.28 <0.0001 1.17 1.04–1.32 0.0110 Lymph node (Positive vs. Negative) 2.65 1.79–3.92 <0.0001 2.36 1.35–4.12 0.0026 Metastasis (Yes vs. No) 2.30 1.15–4.64 0.0193 6.63 3.13–14.09 <0.0001 Grade (III vs. I ~II) 1.54 1.05–2.26 0.0269 2.11 1.23–3.62 0.0065 Tumor subgroups (TNBC vs. non-TNBC) 1.28 0.82–1.99 0.2835 1.66 0.93–2.96 0.0881 Node-positive Age 0.99 0.97–1.01 0.2960 1.04 1.01–1.07 0.0161 Tumor size, cm 1.23 1.10–1.37 0.0002 1.29 1.11–1.51 0.0011 Metastasis (Yes vs. No) 2.37 1.15–4.88 0.0198 7.52 3.37–16.79 <0.0001 Grade (III vs. I ~II) 1.49 0.93–2.36 0.0948 2.46 1.23–4.90 0.0109 Tumor subgroups (TNBC vs. non-TNBC) 1.13 0.63–2.03 0.6847 2.20 1.08–4.49 0.0296 Node-negative Age 1.02 0.99–1.04 0.1801 1.04 1.01–1.07 0.0186 Tumor size, cm 1.16 1.02–1.31 0.0236 1.00 0.74–1.36 0.9813 Metastasis* (Yes vs. No) - - - -Grade (III vs. I ~ II) 1.49 0.75–2.94 0.2526 1.69 0.69–4.12 0.2525 Tumor subgroups (TNBC vs. non-TNBC) 1.52 0.75–3.06 0.2461 1.28 0.47–3.19 0.6815
of different regimens for 4–6 cycles [4]. Mersin said their patients had adjuvant chemotherapy according to the cur-rent guidelines at that time [6]. Fulford et al. reported DFS and overall survival results that were different from ours. Their study demonstrated that basal tumors, mostly TNBC, exhibited a significantly better DFS and overall sur-vival than non-basal tumors; however, the study was based on 470 patients with grade III invasive ductal carci-nomas diagnosed between 1975 and 1991. Twenty six percent of the patients received adjuvant chemotherapy [17].
Our multivariate Cox regression analysis demonstrated that tumor subgroup (TNBC vs. non-TNBC) was not the prognostic factor for 5-year overall survival These findings were in contrast with those of previous studies [3,5,12-14,20]. Liedtke reported that decreased 3-year overall sur-vival was observed for patients with TNBC, compared with non-TNBC (3-year overall survival rates: 74% vs. 89%; HR = 2.53; 95% CI, 1.77 to 3.57; p < 0.001) [3]. In addition, our results are consistent with those from other studies with respect to prognostic factors for overall sur-vival [16]. Kim reported that basal-like carcinoma, mostly TNBC, did not show survival difference between other subgroups, except the HER2-positive subgroup.
To further study the lymph node factor, we stratified patients into node-positive and node-negative groups. In node-positive patients, TNBC breast carcinoma tended to demonstrate the worst 5-year overall survival by log-rank analysis (Figure 3B), and ER-positive and/or PgR-positive and HER2-negative patients had the best 5-year overall survival (p < 0.0001). Figure 3C shows four subgroups of
node-negative patients that did not reveal a 5-year overall survival difference by log-rank analysis (p = 0.8620). Our results are in contrast to those of a previous study by Rakha, which reported that both univariate and multivar-iate analyses showed basal phenotype, mostly TNBC, was the only significant and independent prognostic marker in the node-negative patients [10].
Contrary to our supposition, our data in multivariate analysis showed that tumor subgroup (TNBC vs. non-TNBC) was not a prognostic factor for DFS. This study also revealed ER-positive and/or PgR-positive and HER2-nega-tive patients had the best 5-year DFS, and the HER2-posi-tive subtype showed the worst 5-year DFS. These findings were consistent with those of a previous study [6]. Mean-while, our results contrast with those from other studies in terms of prognostic factors for DFS [3,4,12-14,20]. Liedtke reported that in multivariate analysis, a signifi-cantly decreased progression-free survival was observed for patients with TNBC compared with non-TNBC at the seventh year [3]. Yin reported that in multivariate analy-sis, TNBC had a significantly increased likelihood of recurrence within 2 years after surgery rather than thereaf-ter [4]. Recent studies demonstrated that TNBC tends toward distant metastasis to the bone, soft tissue and vis-cera [3,10]. Liedtke reported that TNBC has a higher pre-dilection for visceral metastasis and early recurrence within the first 3 years of follow-up [3]. Statistically, our study did not substantiate a higher predilection of TNBC factor for metastasis. In this study, there was no difference in DFS and a significant difference in overall survival in univariate analysis. This might indicate the difference in overall survival after recurrence. In our study, treatment
Overall survival curves by tumor subgroup
Figure 1
Overall survival curves by tumor subgroup. Triple negative breast cancer (TNBC) tended to display a worse 5-year overall survival (p = 0.0026) than non-TNBC, by log-rank analysis.
Disease-free survival (DFS) curves according to patient group
Figure 2
Disease-free survival (DFS) curves according to patient group. A, among 1,048 patients, ER-negative and PgR-negative and HER2-positive breast carcinoma tended to display the worst 5-year DFS, by log-rank analysis; ER-positive and/or PgR-pos-itive and HER2-negative patients had the best 5-year overall survival; p < 0.0001. B, in the node-posPgR-pos-itive patients, TNBC tended to display a worse 5-year DFS by log-rank analysis; ER-positive and/or PgR-positive and HER2-negative patients had the best 5-year DFS; p = 0.0088. C, in the node-negative patients, four subgroups showed no 5-year DFS difference by log-rank analysis; p = 0.0720. We followed up the node-negative HER2-positive patients up to 48 months. ER, estrogen receptor; PgR, progesterone receptor; HER2, her2/neu gene over-expression.
A.
B.
C.
40% 50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months D ise ase-Fr ee S uvi val R at e ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)ER(+) and/or PR(+) HER2(-) ER(+) and/or PR(+) HER2(+) p<0.0001 20% 30% 40% 50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months D ise ase -F re e S uvi val R at e ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)
ER(+) and/or PR(+) HER2(-) ER(+) and/or PR(+) HER2(+) p=0.0088 30% 40% 50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months D ise as e-F re e S uvi va l R ate ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)
Overall survival curves according to patient group
Figure 3
Overall survival curves according to patient group. A, among 1,048 patients, HER2-positive breast carcinoma tended to display the worst 5-year overall survival by log-rank analysis; our ER-positive and/or PgR-positive and HER2-negative patients had the best 5-year DFS; p < 0.0001. B, in the node-positive patients, TNBC tended to demonstrate the worst 5-year overall survival by log-rank analysis; ER-positive and/or PgR-positive and HER2-negative patients had the best 5-year overall survival; p < 0.0001. C, in the node-negative patients, four subgroups showed no 5-year overall survival difference, by log-rank analysis; p = 0.8620. We followed up the node-negative HER2-positive patients up to 48 months.
A.
B.
C.
50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months O ve ra ll S ur viv al R at e ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)ER(+) and/or PR(+) HER2(-) ER(+) and/or PR(+) HER2(+)
50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months O ve ra ll S ur viv al R at e ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)
ER(+) and/or PR(+) HER2(-) ER(+) and/or PR(+) HER2(+)
p<0.0001 p<0.0001 50% 60% 70% 80% 90% 100% 0 12 24 36 48 60 Months O ver al l S ur vi val R at e ER(-) PR(-) HER2(+) ER(-) PR(-) HER2(-)
ER(+) and/or PR(+) HER2(-) ER(+) and/or PR(+) HER2(+)
after recurrence was based on NCCN or St. Gallen guide-lines and multidisciplinary care discussions. Most patients who have a recurrence after breast conservation therapy were given completion mastectomy and adjuvant sys-temic chemotherapy.
In node-positive patients, our data supported the ten-dency of TNBC breast carcinoma to show a worse 5-year DFS, by log-rank analysis (Figure 2B). These results con-trast with those from a previous study [10]. In node-nega-tive patients, our results revealed that the four subgroups showed no difference in 5-year DFS or in 5-year overall survival. However, these results contrast with those from previous studies [10,21]. Rhee in Korea demonstrated that triple-negativity was an independent predictor of shorter relapse-free survival [21]. Table 1 in this study demon-strates that TNBC had a higher ratio of lymph node-nega-tive patients than non-TNBC. This may explain why sometimes in our analysis the TNBC group was better than the HER2-positive subgroup.
However, the heterogeneity of TNBC, follow-up time, case number and other limitations may also explain the differ-ences between our conclusions and those of previous studies. Research into the heterogeneity of TNBC, new neoadjuvant regimens and more molecular-based TNBC classification studies could give us more information about the optimal therapies for TNBC subgroups. Liedtke et al. followed their patients to the 7th year, Yin to the 11th year, and Cheang to the 15th years [3-5]. A longer follow-up period may yield different results.
In our study, the TNBC rate was 15.9%, which is similar to reports from Korea and Carolina [16,18], but lower than other reports [3-6,12,21]. The race factor could con-tribute to the difference. Carey also reported that the TNBC subtype has a higher incidence in pre-menopausal African-American women (39%), compared to non-Afri-can-American women of any age (16%) and post-meno-pausal African-American women (14%) [18].
This study revealed TNBC and non-TNBC patients dis-played a similar distribution of clinico-pathological char-acteristics, such as age, tumor size, metastasis and stage, in contrast to other Western studies [3,10,15,19]. These pre-vious reports indicated that TNBC was associated with a larger size, and therefore had a poorer outcome than non-TNBC in terms of DFS and overall survival. In our study, overall survival rates between these groups were statisti-cally different in univariate analysis. This result may be related to lymph node, as mentioned. On the other hand, a higher grade was observed in our TNBC patients. In spite of this finding, the DFS for the TNBC subgroup was not statistically different from that of the non-TNBC sub-group, in contrast to earlier studies [3,6,17].
In our study, all of the data inferred that HER2 status added prognostic information for hormone receptor-pos-itive breast cancer patients, confirming that luminal B tumors constituted a poor outcome compared to luminal A tumors, in accordance with other studies [5,6,22]. In Taiwan, adjuvant trastuzumab targeted therapy was rarely used before 2006 in the HER2-positive subtype, due to the medical insurance policy, which may have contributed substantially to the worst overall survival.
Some research about epidermal growth factor receptor (EGFR) is interesting, and may provide another possible answer for the question of TNBC prognostic value [5,11,23]. Cheang reported that the expanded surrogate of PgR, HER2, EGFR, and cytokeratin 5/6 indicate a more specific definition of basal-like breast cancer, mostly TNBC, which better predicts breast cancer survival [5]. Cheang also showed that the core basal group has 1.62 times greater risk for breast cancer-specific death, whereas the non-core basal group does not have a clinically signif-icant risk [5]. Siziopikou reported that because the major-ity of TNBC patients express EGFR, the subgroup may derive benefit from EGFR-targeted therapies [11].
Conclusion
In conclusion, our study indicates that TNBC tends to dis-play a worse clinical course. Notably in node-positive patients, TNBC does play a prognostic role in overall sur-vival. In Taiwan, new strategies of chemotherapy and tar-geted therapy should be investigated for patients with TNBC.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
CL designed the concept of this study, drafted the manu-script and performed treatment. HST, LSC and SJK col-lected the data and performed the statistical analysis. TWC approved the final manuscript. DRC designed the concept of this study and provided treatment coordination. All authors read and approved the final manuscript.
Acknowledgements
We thank the personnel at the Cancer Registry, Changhua Christian Hos-pital, for their great help.
References
1. Alexe G, Dalgin GS, Scanfeld D, Tamayo P, Mesirov JP, Ganesan S, Delisi C, Bhanot G: Breast cancer stratification from analysis of micro-array data of micro-dissected specimens. Genome
Inform 2007, 18:130-140.
2. Horwitz KB, Dye WW, Harrell JC, Kabos P, Sartorius CA: Rare steroid receptor-negative basal-like tumorigenic cells in luminal subtype human breast cancer xenografts. Proc Natl
Acad Sci USA 2008, 105:5774-5779.
Publish with BioMed Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK Your research papers will be:
available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright
Submit your manuscript here: BioMedcentral
Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol 2008, 26:1275-1281.
4. Yin WJ, Lu JS, Di GH, Lin YP, Zhou LH, Liu GY, Wu J, Shen KW, Han QX, Shen ZZ, Shao ZM: Clinicopathological features of the tri-ple-negative tumors in Chinese breast cancer patients. Breast
Cancer Res Treat 2009, 115(2):325-33.
5. Cheang MC, Voduc D, Bajdik C, Leung S, McKinney S, Chia SK, Perou CM, Nielsen TO: Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-nega-tive phenotype. Clin Cancer Res 2008, 14:1368-1376.
6. Mersin H, Yildirim E, Berberoglu U, Gulben K: The prognostic importance of triple negative breast carcinoma. Breast 2008, 17:341-346.
7. Nguyen PL, Taghian AG, Katz MS, Niemierko A, Abi Raad RF, Boon WL, Bellon JR, Wong JS, Smith BL, Harris JR: Breast cancer sub-type approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J Clin Oncol 2008, 26:2373-2378.
8. Rakha EA, Reis-Filho JS, Ellis IO: Basal-like breast cancer: a criti-cal review. J Clin Oncol 2008, 26(15):2568-81.
9. Mehta RS: Dose-dense and/or metronomic schedules of spe-cific chemotherapies consolidate the chemosensitivity of tri-ple-negative breast cancer: a step toward reversing triple-negative paradox. J Clin Oncol 2008, 26:3286-3288. author reply 3288
10. Rakha EA, El-Sayed ME, Green AR, Lee AH, Robertson JF, Ellis IO: Prognostic markers in triple-negative breast cancer. Cancer 2007, 109:25-32.
11. Siziopikou KP, Ariga R, Proussaloglou KE, Gattuso P, Cobleigh M: The challenging estrogen receptor-negative/progesterone receptor-negative/HER-2-negative patient: a promising can-didate for epidermal growth factor receptor-targeted ther-apy? Breast J 2006, 12:360-362.
12. Kurebayashi J, Moriya T, Ishida T, Hirakawa H, Kurosumi M, Akiyama F, Kinoshita T, Takei H, Takahashi K, Ikeda M, Nakashima K: The prevalence of intrinsic subtypes and prognosis in breast can-cer patients of different races. Breast 2007, 16(Suppl 2):S72-77. 13. Nishimura R, Arima N: Is triple negative a prognostic factor in
breast cancer? Breast Cancer 2008, 15:303-308.
14. Haffty BG, Yang Q, Reiss M, Kearney T, Higgins SA, Weidhaas J, Har-ris L, Hait W, Toppmeyer D: Locoregional relapse and distant metastasis in conservatively managed triple negative early-stage breast cancer. J Clin Oncol 2006, 24:5652-5657.
15. Perreard L, Fan C, Quackenbush JF, Mullins M, Gauthier NP, Nelson E, Mone M, Hansen H, Buys SS, Rasmussen K, et al.: Classification and risk stratification of invasive breast carcinomas using a real-time quantitative RT-PCR assay. Breast Cancer Res 2006, 8:R23.
16. Kim MJ, Ro JY, Ahn SH, Kim HH, Kim SB, Gong G: Clinicopatho-logic significance of the basal-like subtype of breast cancer: a comparison with hormone receptor and Her2/neu-overex-pressing phenotypes. Hum Pathol 2006, 37:1217-1226.
17. Fulford LG, Reis-Filho JS, Ryder K, Jones C, Gillett CE, Hanby A, Eas-ton D, Lakhani SR: Basal-like grade III invasive ductal carci-noma of the breast: patterns of metastasis and long-term survival. Breast Cancer Res 2007, 9:R4.
18. Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S, et al.: Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006, 295:2492-2502.
19. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, Lickley LA, Rawlinson E, Sun P, Narod SA: Triple-negative breast cancer: clinical features and patterns of recurrence. Clin
Can-cer Res 2007, 13:4429-4434.
20. Langerod A, Zhao H, Borgan O, Nesland JM, Bukholm IR, Ikdahl T, Karesen R, Borresen-Dale AL, Jeffrey SS: TP53 mutation status and gene expression profiles are powerful prognostic mark-ers of breast cancer. Breast Cancer Res 2007, 9:R30.
21. Rhee J, Han SW, Oh DY, Kim JH, Im SA, Han W, Park IA, Noh DY, Bang YJ, Kim TY: The Clinicopathologic Characteristics and Prognostic Significance of Triple-Negativity in Node-Nega-tive Breast Cancer. BMC Cancer 2008, 8:307.
22. Ryden L, Landberg G, Stal O, Nordenskjold B, Ferno M, Bendahl PO: HER2 status in hormone receptor positive premenopausal
primary breast cancer adds prognostic, but not tamoxifen treatment predictive, information. Breast Cancer Res Treat 2008, 109:351-357.
23. Kim HJ, Cui X, Hilsenbeck SG, Lee AV: Progesterone receptor loss correlates with human epidermal growth factor recep-tor 2 overexpression in estrogen receprecep-tor-positive breast cancer. Clin Cancer Res 2006, 12:1013s-1018s.
Pre-publication history
The pre-publication history for this paper can be accessed here:
![Table 1 revealed TNBC subgroup had higher rates of node- node-negative cases, in agreement with comparable studies [4,12,16,17]](https://thumb-ap.123doks.com/thumbv2/9libinfo/9026810.312668/5.918.86.838.148.736/table-revealed-subgroup-higher-negative-agreement-comparable-studies.webp)
