Current View on Ethics and Genetics:
The Importance of Progressive Evolution of Medical Genetics and Genetic Counselling
Saša Ostojić, M.D., Ph.D. and Nina Pereza
Department of biology and medical genetics, School of medicine, University of Rijeka, Croatia
M. Louisa Pedri,B.A., B.Ed., M.A.
Centre For Health Care Ethics (CHCE), Lakehead University – Thunder Bay, Ontario, Canada
ABSTRACT
The unprecedented rate of discovery and application of medical genetics requires us to pause and ask if humanity as a species is well served or compromised by this development. Newborn screening tests practiced in developed countries, though beneficial, raise questions of ownership, identity, confidentiality and disclosure or results. Prenatal genetic testing, widely available, but not mandatory, creates pressure on physicians to offer and for patients to undergo them. A new, bizarre notion of ‘responsible parenthood’ means to give birth only to children who are without genetic abnormalities and to abort all others. Most disturbingly, medical genetics’ goal of eliminating severe disorders has silently morphed into a collective evolutionary
“imperative” driven by an ideology of creating the perfect human specimen, and by default appropriating exclusive rights to the production and control of human life. Yet, history provides us with numerous examples to remind us that a prerequisite “to being human, and to be worthy of life” is not synonymous with a state of biological perfection.
In addition, human diversity may be the secret of humankind’s success. Without diversity, there would be no effective selection. We must have a balanced ethical debate. This can happen only after scientists, physicians and all people become educated about the realities of genetics and willfully work at setting limits on these pursuits. Unfortunately, current normative bioethics does not provide a satisfactory solution for a unique, global approach. For the new ‘genethics’, we need to be mindful of bioethical, legal, psychological and social implications of genetic research and its applications. This must inform genetic counselling, which is critical for beneficial interventions, and it requires informed geneticists with imagination and intuition. The
power of human genetics over the future of humankind is unprecedented.
Imperceptibly, the range of genetic interventions is increasing without full consideration to benefits, harms, future consequences or responsibility. It is imperative to embrace genetic responsibility for maintenance of diversity and richness of human life.
Key words: bioethics, eugenics, genetic information, genetic counselling, medical genetics, genethics
Introduction
The science of genetics as it is applied in medicine is advancing under its own energetic momentum to such an extent that it is virtually outstripping all existing checks and bounds previously imposed by various scientific, and political controlling bodies. In light of this unprecedented rate of discovery and application, one must pause and ask if humanity as a species is well served or compromised by this development.
Let there be no doubt, that medical genetics has had and will continue to have its positive effects and outcomes, however, its overall positive attributes will continue to flourish if, and only if, there exists the attentiveness and the will among all concerned – scientists, politicians, lay people in general – to pursue a goal which is defined by its service to human life, and not its converse.
This paper will briefly review some of the advances of genetics with their medical interventions and consequences and its power over the future of humankind.
It also looks at the phenomenal shift in medical goals, which shifted from an attempt to
‘decrease the number of physical and psychological human disorders’ to a quest for achieving ‘biological human perfection’. In view of these extraordinary developments and challenges, we draw attention to the urgency of timely and accurate professional education, and the necessity of an all encompassing form of genetic counselling.
Finally, this paper proposes the development and implementation of appropriate meaningful tools for the enhancement of genetic ethical inquiry, which is so essential for the evaluation, examination and application of the fruits of the new genetics.
I. Recent technological and clinical advances in medical genetics
For most of the 20th century, many medical practitioners viewed genetics as an esoteric academic specialty; that view is now dangerously outdated1. Unquestionably, the completion of the draft sequence of the human genome (2003) was a milestone in the history of biology and medicine2. The explosion of information continues as we write. Every day, researchers are discovering the functions of new genes, and over
6000 known single-gene disorders have been identified3. The outcome of this is translated into uncovering the connection between genes and hereditary diseases, which in turn is then utilized in advancing medical clinical paractice.
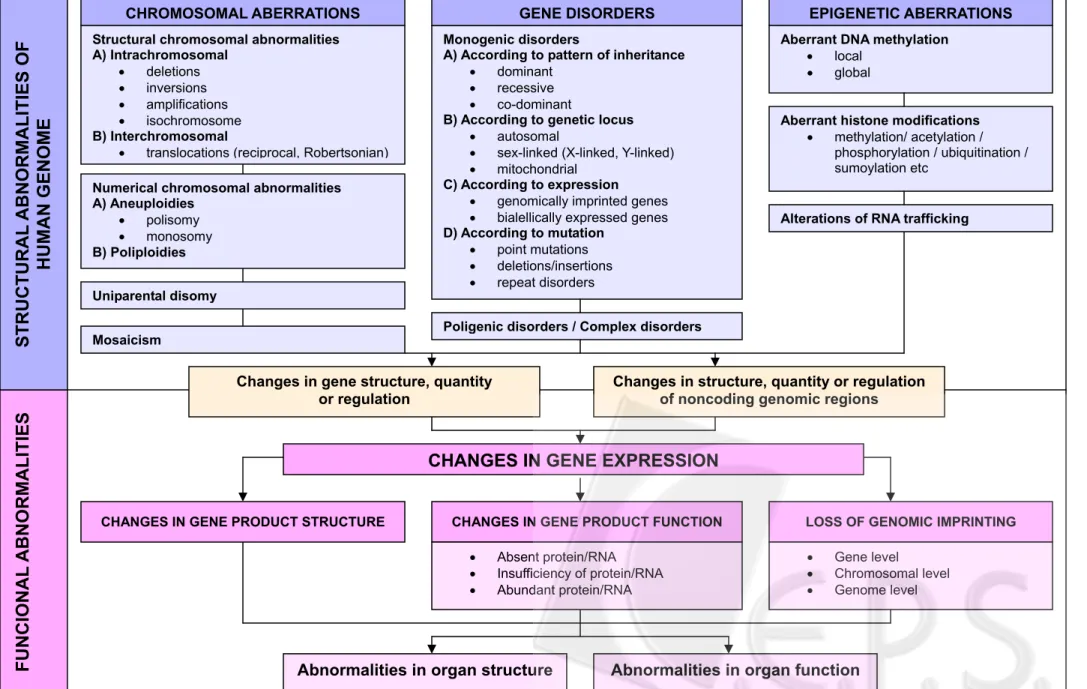
Genetic disorders occur in 1:200 live-births but it is believed that all diseases are affected by genetic factors, either inherited or influenced by environmental factors4. For example, congenital anomalies are present in 3-5% of all newborn children, thus representing a significant part of prenatal and infant mortality and morbidity5. We now know that a significant number of congenital anomalies have a genetic etiology (15-25%) (Figure 1), while only a smaller fraction is caused by environmental factors, such as teratogens (8-12%)6. Many more congenital anomalies are the consequence of the interaction between genes and environment (20-25%). At this time, the etiology in the majority of cases still remains unknown (40-60%), but it is supposed that they are somehow genetically influenced.
Figure 1. Genetic causes of genetic disorders6
EPIGENETIC ABERRATIONS
Poligenic disorders / Complex disorders
ABNO RMALITIES
CHANGES IN GENE EXPRESSION
LOSS OF GENOMIC IMPRINTING CHANGES IN GENE PRODUCT FUNCTION
CHANGES IN GENE PRODUCT STRUCTURE
• Absent protein/RNA
• Insufficiency of protein/RNA
• Abundant protein/RNA
• Gene level
• Chromosomal level
• Genome level Monogenic disorders
A) According to pattern of inheritance
• dominant
• recessive
• co-dominant B) According to genetic locus
• autosomal
• sex-linked (X-linked, Y-linked)
• mitochondrial C) According to expression
• genomically imprinted genes
• bialellically expressed genes D) According to mutation
• point mutations
• deletions/insertions
• repeat disorders
CHROMOSOMAL ABERRATIONS GENE DISORDERS
Structural chromosomal abnormalities A) Intrachromosomal
• deletions
• inversions
• amplifications
• isochromosome B) Interchromosomal
• translocations (reciprocal, Robertsonian) Numerical chromosomal abnormalities A) Aneuploidies
• polisomy
• monosomy B) Poliploidies
Aberrant DNA methylation
• local
• global
Aberrant histone modifications
• methylation/ acetylation / phosphorylation / ubiquitination / sumoylation etc
STRUCTURAL ABNORMALITIES OF HUMAN GENOME
g
Changes in structure, quantity or regulation of noncoding genomic regions
Alterations of RNA traffickin
Changes in gene structure, quantity or regulation
y Mosaicism
parental disom Uni
The new genetic knowledge has brought immense progress in the promotion of human health. Newborn screening programs may screen for up to 50 diseases, including phenylketonuria, cystic fibrosis and hypothyroidism. About 3,000 newborns tested in the United States of America are positive each year for one of these severe disorders7. Newborn screening currently represents the largest single application of genetic testing in medicine and the first and largest public population-wide health program for genetic conditions8.
Genetics has united us and made us equal as every live born infant shall have an adequate blood test for all disorders. Newborn screening programs, often initiated within 48 hours after birth, are madatory in most developed countries. Although they have brought many positive changes in the promotion of human health, their further expansion will lead to grave ethical concerns. Today, newborn screening tests are developed for a more comprehensive genomic screening at birth9. In some parts of the United States of America, the government is now retaining indefinitely, each baby’s test results and DNA for research without parents’ approval10. This practice raises the question of ownership, identity, confidentiality and disclosure11.
Highly developed prenatal genetic testing is widely available and although it is not mandatory, that is, nobody is literally forced to have a genetic analysis, the pressure exists for physicians to offer and for patients to take them12. Today, although it is never really said out loud, responsible parenthood is defined by giving birth to children that are not marred by genetic abnormalities that soon after birth or in the future, may require medical interventions or treatments and will have in the opinion of some people, low quality of life!.
The expectation is that parents will wish to prevent the birth of a child affected by a genetic disorder13-15. No one is literally forced to undergo an abortion, but the subtle pressure is ever present to terminate a pregnancy (genetic abortion) when a genetic problem has been identified. This principle of “procreative beneficence” assumes that parents or single reproducers are at least prima facie obligated to select the child, out of a range of possible children they might have, who will be likely to lead the best life16.
“What does it mean to be human?” the great philosophers asked! “Which humans have a right to be born, or, to continue their existence?” is the new question that modern genetic medicine is forcing us to ask. If not controlled, this unreflected attitude is likely to
evolve into a most pernicious form of a new eugenics. Perhaps, the best way to prevent genetic information from being used to restrict reproductive freedom, by this type of societal pressure, is to educate the public about the scope and limitations of our understanding of genetics and genetic tests17.
In addition, contemporary genetic technology also allows genetic enhancement which refers to the transfer of genetic material intended to modify non-pathological human traits18. The term genetic enhancement is commonly used to describe efforts to make someone not just well, but better than well, by optimizing attributes or capabilities - perhaps by raising an individual from standard to peak levels of performance.
II. More genetic intervention, more problematic consequences
It is necessary to consider how these advances in the biomedical sciences will affect the willingness of all humans to continue their existence as nature formed them, and in particular with the will of mothers and fathers to maintain a pregnancy or even to desire future conceptions. It is also crucial to ponder the paradigm shifts that have taken place, which affect the value we place on all the stages which define human life. For example, pregnancy, the natural, normal, female physiological process has shifted from a “natural condition” which may have required, at times, some medical intervention, to a “medical condition”, which is always in need of medical interventions. Is the fetus a symptom necessitating medical attention for the mother, or is it a normal stage defining a life in process? Or, take genetic prenatal tests, which were previously offered as matter of personal choice, but are now becoming the norm, as a seemingly medical and social necessity. Besides instilling anxiety, this process of medicalizing pregnancy has encouraged a mindset that a child in not a “child” until prenatal tests have been carried out and the results have confirmed that all is well12.
A genetic predisposition to diseases, when established by testing a child or an adult, represents a life-long risk factor which often affects family relations and quality of life, and can lead to the development of depression, tension, anxiety, potential loss of a family member, the possibility of social stigmatization and great financial burden19. Prenatal genetic analysis, whether in the form of genetic testing or screening, according to the
European Comission’s recommendations, should be voluntary and performed only in order to gain knowledge about fetal health status (as described by medical indications)20,21. Following this, prenatal genetic analysis can be requested or recommended based on two different intentions. One intention is to seek and apply, if available, a cure or treatment for the abnormality detected, or else gain information to help one cope and be psychologically, spiritually, materially prepared for the situation20,22. The other, by default, is the intention to terminate the pregnancy and remove the embryo or fetus which has a probability to be diseased22. Both create personal challenges, but the latter is the most morally problematic because the intent is to destroy a yet unborn human life for the simple reason that it could be less than perfect23. In light of such serious outcomes, all those involved must continually ask what the role is of genetic science and medicine, ought it to be at the service of life, or to rule over life?
We must be continually vigilant so that genomic medicine is not reduced to only its technical aspect. Many questions need to be asked. Can we really be certain that this increased power to detect and predict genetic diseases will allow their eradication by
“genetic hygiene”? Certainly not! No genetic test can detect all forms of birth defects and abnormalities, and probably never will because genes can have hundreds of disease-causing mutations, and mutations in different genes can cause same disorders (genetic heterogeneity)24. While it is well known that a good part of our phenotype is strongly influenced by genes, it is now clear that environment plays an important role in the modification of our genome through epigenetic mechanisms. Not only do the non-gene mechanisms of inheritance exist, but these epigenetic modifications also determine most of the human phenotypic variability25. Epigenetic factors govern the interpretation of DNA within each living cell just as the conductor of an orchestra controls the dynamics of a symphonic performance. Epigenetic effects in human populations have been more difficult to identify, but the potential is immense. Do they have a major impact on human health?
Probably yes, but only a large-scale Human Epigenome Project can address this question6.
Genetic determinism, that is, the idea that genes determine all human phenotypes should be seriously re-examined, although not necessarily rejected. Although the environment is greatly implicated in the functioning of our genome, it must not be forgotten that these changes happen inside the genome structure itself, and thus the resulting
phenotype should not be considered as a straight line but more as a circle of interaction between the environment and genetic information27. These interactions are known as epigenetic modifications and comprise a great part of genetic research today. The discovery of epigenetic modifications has finally begun to unravel many mysteries of human physiological and pathophysiological variability. For example, although monozygotic twins share identical DNA sequences, they show numerous epigenetic differences. Even if both twins have a genetic predisposition of the same hereditary disease, there is a minimal chance that the epimutation will progress in the same manner in both of them, which points to the fact that these epigenetic differences in the critical DNA region could result in differences in the expression of specific features28.
Human genetics is often fueled by sensationalist media reporting and developments are often exaggerated and create unrealistic expectations for the "new genetics"29. But this is to be expected, given the desire to control illnesses, eradicate disease as well as all unfavourable traits from the human condition.
Do we need to keep an open mind? Yes! Genetics is a broad field of unexplored treasures which could answer many questions on human existence; it cannot be considered just a technical and scientific discipline, but foremost it is a calling which demands from geneticists immense imagination and above all, good intuition, as we will discuss later6.
III. Elimination of disorders to a quest for human perfection
The development of sophisticated genetic technologies leads to an increase in the availability of genetic tests and screening programs that are more accurate as well as commercially viable. These, in turn, make possible, not only, the detection of hereditary diseases and congenital anomalies, but also, the selection of specific human qualities, which quietly leads to an unavoidable genetic revolution.
Medical genetics moves rapidly from its goal to eliminate severe disorders to its goal to attempt to produce the perfect human specimen. So, it appears that mankind’s noble dream to eradicate diseases has transformed itself into a silent, collective
evolutionary “imperative” for constant improvement of the human species. And the present day perception is that this worthy cause can be achieved only by the utilization of the newest discoveries from within the discipline of genetics.
History provides us with numerous examples to remind us that a prerequisite “to being human, and to be worthy of life” is not synonymous with a state of biological perfection, or, however medical science defines such perfection. History abounds with individuals, who excelled and contributed to the world in remarkable ways in spite of, or even because of their handicaps. Take for instance, Einstein, who was born in the 7th month of gestation; Van Gogh, whose 30 different diagnoses suggested for his insanity;
Toulouse Lautrec, who was only 140 cm tall; Beethoven, who was deaf since age 28;
Baudelaire, who had aphasia (the loss of ability to produce and/or understand language);
Tesla, credited with inventing the 20th century, who had obsessive-compulsive disorder;
and our present day Stephen Hawking, who has Amyotrophic Lateral Sclerosis, motor neuron disease, is considered by many, the greatest physicist of our time. And, who does not recognize the name, Elephant Man, popularized by numerous plays, television productions and David Lynch’s award winning 1980 film by the same name. The life of Joseph (John) Carrey Merrick, 1862-1890, otherwise known as Elephant Man was wrought with physical, emotional and psychological suffering caused by a congenital disorder which manifested itself in macrocephaly, gigantism, and numerous tumors30. Today’s witness, to the extraordinary short life of this remarkable man, will understand that behind Merrick’s deformed body lived a man who was imaginative, emotional and intelligent enough to understand his misery. It was his practice to end his letters with the following poem by Isaac Watts31,32:
Tis true my form is something odd, But blaming me is blaming God.
Could I create myself anew, I would not fail in pleasing you.
If I could reach from pole to pole, Or grasp the ocean with a span, I would be measured by the soul, The mind's the standard of the man.
Although we are all members of the same species, we are significantly different in the ways we perceive our existence, background and lifestyle as well as our genome and genetic knowledge. Even though as human beings we share a common ‘book’ – the genetic code, its interpretation around the world is not the same. As we are unable to standardize the approach to our genome, we behave like children who first want a new toy, but as soon as they get it, they disintegrate it into nonfunctional parts. What we need above all is a discussion which accepts, but also sets out our cultural, social and religious differences, and tries to bring about the view which unites all human knowledge in its essence.
Do we need norms at all? Most certainly yes, but what we need more is a changed global attitude toward the misguided quest for the eliminations of all imperfections that is aiming for a “perfect” human. Let us not forget that the important determinant of natural processes and evolution is the survival of the most adapted and by no means of the best.
Take for example the mutation in the hemoglobin gene which leads to sickle cell disease, but creates a natural defense from malaria. Recently, it was discovered that people with Down syndrome appear to have genetic protection against some forms of cancer, atherosclerosis and possibly multiple sclerosis33,34.
It is possible that there are people who are resistant to all currently known diseases.
Sometimes the evident imperfection brings an unknown evolutionary advantage for survival. But when we admit such a fact, we are opening the way to a global (r)evolution and new order, which is not based on the unsparing battle for the best, but on the cooperation of the imperfect. Domination as an imperative for existence should grow into the toleration of biological, social, political, economical and bioethical differences.
If the imperative of existence is to be the best, and to subsequently transfer these traits to the next generation, then, we should ask what kind of qualities are inherited from
“the best” after several millions of years of perfection and natural selection on Earth?
Technological civilization has come to a crossroads. We are heading for self-destruction unless we change the course. The anthropocentric view of the world where the human dominates over everything around it including members of its own species is turning our life into a meaningless race in which we are being alienated from our
altruistic self. Is it really true that competition is the major drive of survival? Experience would demonstrate that humans are a rare species ready to engage in acts of altruism regardless of reward or recognition and in spite of danger or threat of death to themselves.
The truth tells us that we urgently need a new view on the achievements of medical genetics.
IV. Power which human genetics has over future of mankind
Silently almost invisibly, the range of genetic interventions is increasing without full consideration to the consequences. This development needs to be corrected as we need to enter the age of genetic responsibility35. Developments of new molecular tests have already begun to herald a revolution in the practice of genomic medicine36 and genetic testing is becoming part of the everyday healthcare systems21.
However you look at it, genetic testing has the potential to revolutionize medicine.
But revolutions can have casualties. The metamorphosis of mankind’s dream of
“eradicating disease” to “improving the human species” is perhaps in its final stages of completion.
There is a popular belief in our society about genetic determinism which says that our genome represents a “coded future diary”. But the real truth is that the genetic knowledge gained through the HUGO project is not sufficient and genes are not destiny26. Most diseases are an interplay of (epi)genotype, environment, behaviour and... bad luck.
This is why society cannot choose its own prototype. Take for example breast and ovarian cancer – all breast/ovarian cancers are genetic disorders but only 5% of them are heritable due to the inheritance of high risk cancer susceptibility genes (BRCA1 and 2)37. As quantitative somatic mutations are more important than hereditary mutations, the risk of cancer development associated with mutations is different for every person38. Genetics is just one piece of the “puzzle” that is recently being upgraded with epigenetics. Genetic analysis tells nothing about these epigenetic modifications and environmental influence.
The recently acquired knowledge is not yet matched with a full understanding of the implications for us.
Understanding the function of each and every human gene is a huge undertaking.
However, the undertaking to use this information to understand and treat diseases is of even a larger magnitude. The objective to understand the function of the human genome has forced a redirection of research processes to study hundreds or thousands of (if not all) genes in terms of their expression patterns, pathway interactions and so on39.
Could new genetics provide the final answers? We will never control everything!
The ability to read our “gene horoscope” will take away the true experience of freedom. We can be free only if we don’t know the part of our destiny influenced by our heredity. We should be happy people, not just healthy people. John Merrick died in sleep as his head fell back under the weight, dislocating his neck. He had often spoken of wanting to sleep like normal people, and perhaps he was trying to do so30.
Let us not forget – when you are dealing with humans, be human. Medical clinical genetics is the one branch of biomedical sciences where intuition is a key feature40. By definition, human genetics pertains to relatedness, rather than separateness41.
Although the human race has always longed for perfection in every aspect of life, today this collective evolutionary “imperative“ for constant improvement of human species is becoming even more dangerous because it is happening silently. Today, all that is negative in the idea of human perfection is hidden behind a shield of supposed positive genetic progress, which alleges to give us knowledge of the genetic code and possibly treat genetic disorders, and at the same time it facilitates our rejection and eradication of all that we perceive to be a set-back for our illusory progress. It is quite probable that in trying to ascertain human values and validity from present day developments in hereditary genetic strengths and weaknesses, one can succumb to the old eugenics through a new approach. In this way, we are alienating any progress from the basic bioethical concept of respecting the dignity of every human being regardless of its genetic qualities.
The truth is that we are all carriers of abnormal genes that can cause certain disorders. Discrimination on the basis of genetic tests could make everyone a target. We are all in the same risk pool, and it is very pretentious and erroneous to qualify people as genetically healthy or deficient. Consider the situation faced by Einstein, Van Gogh, Hawking, Toulouse Lautrec, Beethoven, Baudelaire and Tesla; if their parents had the
chance of prenatal genetic selection, would they have chosen them? Modern science brings a growing wealth of knowledge and techniques to the diagnosis, treatment and prevention of genetic disorders. So, what can be considered as acceptable genetic diversity?
To face honestly the consequences of arriving at the edge of the “sustainability” of our civilization - which includes the possibility to change one’s genome, gene therapy, cloning, preimplantation genetic diagnosis and various types of genetic testing - is much more important than all the rules we could set on a piece of paper, because they would not bring a new approach to the understandings of the “Pandora’s box” – our genome.
In the discussion of defective genes, the word “defect” supposes that we have a perfect prototype, negating human diversity. The right of every person to life and dignity includes the right to inherit a genetic code which hasn’t been artificially modified42. Genetic freedom should be the freedom to bring about the conception of a child with any characteristics, whether they are good or bad, desired or undesired43.
V. Need for new gen-ethics
It is obvious from what has been discussed above that no branch of science has ever created more acute or more subtle and interesting ethical dilemmas than genetics44. Given its complex nature, it is not always clear to the patient, what ought to be the right decision following specific genetic consultations. Although there are a number of ethical frameworks that can be employed to assist those concerned in resolving ethical dilemmas within a clinical setting, such as the four principles of biomedical ethics45 and the structured approach to case consultation (Ethox approach), one must always keep in mind that ethics is not a static set of theories or principles that can be easily ‘applied’ to new situations46. Although genethics is defined as the study of ethical issues that arise out of the science of genetics and the uses of genetic technologies, the new challenges or conflicts that emerge from the evolving field of genetics may not be resolved using the established ethical frameworks, which can be compared to Willie Stark’s comment about the law, “The law is like pants you bought last year for a growing boy; it is always too short and too tight for growing mankind”47,48. It is therefore incumbent on every scientist and
clinician active in a genetic field to assume personal responsibility in the development and expansion in this field of ethics and in his/her area of expertise. Science cannot resolve moral conflicts, but it can help frame the debates about those conflicts.
Medical ethicists have traditionally referred to beneficence, nonmaleficence, respect for autonomy, and justice as fundamental principles of medical ethics. Normative bioethics, including these four principles, and even their expansion with the virtue ethics, doesn't provide a satisfactory solution for a unique, global approach to the human being. In the case of genetic counselling, when applied in the context of genetics, beneficence and non-maleficence sit easily, but, autonomy and justice can be problematic49. Counselling and ethical challenges related to genetic diseases require new approaches to ethical analysis, as well as more resources.
Individual autonomy has been the most valued principle in clinical ethics, but if patients possess no knowledge on genetics, how can they make decisions regarding their entire family and progeny? Should autonomy be the most valuable principle of bioethics in new genetics? probably not, because autonomy is not synonymous with unconditional freedom, and part of the concept of autonomy must be the recognition of other people's autonomy, or values50. There are tensions between the rights of individuals and the rights of the family, for whom this information may have relevance to health49.
The familial nature of genetic information demands some modification of the usual principles of privacy and non-disclosure, in both directions. The information should be able to be shared with family members whose health may benefit from their access to this information because it alerts them to the risk of a genetic disease and enables them to institute preventive or therapeutic strategies, but the information must be protected more carefully from outsiders49.
Although uniquely personal, the information from gene analyses impacts not only the human being whose genetic material was analysed but also parents, siblings, children and sometimes entire ethnic groups. When parents are faced with a birth defect of their child or when a patient is faced with an inherited genetic disorder, it still creates a heavy emotional, social and financial burden51. Physicians need to carefully balance the right of a patient to privacy against the wider family and society interests, consistent with ethical
standards and their legal obligations.
While medical genetics is developing faster than law regulations or public opinion, the human species hasn't precisely determined whether its priority is to “shape” new generations according to the will of the parents, or to create a society which is prepared for
“less perfect” individuals. Today, human medical genetics needs to include biomedical, ethical, philosophical, social and theological considerations of genetic disorders which are specific by the fact that they can only be prevented and most of them never completely cured. In addition, gene therapy and genetic drugs (especially orphan drugs) as they are emerging for practical use, are very expensive and it is unclear who should carry the cost.
These developments suggest that instead of “ABSTRACT” bioethics, we need the real, life bioethics, the one that tries to understand the human genome, and not control it.
After all, genethics is an exploration of the clash between modern genetics and human values48. It is a recombinant word that splices the words genetics and ethics together to capture their conceptual inseparability. Genethics represents a search for broad, lasting moral guidelines gleaned from complex, real-life ethical issues in genetics that are at once more imaginative, humane and scientifically sound. And so, the kind of bioethical
“l'art-pour-l'art”-ism should once again try to turn to the understanding of human essence and the right interpretation of the human genome.
Society needs to be involved in setting limits about the individual choices that can be made52. Although there is some disquiet about genetic interventions, as a society, we need to ensure that we have a balanced ethical debate on issues of concern and that we distill the real ethical issues. The challenge ahead is to ensure that the newness of genetics does not unreasonably impede its implementation49.
VI. Education and Counselling as keys to a desirable genetic future
Widespread genetic education is needed across the globe. All discussions of genetic progress and its implications in ethics can be done only when people are highly educated about genetics53.
Despite the exciting advances in medical genetics, many practicing clinicians perceive that the role of molecular genetics, especially that of genomics, is confined primarily to the research arena with little current clinical applicability2. The importance of education in medical genetics for the primary physicians and others who are involved in its practice cannot be exaggerated.
Francis S. Collins once said that most physicians in practice today have had not a single hour of education in genetics and are going to be severely challenged to pick up this new technology and run with it. Primary care physicians and other health care providers who are not specialists of medical genetics are not well prepared to handle patient inquiries about these new genetic tests and capabilities54. They are caught between the popular media and patient curiosity on the one hand, and on the other hand, the lack of research about the clinical utility of these tests, and the outcome of interventions based on these tests. It is important that the central resource of information about human medical genetics and genetic disorders for other health care professionals, patients and the general public must be exclusively medical geneticists.
Genetic counselling as the main form of communication between specialists and patients is under constant pressure to evolve and progress as it is a unique medical specialty that provides clinical health care for patients across the lifespan facing genetic and inherited diseases19. Thus counsellors should possess extraordinary teaching skills, whereas the professionals and patients would have to learn to make decisions and understand their consequences21. It is also important to emphasize the importance of sub-specialization and diversification of genetic counsellors’ roles due to the constant growth of knowledge in medical genetics.
The new knowledge has to be disseminated quickly. It is imperative that opportunities for education are organized for both the public and the media. It is important to increase public awareness, education and understanding of genetic concepts21.
Genetic counselling is complex, not just because of the complex system of genetics, epigenetics and environmental influences, but also because of the numerous ethical dilemmas. The massive amount of genomic information now available allows for new insights into these processes. The problem of complexity becomes even greater when we
consider the fact that hereditary diseases do not follow only the classical monogenic traits, but also include complex mechanisms of genomic imprinting, trinucleotide repeat disorders, multifactorial diseases, mitochondrial inheritance, Y-lined inheritance, incomplete penetrance, variable expressivity, environmental factors, work, lifestyle, health care and many others. And these complex traits are present in the most common diseases of today such as cardiovascular diseases, and they are just small, almost imperceptible, changes in lots of genes.
The fundamental component of genetic counselling is education, attempting to present a large amount of complex information in comprehensible ways that allows a patient to make an informed decision54. Therefore, genetic counselling might be considered more as patient-education than actual advice. The biggest challenge for proper education of patients represents prenatal and presymptomatic diagnostics. Education of parents about the condition of their unborn child can give them the chance to "prepare" for a baby with a health problem and/or enable timely medical or surgical treatment of a condition before or after birth. Proper education of people, who take presymptomatic diagnostics, helps them to cope with discovered mutations before symptoms appear, so they can be monitored for early signs of the disease and treated promptly to reduce morbidity and mortality. With the proper lifelong medical and psychological support the quality of life can be improved55!
When we look at the increasing number of identified genetic disorders - currently, there are tests available for over 1400 disorders - and the huge interest in the role of new genetics, we can more greatly appreciate the importance of genetic counselling and the role that it can play, especially in the lives of those individuals that are directly affected:
those with identified genetic disorder, those whose ancestry points to probable genetic disorder and pregnant women.
When patients at risk are identified, the counsellors must quantify, qualify and contextualize the risk, then provide to the patient pre-test counselling - professional information and education of the patient about his/her condition; receive an informed consent; select and offer testing, disclose results, provide post-test counselling and follow-up. Counsellors must leave clients emotionally and psychologically stronger, and more competent to deal with their own lives55. They protect the individual from making a
precipitous decision which might be regretted, and can help evaluate the client’s understanding of cause and its relation to scientific explanation, clarify alternatives and anticipated consequences56.
Many would attest that in countries that remain deficient in medical resources, selecting and offering genetic or any other form of screening for genetic disorders is definitely the most sensitive aspect of genetic counselling. Our experience tells us that, as people who seek genetic counselling are usually of deficient genetic knowledge, the process of informing about the complex and mostly expensive genetic analyses turns genetic counselling into the highest skill of communication. Not only must the counsellor provide full information about the purpose of the test and testing options but he/she must also explore the patient’s motives for testing57. Once the result of genetic analysis is disclosed the counsellor must discuss the predictive value and meaning of a positive or negative test and explore the potential impact on relatives and the risk to offspring57. Another especially important task is to discuss the future reproductive options: the counsellor must inform individuals that it is their ethical duty to tell blood relatives that they may be at genetic risk57. Because of the sensitivity and potential harmfulness, the person concerned also has the right to decide not to be informed about the results.
Certainly, with the importance placed upon the emerging discipline of genetic counselling, one would infer that the emphasis of genetic science is on service, and that its greatest promise lies in its potential to enhance human life. If we are convinced by the statement that the main goal of genetic counselling is to help individuals or families cope with complex decisions, required because of medical, psychological, emotional, social and economic consequences of genetic disorders56, then, there is hope that a genet(h)ical environment will prevail. Let’s stop divorcing ethics from genetics – we must consider them equally and not forget that genetics as the science of life cannot be complete without ethics as the study of what constitutes right and wrong, and that these are two sides of the same coin… it is the human mind that sets them apart.
The goal of genetic counselling should resemble that of other health education programs: understanding personalized disease risk; enhancement of health-promoting behaviours including the client’s self-determination in exercising choices; and facilitation of client understanding and acceptance, both aspects of adaptation55. Not only is genetic
counselling an important tool for education of patient but it is also a useful tool in preventive medicine as it usually presumes a lifelong dynamic communication process of providing genetic information on the course and prognosis of a specific genetic disorder.
Language can also be a powerful manipulator, body language, even more so.
Patients are always influenced by the kind of information provided and the manner in which it is given. Whatever way you present genetic information, it always reflects the message being sent. And whatever way you present your information, it is wittingly or unwittingly directive, but providers should try to be aware of their own views and not project his/her values on the patient58. A counsellor must know that it would be unwise to answer such a posed question, “What would you do if placed in my position?” Rather, consideration ought to be given to the consequences of each possible course of action that is initiated from a patient’s or society’s interests.
There are two major concepts in providing genetic information – the teaching and the counselling model59. The teaching model is based on the conjecture that clients come to seek information. It assumes that clients should be able to make their own decisions.
The counselling model is based on the conjecture that clients come for complex reasons.
Perhaps here it would be important to emphasize that both models have positive and negative sides. Providing genetic information is sensitive because of its lifelong implications and thus patients expect and need supportive counselling. Genetic counselling is by all means a multi-step process60. It can be imagined as a series of spirals, where each circle is built on previous efforts. All of these circles represent different implications of genetic counselling - social, psychological and legal55 and the steps which must be passed are: diagnosis, disorder management, mode of inheritance, risk/benefits of possible testing, screening and diagnostic tests, risks assessment andprognosis possibilities.
In both models of genetic counselling, the counsellor’s main role is to provide lifelong medical and psychological support55, to assist people to obtain access to medical services and follow-up care. The counsellors also have another very important task as they must learn to minimize distress in their patients because genetic disorders might evoke complex emotions in the individual or his/her family, such as helplessness, guilt and
fear.
Until everyone, who is involved in the process of genetic counselling, understands the sense and achievements of ''new genetics“, they will hardly understand and won't be able to contribute with a meaningful discussion about it, even if it is based on strong medicalprofessionalism. We must all understand how difficult it is to face our own “genetic horoscope“ and that it becomes more difficult when it concerns members of our family.
Conversations on modern medical genetics becomes more complex when we understand that the genetic code is only one of the three main carriers which determine our life, health and disease – genetics, epigenetics and the environment.
VII. Conclusion
Medical genetics, the science of human biological variations related to health and disease is an inevitable part of modern medical practice. The specificity of hereditary diseases comes from the fact that for now, they cannot be cured, but some can be prevented, and with the proper medical and psychological support the quality of life can be improved.
Medicine has a great capacity to test and screen for gene mutations and chromosomal aberrations, but currently little ability to cure the clinical consequences of these mutations. Because of the newness of this information, and the deterministic way in which many interpret the data, there is a risk that predictive genetic information will be misunderstood and too much weight will be placed on it29.
Considering that we will never be able to control everything around us and especially not our genome, it is important for modern society not be deceived by pseudo-excellence and sophisticated gene selection. We must attempt to create a society which is aware, and set to include those less competent individuals61.
Discrimination, which can hurt people with disabilities, is an issue. The challenge we face is a society which claims to recognize disabled people’s human and civil rights, while at the same time it embraces a social discourse and clinical structures that promote
genetic cleansing62. The key to survival on Earth is in the global setting of moral standards and accepting the limits which cannot be crossed, even though technology can make it possible or available.
Now, more than ever, we need to quest for the real truth behind the purpose of the available knowledge concerning our genome, and an intellectual escape from the nonsensical excellence and manipulation to which we are all exposed. The truth about our genome is the greatest test for the survival of our civilization.
Genetic variation is what makes each human being a unique individual. It also can determine our unique susceptibility to disease. Human diversity may be the secret of humankind’s success. Without diversity, there is no effective selection! Variety is not the spice of life, it is life itself. Instead of promoting genetic ‘search and destroy’ strategies, we should extend our sense of the richness of human life62.
No matter how great our contrasts are, they are still something immaterial. The things we share are far more valuable than those which divide us.
REFERENCES
1. Guttmacher AE, Collins FS. Genomic medicine--a primer. N Engl J Med 2002;347:1512.20.
2. Ansell SM, Ackerman MJ, Black JL et al. Primer on medical genomics. Part VI:
Genomics and molecular genetics in clinical practice. Mayo Clin Proc 2003;78:307.17.
3. Online Mendelian Inheritance in Man, OMIM (TM). McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University (Baltimore, MD) and National Center for Biotechnology Information, National Library of Medicine (Bethesda, MD). Available at http://www.ncbi.nlm.nih.gov/omim/. Accessed May 2nd 2009.
4. Winkelman C. Genomics. What every critical care nurse needs to know about the genetic contribution to critical illness. Crit Care Nurse 2004;24:34.45.
5. Kumar P, Burton BK. Congenital Malformations: Evidence-Based Evaluation and Management. New York: McGraw-Hill Professional, 2008.
6. Pereza N, Zergollern-Čupak Lj, Ostojić S. Electronic databases of human genetic disorders: the fundamentals of differential diagnosis in clinical genetics. Medicina 2009;45:22.37.
7. American Academy of Pediatrics. Serving the family from birth to medical home: a report from the Newborn Screening Task Force. Pediatrics 2000;(6 Suppl 2):383.427.
8. Botkin JR. Research for newborn screening: developing a national framework.
Pediatrics 2005;116:862.71.
9. McCabe LL, McCabe ER. Expanded newborn screening: implications for genomic medicine. Annu Rev Med 2008;59:163.75.
10. The Citizens' Council on Health Care. Newborn genetic screening: The New Eugenics?
CCHC Report April 2009. Available at: www.cchconline.org. Accessed May 2nd 2009.
11. Kerruish NJ, Robertson SP. Newborn screening: new developments, new dilemmas. J Med Ethics 2005;31:393.8.
12. Sutton A. Prenatal diagnosis: Fears and expectations. In: Spagnolo AG, Gambino G, eds. Women’s Health Issues. Rome: Società Editrice Universo, 2003.
13. Vehmas S. Parental responsibility and the morality of selective abortion. Ethical Theory Moral Pract 2002;5:463.84.
14. Parker M. The best possible child. J Med Ethics 2007;33:279.83.
15. Dahl E. Ethical issues in new uses of preimplantation genetic diagnosis: should parents be allowed to use preimplantation genetic diagnosis to choose the sexual orientation of their children? Hum Reprod 2003;18:1368.9.
16. Herissone-Kelly P. Procreative beneficence and the prospective parent. J Med Ethics 2006;32:166.9.
17. American Society of Human Genetics. Board of Directors. Eugenics and the misuse of genetic information to restrict reproductive freedom: ASHG statement. Am J Hum Genet 1999;64:335.8.
18. Sass HM. 'Contract Model' for Genetic Research and Health Care for Individuals and Families. Eubios Journal of Asian and International Bioethics 2001;11:130.29.
19. Ciarleglio LJ, Bennett RL, Williamson J et al. Genetic counseling throughout the life cycle. J Clin Invest 2003;112:1280.6.
20. Marteau TM, Croyle RT. The new genetics. Psychological responses to genetic testing.
BMJ 1998;316:693.6.
21. European Commission. 25 recommendations on the ethical, legal and social implications of genetic testing. Brussels, 2004.
22. Aksoy S. Antenatal screening and its possible meaning from unborn baby's perspective. BMC Medical Ethics 2001;2:E3.
23. Kotalik J. Major concerns about ethics of genetic technology. In: Daniel Monsour, ed.
Ethics and the New Genetics. Toronto: H. University of Toronto Press, 2007.
24. Goh KI, Cusick ME, Valle D et al. The human disease network. Proc Natl Acad Sci U S A 2007;104:8685.90.
25. Rodenhiser D, Mann M. Epigenetics and human disease: translating basic biology into clinical applications. CMAJ 2006;174:341.8.
26. American Association for Cancer Research Human Epigenome Task Force; European Union, Network of Excellence, Scientific Advisory Board. Moving AHEAD with an international human epigenome project. Nature 2008;454:711.5.
27. Ostojić S, Pereza N, Kapović M. A Current Genetic and Epigenetic View on Human Aging Mechanisms. Collegium antropologicum 2009;33:In press.
28. Kaminsky ZA, Tang T, Wang SC et al. DNA methylation profiles in monozygotic and dizygotic twins. Nat Genet 2009;41:240.5.
29. Caulfield T. Underwhelmed: hyperbole, regulatory policy, and the genetic revolution.
McGill Law J 2000;45:437.60.
30. Treves F. The Elephant Man, and Other Reminiscences. London: Cassell, 1923.
31. Doctor Secrets! Medical Information. Available at:
http://www.doctorsecrets.com/amazing-medical-facts/elephant-man/the-elephant-man .html. Accessed May 2nd 2009.
32. Curwen T. “Step by surgical step, a life is transformed”, Los Angeles Times, April 6, 2009. Available at:
http://www.latimes.com/news/local/la-me-ana6-2009apr06,0,3469956,full.story.
Accessed May 2nd, 2009.
33. Hasle H, Clemmensen IH, Mikkelsen M. Risks of leukaemia and solid tumours in individuals with Down's syndrome. Lancet 2000;355:165.9.
34. Sussan TE, Yang A, Li F, Ostrowski MC et al. Trisomy represses Apc(Min)-mediated tumours in mouse models of Down's syndrome. Nature 2007;451:73.5.
35. Kitcher P. The Lives to Come: The Genetic Revolution and Human Possibilities. New York: Simon & Schuster Inc, 1996.
36. Biesecker B, Marteau TM. The future of genetic counseling: An international perspective. Nature Genetics 1999;22:133.7.
37. Burke W, Daly M, Garber J et al. Recommendations for follow up care of individuals with an inherited predisposition to cancer. II. BRCA1 and BRCA2. JAMA
1997;277:997.1003.
38. Greenman C, Stephens P, Smith R et al. Patterns of somatic mutation in human cancer genomes. Nature 2007;446:153.8.
39. Debouck CM. The genome: the beginning, not the end…and a means to many ends.
DDT 2001;6:565.6.
40. Reardon W, Donnai D. Dysmorphology demystified. Arch Dis Child Fetal Neonatal Ed 2007;92:F225.9.
41. Mullen MA. The New Human Genetics: Ethical Issues and Implications for Public Policy. Kansas Medicine 1995;96:2.
42. The Council of Europe. European convention on Human rights. Articles 2, 3. 1976.
43. Macer DRJ. Shaping Genes: Ethics, Law and Science of Using Genetic Technology in Medicine and Agriculture. Christchurch: Eubios Ethics Institute, 1990.
44. Burley J, Harris J. A Companion to Genethics. Blackwell Publishing, 2004.
45. Beauchamp T, Childress J. Principles of biomedical ethics. 5th ed. Oxford: Oxford University Press, 2001.
46. Knoppers BM, Chadwick R. Human genetic research: emerging trends in ethics. Nat Rev Genet 2005;6:75.9.
47. Warren RP. All The King's Men. Harcourt, Brace and Co., 1946.
48. Suzuki D, Knudtson P. Genethics: The Clash Between the New Genetics and Human Values. Cambridge, MA: Harvard University Press, 1990.
49. Otlowski MFA, Williamson R. Ethical and legal issues and the "new genetics". MJA 2003;178:582.5.
50. Macer DRJ. Shaping Genes: Ethics, Law and Science of Using Genetic Technology in Medicine and Agriculture. Christchurch: Eubios Ethics Institute, 1990.
51. Weil J. Psychosocial genetic counseling in the post-nondirective era: A point of view. J Genet Counsel 2003;12:199.211.
52. Zergollern L. Human genetics and ethics. Lijec Vjesn 1990;112:63.6.
53. Zergollern L. The future of human genetics is the faster continuum of the past. Acta Med Croatica 1999;53:55.9.
54. Martin JR, Wilikofsky AS. Genetic counseling in primary care: longitudinal,
psychosocial issues in genetic diagnosis and counseling. Prim Care Clin Office Pract 2004;31:509.24.
55. Biesecker BB. Goals of genetic counseling. Clin Genet 2001;60:323.30.
56. National Society of Genetic Counselors. National Society of Genetic Counselors code of ethics. J Genet Couns 1992;1:41.3.
57. Baker DI, Schutte JL, Unlamann WR. A Guide to Genetic Counseling. New York: Wiley Liso Publications, 1998.
58. Bernhardt B. Empirical evidence that genetic counseling is directive: Where do we go from here? Am J Hum Genet 1997;60:17.20.
59. Kessler S. Psychological aspects o genetic counseling. XI. Nondirectiveness revisited.
Am J Med Genet 1997;72:164.71.
60. Contegiacomo A, Pensabene M, Capuano I et al. An oncologist-based model of cancer genetic counselling for hereditary breast and ovarian cancer. Ann Oncol 2004;15:726.32.
61. Rogers A, de Bousingen DD. Bioethics in Europe. Strasburg: Council of Europe, 1995.
62. Albert B. Human genetic testing: what implications? Dialogue and debate at the European stakeholders' and citizens' conference on the ethical, legal and social aspects of genetic testing. Brussels, 2004. Session 1; page 7. Available at:
http://europa.eu.int/comm/research/genetic2004.html. Accessed May 2nd 2009.
Correspondence
Saša Ostojić, M.D.,Ph.D.
Associate Professor
Department of biology and medical genetics,School of medicine, University of Rijeka, 51000 Rijeka, Croatia
E-Mail: sasa.ostojic@medri.hr
tel:+385-51-651131 fax:+385-51-678896