Telemedicine in Cardiovascular Disease
Chih-Chung Hsiao1, Jui-Peng, Tsai1,2,5, Kuo-Tzu Sung1, Ping-Ying Lee1,2,3, Chi-In Lo3,6, Wen-Hung Huang1, Wen-Lin Chang7, and Chung-Lieh Hung1,2,3,4,7
1Division of Echocardiography and Telemedicine, Division of Cardiology,
Cardiovascular Center/Department of Internal Medicine, 6Division of Critical Care Medicine,
7Telehealth and Home care Center, MacKay Memorial Hospital, Taipei, Taiwan;
2Mackay Junior College of Medicine, Nursing and Management, New Taipei City, Taiwan;
3Department of Medicine, Mackay Medical College, New Taipei City, Taiwan;
4Institute of Clinical Medicine, and Cardiovascular Research Center,
5Department of Biomedical Imaging and Radiological Science, National Yang-Ming University, Taipei, Taiwan
Abstract
Cardiovascular disease is a leading cause of death in the United States. Of all that, the coronary heart disease is the leading cause of deaths, followed by stroke, and high blood pressure. Heart failure is the common presentation of the cardiovascular disease and response for billions of medical cost. As the innova- tions of information technology and mobile wireless device, telemedicine has been utilized in various clin- ical disease to reduce medical cost and improve outcome, especially in cardiovascular disease. Physiologic parameters, such as blood pressure and sugar, heart rate, body weight, peripheral oxygen saturation, and electrocardiogram,are obtained at home and transmitted daily to care-providers. So that, early detection of the warning data before disease worsen, the physicians can adjust the medication and strategies. Several randomized trials and meta-analysis studies have demonstrated the clinical benefits of the telemedicine via invasive implanted device, either risk reduction of mortality or heart failure admission rate.However, there are still arguments and more studies are needed to identify the optimal care model in cardiovascular telemedicine.
(J Intern Med Taiwan 2017; 28: 133-139)
Key Words: Telemedicine, Telemonitoring, Remote monitoring
Introduction
Cardiovascular disease is a leading cause of death in the United States, which may account for near 801000 deaths annually, estimated to be 1 of every 3 deaths.1 Direct and indirect costs of cardio- vascular diseases are estimated to more than $316 billion, which includes both health expenditures
and lost productivity. Among them, coronary heart disease is the leading cause (45.1 percent) of deaths attributable to cardiovascular disease in the United States, followed by stroke (16.5 percent), high blood Pressure (9.1 percent), and the others.
Furthermore, heart failure is a common and complex clinical presentation of most heart diseases, such as coronary artery disease, valvular heart dis-
Reprint requests and correspondence:Dr. Chung-Lieh Hung
Address:Division of Cardiology, Cardiovascular Center/Department of Internal Medicine, Mackay Memorial Hospital, No. 92, Chung-Shan North Road, 2nd Section, Taipei, Taiwan
orders, arrhythmias, cardiomyopathy and hyper- tensive heart disease. Heart failure is responsible for a high hospitalization rate of 24.7/1000 in 1999 to 17.8/1000 person-years in 2011 for those elderly population in the United States and more than $30 billion medical cost.1,2 Owing to the multiple co- morbidities and chronicity of the above mentioned highly prevalent cardiovacular disorders, programs to improve care quality and reduce mortality, hospi- talization rate, re-admission rate and total medical cost are crucial and demanding.
Telemedicine was initially designed for remote diagnosis with instructing the procedure of cardiac defibrillation via telephone but subsequently evolved into a more general clinical care model of early detec- tion and management of several chronic diseases.
As the innovations of mobile technology continues to improve, the wearable wireless device with auto- mated real-time data transmission appeared, and the clinical applications are extended to various clinical diseases. More and more studies were conducted and currently ongoing to sort out the appropriate models for specific subgroup of the cardiovascular diseases.
Telemedicine in Critical Care or Cardiovacular Emergency
Acute ischemic stroke
Some meta-analysis and randomized studies had reported thrombolytic therapy for acute ischemic stroke could be performed safely and effectively via real-time audio and video communication with high speed transmission of images and clinical informa- tion in community hospitals where neurological experts was not available. In that work, the 3 and 6 months follow up showed non-significant difference in mortality or functional independence between telemedicine-guided and experts on-site thromboly- sis.3,4 Therefore, American Heart Association (AHA) and American Stroke Association support the tele- medicine strategies for acute stroke whenever on-site stroke expertise physicians are not available.5
ST-segment elevation myocardial infarction (STEMI)
The use of pre-hospital 12-leads ECGs was sug- gested for early diagnosis of STEMI by emergency medical service paramedics utilizing telemedical equipments, with coupled, real-time communication with a PCI-capable center.6 The strategies of ECG transmission wirelessly to the primary PCI center interpreted by on-call cardiologists has been shown to shorten the primary intervention or thromboly- sis reperfusion time with excellent outcomes, and further supported in current latest AHA STEMI guideline.7
Telemedicine in Heart Failure
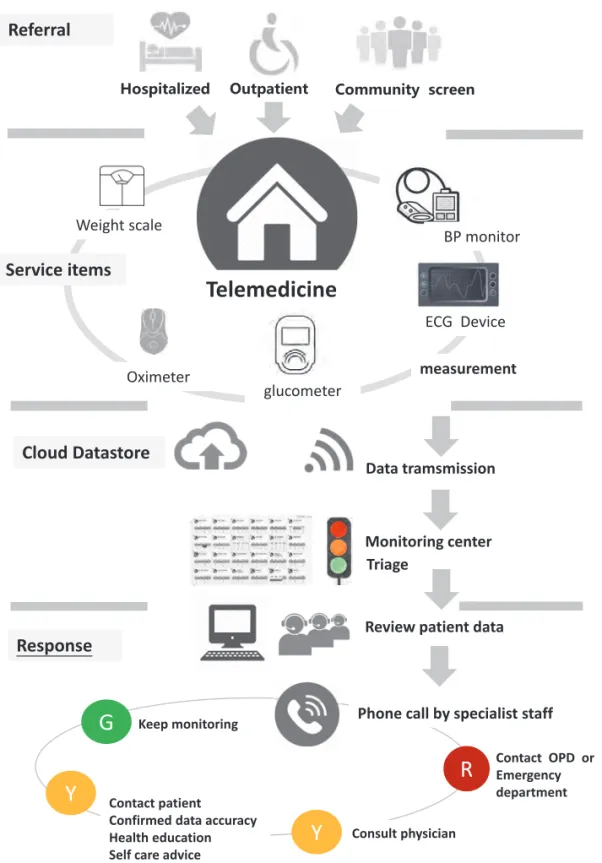
Telemonitoring is a particular medicare model for patients to obtain physiologic parameters at home using equipments with remote data transfer or monitor, such as blood pressure and sugar, heart rate, body weight, peripheral oxygen saturation, and electrocardiogram. These data can be transmit- ted daily via wireless access (Wi-Fi or Bluetooth) or telephone to specific organization or institute (usually hospital-based remote care center or health promotion private company). To date, five main types of non-invasive telemonitoring were identi- fied in one systematic review: (1) video-consulta- tion, with or without transmission of vital signs, (2) mobile telemonitoring, (3) automated device-based telemonitoring, (4) interactive voice response, and (5) Web-based telemonitoring.8 So that the care-pro- viders (nurses or trained specialists) can remotely screened the data and close monitor the patient’s clinical condition without office visits. They can alert the patients to take some action if abnormal parameters were noticed during screen and inform duty physicians to adjust the medication and to modify management strategies of treatment before clinical conditions worsen. (Figure 1) In some coun- tries, the care-provider may directly make a clinical decision to change medications for patients.
So far, this modality has been shown to suc- cessfully reduce heart failure mortality, admis- sion and re-admission rate via recommendation of guideline based medication, and to further guide or monitor device therapies in order to manage
the precipitating causes of heart failure and rel- evant comorbidities, based on a multidisciplinary team care model.9 Numerous systemic reviews and meta-analysis reported that telemonitoring can sub- stantiallly reduce all-cause mortality, heart failure
Figure 1. Workflow of the telemedicine in MacKay Memorial Hospital.
G: Green color means stable condition; Y: Yellow color means alert condition; R: Red color means warning condition.
Hospitalized Outpatient Community screen
Telemedicine
Data tramsmission
Monitoring center Triage
Review patient data
Keep monitoring
Contact patient Confirmed data accuracy Health education Self care advice
Consult physician
Contact OPD or Emergency department
R G
ECG Device
Service items
Y
Y
Phone call by specialist staff measurement
Referral
Cloud Datastore
Response
MacKay Memorial Hospital Telemedicine Workflow
glucometer
BP monitor
Oximeter Weight scale
admission rate, and to further improve quality of life and lower cost.8,10-12 Notwithstanding, some studies showed that remote care delivery only improved quality of life13 or reduction of 30-days readmission rate without benefit on mortality and hospitalization rate.14,15
The largest randomized controlled trial enroll- ing 1653 heart failure patients in the United States by telephone-based interactive voice-response telemon- itoing that collect daily symptoms and body weight was compared to usual care.16 The primary endpoint was readmission for any reason or all-cause mortal- ity at 6 months with secondary endpoints included hospitalization for heart failure. At the end of the study, there were no significant differences between the two groups with respect to the primary or sec- ondary end points. Similar results were observed in another 2 large randomized controlled trials: the BEAT-HF trial, enrolled 1437 patients with HF in the United States, and the TIM-HF trial, enrolled 710 patients in Germany. Both trials showed no dif- ference in mortality or the composite secondary endpoints of cardiovascular death and heart failure hospitalization.17,18
Telemedicine in Arrhythmias
Wearable, non-invasive device: continuous ECG Arrhythmia is responsible for the main cause of syncope, stroke and sudden cardiac death. It is a potentially life threatening condition which may result in serious morbidity, but usually under-detec- tion. Wearable wireless utilizing continuous ECG monitor is clinical validated and allowed up to 24 hours continuous remote transmission of the respira- tory rate, body temperature. ECG rhythm, heart rate and variability. It may increase the diagnosis rate of arrhythmia and impact the strategies of treatment.
One meta-analysis of 25 RCT trials for wearable devices showed wearable devices were associated with decreased mortality [RR (95%CI) =0.76 (0.63, 0.92)] and the risk of hospitalizations [0.81 (0.72,
0.91].19. The study found clinical benefits among younger patients (<70 years) and reduced hospital- izations at 3 months with improved mortality and hospitalizations at 1 year follow up. However, the benefits was not observed among older patients or in study design that enrolled ambulatory patients as contrary to patients recently hospitalized for heart failure.
Implantable Device
The prospective, randomised, single-blinded, CHAMPION study, enrolled 550 NYHA class III heart failure patients, showed clinical benefits with implanted wireless CardioMems system to monitor pulmonary artery pressure.20 The pulmonary artery pressure may increase markedly prior to overt symp- toms of heart failure. The patients were treated base on the changes of pulmonary artery pressure infor- mation. The admission rate for heart failure was 33% decreasein the treatment group compared with the control group (hazard ratio [HR] 0.67 [95% CI 0.55–0.80]; p<0·0001). The sustained benefit could be observed at 18-month (average) follow-up, as well as in the control group during the subsequent open access periods.21 Pulmonary artery pressure infor- mation has became clinically available and useful in guiding therapy after that landmark study. Nev- ertheless, the safety endpoints of device-related or system-related complications were 1.4 percent.
Previously, the intrathoracic impedance and heart rate variability parameters were found to have a role in early detection the symptoms of heart failure.
The former parameter was related to lung water and the later one was associated with post-myocardial infarction mortality, heart failure and various clini- cal conditions. Remote monitor with intrathoracic impedance transmission from Implanted device ICD, or CRT/+D were reported in some studies that demonstrated decreasing of unscheduled visits and better adherence. But there were no significant benefits in all–cause mortality and heart failure
admission rate.22,23 However, the device associated precipitating factors of heart failure exacerbation include atrial or ventricular tachyarrhythmia, inap- propriate defibrillation shocks, low percentage of biventricular pacing, abnormal device function and inappropriate setting or placement, lung fluid accu- mulation, and low heart rate variability.
Recently, the IN-TIME study, randomized con- trolled trial, enrolled 664 patients underwent ICD or CRT-D with chronic heart failure, NYHA class II–
III, ejection fraction of no more than 35%. reported significant reduction of primary endpoint in com- posite death and heart failure admission at 1 year, 63 (18.9%) of 333 patients in the telemonitoring group versus 90 (27.2%) of 331 in the control group (p=0.013) (odds ratio 0.63, 95% CI 0.43–0.90).24 Pos- sible mechanisms response for this findings were early detection of the onset or progression of ventric- ular and atrial tachyarrhythmias, early recognition of suboptimal device function and encouraged patients to take more responsibility for healthy life style, including adherence to medicine. Similar positive result was observed in another retrospective cohort study, which included 269,471 patients implanted with pacemakers, implantable cardioverter-defibril- lators, or cardiac resynchronization therapy with pacing capability (CRT-P)/defibrillation capability (CRT-D) via wireless remote monitoring.25
The prospective randomized CONNECT TRIAL, enrolled 1,997 patients with implantable cardioverter-defibrillators and cardiac resynchroni- zation therapy devices showed significantly reduced the response time to clinical events and the length of CV hospital stay during 15 months follow up.26
Telemedicine in Chronic Diseases (DM, HTN, Sleep Apnea)
Telemedicine was reported to be more effec- tive in control blood sugar and achieved the HbA1c target in one meta-analysis which enrolled 55 ran- domize controlled trials.27 The impact of telemed-
icine in diabetes management and dysglycemic onctrol was more prominent in the first 6 months but decrease overtime.
As compared to usual care, substantial BP reduction was observed in non-diabetic patients in the telemedicine group of the RCT trial.28 The main cause of BP reduction was associated with more pre- scribed medications in the telemedicine group.
Obstructive sleep apnea is a known risk factor associated to cardiovascular disease and tendency to higher blood pressure. One multi-center random- ized controlled trial that compared standard continu- ous positive airway pressure (CPAP) care and CPAP care with a telemedicine support on blood pressure reduction in high cardiovascular risk OSA patients.
The study didn’t found any significant difference on primary outcome of blood pressure reduction or secondary outcome of cardiovascular risk reduction between the 2 groups.29
Challenges of Telemedicine
Despite the widely spread of Telemedicine technologies and medicare models, there remains some challenges in the clinical implementation or use of telemedicine as routine clinical practice: (1) Technical demand on data transmission assurance, diagnostic accuracy and feeedback for subjects at risk in a timely fashion, either in day-time or 24 hours continuos monitor; (2) Financial issue, either from healthcare system or self-pay in any individ- ual affordable for the business model of remote care;
(3), Legal issue, the care system or team members are supposed to take actions to patient’s disease and transmitted biological or physiological information, and how to clarify the responsibility between physi- cian, institute and patients remained to be clarified further.
Conclusion
Telemedicine is designed to reduce unneces- sary hospital visits by implementing health promo-
tion activities in primary health care, to continuously monitor disease condition, to extend disease man- agement after discharge, and thus to improve the clinical treatment efficacy and clinical outcomes.
Several randomized trials and meta-analysis studies have demonstrated the risk reduction on mortality and decreased re-admission rate via more aggresive implanted devices. There are still a few arguments and debates on the generalizibility of such emerging innovations and more studies are needed to provide the most optimal way in the aspect of cardiovascu- lar disorders.
References
1. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017; 135: e146-e603.
2. Krumholz HM, Normand SL, Wang Y. Trends in hospital- izations and outcomes for acute cardiovascular disease and stroke, 1999-2011. Circulation 2014; 130: 966-75.
3. Kepplinger J, Barlinn K, Deckert S, et al. Safety and efficacy of thrombolysis in telestroke: A systematic review and meta- analysis. Neurology 2016; 87: 1344-51.
4. Schwab S, Vatankhah B, Kukla C, et al. Long-term outcome after thrombolysis in telemedical stroke care. Neurology 2007; 69: 898-903.
5. Jauch EC, Saver JL, Adams HP, Jr., et al. Guidelines for the early management of patients with acute ischemic stroke:
a guideline for healthcare professionals from the Ameri- can Heart Association/American Stroke Association. Stroke 2013; 44: 870-947.
6. Diercks DB, Kontos MC, Chen AY, et al. Utilization and impact of pre-hospital electrocardiograms for patients with acute ST-segment elevation myocardial infarction: data from the NCDR (National Cardiovascular Data Registry) ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry. J Am Coll Cardiol 2009; 53: 161-6.
7. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/
AHA guideline for the management of ST-elevation myocar- dial infarction: a report of the American College of Cardiol- ogy Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 127: e362-425.
8. Kitsiou S, Pare G, Jaana M. Effects of home telemonitoring interventions on patients with chronic heart failure: an over- view of systematic reviews. J Med Internet Res 2015; 17: e63.
9. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guide- lines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129-200.
10. Clark RA, Inglis SC, McAlister FA, et al. Telemonitoring or structured telephone support programmes for patients with chronic heart failure: systematic review and meta-analysis.
BMJ 2007; 334: 942.
11. Inglis SC, Clark RA, McAlister FA, et al. Structured tel- ephone support or telemonitoring programmes for patients with chronic heart failure. Cochrane Database Syst Rev 2010:
Cd007228.
12. Pandor A, Gomersall T, Stevens JW, et al. Remote monitoring after recent hospital discharge in patients with heart failure:
a systematic review and network meta-analysis. Heart 2013;
99: 1717-26.
13. Flodgren G, Rachas A, Farmer AJ, et al. Interactive telemed- icine: effects on professional practice and health care out- comes. Cochrane Database Syst Rev 2015: Cd002098.
14. Blum K, Gottlieb SS. The effect of a randomized trial of home telemonitoring on medical costs, 30-day readmissions, mor- tality, and health-related quality of life in a cohort of com- munity-dwelling heart failure patients. J Card Fail 2014; 20:
513-21.
15. Vadlamani L, Anderson K, Kumar S. Using technology to reduce readmission rates for congestive heart failure in high risk patients. J Am Coll Cardiol 2016; 67: 1410.
16. Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure. N Engl J Med 2010; 363: 2301-9.
17. Ong MK, Romano PS, Edgington S, et al. Effectiveness of Remote Patient Monitoring After Discharge of Hospitalized Patients With Heart Failure: The Better Effectiveness After Transition -- Heart Failure (BEAT-HF) Randomized Clinical Trial. JAMA Intern Med 2016; 176: 310-8.
18. Koehler F, Winkler S, Schieber M, et al. Impact of remote tel- emedical management on mortality and hospitalizations in ambulatory patients with chronic heart failure: the telemedi- cal interventional monitoring in heart failure study. Circula- tion 2011; 123: 1873-80.
19. Bhavnani S, Waalen J, Srivastava A, et al. Which patients?
which devices? mhealth monitoring with wearable and implantable devices in heart failure: meta analyses of rand- omized trials. J Am Coll Cardiol 2015; 65: A1030-A.
20. Abraham WT, Adamson PB, Bourge RC, et al. Wireless pul- monary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011; 377:
658-66.
21. Abraham WT, Stevenson LW, Bourge RC, et al. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow-up results from the CHAMPION randomised trial. Lancet 2016; 387: 453-61.
22. van Veldhuisen DJ, Braunschweig F, Conraads V, et al.
Intrathoracic impedance monitoring, audible patient alerts, and outcome in patients with heart failure. Circulation 2011;
124: 1719-26.
23. Varma N, Epstein AE, Irimpen A, et al. Efficacy and safety of automatic remote monitoring for implantable cardioverter- defibrillator follow-up: the Lumos-T Safely Reduces Routine Office Device Follow-up (TRUST) trial. Circulation 2010;
122: 325-32.
24. Hindricks G, Taborsky M, Glikson M, et al. Implant-based
multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet 2014; 384:
583-90.
25. Varma N, Piccini JP, Snell J, et al. The Relationship Between Level of Adherence to Automatic Wireless Remote Monitor- ing and Survival in Pacemaker and Defibrillator Patients. J Am Coll Cardiol 2015; 65: 2601-10.
26. Crossley GH, Boyle A, Vitense H, et al. The CONNECT (Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision) trial: the value of wireless remote mon- itoring with automatic clinician alerts. J Am Coll Cardiol 2011; 57: 1181-9.
27. Su D, Zhou J, Kelley MS, et al. Does telemedicine improve treatment outcomes for diabetes? A meta-analysis of results from 55 randomized controlled trials. Diabetes Res Clin Pract 2016; 116: 136-48.
28. Bove AA, Homko CJ, Santamore WP, et al. Managing hyper- tension in urban underserved subjects using telemedicine--a clinical trial. Am Heart J 2013; 165: 615-21.
29. Mendelson M, Vivodtzev I, Tamisier R, et al. CPAP treatment supported by telemedicine does not improve blood pressure in high cardiovascular risk OSA patients: a randomized, con- trolled trial. Sleep 2014; 37: 1863-70.
遠距醫療在心臟血管疾病的應用
蕭智忠1 蔡瑞鵬1,2,5 宋國慈1 李秉穎1,2,3 羅志賢3,6 黃文弘1 張雯姈7 洪崇烈1,2,3,4,7
馬偕紀念醫院 1心血管中心/內科部 心臟內科 心臟超音波及遠距中心
6重症醫學科 7遠距暨居家照護服務中心
2馬偕醫護管理專科學校 3馬偕醫學院醫學系
國立陽明大學 4臨床醫學研究所及心臟血管疾病研究中心 5生物醫學影像暨放射科學系
摘 要
一直以來,心臟血管疾病在美國佔據死亡原因首位,其中冠狀動脈疾病包含心肌梗塞是 最多數,其次是腦中風,緊接是高血壓性心臟病。然而,心臟衰竭在所有死亡人數中 , 佔據超 過三分之一的比例。大部分心臟血管疾病經常表現出心臟衰竭症狀,包括冠狀動脈疾病、心 律不整、瓣膜性心臟病、心肌病變、及高血壓。這些病患經常因為心臟衰竭症狀而住院,每 年花費大量醫療人力及資源。改善照顧品質,降低住院率及死亡率,進而減少醫療花費就成 為一個重要的議題。隨著資訊科技及無線傳輸醫療儀器的廣泛應用,遠距醫療在眾多醫學次 專科領域因應而起。尤其是在心臟血管疾病應用,包括急性心肌梗塞、腦中風、心律不整、
心臟衰竭、高血壓及糖尿病。許多文獻已證實遠距醫療的好處,然而仍然有部分爭議需要更 多大型臨床試驗數據來釐清疑惑及驗證效益。