國立臺灣大學醫學院職能治療學系 碩士論文
School of Occupational Therapy College of Medicine
National Taiwan University Master Thesis
機器前誘式鏡像治療與雙側上肢練習結合居家轉移練習 方案於中風復健療效:先導性研究
Effects of Robotic Priming of Mirror Therapy and Bilateral Arm Training With a Transfer Package in Stroke
Rehabilitation: A Pilot Study
羅俊雄 Chon-hong Lo
指導教授: 林克忠 博士 Advisor: Keh-chung Lin, ScD
中華民國108年7月
July, 2019
誌謝
光陰似箭,歲月如梭,不知不覺就到了畢業的時候。首先要感謝的是我的指導老 師林克忠教授平日的諄諄指導,在團隊無論在收案及日常運作遭遇大變革之際,仍能 沉著應對,以至團隊仍能繼續運作。在閱讀文獻和研究上遇上不少難題,老師都會耐 心指導,助我解決問題,對我的思考有很大啟發。除了指導老師外,口試委員張雅
如、陳嘉玲和姚開屏教授,在論文撰寫給予我很寶貴的意見及提點,讓我獲益良
多。有賴各位老師的栽培,這兩年的碩班學習非常札實,祝福各位老師身體健康,萬 事順意。
另外, 要感謝婉彣、從善和怡君學姐, 謝謝你們循循善誘, 帶我適應團隊的研究 生活, 在執行研究上給予各種幫助和支持, 毫不分享了自己的經驗,對我提出的問 題知無不答,亦在收案的過程中適時給予不少意見,幫助解決了不少難題,祝福你們 鵬程錦秀。
在團隊中, 感謝于琦、奕宏、家瑋和玉娟,把 IRB 和行政的工作處理得天衣無縫, 令我可專注在收案和研究中,祝福你們前程錦秀。在收案過程中,承蒙臺大醫院和臺 北醫院的治療師們鼎力相助, 謝謝巫怡萱和張婉嫈組長在研究空間及程序上給予協 助, 感謝各位治療師不斷介紹個案給我, 令研究順利進行,祝福各位治療師萬事順 心。最後, 感謝我的家人和朋友, 在背後默默支持和陪伴, 令我在學習過程中得以
舒發壓力和大膽做每個決定。由衷感激這兩年來陪伴我的人,由此獻上此論文,願
大家能一起分享此喜悅。
中文摘要
研究背景和目的:中風在台灣仍是主要健康照護負擔之一。當代的復健療法包含 鏡像療法、雙肢練習,和機器輔助療法。雙側上肢練習及鏡像治療,皆基於雙側練 習引發雙腦耦合的密集練習概念,唯鏡像治療較雙側上肢練習增加了由鏡像產生的 視覺回饋。本研究的目的為探討雙側機器誘導雙側上肢練習與雙側機器誘導鏡像治 療對慢性中風患者的感覺運動功能,日常功能,自我效能和生活質量的療效。
研究設計:採用隨機分派、單盲試驗設計,進行前測,後測和追蹤測評估。慢性 中風患者被隨機分派至雙側機器誘導雙側上肢練習組(RBAT)或雙側機器誘導鏡像 治療組(RMT)。所有患者每次接受 90 分鐘的治療,每週 3 天,連續 6 週,共 18 次治療。
成效評量:結果測量包括:傅格梅爾動作量表 (Fugl-Meyer Assessment)、英國醫 學研究顧問團體量表 (Medical research council scale)、修訂版諾丁漢感覺評 估量表(Revised Nottingham Sensory Assessment)、沃夫動作功能測驗(Wolf Motor Function Test)、功能性獨立測驗(Functional independent
measure)、動作活動記錄表(Motor Activity Log)、ABILHAND 問卷(ABILHAND Questionnaire)、中風影響量表(Stoke Impact Scale)、目標達成量表(goal attainment scale)、諾丁漢延伸性日常生活量表(Nottingham Extended
Activities of Daily Living Scale)和腕動計測量活動度。所有參與者進行三次
評估(治療前,治療後和三個月後)。 本研究使用 Wilcoxon signed-rank test 和 Mann-Whitney U test 分析組內和組別間差異。
結果:共有 17 名參與者隨機分配到兩組。各組之間沒有基線差異。兩組參與者在 各評估量表有顯著進步並能維持至追蹤測。在主要指標中,RMT 組在傅格梅爾動作 量表和修訂版諾丁漢感覺評估量表上較有進步趨勢。在次要指標中,RMT 組在諾丁 漢延伸性日常生活量表和中風影響量表上較有進步趨勢。另一方面,RBAT 組在目 標達成量表上發現了較有進步趨勢。
結論:本研究的初步研究顯示雙側機器誘導鏡像治療在運動能力方面顯著比雙側
機器誘導雙側上肢練習有更大進步,在感覺功能、日常生活活動和生活質量較有進
步趨勢。另外,雙側機器誘導雙側上肢練習則在實現自我復健目標上較有進步趨
勢。本研究是前軀研究,且樣本數不足,未來需要招募更多受試者來進一步深入研
究療效結果。
關鍵字: 雙側機器誘導,雙側上肢訓練,鏡像治療,中風
Abstract
Background and Study Purpose: Stroke is one of the major medical conditions that leads to long-term disability and causes heavy health care. Current evidence indicates that robot-aided therapy, mirror therapy (MT), and bilateral arm training (BAT) are prominent approaches to improve upper extremity motor function and daily function in patients with stroke. These approaches are bilateral approaches to intensive practice based on theories of neuroplasticity. The purpose of this study is to examine the effects of bilateral robotic priming combined with BAT versus bilateral robotic priming combined with MT on sensorimotor function, daily function, self-efficacy, and quality of life in patients with chronic stroke.
Methods: A randomized and single-blinded trial design with pretest, posttest and follow- up assessment was conducted. Participants with chronic stroke were randomly assigned to receive bilateral robotic priming combined with BAT (RBAT) or bilateral robotic priming combined with MT (RMT). All participants received a daily 90-minute therapy session, 3 days/week for 6 weeks, for a total of 18 sessions.
Outcome Measures: The outcome measures were included: upper extremity Fugl-Meyer Assessment (FMA-UE), Revised Nottingham Sensory Assessment (rNSA), Medical Research Council (MRC), Motor Activity Log (MAL), Functional Independence
Measure (FIM), Nottingham Extended Activities of Daily Living Scale Stroke (NEADL), Goal Attainment Scaling (GAS), Impact Scale Version 3.0 (SIS) and the wrist-worn accelerometers. All participants were assessed three times (before, immediately after
intervention and follow-up test). The Wilcoxon signed-rank test and Mann-Whitney U test was used for statistical analysis.
Results: A total of 17 participants were enrolled and randomly assigned to the two group.
There were no baseline differences between groups. Both conditions demonstrated significant within-group improvements in outcome measures and retained the
improvements to 3 months. In primary outcome measures, a positive trend was observed in the RMT group in the FMA-UE, rNSA. In the secondary outcome measures, a positive trend was found in RMT group on NEADL and SIS. On the other hand, a positive trend was found in RBAT group on GAS
Conclusion: On the primary outcomes, the RMT group significantly gained greater benefit on motor ability than the RBAT and a positive trend on sensory function. On the secondary outcomes, the RMT group showed positive trends on IADL and quality of life.
On the order hand, RBAT group show a positive trend on the achievement of self- expectation. More participants are needed to support this preliminary findings.
Key words: bilateral robotic priming, bilateral arm training, mirror therapy, stroke rehabilitation
Contents
誌謝………..………i
中文摘要……….……ii
ABSTRACT………...…...….iv
CONTENTS………vi
LIST OF FIGURES………..………viii
LIST OF TABLES……….…….ix
Chapter Ⅰ Introduction……….………..………...1
1.1 Background and Purpose………...……....1
1.2 Study Hypotheses………..…...5
Chapter Ⅱ Methods……….……….6
2.1 Study design ………...6
2.2 Participants………..……...…6
2.3 Intervention Protocols and setting……….…7
2.4 Interventions………. 8
2.5 Outcome Measures………... 10
2.6 Data Analysis………...…..16
Chapter Ⅲ. Result………...………..…...……..17
3.1 Participants’ baseline characteristics……….…………..….17
3.2 Effects of Intervention on the Primary Outcome Measures …………...…...18
3.3 Effects of Intervention on the Secondary Outcome Measures ……….……...19
3.4 Possible adverse effect………..………...……22
Chapter Ⅳ. Discussion………..…23
4.1 Summary of the Study Results………...………..……23
4.2 The Benefits of RMT group………....…….24
4.3 The Benefits of RBAT group………...……25
4.4 Study Implication………...26
4.5 Study Limitation………..…26
Chapter Ⅴ. Conclusions……….………..……..…28
References………..29
LIST OF FIGURES
Figure 1. Flow Chart of the Study Procedure………...……….36
Figure 2. Experimental Materials and Setting………..…37
Figure 3. Treatment Procedures for two groups………..………..…39
Figure 4. The changes on FMA-UE score………...………..…40
Figure 5. The changes on rNSA score……..………...………..…40
Figure 6. The changes on MRC score……..………...……….………..…41
Figure 7. The changes on ABILHAND score……..………...….………..…41
Figure 8. The changes on WMFT-Time score……….………...….………..…42
Figure 9. The changes on WMFT-Quality score……….………...….………..…42
Figure 10. The changes on CAHAI score……….………...….………..…43
Figure 11. The changes on MAL score……….………...….………..…43
Figure 12. The changes on NEADL score……….………...….…...……..…44
Figure 13. The changes on FIM score……….………...….…….…..…44
Figure 14. The changes on GAS score……….………...….…….…..…45
Figure 15. The changes on SIS score……….………...….…….………45
Figure 16. The changes on Actigraphy score……….………...….…….…....…46
LIST OF TABLES
Table 1. Descriptive and Inferential Statistics of clinical characteristics….……….47
Table 2. Descriptive and Inferential Statistics of FMA-UE by group.………...…...……48
Table 3. Descriptive and Inferential Statistics of FMA-UE from posttreatment to follow- up by group………49
Table 4. Descriptive and Inferential Statistics of rNSA by group.………...…...……50
Table 5. Descriptive and Inferential Statistics of MRC by group.………...…...….…51
Table 6. Descriptive and Inferential Statistics of ABILHAND by group……...…...……52
Table 7. Descriptive and Inferential Statistics of WMFT by group.………...……53
Table 8. Descriptive and Inferential Statistics of CAHAI by group………..54
Table 9. Descriptive and Inferential Statistics of MAL by group………..55
Table 10. Descriptive and Inferential Statistics of MAL from posttreatment to follow-up by group………...……..56
Table 11. Descriptive and Inferential Statistics of NEADL by group………..57
Table 12. Descriptive and Inferential Statistics of FIM by group………...…..58
Table 13. Descriptive and Inferential Statistics of GAS by group………..………..59
Table 14. Descriptive and Inferential Statistics of SIS by group……….………..60
Table 15. Descriptive and Inferential Statistics of SIS from posttreatment to follow-up by group……….………...……..61 Table 16. Descriptive and Inferential Statistics of the ratio of affect and nonaffect arm activity counts………62 Table 17. The summary table of results………...………..63 Table 18. Descriptive and Inferential Statistics of MAS by group………64
Chapter Ⅰ. Introduction
1.1 Background and Purpose
Stroke remains a leading cause of permanent disability and is a large source of disease burden in the world. Upper limb (UL) paralysis is one of the most common and persistent disabilities after stroke. UL paresis can lead to deficits in motor control, motor
dysfunction, and in participating in activities of daily. Therefore, developing and
providing effective therapeutic techniques to improve UE motor control and recovery is crucial. The goal of neurorehabilitation is to restore and maximize physiological function, activities of daily living (ADL), and quality of life for patients with neurological
disorders. Current evidence indicates that robot-aided therapy, mirror therapy (MT), and bilateral arm training (BAT) are prominent approaches to improve upper extremity motor function and daily function in patients with stroke. These approaches are bilateral
approaches to intensive practice based on theories of neuroplasticity.
Bilateral arm training (BAT) is provided in different forms, such as symmetric or alternating patterns, task-oriented or non–task-oriented practice, robots, or auditory cueing (Coupar et al., 2010). Bilateral upper limb training has been shown to activate the central nervous system (McCombe Waller & Whitall, 2008) and activate similar neural networks in both hemispheres of the brain, promoting neural plasticity and cortical repair that may result in improved motor control of the affected arm. Previous studies
demonstrated that BAT reduced motor impairment, increase grip strength, and improve motor control (Lin et al., 2010). However, BAT may not provide enough practice
relevant to bilateral complementary tasks, such as opening a jam jar, occurring in daily living situations that require a differentiated role for each hand (Lin et al., 2010). Recent research has explored the effects of BAT in improving upper limb function and ADL performance in hemiplegic stroke patients and found that BAT combined with
conventional occupational therapy is more effective than occupational therapy alone for improving upper limb function and ADL performance (Lee et al., 2017).
Mirror therapy (MT) is a rehabilitation therapy in which a mirror is placed between the arms so that the mirror box blocks the vision of the paretic arm, and the individual can only see the actual movements of the non-paretic arm and its mirror reflection. The image of the non-affected limb gives the illusion of normal movements in the affected limb. At the same time, the participant is encouraged to move the paretic arm along with the mirror reflection. MT could induce greater improvements in motor functions movement control strategies, and activities of daily compared with conventional occupational therapy (Lin et al., 2014; Wu, Huang, et al., 2013). In addition to MT treatment alone, MT combined with afferent stimulation improved manual dexterity, ambulation function and daily function, and led to reduced motor impairment and synergistic shoulder
abduction (Lee et al., 2015; Lin et al., 2014; Lin et al., 2014). The findings support the benefit of MT as an alternative regimen to BAT. Both MT and BAT are functionally based and task-specific in the nature of their practice. As a restriction, the number of repetitions in these formats of practice is limited. A priming procedure that may be implemented prior to functional task practice may augment the treatment effect. Robotic therapy is technology-based and relevant to serve the purpose of movement priming.
Robot-assisted therapy (RT) is an emerging intervention approach that provides high- intensity, high-repetition, and task-specific training to enhance motor learning and control in patients with stroke (Hsieh et al., 2016). Previous studies demonstrated that RT
provides better or different improvement for patients with stroke compared with dose- matched therapist-based rehabilitation (Liao et al., 2012), and higher intensity of RT could lead to greater improvements in motor ability and functional performance than lower intensity of RT (Hsieh et al., 2011). However, because of the limitation of RT devices that focusing on specific joint movements, RT lack functional practice and linkage to daily life (Hung et al., 2016). In order to optimize the effect of RT treatment, several studies combined RT with different therapies.
Combining RT with the constraint-induced therapy (CIT) in a sequential manner and found that the combined group addictively improved motor control strategies, motor function, and functional independence of instrumental activities of daily living compared with the monotherapy (Hsieh et al., 2016). Also, patients who received the task-oriented intervention immediately after RT had greater improvement in self-reported strength and disability degrees than patients who received task-oriented intervention alone (Hsieh et al., 2017). However, the evidence of RT on QOL improvement is insufficient. RT
protocols should be modified, such as combining RT with bilateral arm training or mirror therapy to intensify the treatment and enhance the benefits on functional outcomes pertaining to the trained task activities. Moreover,the BRT training in con-junction with a 10-minute sensorimotor stimulation program can have benefits for motor restoration in the affected upper extremities of chronic stroke patients. The experience of normal
proprioceptive feedback and neuro-physiological adaptation through repetitive- and- intensive bilateral movement practice can help restore patients’ motor capability in affected upper limbs. (Hsu et al., 2019)
Motor priming in neurorehabilitation can be defined as a change in behavior on the basis of previous stimuli and is an emerging strategy to facilitate motor relearning
(Stoykov & Madhavan, 2015). Various types of priming techniques have been developed, including movement- or stimulation-based priming. Bilateral priming is a type of
movement-based priming technique which involves bimanual, repetitive, and mirror- symmetric movement training before functionally-based rehabilitative therapy. Bilateral priming may promote brain plastic change after stroke for improved functional recovery (Stinear et al., 2008). Bilateral priming of conventional rehabilitation therapy may facilitate or accelerate improvements in upper-limb motor function for chronic stroke (Stinear et al., 2008) and subacute stroke (Stoykov & Stinear, 2010) at follow-up assessments. Previous research indicated that bilateral robotic training can be used as a priming technique that in which both arms can be passively or actively moved in a progressive manner to improve upper limb motor function, affected arm use, and reduce compensatory movements (Wu, Yang, et al., 2013). As a therapeutic possibility, bilateral robotic therapy may be used in combination with different task-oriented therapies (Hsieh et al., 2017) such as MT and BAT and may yield differential benefits. This project aims to investigate the comparative efficacy of these different combinatory approaches based on the tenet of bilateral movement practice approach
Mirror therapy (MT) and bilateral arm training (BAT) are both task-oriented and bilateral movement practice, but mirror therapy provides additional mirror visual feedback. Whether the mirror visual feedback in MT may lead to differential benefits comparing with the BAT is unclear. In addition, bilateral robotic priming of MT versus BAT may lead to differing effects, depending on the domain of treatment outcome. To address these issues, the purpose of this study is to examine the treatment effects of bilateral robotic priming combined with bilateral arm training approach versus bilateral robotic priming combined with mirror therapy on sensorimotor function, daily function, self-efficacyand quality of life in patients with stroke.
1.2 Study Hypotheses
The hypotheses of this study described as follows: (1) we hypothesized that the RMT and RBT will lead to improvements on the study outcomes immediately after the
intervention and at 3-month follow-up.; (2) we hypothesized that the RMT and RBAT will lead to differential effects on the study outcomes.
Chapter Ⅱ. Methods
2.1 Study design
We used a single-blind randomized controlled design to compare the effects of two treatments regimens. There were two group in this study: (1) Bilateral robotic priming combined with bilateral arm training group (RBAT) and (2) Bilateral robotic priming combined with mirror therapy group (RMT). Eligible outpatient participants were randomized into the RMT or RBAT group using a computerized random number table.
2.2 Participants
Occupational therapists screened and recruited 20 community-dwelling patients between November 2018 and July 2019 from the occupational therapy departments at three hospitals in Taiwan. The institutional review boards of the participating hospitals approved the study. Participants were blind to the study hypotheses. During the
intervention period, participants stopped their original occupational therapy sessions, but other routine rehabilitation programs (e.g., physical therapy) were conducted as usual.
A total of 17 participants were enrolled in this study. The inclusion criteria were as follows: (1) ⩾3 months onset from a first-ever unilateral stroke; (2) aged from 18 to 80 years; (3) baseline upper extremity motor score on the Fugl-Meyer Assessment >18 (Fugl-Meyer et al., 1975); (4) no severe spasticity in any joints of the affected arm (Modified Ashworth Scale ⩽ 3) (Charalambous, 2014); (5) able to follow study
instructions (Mini-Mental State Examination Score ⩾24) (Skidmore et al., 2010); (6) no
serious vision deficits and no other neurologic or major orthopedic diseases; (7) able to participate in a rehabilitation intervention program for 6 weeks; (8) no participation in other studies during the study period and willing to provide written informed consent.
2.3 Intervention Protocols and setting
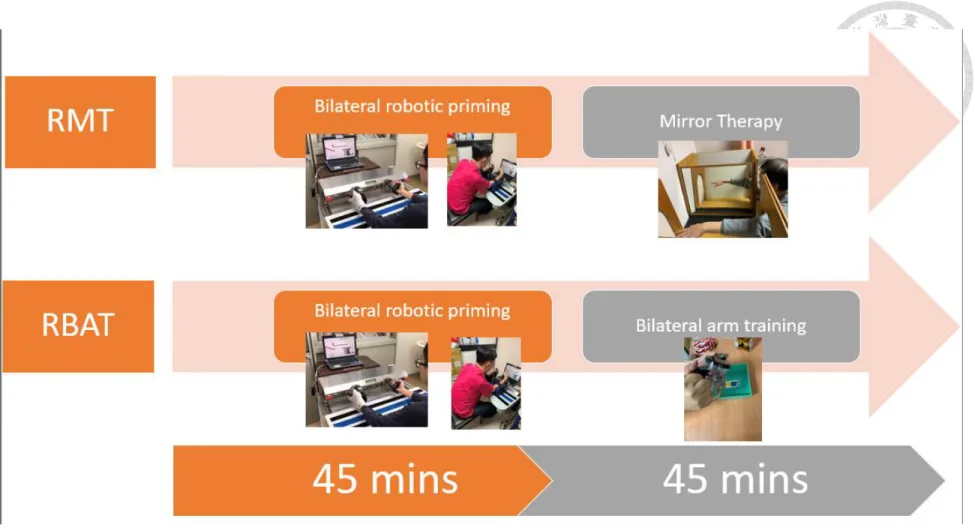
This study was a single-blind, randomized-block controlled trial with pretest and posttest. Participants received a daily 90-minute therapy session, 3 days/week for 6 weeks, for a total of 18 sessions. All treatment groups received 40 to 45 minutes of bilateral robotic priming and 40 to 45 minutes of bilateral arm training or mirror therapy.
In order to make the patient a more active participant in their own improvement at daily life, transfer package was used in conjunction rehabilitation regimens and carried out in a relatively brief period of time. All participants received transfer package and 30-minute home practice, 5 days/week for 3 months. (Fig.3)
The Bi-Manu-Track (BMT) robot (Reha-Stim Co., Berlin, Germany) (Fig.2A) used as the robotic priming practice in the two experimental groups. Participants set at a height- adjustable table, with elbows bent at 90°, placed in the mid position into the arm troughs, and with hands grasping 3-cmdiameter handles so that the movement practiced was restricted to the arm and would not involve the trunk. Computer games such as picking up and placing apples to make apple jam was used to provide visual feedbacks to facilitate participation and motivation during the robotic therapy session. The BMT enables 2 mirror-like movements: forearm pronation-supination and wrist flexion- extension with three computer-controlled modes. Each movement pattern has three
computer-controlled modes: (1) passive-passive, with both arms being moved by the machine with speed and range of motion individually adjustable; (2) active-passive, with the unaffected arm driving the affected arm in a mirror-like fashion; and (3) active-active, with both arms actively moving against resistance. The speed of movement, the amount of resistance, and the range of movement can be adjusted individually on the BMT.
2.4 Intervention
2.4.1 Bilateral robotic priming combined with bilateral arm training (RBAT)
Participants in this group received bilateral robotic priming and bilateral arm training within the 90-minute training sessions. Specifically, the participants will first receive 40 to 45 minutes of bilateral robotic priming using the BMT. During the bilateral priming process, the device will first move both arms passively and then progress to movements by passive-passive, active-passive and active-active modes. The range of motion, resistance, and speed of the movements can be adjusted individually. Participants are expected to perform approximately a total of 1,200 to 1,600 repetitions of movements as bilateral robotic priming. After the robotic priming, participants received another 40 to 45 minutes training in tasks focusing on bilateral symmetric movements of both ULs. The activities performed by the participant may involve 5-minute intransitive movements (e.g., elbow flexion/extension or forearm pronation/supination) (Fig.2C-2D)(Fig.2B) and 35 to 40 minutes’ transitive task (Fig.2F) (e.g., flipping cards, scooping soup out of a bowl or wiping the table), depending on the level of UL function.
2.4.2 Bilateral robotic priming combined with mirror therapy (RMT)
Participants in this group received bilateral robotic priming and mirror therapy within one 90- minute training session. Similar to the RBAT group, the participants will first receive 40 to 45 minutes of bilateral robotic priming delivered by the BMT with the same priming protocol. After bilateral robotic priming, participants will receive 40 to 45
minutes of mirror therapy. During mirror therapy, a wooden mirror box (41cm ×50 cm
×33cm) (Fig.2B) was placed in front of the participant. The mirror box is designed to block the participant’s view of the paretic UL performance; thus, the participant can only see the less paretic UL and its mirror image. The participants were asked to use their less paretic UL to perform certain functional tasks, and to observe the less paretic UL
movements reflected from the mirror. The participants were instructed to look at the mirror and imagined that the movement reflection is performed by their paretic arm.
Also, the therapist encouraged the participant to perform the task with their paretic UL behind the mirror as symmetrically as possible. The mirror therapy protocol was similar to that of bilateral arm training except for the use of mirror feedback in MT. The
activities and tasks (Fig.2E) performed by the participant depending on the level of UL function and the participants’ personal need for recovery.
2.4.3 Transfer Package
In transfer package, a consent form for a “behavioral contract” was obtained.
Participants chose 6 specific ADL tasks from Motor Activity Log and a wrote check-off sheet 6 specific ADL tasks in which the more-affected arm should be used, with 3 easy
tasks for that participant and 3 more difficult. Participants agreed that they would use the affected arm for specific activities of daily living items during real-life situations.
Additionally, the participants were asked to finish the 30-minute home practice, 5 days/week. The home practices were structure activities that relate to the treatment. For the treatment period, the diary was reviewed in detail with the therapist (Fig.2G). For the follow up period, weekly phone contacts were used to monitor the execute efficiency.
2.5 Outcome Measures
The following outcome measures are selected because they are relevant for stroke rehabilitation trials and are in line with the International Classification of Functioning, Disability and Health framework to facilitate interpretability of the functional
significance of treatment outcomes (Lemmens et al., 2012). The primary treatment outcomes pertain to change in sensorimotor recovery and daily activity performance.
2.5.1 Primary outcomes
1. Fugl-Meyer Assessment (FMA).
The upper-extremity subscale of the FMA will be used to assess motor impairment (Fugl-Meyer et al., 1975). There are 33 upper extremity items measuring the movements and reflexes of the shoulder/elbow/forearm, wrist, hand, and coordination/speed. Each score is on a 3-point ordinal scale (0 = cannot perform, 1 = performs partially, 2=
performs fully). The maximum score is 66, indicating optimal recovery. The subscale score of a proximal shoulder/elbow (FMA s/e: 0-42) and a distal hand/wrist (FMA h/w:
0-24) will be calculated to investigate the treatment effects on separate upper extremity
elements. The FMA has good reliability, validity, and responsiveness in stroke patients (Hsieh et al., 2009; Platz et al., 2005).
2. Medical Research Council (MRC)
The MRC will be used for measurement of muscle strength of the affected arm. The muscle strength of shoulder flexors/abductors, elbow flexors/extensors, wrist
flexors/extensors, and flexors/extensors of the metacarpophalangeal joints will be evaluated by the 6- point ordinal scale (0 = no contraction, 1 = flicker or trace
contraction, 2 = active movement with gravity eliminated, 3 = active movement against gravity, 4 = active movement against gravity and resistance and 5 = normal power) and the average MRC score will be calculated. The MRC demonstrates reliability in muscle power measurement (Gregson et al., 2000; Hsieh et al., 2011).
3.Revised Nottingham Sensory Assessment (rNSA).
The rNSA will be used to evaluate changes in sensation. Various sensory modalities will be utilized to assess the tactile sensation, proprioception, and stereognosis of
different segments of the body. Scoring of rNSA is based on a 3-point ordinal scale (0-2), with a lower score suggests greater sensory impairment. The psychometric properties have been established for patients with stroke(Lincoln et al., 1998).
4. ABILHAND Questionnaire.
The ABILHAND Questionnaire will be used to evaluate the ability of the UL in functional activities. It consists of 23 bimanual activities that measure subjectively perceived difficulty in performing some common activities in daily living, such as
buttoning, cutting nails, and opening a bottle. The scale ranges from 0 to 3 (0 = cannot perform, 1 = performs partially or with great difficulty, 2 = performs with some
difficulty, 3 = performs fully). Its reliability and construct validity has been confirmed in stroke patients(Penta et al., 2001)..
2.5.2 Secondary outcomes
5. Wolf Motor Function Test (WMFT).
The WMFT was designed to assess the effects of CIT on arm function after stroke and traumatic brain injury. There are 15 function-based and 2 strength-based tasks. For timed functional tasks, completion times from 0 to 120 seconds are averaged. For functional ability scoring, 6-point ordinal scales are used, where 0 indicates “does not attempt with the involved arm” and 5 indicates “arm does participate, movement appears to be normal.”
6. Motor Activity Log (MAL).
The MAL consists of 30 structured questions to interview how the patients rate the frequency (amount of use subscale) and quality (quality of movement subscale) of movements while using their affected arm to accomplish 30 daily activities. The score of each item ranges from 0 to 5, with a higher score indicating more frequent use or higher quality of movement. The summary score is the mean of the item scores.
7. Chedoke Arm and Hand Activity Inventory (CAHAI)
The CAHAI evaluated the ability to perform functional task with both arms and the affected arm included as much as possible, rather than the affect arm only. It included 13 functional activities. Participants were encouraged to completed all activities with both hands. Each activity was scored on a 7-point ordinal scale (1=total assistance, 2=maximal assistance, 3=moderate assistance, 4=minimal assistance, 5=supervision, 6=modified independence, 7=complete independence). The total score ranged from 13 to 91 points.
8. Functional Independence Measure (FIM).
The FIM consists of 18 items grouped into 6 subscales measuring self-care, sphincter control, transfer, locomotion, communication, and social cognition ability (Hamilton, 1987). Each item is rated from 1 (complete assistance) to 7 (complete independence), as determined by the (Hamilton et al., 1994) required level of assistance to perform the tasks, with a higher score (maximum score, 126) indicating less disability. The FIM has good inter-rater reliability, construct validity, and discriminant validity.
9. Nottingham Extended Activities of Daily Living Scale (NEADL).
The NEADL consists of 22 items scored on the basis of the requirement for help in performing the activity. There are four subscales (mobility, domestic, leisure and kitchen) and a total score. The scores range from 0 to 22, with higher scores representing better function. The psychometric properties of the NEADL have been validated in stroke patients .
10. Goal Attainment Scaling (GAS).
The GAS will be used for measurement the achievement of each participant’s expectation in the course of intervention. According to the principle of SMART (i.e.
specific, measurable, attainable, realistic and timely), the individual intervention goals related to daily activity will be negotiated by the therapists and participants. The goals will be set prior to the intervention and scored on the day before the treatment (pretest), the 3-week interim test and after 6 weeks of treatment (posttest). For the goals potentially achievable and not overly ambitious, each goal will be rated on a 5-point ordinal scale with the level of attainment captured (+2 = a much better than expected level, +1 = a somewhat better than expected level, 0 = the expected level of achievement, -1 = a
somewhat less than expected level, -2 = a much less than expected level). The importance and the difficulty for each goal will be scored also based on a 3-point ordinal scale (1 to 3). The overall GAS score will be calculated by the following formula:
, where I indicates the importance, D is the difficulty, and L is the baseline level in the baseline GAS score or the attainment level in posttest GAS score. GAS scores meet the assumption of normal distribution and represent a standardized score. A GAS score larger than 50 refers to an above-expected performance (Eftekhar et al., 2016; Turner-Stokes, 2009).
11. Stroke Impact Scale Version 3.0 (SIS 3.0).
The SIS 3.0 is a stroke-specific health-related quality of life instrument (Duncan, Bode, Lai, & Perera, 2003). It consists of 59 items assessing 8 domains (i.e., strength,
hand function, activities of daily living/instrumental activities of daily living, mobility, communication, emotion. memory and thinking and participation) with a single item assessing perceived overall recovery from stroke. Items are rated on a 5-point Likert scale, with lower scores indicating greater difficulty in task completion during the past week. The SIS 3.0 has satisfactory reliability, validity, and responsiveness in stroke patients (Duncan, et al., 2003).
12. Wrist-worn accelerometers.
ActiGraph GT3X+ accelerometers were used to provide an objective measure of the amount the affected arm was used in the patient’s real-life situation. The participants wore the triaxial ActiGraph GT3X+ on each wrist for 3 consecutive days, before and after treatment. The ActiGraph accelerometers were only used in the P-IMT and D-IMT groups because of a limited number of devices. The ActiLife 6.10 software (ActiGraph, Pensacola, FL, USA) was used to process acceleration data. The raw data were integrated into 60-second epochs. The ratio of affect and nonaffect arm activity counts.
2.5.3 Possible adverse effect
Modified Ashworth Scale (MAS)
Possible adverse effect was evaluated for muscle tone. The MAS grades spasticity from 0 (no increase in muscle tone) to 5 (affected part is rigid in flexion and extension;
(Bohannon & Smith, 1987). We calculated the mean scores of the overall, proximal (shoulder and elbow), and distal (forearm, wrist, and finger) portions of UE muscle tone
2.6 Data Analysis
All statistical analyses will be conducted using SPSS 25.0 software (SPSS Inc, Chicago, IL, USA). Considering the sample size and the distribution of data, the
nonparametric statistics is used in all statistical analyses. We used Fisher’s exact test for categorical data and the Mann–Whitney U test for continuous variables to compare the baseline differences among the two groups. The pretest, posttest and follow up
differences within each group were analyzed using the Wilcoxon signed-rank test.
Treatment efficacy was calculated by computing the change scores from pretest to posttest. Treatment efficacy among groups was compared using the Mann–Whitney U test with the change scores between pretest and posttest. The effect size (r) was calculated with the following formulas for each variable to illustrate the magnitude of group
difference:
with an r of at least .50 for a large effect, .30 for a moderate effect, and .10 for a small effect.
In order to discuss the relationship betweenthe subjective and objective amount the affected arm was used, the spearman correlation is used to calculate the relationship between the change score of wrist-worn accelerometers and MAL (Amount of use) change score.
Chapter Ⅲ. Result
3.1 Participants’ baseline characteristics.
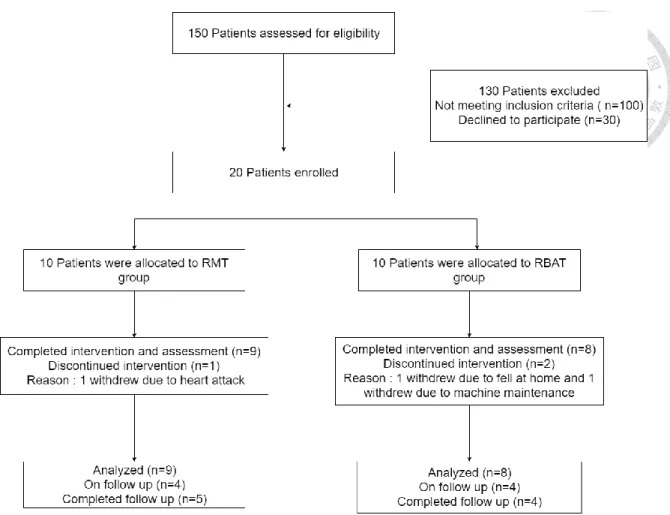
In this study, we enrolled 3 hospitals in Taiwan from November 2018 to July 2019, a total of 150 participants were screened; 130 were excluded due to not meeting the study criteria or refused to participate. Therefore, twenty participants were recruited for study and randomly assigned to one of two group. According to the result of randomization, there were ten participants in RMT group, and ten participants in RBAT group. However, 1 participant discontinued the intervention due to heart attack from the RMT group, two participants dropped out due to fell at home and machine maintenance from RBAT group.5 participants in RMT group and 4 participants in RBAT group finished the
follow-up test (Fig.1). Of the seventeen participants, 10 were male and 7 were female, the average age was 57.60±8.64 years, and their average time after stroke onset was
22.30±17.91 months, indicating all participants were in the chronic stage of stroke. There were 4 participants with right hemisphere lesion and 13 with left hemisphere lesion; 8 participants with ischemic stroke and 9 participants with hemorrhage stroke. In addition, their average score of FMA-UE was 32.35±5.98 indicating their severity of upper limbs impairment was moderate; their baseline score of MMSE score was 26.53±2.45. o statistically significant differences were found for the baseline characteristics of the participants among the 2 groups (Table 1).
3.2 Effects of Intervention on the Primary Outcome Measures
The results of descriptive statistics by group on the primary outcome measures were shown in Table 2-5, the change scores were shown in Figure 4-7.
On the motor functions assessed by FMA-UE, the mean change scores of the overall FMA–UE were 12.00 points in the RMT group, 4.83 points in the RBAT group. The pretreatment to posttreatment changes in the scores of the two groups were significant on the overall, proximal and distal FMA–UE. However, both two groups had nonsignificant result from posttreatment to follow-up test (both p>0.05). The differences among the two groups were significant on the overall score with a moderate effect size in favor of the RMT group over the RBAT group (overall r = 0.49, p = .04; proximal r = .31, p = .19).
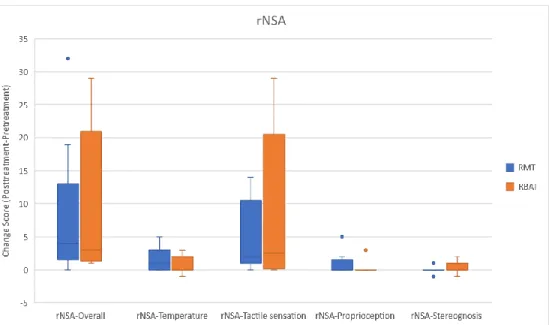
On the sensory functions assessed by rNSA, the mean of the overall score increased 1.00 in the RMT group and 1.50 in the RBAT group. For within comparison, the
pretreatment to posttreatment changes in the scores of the RMT group was significant on the overall, temperature, tactile sensation and proprioception. In contrast, the
pretreatment to posttreatment changes in the scores of the RBAT group were significant on the overall and tactile sensation. For between group comparison, the differences among the two groups were nonsignificant on the overall, temperature, tactile sensation, proprioception and stereognosis score. On the other hand, a moderate effect size in favor of the RMT group over the RBAT group was found on temperature (r=.304, p=.321).
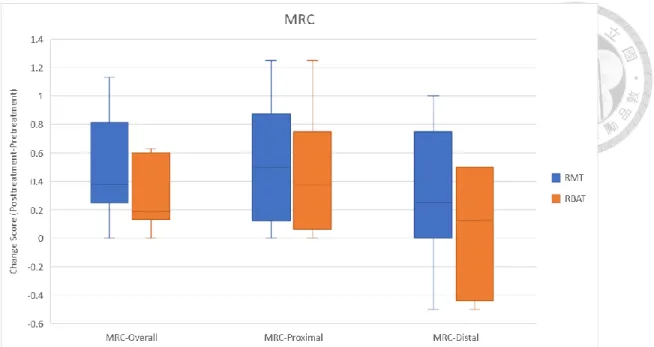
On the muscle strength assessed by MRC, the mean of the overall score increased 0.50 in the RMT group and 0.24 in the RBAT group. For within comparison, the pretreatment
to posttreatment changes in the scores of the two groups were significant on the overall and proximal MRC. For between group comparison, there were nonsignificant on the overall, proximal and distal MRC.
On the daily functional activities assessed by ABILHAND Questionnaire, the mean change scores were 23.00 in the RMT group and 13.50 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant. For between group comparison, there were nonsignificant between two groups.
In short, the motor recovery assessed by the FMA total, proximal and distal scores were improved in both groups after interventions. Both groups retained the improvement total, proximal and distal FMA scores after 3 months. The RMT group significant improved more than RBAT group in FMA total score at pretreatment and posttreatment. The sensory function assessed by rNSA score, muscle strength assessed by MRC score and daily functional activities assessed by ABILHAND Questionnaire score were improved in both over time, and the improvements were no difference among two groups.
3.3 Effects of Intervention on the Secondary Outcome Measures
The results of descriptive statistics by group on the secondary outcome measures were shown in Table 6-11, the change scores were shown in Figure 8-16.
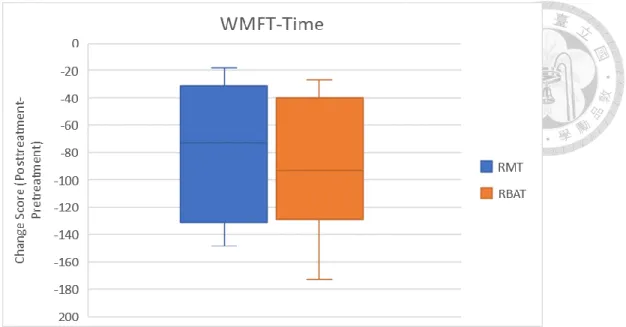
In the WMFT, the mean time score decreased 82.88 sec in the RMT group and 103.91 sec in the RBAT group. the mean change scores of the quality were 8.5 in the RMT group and 5 in the RBAT group. For within comparison, the pretreatment to
posttreatment changes in the scores of the two groups were significant. For between group comparison, there were nonsignificant between two groups.
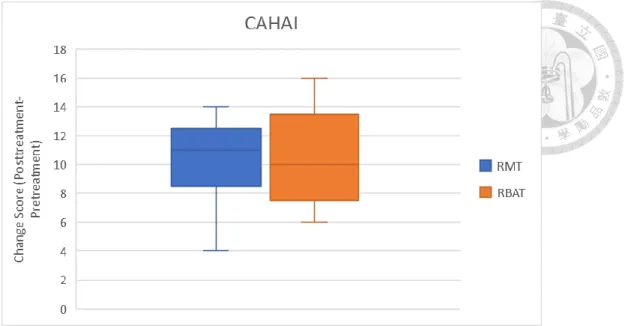
In the CAHAI, the mean change scores were 10 in the RMT group and 10 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant. For between group comparison, there were
nonsignificant between two groups.
In the MAL, the mean change scores of the amount of use MAL were 21 in the RMT group and 33 in the RBAT group. The mean change scores of the quality of movement MAL were 24.5 in the RMT group and 23.5 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were
significant.However, both two groups had nonsignificant result from posttreatment to follow-up test (both p>0.05). For between group comparison, there were nonsignificant between two groups.
In the FIM, the mean change scores were 2 in the RMT group and 1.5 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the score of the RBAT group were significant but not significant on RMT group. For between group comparison, there were nonsignificant between two groups.
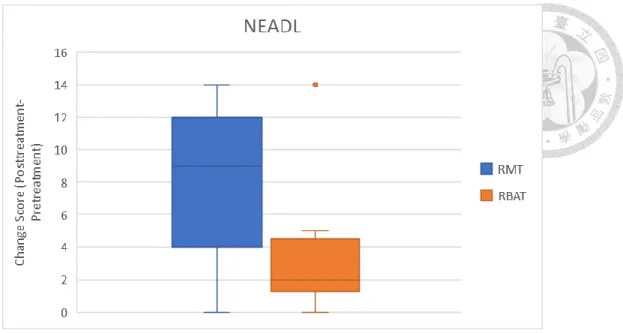
In the NEADL, the mean change scores were 1 in the RMT group and 9 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant. For between group comparison, there were
nonsignificant between two groups with a moderate effect size in favor of the RMT group over the RBAT group (r = 0.44, p = .06).
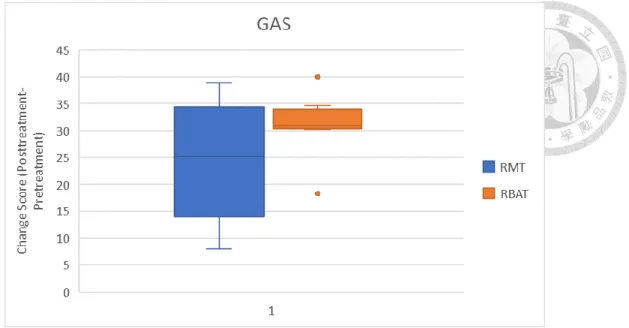
In the GAS, the mean change scores were 21 in the RMT group and 31.5 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant. For between group comparison, there were
nonsignificant between two groups with a moderate effect size in favor of the RBAT group over the RMT group (r = 0.30, p = .27).
In the SIS, the mean change scores were 9.32 in the RMT group and 11.63 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant on the overall, hand function and physical function. Moreover, the pretreatment to posttreatment changes in the scores of the RMT group were significant on the mobility, ADL and recovery. However, both two groups had nonsignificant result from posttreatment to follow-up test (both p>0.05). For between group comparison, the differences among the two groups were nonsignificant on the overall, strength, ADL, mobility, hand function, recovery and physical function score. On the other hand, a moderate effect size in favor of the RMT group over the RBAT group was found (overall r=.344, p=.149; ADL r=.426, p=.079; Mobility r=.477, p=.065;
Physical Function r=.349, p=.149).
On the activity level evaluated by actigraphy, we consider the ratio of affect and nonaffect arm activity counts. 2 data from RMT group and 2 data from RBAT group were excluded since the difference of pretreatment and posttreatment wearing time. the difference of wearing time in these 4 participants was over 200 minutes, there may be
some mistakes on implementing the protocol while they used the actigraphy. The mean change scores were 0.04 in the RMT group and 0.05 in the RBAT group. For within comparison, the pretreatment to posttreatment changes in the scores of the two groups were significant. For between group comparison, there were nonsignificant findings could be found in between groups comparison. The correlation between self-perceived arm use (the amount of use in MAL score) and the ratio of affect arm activity counts change score change score was no relevance. The Spearman correlation showed an r value of 0.120, p= 0.646.
In short, the motor recovery assessed by the FMA total, proximal and distal scores were improved in both groups after interventions. On the activity level, both group were improvement on the WMFT, MAL, FIM, NEADL, SIS, GAS and CAHAI without between group difference. The summary of the effect size of outcome measures was shown in table 17
3.4 Possible adverse effect
The results of descriptive statistics by group on MAS shown in Table 18. On the muscle tone assessed by MAS, no group showed an increase of spasticity of the upper limb after treatment; furthermore, both groups showed a significant decrease in spasticity (p<0.05).
Chapter Ⅳ. Discussion
4.1 Summary of the Study Results
Our findings were partially consistent with our hypotheses. The objectives of this study were to compare the differential efficiency among the RMT and RBAT group. All two groups have improved on sensorimotor function, daily function, self-efficacy and quality of life in patients after the interventions. No severe adverse effect was found and both groups had significantly decreased muscle tone in the upper limb. The results indicated that the different hybrid therapies may lead to different treatment effects, and that the robotic priming was applicable, safe, and promising interventions on chronic stroke rehabilitation.
The within-group results showed that both two groups led to the improvements on motor ability, muscle power, functional ability, self-perceived arm use, functional goal achievement, instrumental activities of daily living, quality of life and the ratio of affect arm activity counts. Form posttreatment to follow-up test, both two groups had no change on FMA, MAL, and SIS (both p>0.05) however there are only 9 participants finished the follow-up test, the result should be interpreted with caution. The correlation between self- perceived arm use and the ratio of affect arm activity counts change score was no
relevance, some participants did not wear enough amount of time in posttreatment test, the large difference of wearing time may affect the reliability of the evaluation. On the order hand, the daily routine of the participants in wearing days may be reason is also reason that affect the reliability of the evaluation.
For the between-group analyses, the participants receiving the RMT improved their motor ability more than those receiving the RBAT. Even though RMT group didn’t reach the statistically significant level on most of measure outcome, a positive tendency was observed in the FMA-UE proximal, rNSA-temperature, NEADL, SIS-overall, SIS-ADL, SIS-mobility and SIS-physical function compared to the RBAT group. In contrast, the RBAT group revealed a positive trend in the GAS and SIS-hand function compared to the RMT group.
4.2 The Benefits of RMT group
RMT group showed a significantly increase on the FMA-UE scale and a trend of more improvement on proximal UE. Previous study demonstrated that mirror therapy might be more associated with motor recovery in the distal part of the body (Wu et al.,2013).
Conversely, bilateral robotic training mainly led to improvement on proximal segments (Yang et al.,2012). In addition, the change scores were 5-11 point, most of the participant reached minimal clinically meaningful values. It seems that the bilateral robotic priming combined with mirror therapy would enchase the treatment effect of bilateral robotic training compared with the RBAT group. The effects might result from cortical reorganization. MT could provide “proper visual input” and, perhaps, “substitutes” for absent or reduced proprioceptive input from the affected body side. MT might also facilitate self-awareness and spatial attention by activating the superior temporal gyrus, precuneus, and the posterior cingulate cortex. Consequently, the experience during MT might help recruit the premotor cortex or balance the neural activation within the primary motor cortex toward the affected hemisphere to facilitate motor improvements.
The visual illusion of mirror could provide sensory inputs that might modulate the somatosensory cortex network and contribute to the recovery of somatosensation (Wu et al.,2013). RMT group shows tend to get more improvement than the RBAT group on rNSA- temperature sensation. This finding is also consistent with previous study that mirror therapy may get more benefits on temperature sensation (Wu et al.,2013).The benefits could relate to multi-modal neurons. Multimodal neurons in the posterior parietal and premotor cortical areas respond to sensory stimuli, such as visual input, as well as movement stimuli. The visual illusion of MT could provide sensory inputs that might modulate the somatosensory cortex network and contribute to the recovery of
somatosensation.
For quality of life, RMT group shows trend to get more improvement than the RBAT group on NEADL, SIS-overall, SIS-ADL, SIS-mobility and SIS-physical function although the previous study demonstrated that mirror therapy might not significantly get better effects on ADL (Wu et al.,2013) and bilateral robotic priming gets better
improvement on the Stroke Impact Scale strength (Hsieh et al.,2017). These slight positive trends might be the result of the reaction between bilateral robotic priming and mirror therapy which provides additional mirror visual feedback.
4.3 The Benefits of RBAT group
The RBAT group showed significantly improvements on motor ability, muscle power, functional ability, self-perceived arm use, functional goal achievement, instrumental activities of daily living and quality of life after six weeks intervention.
There was a trend in RBAT group that more improvements could be found on GAS.
This may be explained in part by the nature of functional task practice involved in this regimen. Since the participant could practice their self-preserved task directly without the mirror box, it might help them achieve their own expectation more easily.
4.4 Study Implication
To our best knowledge, this study was the first study compared the bilateral robotic priming combined with different types of bilateral arm training to chronic stroke with moderate to severe motor impairments.
The bilateral robotic priming combined with mirror therapy can be optimal intervent ion to improving the motor ability and positive trends on sensorimotor function, daily function and quality of life. Moreover, the bilateral robotic priming combined with bilateral arm training has a positive trend on the achievement of self-expectation, it can provide an individualized intervention focused on functional goals and can connect to the real-life environment.
The robotic priming was applicable, safe, and promising interventions on chronic stroke rehabilitation.
4.5 Study Limitation
There are several limitations in this study should be mentioned. Due to the small sample size, the findings should be interpreted with caution and difficult to generalize the results to all stroke patients. Also, the wearing time of accelerometers were not equal
during pretest and posttest, it affected the reliability of the objective measure the amount affected arm used in real-life situation. Furthermore, the ratio of side brain hemisphere lesion of participants was large in this study, there were 13 participants with left
hemisphere lesion but only 4 participants with right hemisphere lesion, it would make a sampling bias in this study.
Further researches should expand the sample size. The sample size calculation resulted in 56 participants pre group with an overall effect size of 0.48, a power set at 0.80, and alpha of 0.05. Also, the wearing time of accelerometers during pretest and posttest should be confirmed as equally., the number of side brain hemisphere lesion of participants should be balance. Last but not least, a control group should be set to clarifiy the treatment effect of two groups in the future.
Chapter Ⅴ. Conclusions
This study compared the differential efficiency among RMT and RBAT. The result indicated that both two intervention were promising interventions and lead to positive change on patients’ sensorimotor function, daily function, self-efficacy, quality of life, and motor function and retain to 3 months.
On the primary outcomes, the RMT group significantly gained greater benefit on motor ability than the RBAT and a positive trend on sensorimotor function. On the secondary outcomes, the RMT group showed positive trends on IADL and quality of life. On the order hand, RBAT group show a positive trend on the achievement of self-expectation.
Due to the preliminary nature of the study, the findings should be interpreted with caution. Further research may be implemented based on a well-designed randomized controlled trial with a larger sample.
References
Chang, J.-J., Tung, W.-L., Wu, W.-L., Huang, M.-H., & Su, F.-C. (2007). Effects of robot-aided bilateral force-induced isokinetic arm training combined with
conventional rehabilitation on arm motor function in patients with chronic stroke.
Archives of Physical Medicine and Rehabilitation, 88(10), 1332-1338.
Charalambous, C. P. (2014). Interrater reliability of a modified Ashworth scale of muscle spasticity. In Classic Papers in Orthopaedics (pp. 415-417): Springer.
Chuang, L.-L., Lin, K.-C., Hsu, A.-L., Wu, C.-Y., Chang, K.-C., Li, Y.-C., et al. (2015).
Reliability and validity of a vertical numerical rating scale supplemented with a faces rating scale in measuring fatigue after stroke. Health and quality of life outcomes, 13(1), 91.
Coupar, F., Pollock, A., van Wijck, F., Morris, J., & Langhorne, P. (2010). Simultaneous bilateral training for improving arm function after stroke. The Cochrane database of systematic reviews
Eftekhar, P., Mochizuki, G., Dutta, T., Richardson, D., & Brooks, D. (2016). Goal attainment scaling in individuals with upper limb spasticity post stroke.
Occupational Therapy International, 23(4),379-389.
Fugl-Meyer, A. R., Jääskö, L., Leyman, I., Olsson, S., & Steglind, S. (1975). The post- stroke hemiplegic patient. 1. a method for evaluation of physical performance.
Scandinavian Journal of Rehabilitation Medicine, 7(1), 13-31.
Gregson, J. M., Leathley, M. J., Moore, A. P., Smith, T. L., Sharma, A. K., & Watkins, C. L. (2000). Reliability of measurements of muscle tone and muscle power in stroke patients. Age and Ageing,29(3), 223-228.
Hsieh, Y.-W., Liing, R.-J., Lin, K.-C., Wu, C.-Y., Liou, T.-H., Lin, J.-C., et al. (2016).
Sequencing bilateral robot-assisted arm therapy and constraint-induced therapy improves reach to press and trunk kinematics in patients with stroke. Journal of Neuroengineering and Rehabilitation, 13, 31.
Hsieh, Y.-W., Lin, K.-C., Horng, Y.-S., Wu, C.-Y., Wu, T.-C., & Ku, F.-L. (2014).
Sequential combination of robot-assisted therapy and constraint-induced therapy in stroke rehabilitation: a randomized controlled trial. Journal of Neurology, 261(5), 1037-1045.
Hsieh, Y.-W., Wu, C.-Y., Liao, W.-W., Lin, K.-C., Wu, K.-Y., & Lee, C.-Y. (2011).
Effects of treatment intensity in upper limb robot-assisted therapy for chronic stroke: a pilot randomized controlled trial. Neurorehabilitation and Neural Repair, 25(6), 503-511.
Hsieh, Y.-W., Wu, C.-Y., Lin, K.-C., Chang, Y.-F., Chen, C.-L., & Liu, J.-S. (2009).
Responsiveness and validity of three outcome measures of motor function after stroke rehabilitation. Stroke, 40(4), 1386-1391.
Hsieh, Y.-W., Wu, C.-Y., Lin, K.-C., Yao, G., Wu, K.-Y., & Chang, Y.-J. (2012). Dose- response relationship of robot-assisted stroke motor rehabilitation: the impact of initial motor status. Stroke, 43(10), 2729-2734.
Hsieh, Y.-W., Wu, C.-Y., Wang, W.-E., Lin, K.-C., Chang, K.-C., Chen, C.-C., et al.
(2017). Bilateral robotic priming before task-oriented approach in subacute stroke rehabilitation: a pilot randomized controlled trial. Clinical Rehabilitation, 31(2), 225-233.
Hsu, H.-Y., Chiu, H.-Y., Kuan, T.-S., Tsai, C.-L., Su, F.-C., Kuo, L.-C., et al. (2019).
Robotic-assisted therapy with bilateral practice improves task and motor performance in the upper extremities of chronic stroke patients: A randomised controlled trial. Australian Occupational Therapy Journal, (2019)
Huang, Y.-H., Wu, C.-Y., Hsieh, Y.-W., & Lin, K.-C. (2010). Predictors of change in quality of life after distributed constraint-induced therapy in patients with chronic stroke. Neurorehabilitation and Neural Repair, 24(6), 559-566.
Hung, C.-S., Hsieh, Y.-W., Wu, C.-Y., Lin, Y.-T., Lin, K.-C., & Chen, C.-L. (2016). The effects of combination of robot-assisted therapy with task-specific or impairment- oriented training on motor function and quality of life in chronic stroke. PM&R, 8(8), 721-729.
Lee, M.-J., Lee, J.-H., Koo, H.-M., & Lee, S.-M. (2017). Effectiveness of bilateral arm training for improving extremity function and activities of daily living performance in hemiplegic patients. Journal of Stroke and Cerebrovascular Diseases, 26(5), 1020-1025.
Lee, Y.-Y., Lin, K.-C., Wu, C.-Y., Liao, C.-H., Lin, J.-C., & Chen, C.-L. (2015).
Combining afferent stimulation and mirror therapy for improving muscular,
sensorimotor, and daily functions after chronic stroke: a randomized, placebo- controlled study. American Journal of Physical Medicine and Rehabilitation, 94(10S), 859-868.
Lemmens, R. J., Timmermans, A. A., Janssen-Potten, Y. J., Smeets, R. J., & Seelen, H.
A. (2012). Valid and reliable instruments for arm-hand assessment at ICF activity level in persons with hemiplegia: a systematic review. BMC Neurology, 12(1), 21.
Liao, W.-W., Wu, C.-Y., Hsieh, Y.-W., Lin, K.-C., & Chang, W.-Y. (2012). Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic stroke: a randomized controlled trial. Clinical Rehabilitation, 26(2), 111-120.
Lin, K.-C., Chen, Y.-A., Chen, C.-L., Wu, C.-Y., & Chang, Y.-F. (2010). The effects of bilateral arm training on motor control and functional performance in chronic stroke: a randomized controlled study. Neurorehabilitation and Neural Repair, 24(1), 42-51. https://doi.org/10.1177/1545968309345268.
Lin, K.-C., Chen, Y.-T., Huang, P.-C., Wu, C.-Y., Huang, W.-L., Yang, H.-W., et al.
(2014). Effect of mirror therapy combined with somatosensory stimulation on motor recovery and daily function in stroke patients: a pilot study. Journal of the Formosan Medical Association, 113(7), 422-428.
Lin, K.-C., Huang, P.-C., Chen, Y.-T., Wu, C.-Y., & Huang, W.-L. (2014). Combining afferent stimulation and mirror therapy for rehabilitating motor function, motor
control, ambulation, and daily functions after stroke. Neurorehabilitation and Neural Repair, 28(2), 153-162.
Lincoln, N., Jackson, J., & Adams, S. (1998). Reliability and revision of the Nottingham Sensory Assessment for stroke patients. Physiotherapy, 84(8), 358-365.
McCombe Waller, S., & Whitall, J. (2008). Bilateral arm training: why and who benefits?
NeuroRehabilitation, 23(1), 29-41.
Penta, M., Tesio, L., Arnould, C., Zancan, A., & Thonnard, J.-L. (2001). The ABILHAND questionnaire as a measure of manual ability in chronic stroke patients: Rasch-based validation and relationship to upper limb impairment.
Stroke, 32(7), 1627-1634.
Platz, T., Pinkowski, C., van Wijck, F., Kim, I.-H., Di Bella, P., & Johnson, G. (2005).
Reliability andvalidity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: a multicentre study. Clinical Rehabilitation, 19(4), 404-411.
Skidmore, E. R., Whyte, E. M., Holm, M. B., Becker, J. T., Butters, M. A., Dew, M. A., et al. (2010). Cognitive and affective predictors of rehabilitation participation after stroke. Archives of Physical Medicine and Rehabilitation, 91(2), 203-207.
Stinear, C. M., Barber, P. A., Coxon, J. P., Fleming, M. K., & Byblow, W. D. (2008).
Priming the motorsystem enhances the effects of upper limb therapy in chronic stroke.Brain, 131(Pt 5), 1381-1390.
Stoykov, M. E., & Madhavan, S. (2015). Motor priming in neurorehabilitation.Journal of Neurologic Physical Therapy, 39(1), 33-42.
Stoykov, M. E., & Stinear, J. W. (2010).Active-passive bilateral therapy as a priming mechanism for individuals in the subacute phase of post-stroke recovery: a feasibility study. American Journal of Physical Medicine and Rehabilitation, 89(11), 873-878.
Turner-Stokes, L. (2009). Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clinical Rehabilitation, 23(4), 362-370.
Turner-Stokes, L. (2009). Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clinical Rehabilitation, 23(4), 362-370
Wu, C.-Y., Huang, P.-C., Chen, Y.-T., Lin, K.-C., & Yang, H.-W. (2013). Effects of mirror therapy on motor and sensory recovery in chronic stroke: a randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 94(6), 1023- 1030.
Wu, C.-Y., Yang, C.-L., Chen, M.-D., Lin, K.-C., & Wu, L.-L. (2013). Unilateral versus bilateral robotassisted rehabilitation on arm-trunk control and functions post stroke: a randomized controlled trial. Journal of Neuroengineering and Rehabilitation, 10(1), 35.
Wu, C.-Y., Yang, C.-L., Chuang, L.-L., Lin, K.-C., Chen, H.-C., Chen, M.-D., et al.
(2012). Effect of therapist-based versus robot-assisted bilateral arm training on
motor control, functional performance, and quality of life after chronic stroke: a clinical trial. Physical Therapy, 92(8), 1006-1016.
Figure 1. Flow Chart of the Study Procedure
Figure 2A. Figure 2B.
Figure 2C. Figure 2D.
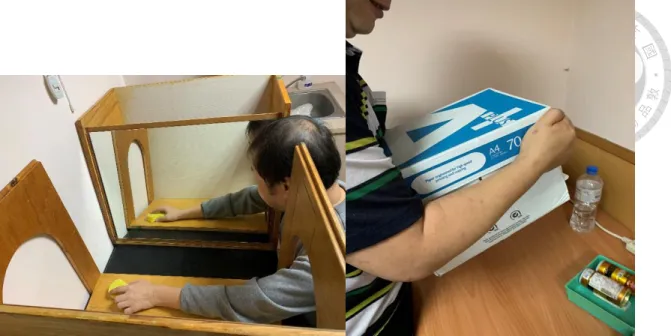
Figure 2A-D. Experimental Materials and Setting (2A) Bi-Manu-Track – Reha-Stim;
(2B) Mirror Box; (2C) Bi-Manu-Track in forearm pronation/supination mode; (2D) Bi- Manu-Track in elbow flexion/extension mode
Figure 2E. Figure 2F.
Figure 2G
Figure 2E-G. (2E) Functional task in mirror therapy; (2F) Functional task in Bilateral arm training; (2G) Transfer Package checklist
Figure 3. Treatment Procedures for two groups
Figure 4. Box-and-whisker plot showing the score changes of FMA-UE in the two study groups.
Figure 5. Box-and-whisker plot showing the score changes of rNSA in the two study groups.
Figure 6. Box-and-whisker plot showing the score changes of MRC in the two study groups.
Figure 7. Box-and-whisker plot showing the score changes of ABILHAND in the two study groups.
Figure 8. Box-and-whisker plot showing the score changes of WMFT-Time in the two study groups.
Figure 9. Box-and-whisker plot showing the score changes of WMFT-Quality in the two study groups.
Figure 10. Box-and-whisker plot showing the score changes of CAHAI in the two study groups.
Figure 11. Box-and-whisker plot showing the score changes of MAL in the two study groups.
Figure 12. Box-and-whisker plot showing the score changes of NEADL in the two study groups.
Figure 13. Box-and-whisker plot showing the score changes of FIM in the two study groups.
Figure 14. Box-and-whisker plot showing the score changes of GAS and FIM in the two study groups.
Figure 15. Box-and-whisker plot showing the score changes of SIS in the two study groups.
Figure 16. Box-and-whisker plot showing the score changes of the ratio of affect arm activity counts in the two study groups.
Table 1. Descriptive and Inferential Statistics of clinical characteristics
Variable RMT (n = 9) RBAT (n = 8) p
Sex .788
Male 5 5
Female 4 3
Age, years Mean (SD) 57.31 (6.11) 57.91 (11.30) .471
Time since stroke, months, Mean (SD)
19.22 (11.67) 25.75 (23.49) .891
Side of stroke .901
Left 2 2
Right 7 6
Type of stroke .832
Hemorrhagic 5 4
Ischemic 4 4
Handedness <.99
Left 0 0
Right 9 8
MMSE score, Mean (SD) 25.53 (2.10) 25.43 (2.30) .83
NIHSS score, Mean (SD) 4.20 (2.47) 4.00 (2.01) .92
PT time, hours/week Mean (SD)
2.55 (1.01) 1.79 (1.53) .249
Table 2. Descriptive and Inferential Statistics of FMA-UE by group
FMA–UE RMT, Median
(Q1–Q3) n=9
p RBAT, Median
(Q1–Q3) n=8
p Mann-Whitney U p
Effect size r
Overall
Pretreatment 30.00(26.50-38.00) .008* 31.67(30.25-35.25) .011* .044^ .487 Posttreatment 42.00(33.50-47.00) 36.50(34.50-41.25)
Proximal
Pretreatment 26.00(23.00-28.50) .007* 27.00(24.25-31.50) .011* .198 .311 Posttreatment 31.00(28.00-33.00) 30.50(27.25-34.50)
Distal
Pretreatment 6.00(3.00-10.50) .011* 6.00(2.00-7.00) .011* .222 .295 Posttreatment 11.00(6.00-16.00) 7.50(4.25-9.00)
Within-group comparison: *p<0.05, when compared with pretreatment
Between-group comparison: ^p<0.05, when RMT group greater than RBAT group
Table 3. Descriptive and Inferential Statistics of FMA-UE from posttreatment to follow-up by group
FMA–UE RMT, Median (Q1–
Q3) n=5
p RBAT, Median (Q1–Q3)
n=4
p
Overall
Posttreatment 40.00 (33.75-50.00) .109 36.00(32.50-49.50) .197 Follow up 38.00 (31.25-48.50) 34.00(27.50-47.50)
Proximal
Posttreatment 32.00 (29.50-33.75) .197 28.00(25.50-37.00) .99 Follow up 30.00 (27.50-33.50) 30.00(25.50-36.50) Distal
Posttreatment 9.00 (3.25-16.25) .414 8.00(6.00-13.50) .273 Follow up 6.50(3.00-16.00) 7.50(3.50-11.00)
Within-group comparison: *p<0.05, when compared with pretreatment
Between-group comparison: ^p<0.05, when RMT group greater than RBAT group