國立臺灣大學公共衛生學院 公共衛生碩士學位學程
碩士論文-實務實習成果報告
Master of Public Health Degree Program College of Public Health
National Taiwan University Master Thesis - Practicum Report
以 Dolutegravir 為本的抗反轉錄病毒處方相較於其他處方之 療效及耐受性:統合分析
Efficacy and Tolerability of Dolutegravir (DTG) Based Antiretroviral Therapy Compared to Other Combination
Antiretroviral Therapy for HIV-Positive Patients:
A Meta-Analysis
范志杰 Fan Chi Kit
校內指導老師:方啟泰 教授 Advisor:Chi-Tai Fang 單位指導老師:林淑文 副主任
Preceptor:Shu-Wen Lin 中華民國 108 年 7 月
July 2019
中文摘要
研究目的
自2018 年,世界衛生組織(World Health Organization, WHO)建議使用 Dolutegravir
(DTG)配合兩種核苷酸反轉錄酶抑制劑(nucleoside reverse transcriptase inhibitors, NRTIs)為抗反轉錄病毒療法(antiretroviral therapy, ART),作為成人和青少年治療 初期感染人類免疫缺乏病毒(human immunodeficiency virus, HIV)的首選用藥,指
引基於WHO 其自行發起的系統性文獻回顧及網絡統合分析研究,發現 DTG 為本
的處方(DTG-based)相較於其他 ART 處方,特別是以往被建議一線使用的 Efavirenz
為本的處方(EFV-based),能表現更有效的病毒抑制成功率、CD4 細胞數恢復率及
較低的用藥中止治療風險。但即便如此,分析使用了有限數量直接比較(head-to- head)的隨機對照試驗(randomized control trials, RCTs),而目前已有更多已完成
且設計良好的RCTs 發表,所以我們希望可以整理出更有系統且最完整的證據,回
答DTG-based 處方其療效和耐受性兩大面向,進行一個更全面的統合分析。
方法
自Pudmed,Embase,Cochrane database,AIDSinfo 和 Clinicaltrial.gov 等資料庫進
行文獻搜尋,搜尋結果到2019 年 5 月,納入相關的 RCTs 做為分析,篩選符合的
文獻會進行偏差風險(Risk of bias)評估。療效結果以 FDA 演算法(snapshot algorithm)為定義;耐受性結果以任何藥物產生的副作用(Adverse events, AEs)所 導致研究過程中停止用藥為定義,結果都以風險比(risk ratio, RRs)作基準。當中 也使用次群組分析(subgroup analysis)和敏感度分析(sensitivity analysis),獨立
分析不同病理狀況的HIV 感染者,比較 DTG 與其他 ART 之間的特徵差異。
結果
共納入了19 篇 RCTs,總包括 8936 名 HIV 感染者,當中分成三種 HIV 感染者狀
態:(1)已達到病毒學抑制(virally suppressed)、(2)從未接受過任何 ART 治療
(treatment-naive)和(3)接受過 ART 治療但治療失敗(treatment-experienced)。
6 篇 RCTs 評估了已達到病毒學抑制的 HIV 感染者; 在比較 DTG-based 和其他 ART 治療之間,病毒抑制(RR 0.95, 95 % CI 0.42-2.16)和因副作用產生而停藥發生率
(RR 2.65, 95%CI 0.59-11.93)都無統計上顯著的差異,但估計的效果顯示該群組
的感染者在轉換成DTG 為本的處方後,因副作用產生而停藥發生率的比例有明顯 較高的風險。11 篇 RCTs 評估了從未接受過任何 ART 治療的 HIV 感染者; 在使用 DTG-based 的情況下,比較使用 EFV-based 和蛋白酶抑製劑為本(protease inhibitor, PI-based)的次群組分析,顯示出病毒抑制和停藥發生率都有正向的效果。2 篇 RCTs
評估了接受過ART 首選治療但失敗的感染者,結果顯示以 DTG-based 的治療,其
病毒抑制(RR 1.16, 95%CI 1.08-1.24)和因副作用產生而停藥發生率(RR 0.56, 95
%CI 0.31-1.00)風險都較其他 ART 處方,呈現正向的效果。
結論
我們統合分析結果建議以DTG 為本的抗反轉錄病毒處方可作為 HIV 感染者,治療
人類免疫缺乏病毒一線首選和首選用藥失敗後二線替代時的用藥選擇。但考慮使
用於已達到病毒學抑制的HIV 感染者並選擇轉換使用 DTG 處方時,應採取謹慎且
長期追蹤的措施。
關鍵字
人類免疫缺乏病毒、抗反轉錄病毒藥物、整合酶抑制劑、療效、耐受性
Abstract
Background
Since 2018, World Health Organization (WHO) recommended Dolutegravir (DTG) plus
two nucleoside reverse-transcriptase inhibitors (NRTIs) antiretroviral therapy (ART) as
the preferred first-line regimen for treatment-naive HIV-positive adults and adolescents
as because which showed DTG-based regimen was more effective with higher viral
suppression rate, better CD4 cell count recovery and lower risk of treatment
discontinuation compared with another widely used first-line regimen, Efavirenz (EFV)-
based ART, after WHO self-initiated systematic review and network meta-analysis. Since
the synthesized results of previous meta-analysis with a limited number of head-to-head
randomized control trials (RCTs), and to date there were several newly published and
robust RCTs available, we aimed to conducted a comprehensive meta-analysis of efficacy
and tolerability outcome of DTG-based regimens.
Methods
Pudmed, Embase, Cochrane databases, AIDSinfo and Clinicaltrial.gov were searched up
to May 2019 for RCTs on DTG-based regimen in HIV-positive patients. Efficacy was
analysed by FDA snapshot algorithm, and tolerability was defined as any adverse events
leading to study drug discontinuation. Each various characteristics of HIV participants
were considered in subgroup and sensitivity analysis. Risk of bias and certainty of
evidences were also assessed.
Results
Nineteen eligible RCTs comprising 8936 patients were included, which were divided into
three scenarios: virally suppressed, treatment-naive and treatment-experienced. Among 6
trials assessing virally suppressed populations, no significant difference was shown in
terms of viral suppression (RR 0.95, 95 % CI 0.42 to 2.16) and discontinuation rate (RR
2.65, 95 % CI 0.59 to 11.93) between DTG-based and others ART regimens, but the
estimated effect showed higher proportions of discontinuation rate of study drug related
to adverse events after switch to DTG-based regimen. Among 11 trials assessing
treatment-naive populations, beneficial effects of viral suppression and discontinuation
rate were showed for DTG-based regimen compared with EFV-based and protease
inhibitor (PI-) based regimens after a subgroup analysis. Only 2 trials assessed treatment-
experienced populations, which showed a significant difference of better viral
suppression (RR 1.16, 95 % CI 1.08 to 1.24), and lower discontinuation rates (RR 0.56,
95 % CI 0.31 to 1.00) for DTG-based regimen.
Conclusion
Our meta-analysis showed that DTG-based regimen was a preferred ART regimen for
first-line and second-line regimen among HIV-positive patients, but for virally suppressed
patients, cautions should be taken and long-term follow-up is needed.
Key words
human immunodeficiency virus (HIV), antiretroviral therapy (ART), dolutegravir (DTG),
efficacy, tolerability
Tables of Contents
口試委員會審定書 ... ii
摘要 ... iii
Abstract ... v
Tables of Contents ... viii
List of Tables ... ix
List of Figures ... x
實習單位簡介 ... xi
Chapter 1: Introduction ... 1
Chapter 2: Methods ... 3
2.1 Inclusion and exclusion criteria ... 3
2.2 Search strategy and selection criteria ... 4
2.3 Data extraction ... 4
2.4 Assessment of quality of included studies ... 5
2.5 Data synthesis and statistical analysis ... 5
2.6 Sensitivity analysis ... 6
2.7 Assessment of certainty of evidence ... 6
Chapter 3: Result ... 8
3.1 Efficacy ... 9
3.2 Tolerability ... 12
3.3 Quality assessment... 14
Chapter 4: Discussion ... 16
Reference ... 21
List of Tables
Table 1 PubMed and Embase search strategy... 25
Table 2 Characteristics of patients included in the selected randomized control trial studies ... 26
Table 3 Summary of findings: certainty of evidence for HIV virally suppressed patients ... 28 Table 4 Summary of findings: certainty of evidence for HIV treatment-naive patients:
DTG-based versus Efavirenz-based ... 29
Table 5 Summary of findings: certainty of evidence for HIV treatment-naive patients:
DTG-based versus Protease inhibitors-based ... 30
Table 6 Summary of findings: certainty of evidence for HIV treatment-naive patients:
DTG-based versus others generations of InSTI-based ... 31
Table 7 Summary of findings: certainty of evidence for HIV treatment-experienced patients ... 32
List of Figures
Figure 1 Flow chart of articles identified, screened, assessed and included ... 33
Figure 2a Assessment of the risk of bias by Cochrane Collaboration tool: risk of bias summary ... 34
Figure 2b Assessment of the risk of bias by Cochrane Collaboration tool: risk of bias graph ... 35
Figure 3a Virally suppressed patients reached virological non-response ... 36
Figure 3b Virally suppressed patients reached virological non-response, stratified by follow-up duration endpoint ... 37
Figure 4a Treatment-naive patients achieved viral suppression ... 38
Figure 4b Treatment-naive patients achieved viral suppression with sensitivity analysis, excluding DoIPHIN-1 and INSPIRING ... 39
Figure 5 Treatment-naive patients with subgroup analysis of viral suppression among regimens of different mechanisms of action ... 40
Figure 6 Treatment-experienced patients who failed the first-line regimens, and
achieved viral suppression ... 41
Figure 7 Tolerability, defined as any adverse events leading to discontinuation of study drug in three sub-population patients ... 42
Figure 8 Treatment-naive patients with subgroup analysis of tolerability among
regimens of different mechanisms of action.. ... 43
實習單位簡介
一、實習單位
臺大醫院藥劑部、綜合病房及感染科門診
二、單位介紹
1. 臺大醫院藥劑部
住院調劑組:提供基本之藥品調劑服務,藥師每日會依據病人肝、腎功能或病 況變化,提供個別化的臨床藥事服務,藥品劑量調整、藥品選擇、藥品療效監測、
藥品不良反應評估與通報、用藥諮詢、病人衛教及藥事相關教育訓練。另有臨床藥 師參與部分病房的病房迴診。
臨床藥事組:目前在加護病房、腎臟科及血液腫瘤科等有專職的臨床藥師提供 臨床藥事服務。臨床藥師參與予病房的迴診及給予用藥上的建議以確保藥物治療 的適當性及安全性。臨床藥師也負責臨床藥學研究所碩士班學生及六年制藥學生 的進階臨床藥學實習,同時也負責訓練新進藥師們。除此之外,臨床藥師也參與病 歷審查工作小組、加護病房管理委員會及感染控管制委員會運作,以改善這兩個領 域的院內相關藥物使用及流程。
2. 綜合病房及感染科門診(加會實習部門)
感染科在臨床方面服務層面涵蓋住院病患診療,門診病患診療(一般內科門診 及感染症門診),以及全院有關感染症之照會,並負責院內感染管制之各項事宜以 及隔離病房之統籌運用。同時持續追蹤本院臨床分離菌株之抗生素感受性,提供作 為臨床選擇抗生素時的參考。
三、組織發展與目標
臺大藥劑科在服務、教學與研究均有長足的發展。未來仍將持續優化藥事作業 環境,強化資訊科技運用,深耕臨床教學與藥學教育,提供六年制 Pharm. D 及 PGY 藥師最佳的訓練環境,永續藥學人才培育,並持續擴展臨床專責藥師服務的範疇,
專注以病人為中心的服務,以成為醫療團隊重要且信賴的夥伴。另將持續推動全院 藥品管理制度的變革,使藥品安全提升至更高標準,並與國際同步。藥劑部持續努 力,落實培養卓越藥學人才、進行創新藥事及臨床研究、提供高品質的藥事服務並 為臺大全院用藥安全做最好的把關。
四、實習單位提供的資源與限制
這次在實習單位中可以運用臺大院內系統提供的電子資源與資料庫。研究可 能遇到的障礙預期有某些文獻本身資料型態上的差異,像是某些隨機對照試驗
(RCT)分組試驗人數較少、學術海報記錄中並沒有完整提供試驗的執行方法,當 中所帶來的不完整結果數據(incomplete outcome data)、選擇性結果報告(selective outcome reporting)和各篇文獻都會存在的一些潛在偏差,以上都是較為繁瑣需要 單獨獨立分析處理的部分。預期在本校及本院的單位老師指導下,在研究方面可以 學習如何系統性的搜尋文獻、評讀文獻品質和進階統計觀念等。
Chapter 1: Introduction
Background
Before 2016, dolutegravir (DTG)-based regimen was recommended as an alternative
regimen because of limited information on efficacy and safety, according to the WHO’s
guidelines on the use of antiretroviral (ARV) drugs for treating and preventing HIV
infection.1 A large network meta-analysis2 pooled 71 direct and indirect trials, which
included four head-to-head randomized control trials (RCTs) related to DTG, overall
effect compared with Efavirenz (EFV)-based antiretroviral therapy (ART) in treatment-
naive adults and adolescents, reaching the primary outcome with viral suppression at 48
weeks was significantly beneficial (OR 1.87, 95 % CI 1.34 to 2.64). Since that time,
evidence and experience have accumulated on the use of DTG in both first- and second-
line ART, WHO published a latest consolidated 2018 interim guidelines and policy brief,3,
4 both cited self-initiated systematic review and network meta-analysis,5 among eight
head-to-head RCTs which explored DTG were included, identically supported the
preceding review findings; DTG plus two nucleoside reverse-transcriptase inhibitors
(NRTIs) was more effective with viral suppression compared with EFV-based ART in
treatment-naive adults and adolescents (OR 1.86, 95 % CI 1.44 to 2.40), and overall
supported by moderate certainty evidence. Other than first-line regimens, WHO guideline
also recommended DTG-based as a preferred second-line regimen for HIV-positive
people who have failed non-DTG-based regimen, basically with non-nucleoside reverse-
transcriptase inhibitors (NNRTIs) or protease inhibitor (PI)-based first-line regimen, also
comprised a conditional recommendation with different certainty evidence correspond to
various HIV sub-populations.
For safety, DTG also performed a well protective effect than EFV, with fewer drug-
drug interactions, higher genetic barrier to ART resistance, also with respect to financial
feasibility; the availability of a generic fixed-dose combinations (FDC) in low- and
middle-income countries (LMICs).6 Despite DTG-based programme rapidly
implementing or planning as a first-line regimen in national HIV guidelines and some
countries was stopping the FDC procurement of EFV-based treatment, approximately 98
LMICs counted in the July of 2018,7 DTG-based regimen is still an importance issues on
how likely to perform within HIV-positive patients.
Between 2017 to 2019, total of 11 key clinical trials have been being published online,
most of those were investigating the efficacy and safety of DTG-based regimen used,
comparator was included the standard triple-regimen or novel dual-regimen. To further
enhance the evidences on DTG-based profile, we performed a meta-analysis by pooled
samples from RCTs and aggregated an enlarged sample size, in order to obtain a better
evaluation of the efficacy and tolerability of DTG-based regimen, and to analysis the
effect on specific sub-population of HIV-positive patients, comprised of new scenario
setting which did not discuss in pervious meta-analysis; virally suppressed patients who
switched to DTG-based regimen from other regimen and treatment-experienced patients
who failed using first-line regimens.
Chapter 2: Methods
2.1 Inclusion and exclusion criteria
Eligibility criteria were based on study design, characteristic of participants, components of ART’s base and backbone and outcome measures. The study were eligible to include if meeting the criteria as follows: (i)study design was randomized control trial; (ii) HIV positive participants; and (iii) participants were assigned to either DTG-based or other combination ART. Studies have at least one of record on efficacy or tolerability would be included. Efficacy were defined as virological non-response rate with virally suppressed patients or viral suppression to non-detectable ratios with treatment-naive patients (HIV RNA< 50 copies/ml, US Food and Drug Administration FDA snapshot algorithm) in the end of follow-up period, and tolerability were defined as any adverse events leading to study drug discontinuation during the clinical trial. Some studies reported more than two groups of ART intervention, the group only conform to the inclusion criteria will selected.
We also excluded studies which involved DTG monotherapy which is not recommended
regimen in guidelines, studies on experimental drugs, pharmacokinetic, reviews, and
technical papers. When the related studies by the same authors were found, only included
the study with the biggest sample size and the most standard follow-up period. Study will be considered in any language.
2.2 Search strategy and selection criteria
This meta-analysis was drafted in accordance with the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) guidance.8 We searched the PubMed,
Embase, Cochrane databases for three sets of terms (Table 1) from their establishments
to May 2019: (i) ‘Dolutegravir’ or relative terms such as ‘Anti-Retroviral Therapy’ or
‘Integrase Strand Transfer Inhibitor’; (ii) ‘efficacy’ or ‘tolerability’ between DTG-based
regimen and others combination ART; (iii) ‘randomized controlled’ study design. The
same searching terms were used in abstracts from International AIDS Society Conference
on HIV Science, European AIDS Conference, Conference on Retroviruses and
Opportunistic Infections and ClinicalTrial.gov for unpublished clinical trials.
2.3 Data extraction
Data of study were independently assessed and extracted from included studies on the
following items: author, publication year, study design, study population including
sample size, characteristics of HIV participants (divided into three scenarios: virally
suppressed, treatment-naive and treatment-experienced), pre-trial antiretroviral treatment,
intervention including the ART used, dosage of treatment, following-up time and
outcome parameters data. Efficacy outcome were frequently reported at multiple
timepoints, but we standardize the time frame in each included study if possible, typically
defined as 48 weeks. For tolerability outcome, studies were included in the meta-analysis
if the number of study drug discontinuation due to any adverse events were reported.
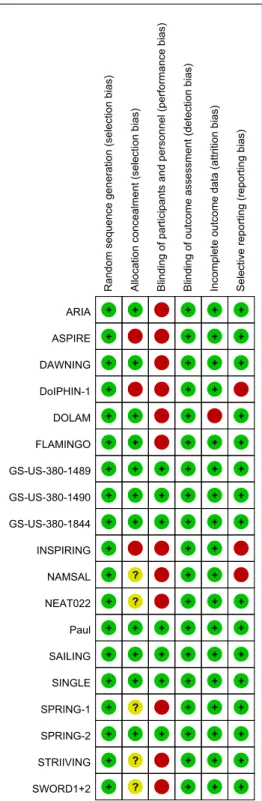
2.4 Assessment of quality of included studies
We also used Cochrane Collaboration tool9 to assess the possible risk of bias in the results
of each of the eligible studies. Risk of biases will considered into five domains; selection
bias, performance bias, detection bias, attrition bias and reporting bias. Each domain will
be made a judgment by the tool, rated as ‘high risk’, ‘low risk’ or ‘unclear’.
2.5 Data synthesis and statistical analysis
We used risk ratios (RRs) for binary outcomes, as the effect measures. Studies results
were pooled by random-effects models, because of certainly different characteristics
baseline of HIV participants. Statistical and degree of heterogeneity was assessed by I2
measure.10 To explore the effect of different groups of ARV drugs on virological
performance, we utilized a subgroup analysis with stratification based on various ARV
drug’s mechanisms of action within the intervention; versus Efavirenz, classified as
NNRTI, versus group of protease inhibitor (PIs) and versus Integrase Strand Transfer
Inhibitor (InSTI) which DTG classified to but different generations, respectively.
Publication bias was assessed by funnel plot and visual assessments if needed. The meta-
analysis was performed using by Review Manager Software version 5.3 (Cochrane
Library Software, Oxford, UK).
2.6 Sensitivity analysis
The results may be influenced by the variable baseline characteristics within the trials,
that is always the statistical heterogeneity of real treatment effects among trials while
conducting meta-analysis. We compared the outcome with using sensitivity analysis,
performed by repeating the pooled analysis by systematically excluded some individual
study, instead of substituting alternative decisions that were arbitrary.
2.7 Assessment of certainty of evidence
We used the well-validated Grading of Recommendation Assessment, Development and
Evaluation (GRADE) approach to rating the certainty of evidence for each outcome
across the literature.11 Data from RCTs without any important limitations are initially
considered high quality evidence but can be downgraded depends on five factors: 1)
Limitations in study design or execution (risk of bias); 2) Inconsistency of results; 3)
Indirectness of evidence; 4) Imprecision; and 5) High probability of publication bias.
Meanwhile, there are factors that can upgrade the quality of the evidence despite
downgrade decision be made. After the evaluation of these criteria, the quality of the body
evidence will determine into four levels: high, moderate, low or very low. We employed
GRADEpro Guideline Development Tool (GDT) to create summary tables of the findings
for each outcome and justified all decisions to downgrade or upgrade the quality of
evidence using footnotes and comments.
Chapter 3: Result
Our search criteria identified 2624 publications and clinical trials, of which 391 were
excluded as duplicated (Figure 1). The remaining 2233 full texts were assessed according
to eligibility criteria, of which 1984 were excluded by irrelevant on the basis of the title
and abstract. After assessing the full text of the remaining 249 studies, the reasons as we
excluded were: monotherapy, study without comparable intervention group or did not
mention the outcomes that we focused. Eleven trials were newly published studies,
compared to the pervious meta-analysis conducted by WHO, giving a total of nineteen
studies12-30 met all the inclusion criteria and were included in the meta-analysis.
Table 2 presents descriptive data for this nineteen qualifying trials, mostly were large-
scale clinical trials, conducted over the past two years and total comprising 8936 patients;
2704 for virally suppressed group; among three studies12-14 compared DTG-based triple
regimen with others triple ART regimen and three studies15-17 compared DTG-based dual
regimen with continuation of current ART regimen (cART), among SWORD-1 and
SWORD-2 trials;17 those extended 148 weeks on efficacy and safety data, proved to FDA
as evidences to approved the first and only DTG plus Rilpivirine (RPV) dual-therapy
single-table simplification medication. 4893 for treatment-naive group; all eleven
studies18-28 compared a strategy based on DTG-based triple therapy to others triple ART,
within one study populations specified for LMICs setting in Cameroon,28 one for HIV
treatment-naive women,24 one for pregnant HIV women26 and one for HIV-associated TB
coinfected patients,27 1339 for treatment-experienced group; two studies29, 30 each with
DTG plus investigator-selected optimized backbone regimen (OBR) compared with
raltegravir (RAL) plus OBR and lopinavir/ritonavir (LPV/r) plus OBR, separately.
Treatment-experienced patients who enrolled in trials taking previous background ART
regimens mainly included PI-based (85%) and EFV (78%) in SAILING29 and
DAWNING30 respectively. The setting target population was stricter with SAILING,
which eligible patients must had resistance to two or more classes of ARV drugs. The
DAWNING were designed by low-resource settings, and the protocol of study was
amended to permit patients who originally started LPV/r group, but transition to DTG-
based regimen if considered appropriate by the investigator, because superiority in
virological suppression of DTG-based was demonstrated before the study endpoints; 12
patients switched to dolutegravir during the study and will be counted with intention-to-
treat (ITT) population. Total of seven studies were double-blinded randomized clinical
trial,14,19,20,22,23,25,29 and the rest of twelve studies were open-label randomized clinical
trial.
3.1 Efficacy
At the endpoint, basically at week 48, six studies published in 2017 to 2018, involved
2704 virally suppressed patients reported the 12 patients on DTG-based regimen (0.89%)
versus 12 patients on others ART (0.88 %) had reached virological non-response at the
study endpoint. There was no significant difference shown in the ITT population pooled
proportion of virological non-response between DTG-based and others ART (RR 0.95,
95 % CI 0.42 to 2.16; Figure 3a). For robustness of synthesis data, subgroup analysis was
performed and demonstrated that the viral suppression ratio between DTG and others
ART was not affected by follow-up duration whether 24 weeks or 48 weeks, proved by
consistent effect size (RR 0.98, 95 % CI 0.26 to 3.78; RR 1.01, 95 % CI 0.31 to 3.29,
respectively) and well homogeneity (I2=0% and I2=15%; Figure 3b).
The eleven studies included in a total of 4893 HIV treatment-naive patients, with 2119
patients on DTG triple therapies (86.6%) versus 2001 patients on other standard triple
ART therapies (81.8%) had achieved viral suppression to non-detectable viral load (HIV
RNA< 50 copies/ml), control group mostly combined with efavirenz (EFV) plus dual
NRTI, followed by InSTI group: bictegravir (BIC) or raltegravir (RAL) plus dual NRTI.
Among one study28 used low dose 400mg EFV plus dual NRTI as comparator. Based on
the setting criteria for meta-analysis, there was a difference with a consistent beneficial
direction toward DTG-based regimen, contrary to the study by Paul25 and INSPIRING27;
overall with a significant better virological suppression outcome within the intention-to-
treat (ITT) population (RR 1.05, 95 % CI 1.01 to 1.09; Figure 4a). As two studies
compared to others nine studies, DoIPHIN-126 and INSPIRING; both were presented
wide confident intervals, (95% CI 1.07 to 2.95 and 95% CI 0.76 to 1.12, respectively),
we concerned the heterogeneity issue (I2 = 55%) by indirectness among studies, because
one was enrolled HIV populations who specify with pregnant HIV women and one with
HIV-associated TB coinfected patients. Hence, we performed a sensitivity analysis with
retained the rest of nine studies, which consistently resulted in better virological
suppression among HIV patients while taking DTG-based regimen (RR 1.05, 95 % CI
1.02 to 1.09; Figure 4b). However, the heterogeneity still existed but slightly decreased
(I2 changed from 55% to 49%), eliminating the different sub-population of HIV patients
which did not appear explain the heterogeneity rationally.
In the ARV mechanism of action subgroup analysis (Figure 5), DTG plus two NRTIS
versus EFV-based, PI-based and others InSTI-based triple therapy with various naive
patients, all were showed beneficial effects on virological suppression, excepted HIV-TB
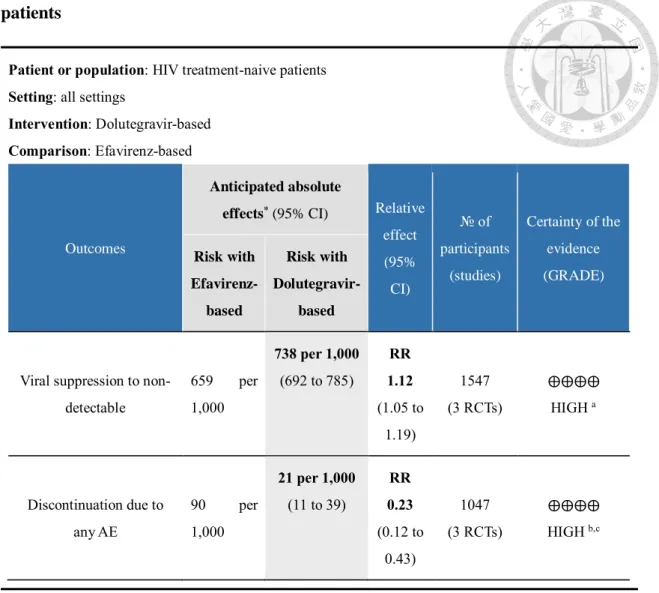
coinfected patients (Figure 5-3). Beside the benefits of DTG versus EFV-based and versus
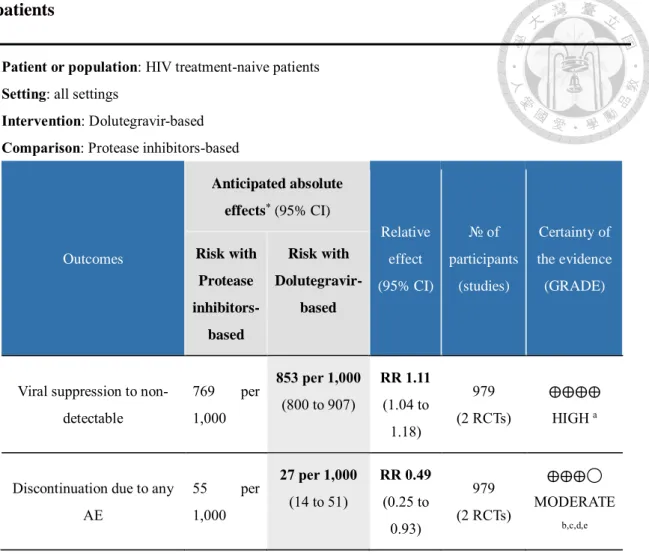
PI-based were shown significance, (RR 1.12, 95 % CI 1.05 to 1.19 with I2 = 0%; RR 1.11,
95 % CI 1.04 to 1.18 with I2 = 11%, respectively, Figure 5-1, 5-4). The beneficial effect
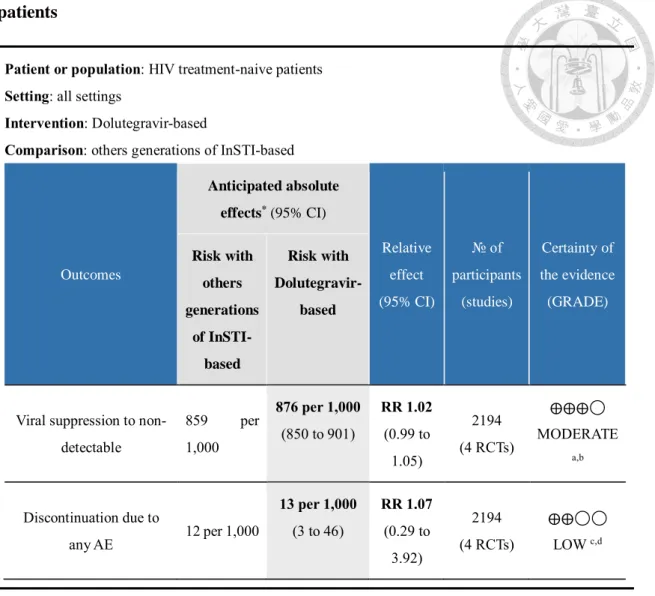
of virological outcome was small and no significant differences was seen when versus
others InSTI-based regimen (Figure 5-5). Furthermore, the test for subgroup differences
(p = 0.004) meaning that ARV mechanism of action statistically and significantly
modifies the outcome of virological effect.
Among the treatment-experienced patients, there were large and higher response rate
for the DTG-based regimen was primarily driven by two well design RCTs, SAILING
and DAWNING29-30, total including 512 patients on DTG-based regimen (76.9%) and
449 patients on others ART (66.7%) who previously had virological failure (defined as
plasma HIV-1 RNA assessments of 400 copies per mL or higher), and achieved viral
suppression to non-detectable viral load at weeks 48. The risk ratio in the pooled
proportions of virological suppression between two groups was 1.16 (95 % CI 1.08 to
1.24), showed a significant difference and favours DTG-based regimen (Figure 6).
3.2 Tolerability
Fifteen studies involving 8111 patients reported tolerability outcome, defined as any
adverse events leading to discontinuation of study drug. Among four studies indicated
virally suppressed patients,12-14,17 nine studies indicated treatment-naive patients18-25,27
and two studies indicated treatment-experienced patients29-30 (Figure 7).
Overall 49 virally suppressed patients discontinued ART; 37 (2.9%) on DTG-based
regimen versus 12 (0.9%) on others ART (RR 2.65, 95 % CI 0.59 to 11.93; Figure 7-1).
DTG-based was not statistically differentiable from others ART, but the estimated risk
ratio showed higher proportions of discontinuation of DTG-based group related to
adverse events, only GS-US-380-184414 study favours DTG-based regimen which
performed better tolerability, although two groups of event risk also did not reach
statistically significant level. Considered the estimated effect of events reported by
STRIIVING study13 was deviant from the other three studies (no event occurred on others
ART regimen group), and also the 95% confident interval was substantially wider than
expectation, so sensitivity analysis was conducted with removing this study. The pooled
result showed consistently no significant difference between two groups with
heterogeneity had somewhat increased from 71% to 74%, suggesting this was not the
notable factor causing variation within this sub-population studies. The majority of
adverse event leading to discontinuations for virally suppressed patients in the DTG-
based regimen were psychiatric disorders (mood and/or sleeping issues), gastrointestinal
disorders, nervous system disorders (headache) and subcutaneous disorders (pruritus).
Nine studies involving 126 treatment-naive patients reported discontinuation of study
drug related to adverse events, 38 (1.8%) on DTG-based regimen versus 88 (4.2%) on
others ART regimen (RR 0.47, 95 % CI 0.24 to 0.92; Figure 7-2). The majority of those
confidence intervals included 1.0, seven studies found that discontinuation event were
less frequent in the DTG-based regimen than others ART regimen, but two other
studies19,22 with a opposite result in favour of others ART regimen. A clear-cut distinction
between estimates on the forest plot stand out again the heterogeneity between studies (I2
= 49%), hence same methodology we had done; subgroup analysis with stratification
based on various ARV drug’s mechanisms of action within the intervention. In the ARV
mechanism of action subgroup analysis (Figure 8), DTG plus two NRTIS versus EFV-
based and PI-based triple regimen with treatment-naive patients, were showed significant
beneficial effects on tolerability. The benefits from DTG-based versus EFV-based,
SINGLE study20 contributed an enormous weight and reached statistical significance,
pooled result with showing a risk ratio reduction in discontinuation of 77% (RR 0.23, 95
% CI 0.12 to 0.43, I2 = 0%). DTG-based compared to PI-based were also found
significance and well homogeneous results with a 51% reduction in risk of intolerability
(RR 0.49, 95 % CI 0.25 to 0.93, I2 = 0%). The beneficial effect of tolerability outcome
was not seen when DTG-based versus others InSTI-based regimen. The difference in
discontinuations was also mainly driven by psychiatric, gastrointestinal, nervous system
and subcutaneous disorders in treatment-naive patients receiving DTG-based regimen.
There were 17 treatment-experienced patients on DTG-based regimen (2.6%) and 31
treatment-experienced patients on Others ART regimen (4.6%) who discontinued ART
after the prior ART regimen failed, less frequent for DTG-based regimen were found with
a borderline statistical significance (RR 0.56, 95 % CI 0.31 to 1.00; Figure 7-3).
3.3 Quality assessment
Overall, the risk of bias for all studies was generally low, with the exception of the unclear
mentioned of allocation concealment, and blinding of participants and personnel because
of the nature of open-label design. The objective analysis of the efficacy and viral load
measurement were not likely to be disrupted by blinding or not, but the process of
blinding may have been important for assessment of subjective analysis, for examples,
drug-related adverse events. Three studies26-28 assessed with unclear risk on reporting bias,
because those published as an abstract on posters or reports on AIDS conferences with
preliminary or simplistic results. No study assessed the attrition bias for incomplete
outcome data because of high rate of loss to follow-up (Figure 2a, 2b).
We summarized the certainty of evidence findings for three HIV-positive populations;
virally suppressed (Table 3), treatment-naive with stratification of ARV mechanism
(Table 4,5,6) and treatment-experienced (Table 7) by GRADE approach. For the
virological suppression outcomes at 48 weeks, the certainty of evidence was high for
treatment-naive patients when compared to EFV-based regimen, PI-based regimen and
treatment-experienced patients. There was moderate quality evidence that both treatment-
naive patients using DTG-based compared to InSTI-based regimen and virally suppressed
patients switched to DTG-based, both did not reached significantly different, contributed
by four and six trials separately. Evidence quality was mainly downgraded for imprecision
because of few clinical events in several studies14-16,25. For tolerability outcomes, the
certainty of evidence was low for most scenarios, mainly downgraded by potential
performance bias because limited by open-label design and imprecise estimates for
limited number of events and wide confidence intervals reported. In contrast, evidence
quality were upgraded one level because of large magnitude of estimated effect with no
plausible confounders while DTG-based compared to EFV-based and PI-based regimen
in treatment-naive patients group.
Chapter 4: Discussion
Although the aspect of cost-benefit considerations and the global health burden
endorsed by international agencies, especially the WHO, there had been more LMICs
large-scale initiative to implement DTG transition programme, switching DTG-based as
the first-line regimen, which is still an importance issues on how likely to perform within
HIV-positive patients. In this meta-analysis, we provided a more comprehensive view of
relative efficacy and tolerability between DTG-based regimen and others combination
ART in three independent scenarios of HIV-positive populations. Our results
demonstrated that HIV virally suppressed patients who was no significant difference rate
of both viral suppression and discontinuation due to any adverse events. For efficacy,
among three studies12,15,16 showed virological benefit were trend toward others ART-
based regimen. Patients in DOLAM15 and ASPIRE16 who were assigned to control group
for non-switching regimen but remained current ART (cART), among patients in
DOLAM mostly with NNRTI-based regimen (71%) at baseline. Patients in NEAT02212
control group were assigned to continue using ritonavir-boosted PI regimen, primarily
ritonavir-boosted darunavir (51%), with TDF/FTC backbone (65%) at baseline. Results
of efficacy demonstrated a robust and well homogeneity, supported by stratification
factors of different follow-up durations. For tolerability, the estimated risk ratios showed
a large effect and higher proportion of discontinuation of study drug related to adverse
events after switched to DTG-based regimen, among three DTG-switch trials12,13,17
shown a well-tolerated aspect on another ART regimen, even there was no significant
difference between both groups at the endpoint. Nevertheless, the particularly notable risk
ratio of discontinuation due to any AEs reported within the DTG-switch arm was
expectable while compared with remaining on a stable baseline regimen that patients have
been well-tolerating from a long period of time. Based on the results that we did not
support a proactive practice to switch the current ART to DTG-based regimen while the
patients were reaching virological suppression, since the risk of switching could outweigh
the benefits. But for specific long-term safety, patients who switched from tenofovir
disoproxil fumarate (TDF) combination to DTG-based regimens was associated with
reduced bone mineral density31 and improved bone turnover markers.17 Moreover, DTG
is likely to be a good substitute therapeutic ART class to LPV/r for HIV patients due to
less likely to dyslipidemia. Patients with those comorbidities that may derive benefit from
being switched to DTG-based regimen. However, in some LMICs had been already
completed the DTG transition programme by amended their national guidelines and prior
preferred standard EFV were no longer available, that is necessary for national healthcare
and provider take caution the emergence of ART discontinuation while patients switching
regimen to DTG-based.
A second sub-population analysis was performed to compare efficacy and tolerability
in treatment-naive patients using DTG-based regimen, could had a significantly better
efficacy up to week 48, either included the study of pregnant women and HIV-associated
TB coinfected patients or not. Sensitivity analyses all showed treatment differences in
favour of the DTG-based regimen and subgroup analysis revealed DTG-based regimen
versus EFV- and PI-based regimen, was associated with a greater proportion of patients
being virally suppressed; versus others InSTI-based regimen with marginally
significantly better, at week 48 after ART initiation, which was partly consistent with the
pooled result by George;32 included two original DTG versus EFV RCTs with HIV-
positive treatment-naive populations. However, we cannot directly contrast the result with
Junjun’s study33, since the misclassification subgroup analysis. There was moderate to
high quality evidences of achieved viral suppression for DTG-based relative to others
mechanisms-based ART in treatment-naive patients. For tolerability, the superior
responses were also driven by a reduction risk to discontinue ART due to any adverse
events in the DTG-based regimen than EFV-based and PI-based regimen, both evidences
was upgraded to high and moderate quality separately, based on the large magnitude of
effect that was observed. Although the comparison to others InSTI-based regimen was no
statistically significant, which was correspond to the large prospective cohort study,34 but
with low quality evidences nevertheless. Overall, our results consistently supported the
WHO 2018 latest guideline suggestion; recommended DTG-based as the preferred first-
line regimen for people living with HIV initiating ART with conditional recommendation.
For DTG-based used in treatment-experienced patients, despite insufficient number of
RCTs included, we found that DTG-based regimen was associated with a significantly
greater proportion of treatment-experienced patients achieving virological suppression,
at the end of 48 weeks after initiated second-line regimen. Our results provided the
efficacy related quality evidence was high certainty; which showed that DTG-based was
an effective ART regimen for second-line among adults for whom a NNRTI- or PI- based
first-line regimen had failed. For tolerability, results also supported DTG-based as an
alternative regimen based on patients in the DTG-based regimen were almost a half times
the risk less likely to discontinue their ART due to any adverse events. On the overall of
our findings, DTG in combination with an optimized backbone was a superior regimen
for treatment-experienced patients with HIV.
Our meta-analysis was included all adequate RCTs and introduced new scenario which
contributed to a consolidated view for DTG-based efficacy and tolerability profile.
However, there were few limitations existed. First, the predominant of the study
characteristics, which may not be fully represented to the global HIV epidemic, since the
mainly completed by white and male adults in developed country settings, typically
limiting the evidences for pregnant women, people with HIV-associated TB and people
with advanced HIV infection. Recent studies also did not consider the integral
circumstances, the people who lived in resource-limited LMICS, where an increasing rate
of NRTI- and NNRTI-transmitted resistance and local people without sufficient medium
of healthcare services,35 for example: HIV viral load monitoring, drug mutation or
resistance testing. Second, tolerability outcome was analyzed considering ART
discontinuations due to any adverse events, but study drug-related adverse events were
not independently reported on each included RCT, thus it may leading to an
overestimation of ART discontinuations rate. Nonetheless, there are several ongoing
RCTs will enable to fit the evidence gaps in the forthcoming year, using DTG-based
regimen with assessment of virologic efficacy and safety of HIV-positive pregnant
women and their infants; VESTED (NCT03048422) and DolPHIN2 (NCT03249181),
switching to DTG-based regimen with dual regimen simplification; DUALIS
(NCT02486133), the more detailed data highlight the HIV-positive patients from LMICs
who failing the first-line regimen; D2EFT (NCT03017872).
In summary, our meta-analyses show that the DTG-based regimens have superior
efficacy and tolerability to EFV- and PI- based regimens for patients who are treatment-
naive, and treatment-experienced patients with virological failure. Conversely, for those
who already achieved virological suppression under other regimens, switch to DTG-
based regimen did not yield a better virological suppression rate by 24-48 weeks.
Furthermore, for this group of patients, switch from a stable regimens to DTG-based
regimens is associated with an inferior tolerability.
Reference
1. World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing hiv infection recommendations for a public health approach,second edition. 2016.
2. Kanters S, Vitoria M, Doherty M et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and
network meta-analysis. The Lancet HIV 2016; 3: e510-e20.
3. World Health Organization. Updated recommendations on first-line and second- line antiretroviral regimens and post-exposure prophylaxis and recommendations on early infant diagnosis of HIV: interim guidelines. Supplement to the 2016 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection.
Geneva: (WHO/CDS/HIV/18.51). Licence: CC BY-NC-SA 3.0 IGO., 2018.
4. World Health Organization. Updated recommendations on first-line and second- line antiretroviral regimens and post-exposure prophylaxis and recommendations on early infant diagnosis of HIV: interim guidance. Geneva: (WHO/CDS/HIV/18.18).
Licence: CC BY-NC-SA 3.0 IGO., 2018.
5. World Health Organization. Kanters S, Jansen J, Zoratti M, Forrest J, Humphries B, Campbell J. Web Annex B. Systematic literature review and network meta-analysis assessing first-line antiretroviral treatments In: Updated recommendations on first-line and second-line antiretroviral regimens and post-exposure prophylaxis and
recommendations on early infant diagnosis of HIV: interim guidelines. Supplement to the 2016 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Geneva: (WHO/CDS/HIV/18.25). Licence: CC BY-NC-SA 3.0 IGO., 2018.
6. Vineet Prabhu CW, Sarah Jenkins, Saman Nizami, Kelly Catlin, Paul Domanico.
New ARVs Could Represent Over USD 3 Billion in Cost Savings Through 2025.
Conference on Retroviruses and Opportunistic Infections. Boston, MA, USA, 2016.
7. Vitoria M, Ford N, Clayden P et al. When could new antiretrovirals be
recommended for national treatment programmes in low-income and middle-income countries: results of a WHO Think Tank. Curr Opin HIV AIDS 2017; 12: 414-22.
8. Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6: e1000097.
9. Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of
Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011.
Available from http://handbook.cochrane.org.
10. Higgins JP, Altman DG, Gotzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011; 343: d5928.
11. Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for
grading quality of evidence and strength of recommendations. Updated October 2013.
The GRADE Working Group, 2013. Available fromguidelinedevelopment.org/handbook.
12. Gatell JM, Assoumou L, Moyle G et al. Switching from a ritonavir-boosted protease inhibitor to a dolutegravir-based regimen for maintenance of HIV viral suppression in patients with high cardiovascular risk. AIDS 2017; 31: 2503-14.
13. Trottier B, Lake JE, Logue K et al. Dolutegravir/abacavir/lamivudine versus current ART in virally suppressed patients (STRIIVING): a 48-week, randomized, non- inferiority, open-label, Phase IIIb study. Antivir Ther 2017; 22: 295-305.
14. Molina J-M, Ward D, Brar I et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from dolutegravir plus abacavir and lamivudine in virologically suppressed adults with HIV-1: 48 week results of a
randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial.
The Lancet HIV 2018; 5: e357-e65.
15. Blanco JL, Rojas J, Paredes R et al. Dolutegravir-based maintenance monotherapy versus dual therapy with lamivudine: a planned 24 week analysis of the DOLAM randomized clinical trial. J Antimicrob Chemother 2018; 73: 1965-71.
16. Taiwo BO, Marconi VC, Berzins B et al. Dolutegravir Plus Lamivudine Maintains Human Immunodeficiency Virus-1 Suppression Through Week 48 in a Pilot
Randomized Trial. Clin Infect Dis 2018; 66: 1794-7.
17. Llibre JM, Hung C-C, Brinson C et al. Efficacy, safety, and tolerability of dolutegravir-rilpivirine for the maintenance of virological suppression in adults with HIV-1: phase 3, randomised, non-inferiority SWORD-1 and SWORD-2 studies. The
Lancet 2018; 391: 839-49.
18. van Lunzen J, Maggiolo F, Arribas JR et al. Once daily dolutegravir
(S/GSK1349572) in combination therapy in antiretroviral-naive adults with HIV:
planned interim 48 week results from SPRING-1, a dose-ranging, randomised, phase 2b trial. The Lancet Infectious Diseases 2012; 12: 111-8.
19. Raffi F, Rachlis A, Stellbrink H-J et al. Once-daily dolutegravir versus raltegravir in antiretroviral-naive adults with HIV-1 infection: 48 week results from the
randomised, double-blind, non-inferiority SPRING-2 study. The Lancet 2013; 381: 735- 43.
20. Walmsley SL, Antela A, Clumeck N et al. Dolutegravir plus abacavir-lamivudine for the treatment of HIV-1 infection. N Engl J Med 2013; 369: 1807-18.
21. Clotet B, Feinberg J, van Lunzen J et al. Once-daily dolutegravir versus darunavir plus ritonavir in antiretroviral-naive adults with HIV-1 infection (FLAMINGO): 48 week results from the randomised open-label phase 3b study. The Lancet 2014; 383:
2222-31.
22. Gallant J, Lazzarin A, Mills A et al. Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised
controlled non-inferiority trial. The Lancet 2017; 390: 2063-72.
23. Sax PE, Pozniak A, Montes ML et al. Coformulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection (GS-US-380–1490): a randomised, double-blind, multicentre, phase 3, non-inferiority trial. The Lancet 2017; 390: 2073-82.
24. Orrell C, Hagins DP, Belonosova E et al. Fixed-dose combination dolutegravir, abacavir, and lamivudine versus ritonavir-boosted atazanavir plus tenofovir disoproxil fumarate and emtricitabine in previously untreated women with HIV-1 infection
(ARIA): week 48 results from a randomised, open-label, non-inferiority, phase 3b study.
The Lancet HIV 2017; 4: e536-e46.
25. Sax PE, DeJesus E, Crofoot G et al. Bictegravir versus dolutegravir, each with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection: a randomised, double-blind, phase 2 trial. The Lancet HIV 2017; 4: e154-e60.
26. C. Orrell KK, J.A. Coombs, A. Amara, L. Myer, J. Kaboggoza. DolPHIN-1 : Randomised controlled trial of dolutegravir (DTG)- versus efavirenz (EFV)-based therapy in mothers initiating antiretroviral treatment in late pregnancy. 22nd
International AIDS Conference, 2018.
27. Dooley KE, Kaplan R, Mwelase N et al. Dolutegravir-Based Antiretroviral Therapy for Patients Co-Infected with Tuberculosis and Hiv: A Multicenter, Noncomparative, Open-Label, Randomized Trial. Clin Infect Dis 2019.
28. A Cournil CK, S Eymard-Duvernay, S Lem, M Mpoudi-Ngole, P Omgba.
Dolutegravir- versus an efavirenz 400 mg-based regimen for the initial treatment of HIV-infected patients in Camer- oon: 48-week efficacy results of the NAMSAL ANRS 12313 trial. J Int AIDS Soc, 2018.
29. Cahn P, Pozniak AL, Mingrone H et al. Dolutegravir versus raltegravir in
antiretroviral-experienced, integrase-inhibitor-naive adults with HIV: week 48 results from the randomised, double-blind, non-inferiority SAILING study. The Lancet 2013;
382: 700-8.
30. Aboud M, Kaplan R, Lombaard J et al. Dolutegravir versus ritonavir-boosted lopinavir both with dual nucleoside reverse transcriptase inhibitor therapy in adults with HIV-1 infection in whom first-line therapy has failed (DAWNING): an open-label, non- inferiority, phase 3b trial. The Lancet Infectious Diseases 2019; 19: 253-64.
31. McComsey GA, Lupo S, Parks D et al. Switch from tenofovir disoproxil fumarate combination to dolutegravir with rilpivirine improves parameters of bone health. AIDS 2018; 32: 477-85.
32. Rutherford GW, Horvath H. Dolutegravir Plus Two Nucleoside Reverse
Transcriptase Inhibitors versus Efavirenz Plus Two Nucleoside Reverse Transcriptase Inhibitors As Initial Antiretroviral Therapy for People with HIV: A Systematic Review.
PLoS One 2016; 11: e0162775.
33. Jiang J, Xu X, Guo W et al. Dolutegravir(DTG, S/GSK1349572) combined with other ARTs is superior to RAL- or EFV-based regimens for treatment of HIV-1
infection: a meta-analysis of randomized controlled trials. AIDS Res Ther 2016; 13: 30.
34. Llibre JM, Montoliu A, Miro JM et al. Discontinuation of dolutegravir,
elvitegravir/cobicistat and raltegravir because of toxicity in a prospective cohort. HIV
Med 2019; 20: 237-47.
35. World Health Organization. Guidelines on the public health response to pretreatment HIV drug resistance,Geneva Licence: CC BY-NC-SA 3.0 IGO. 2017.
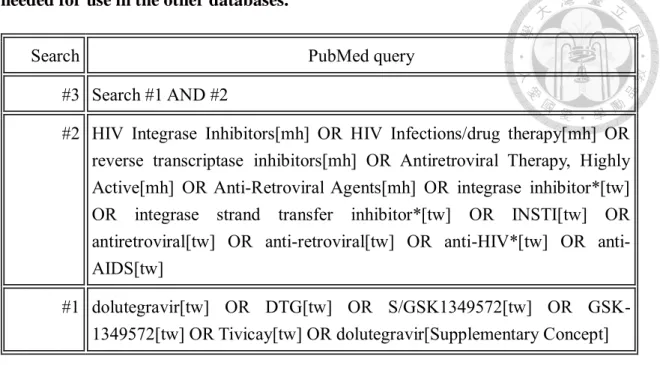
Table 1: PubMed and Embase search strategy, which was modified and adapted as needed for use in the other databases.
Search PubMed query
#3 Search #1 AND #2
#2 HIV Integrase Inhibitors[mh] OR HIV Infections/drug therapy[mh] OR reverse transcriptase inhibitors[mh] OR Antiretroviral Therapy, Highly Active[mh] OR Anti-Retroviral Agents[mh] OR integrase inhibitor*[tw]
OR integrase strand transfer inhibitor*[tw] OR INSTI[tw] OR antiretroviral[tw] OR anti-retroviral[tw] OR anti-HIV*[tw] OR anti- AIDS[tw]
#1 dolutegravir[tw] OR DTG[tw] OR S/GSK1349572[tw] OR GSK- 1349572[tw] OR Tivicay[tw] OR dolutegravir[Supplementary Concept]
[mh] = Medical Subject Heading (MeSH) term. [tw] = text word. [pt] = publication type.
Search Embase query
#3 Search #1 AND #2
#2 HIV Integrase Inhibitors OR HIV Infections therapy OR HIV drug therapy OR reverse transcriptase inhibitors OR Antiretroviral Therapy, Highly Active OR Anti-Retroviral Agents OR integrase inhibitor* OR integrase strand transfer inhibitor* OR INSTI OR antiretroviral OR anti-retroviral OR anti-HIV* OR anti-AIDS
#1 dolutegravir OR DTG OR GSK1349572 OR GSK-1349572 OR Tivicay
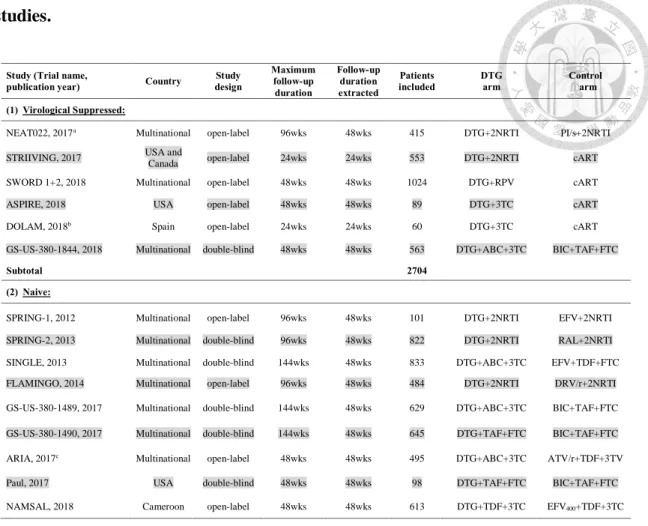
Table 2: Characteristics of patients included in the selected randomized control trial studies.
Study (Trial name,
publication year) Country Study
design
Maximum follow-up duration
Follow-up duration extracted
Patients
included DTG
arm Control
arm (1) Virological Suppressed:
NEAT022, 2017a Multinational open-label 96wks 48wks 415 DTG+2NRTI PI/s+2NRTI STRIIVING, 2017 USA and
Canada open-label 24wks 24wks 553 DTG+2NRTI cART
SWORD 1+2, 2018 Multinational open-label 48wks 48wks 1024 DTG+RPV cART
ASPIRE, 2018 USA open-label 48wks 48wks 89 DTG+3TC cART
DOLAM, 2018b Spain open-label 24wks 24wks 60 DTG+3TC cART
GS-US-380-1844, 2018 Multinational double-blind 48wks 48wks 563 DTG+ABC+3TC BIC+TAF+FTC
Subtotal 2704
(2) Naive:
SPRING-1, 2012 Multinational open-label 96wks 48wks 101 DTG+2NRTI EFV+2NRTI SPRING-2, 2013 Multinational double-blind 96wks 48wks 822 DTG+2NRTI RAL+2NRTI SINGLE, 2013 Multinational double-blind 144wks 48wks 833 DTG+ABC+3TC EFV+TDF+FTC FLAMINGO, 2014 Multinational open-label 96wks 48wks 484 DTG+2NRTI DRV/r+2NRTI GS-US-380-1489, 2017 Multinational double-blind 144wks 48wks 629 DTG+ABC+3TC BIC+TAF+FTC GS-US-380-1490, 2017 Multinational double-blind 144wks 48wks 645 DTG+TAF+FTC BIC+TAF+FTC ARIA, 2017c Multinational open-label 48wks 48wks 495 DTG+ABC+3TC ATV/r+TDF+3TV
Paul, 2017 USA double-blind 48wks 48wks 98 DTG+TAF+FTC BIC+TAF+FTC
NAMSAL, 2018 Cameroon open-label 48wks 48wks 613 DTG+TDF+3TC EFV400+TDF+3TC
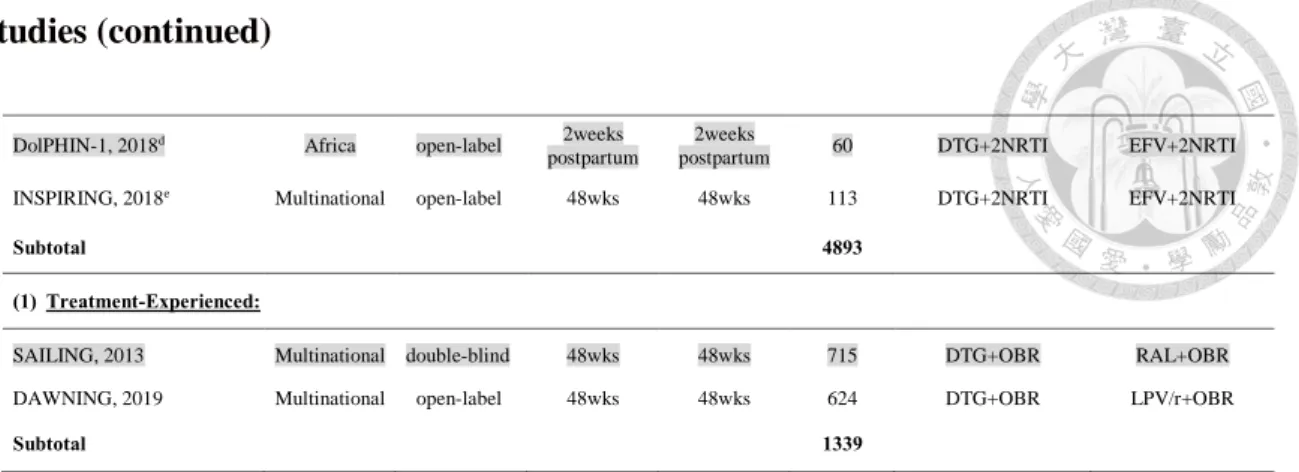
Table 2: Characteristics of patients included in the selected randomized control trial studies (continued)
DolPHIN-1, 2018d Africa open-label 2weeks postpartum
2weeks
postpartum 60 DTG+2NRTI EFV+2NRTI
INSPIRING, 2018e Multinational open-label 48wks 48wks 113 DTG+2NRTI EFV+2NRTI
Subtotal 4893
(1) Treatment-Experienced:
SAILING, 2013 Multinational double-blind 48wks 48wks 715 DTG+OBR RAL+OBR
DAWNING, 2019 Multinational open-label 48wks 48wks 624 DTG+OBR LPV/r+OBR
Subtotal 1339
NRTI, Nucleoside reverse transcriptase inhibitors; PI/s, ritonavir-boosted protease inhibitor; RPV, Rilpivirine; 3TC, lamivudine;
ABC, abacavir; FTC, emtricitabine; BIC, bictegravir; TAF, Tenofovir alafenamide; DRV/r, darunavir/ritonavir; ATV/r,
Atazanavir/ ritonavir; EFV, Efavirenz; EFV400, 400mg Efavirenz; RAL, raltegravir; LPV/r, lopinavir/ritonavir; cART, current ART regimen;
OBR, investigator-selected optimized backbone regimen.
a In total, 74% patients with a Framingham CVD risk score 10-year risk score more than 10%.
b This study included three different treatment arms with DTG dual- and mono-therapy.
c Eligible patients in this study were only women who aged 18 years or older, pregnant women were excluded.
d This study included Pregnant HIV positive women, initiated ART in third trimester of pregnancy, who randomised to receive DTG or EFV until two weeks postpartum.
e This study enrolled HIV-1 infected ART-naive patients with drug-sensitive tuberculosis, who allocated to DTG arm and received 50 mg twice-daily during and 2 weeks post-tuberculosis therapy, then 50 mg once-daily.
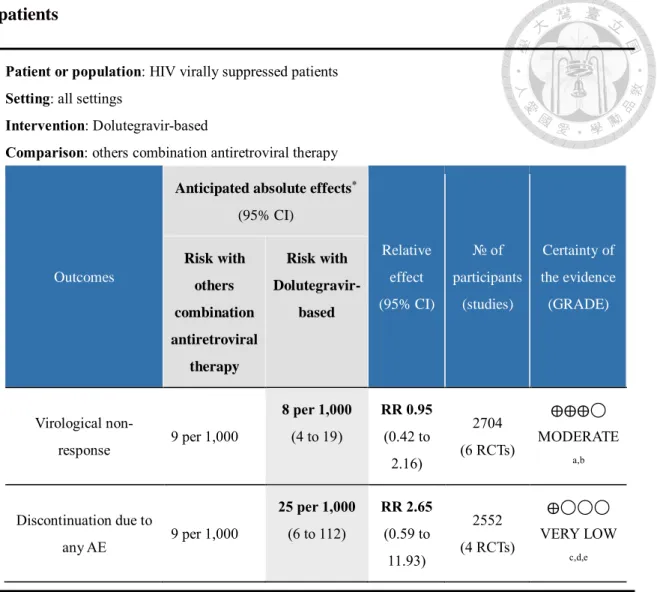
Table 3: Summary of findings: certainty of evidence for HIV virally suppressed patients
Patient or population: HIV virally suppressed patients Setting: all settings
Intervention: Dolutegravir-based
Comparison: others combination antiretroviral therapy
Outcomes
Anticipated absolute effects
*(95% CI)
Relative effect (95% CI)
№ of participants
(studies)
Certainty of the evidence (GRADE) Risk with
others combination antiretroviral
therapy
Risk with Dolutegravir-
based
Virological non-
response 9 per 1,000
8 per 1,000 (4 to 19)
RR 0.95 (0.42 to
2.16)
2704 (6 RCTs)
⨁⨁⨁◯
MODERATE
a,b
Discontinuation due to
any AE 9 per 1,000
25 per 1,000 (6 to 112)
RR 2.65 (0.59 to
11.93)
2552 (4 RCTs)
⨁◯◯◯
VERY LOW
c,d,e
*The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio
GRADE Working Group grades of evidence
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
a. Risk of bias: five trials were open-label, but we did not downgrade for this because objective outcome unlikely to be affected b. Imprecision: downgraded by 1 for some trials with wide CIs and few clinical events.
c. Risk of bias: downgraded by 1 due to three of four trials were open-label.
d. Inconsistency: downgraded by 1 as unexplained heterogeneity.
e. Imprecision: downgraded by 2 for few clinical events and wide CIs.
Table 4: Summary of findings: certainty of evidence for HIV treatment-naive patients
Patient or population: HIV treatment-naive patients Setting: all settings
Intervention: Dolutegravir-based Comparison: Efavirenz-based
Outcomes
Anticipated absolute
effects
*(95% CI) Relative effect (95%
CI)
№ of participants
(studies)
Certainty of the evidence (GRADE) Risk with
Efavirenz- based
Risk with Dolutegravir-
based
Viral suppression to non- detectable
659 per 1,000
738 per 1,000 (692 to 785)
RR 1.12 (1.05 to
1.19)
1547 (3 RCTs)
⨁⨁⨁⨁
HIGH
aDiscontinuation due to any AE
90 per 1,000
21 per 1,000 (11 to 39)
RR 0.23 (0.12 to
0.43)
1047 (3 RCTs)
⨁⨁⨁⨁
HIGH
b,c*The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio
GRADE Working Group grades of evidence
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
a. Risk of bias: two trials were open-label, but we did not downgrade for this because objective outcome unlikely to be affected.
b. Risk of bias: downgraded by 1 due to two trials were open-label.
c. Other factors: Large effects can lead to upgrading the quality by one level, using by RR >2 or <0.5 as a guide.