Graduate Institute of Linguistics College of Liberal Arts
National Taiwan University Master Thesis
醫病溝通中之協商:以北台灣之眼科醫師為例 Politeness in Medical Communication:
A Study Based on an Ophthalmology Clinic in Northern Taiwan
許學旻
Vian Hsueh-Min Hsu
指導教授:蘇以文 博士 Advisor: Lily I-Wen Su, Ph.D.
中華民國 106 年 7 月
July 2017
Acknowledgements
非常感謝我的指導教授,蘇以文教授,願意支持我做這麼具有挑戰的題目,
在醫療現場採集實際醫病溝通的語料並不容易,蘇老師全然的支持是我這個研究 最大的動力,蘇老師的鼓勵印證了“Do the right thing even if it's hard.”在研究過程中 蘇老師樂於提供各種協助,當我遇到困難時,總是能藉由討論,激盪出更多想法 與解決的方式,為我指點迷津,並給予強大的支持與鼓勵,因為有老師的引導,
這個研究才能更加完整的呈現,能有這個研究,蘇老師無疑是最大的推手。
同時,也非常感謝我的口試委員,蔡美慧教授與蔡宜妮教授,他們寶貴的建 議對於研究有極大的助益,蔡美慧教授是臺灣從語言學角度研究醫病關係的先驅 與巨擘,能有機會請蔡美慧教授提點我的研究真是莫大的榮幸,蔡教授對於研究 的建議深入而透澈,當初決定研究的主題便是受到蔡美慧教授研究的啟發,很感 謝能有機會對台灣的醫病溝通研究做一些貢獻。蔡宜妮教授曾指導我篇章分析的 課程,課堂上精闢的解析與實作為我打下做言談分析深厚的基礎,蔡教授提供的 建議對於這個研究的精進貢獻良多、功不可沒,更幫助我解決很多在研究中所遇 到的問題。
很感謝語言所老師們的指導,謝舒凱教授、李佳霖教授、呂佳蓉教授、江文 瑜教授紮實的訓練培養出我在語言學的專業,多元化的課程使我擁有跨領域的能 力。也很感謝師大英語系老師們的專業教學與全方位的訓練,讓我保有熱忱繼續 求知,為我打下良好的基石並擁有不同的視野,特別感謝梁孫傑教授、劉宇挺教
授、蘇席瑤教授、詹曉蕙教授、李宜倩教授與Professor Mary A. Goodwin 的啟發與
鼓勵,讓我可以在朝著目標邁進時昂首闊步,擁有智慧與執著的勇氣。
非常感謝臺大醫院眼科部的醫師,在極度繁忙的門診中願意協助研究的進行 與收案,使臺灣的醫病溝通現況能以語言學的角度呈現。從研究主題發想開始,
我有機會能與蘇以文教授團隊夥伴相互討論,幫助我建立研究的主軸與方向,感
謝Chester, Hsin-Yen, Val 與 Veasna 的意見及在研究過程中所有的提攜與協助。感
謝摯友Anita, Bill, John, Ying 的各種支持、幫助與陪伴,這個研究才得以順利完成。
也很感謝所有曾經不吝給予幫助、建議、支持、鼓勵、包容與關懷的老師與朋友,
你們是我堅持下去的動力。
最後很謝謝我的家人,一路上無條件的支持、包容與愛,讓我得以追求夢想 與心之所向,很感激你們總是相信我、理解我、深愛我,今天能有任何一點小成 就都要歸功於我的家人。
謝謝所有在人生旅途中相助相知相惜的人們,讓我成為更好的自己,打從心 底愛你們!
Abstract
This study investigates face-to-face doctor-patient communication and aims to provide a linguistic viewpoint of doctor-patient relationships. It illustrates doctor-patient communication as a negotiated and co-constructed process between the doctor, patients, and patients’ companions. Due to their power asymmetry, the participants use different politeness strategies to achieve their communicative goals. When the patients’
companions are present, the consultation is more complex.
Researches related to doctor-patient communication have increased in the past few decades in the West. Medical education and system in Taiwan have also adapted accordingly. Studies have shown that communication between doctors and patients is influenced by their institutional power asymmetry. From a doctor's point of view, the purpose is to provide the best medical treatment for the patients. On the other hand, patients want to choose their preferred treatments. The doctor and patient parties exchange information and reach their decisions through communication.
In this study, we analyze qualitatively how the doctor, the patients, and their companions co-construct communication during their negotiations. This research is conducted in an eye clinic in a medical center in Northern Taiwan. There are in total 45 patients (16 males and 29 females), and 5 companions (2 wives, 1 husband, 2 daughters, and 1 son) in this study. We explore the data by referring to Brown and Levinson’s (1978) politeness model, specifically bald recommendations, collaborative plural, and hedges under Taiwanese social and cultural factors. During the consultations, when the participants give advice or make requests, they try to protect each other’s positive or negative faces. If the family companions join the consultation, they may raise questions or make requests for the patients. The consultation is different depending on the participants involved.
This research shows how the power asymmetry between the doctor and patients affects the way they use politeness strategies to achieve their communicative goals.
Finally it also allows us to understand the importance of doctor-patient negotiation to create more equal and harmonious doctor-patient relationships in Taiwan.
Keywords: medical discourse, doctor-patient communication, doctor-patient-companion communication, triadic medical communication, politeness
Chinese Abstract
本研究主要關注於醫病溝通間醫師、病人與陪同者相互協商與共同建構的溝 通過程。由於權力的不同導致在看診時,參與者為了達到各自的溝通目的而使用 不同的禮貌策略,當有陪同者在現場時,會使問診過程更加複雜。本論文希望藉 由臨床上實際醫病溝通的語料,提供一個增進醫病關係的切入點,從語言學觀點 探討增進醫病溝通的可能。
醫病溝通相關研究在西方已蓬勃發展數十年,台灣的醫學教育與體系也是承 襲西方醫學,然而,醫病問診中因為醫師與病人地位不平等或是權力的拉鋸,是 影響醫病溝通的因素。在醫師的角度,希望能給予病患最好的治療,並增加病人 遵醫囑的接受度,對於患者而言,他們想要選擇偏好的治療,或是對於病況有疑 問能得到解答,雙方透過溝通來達到交換資訊與達到共同決策的目的。
本研究採用質化的方式分析語料,藉由醫病與陪同者間一步步共同構築而成 的協商來探究參與者實際的溝通目的,本研究在北部一間醫學中心的眼科門診執
行,總共有45 位患者參與本研究,16 位男性,29 位女性,陪同者共有 5 位,2 位
妻子、1 位先生、2 位女兒與 1 位兒子。在台灣的社會與文化背景中,從 Brown 及 Levinson (1978)的禮貌模型出發,著重在三個禮貌策略:直接提出要求、使用第一 人稱複數來涵蓋所有參與者、避免正面回答,因為在問診過程中,參與者在給予 意見與提出要求時,會為了要保護對方或自己的正反面子而會有所調整。若陪同 者加入,他們會替病人問問題或是提出要求,整個問診過程會因為角色與溝通目 的的不同而有所改變及調整。
本研究的目標是希望能呈現醫師與病人因為權力不平等,進而影響他們為了 達到溝通目的時所使用的不同禮貌策略,透過實際語料的分析,加上台灣特殊的 文化背景,提供醫療服務人員與患者一個不同的視角,從語言學的角度剖析醫病 協商的現況與重要性,以期在未來達到更平等更和諧的醫病溝通與醫病關係。
關鍵字:醫病言談、醫病溝通、醫師病人陪同者溝通、醫病三方溝通、禮貌
Table of Contents
ACKNOWLEDGEMENTS ... I ABSTRACT ... II CHINESE ABSTRACT ... III TABLE OF CONTENTS ... IV LIST OF FIGURES ... V TRANSCRIPTION CONVENTIONS ... VI
CHAPTER 1. INTRODUCTION ... 1
1.1MOTIVATION ... 5
1.2RESEARCH QUESTIONS ... 8
1.3ORGANIZATION OF THE THESIS ... 9
CHAPTER 2. LITERATURE REVIEW ... 10
2.1DOCTOR-PATIENT COMMUNICATION ... 10
2.2POLITENESS ... 13
2.3POWER ... 20
CHAPTER 3. METHODOLOGY ... 23
3.1DATA COLLECTION ... 24
3.2THEORETICAL BACKGROUND ... 26
3.3ANALYTICAL FRAMEWORK ... 27
3.4DATA TRANSCRIPTION ... 29
CHAPTER 4. POLITENESS STRATEGIES IN MEDICAL COMMUNICATION .. 30
4.1STRATEGIES IN DYADIC INTERACTION ... 31
4.1.1BALD RECOMMENDATIONS ... 32
4.1.2COLLABORATIVE PLURAL ... 46
4.1.3HEDGES ... 50
4.2STRATEGIES IN TRIADIC INTERACTION ... 55
4.2.1BALD RECOMMENDATIONS ... 56
4.2.2COLLABORATIVE PLURAL ... 63
4.2.3HEDGES ... 66
CHAPTER 5. DISCUSSION AND CONCLUSION ... 71
5.1POLITENESS IN MEDICAL DISCOURSE ... 71
5.2SIGNIFICANCE OF THE STUDY ... 74
5.3LIMITATIONS AND SUGGESTIONS FOR FUTURE STUDIES ... 76
REFERENCES ... 78
List of Figures
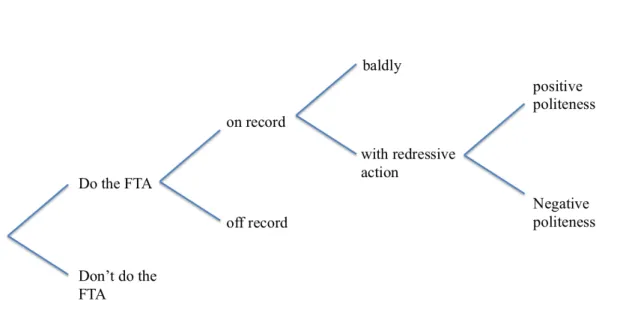
Figure 1. Possible strategies for doing FTAs ………16
Transcription Conventions
[ ] Beginning and ending of overlap in speakers’ utterances
? Upward intonation
CAPITALS Relatively high amplitude (in Mandarin transcription: bold)
/ / Encloses description of how talk is delivered
_____ Code-switching (e.g. Taiwanese)
= Latching
.. Short pause
… Long pause
[…] Text omission
Chapter 1. Introduction
This study examines doctor-patient communication as a negotiated and
co-constructed process between health providers, patients, and patients’ family
members. Studies from Western countries have revealed that an open communication
can improve the quality of health care, the patients’ compliance, and both the doctors’
and patients’ mental health (Ong et al., 1995; Maguire and Pitceathly, 2002). It also
allows patients to express their concerns and medical preferences (Charles et al., 1999;
Makoul and Clayman, 2006). Many doctors in Southeast Asia receive their medical
education through a Western system (Claramita et al., 2011), following the curriculum
of Western medicine schools. Studies have shown that in Southeast Asian settings both
doctors and patients favor the egalitarian communication style (Haviland et al., 2005).
When under a specific clinical context, doctor-patient communication is influenced
by the power asymmetry between the participants. Because of the asymmetry between
doctors and patients, patients tend to respect doctors and not challenge their authority in
order to maintain harmony during medical consultation. Their communication is
examined as a tool for rapport and solidarity (Kuipers, 1989; Tannen, 1990).
In Medical communication, some topics are commonly addressed:(1) different
purposes of medical communication; (2) analysis of doctor-patient communication; (3)
specific communicative behaviors; (4) the influence of communicative behaviors on
patient outcomes; and (5) concluding remarks (Ong, 1995). Most studies focus on
doctor-patient relationships only. However, patient’s companion (e.g. spouses, family
members, friends) as a third party influence the doctor-patient relationship (Keady and
Nolan, 2003; Ishikawa et al., 2005; Karnieli-Miller et al., 2012). Besides, the different
visits, companion roles, and the companion involvement are the factors to change the
dynamic of the consultations. The companion may limit the patient’s involvement or
even exclude the patient from the decision-making (Coe and Prendergast, 1985;
Beisecker , 1989; Greene et al., 1994) or can benefit the doctor-patient communication
and increase patient’s comprehension and involvement compared with the
unaccompanied patients (Clayman, 2005; Labrecque et al., 1991; Prohaska and Glasser,
1996; Schilling et al., 2002).
The growing studies examine the involvement of patient’s family companions to
the medical consultations (Wolff and Roter, 2011; Laidsaar-Powell et al., 2013; Wolff
et al., 2017). But the focuses are mostly on the specific doctor-patient-companion
communication on the elderly or cognitively impaired patients (Smith and Beattie, 2001;
Werner and Kitai, 2004; Zaleta and Carpenter, 2010; Sakai and Carpenter, 2011;
Karnieli-Miller et al., 2012), or on doctor-parent-child communication (Tannen and
Wallat, 1983; Aronsson and Rundström, 1988; Van Dulmen, 1998; Tates and
Meeuwesen, 2001). In the United States, over one-third of elderly patients have a
companion when seeing the doctors (Wolff and Roter, 2008). In Taiwan, there are
already some researches related to the triadic doctor-patient-companion communication.
For example, the companion’s participation can influence the patient parties’
information providing sequences (Tsai, 2007b). And the opening stage in medical
encounters in Taiwan is very different from the western style because of the time limits
and replaced by situational greeting instead (Tsai, 2005). Another study focuses on the
verbal and nonverbal triadic interaction in Taiwan, the spatial arrangement of patient
companions in geriatric triadic medical consultations can reflect the patient’s role in the
medical consultations and the relationships with their family companions (Tsai, 2007a).
The present framework for analyzing the third party’s participant may not be suitable
for Mandarin and Southern Min, Tsai (2003) identifies the problems when identifying
the participant structure in medical triadic consultations in Taiwan and provides some
solutions when examining the companion’s participation.
Tsai (2000) proposed a systematic framework to analyze the companion’s
participation. One of the results shows that the companion’s interruption does influence
the communication between the doctor and the patient. Even though most of the patients
are the main information providers, it is hard for them to complete their responses when
both the patient and the companion are talking.
Instead of studying the patterns, participants’ involvement, or patient’s satisfaction
in medical discourse, we try to analyze medical communication in a different domain,
the idea of politeness. Previous study applies politeness strategies to doctor-patient
communication to study the collaborative thinking of the doctor and patients (Aronsson
& Sätterlund-Larsson, 1987). The other study focuses on the politeness and coherence
in pediatric discourse to see how discourse is continuous negotiated between
participants (Aronsson & Rundström, 1989). The politeness model proposed by Brown
and Levinson’s (1978) is universal and with examples from different societies and
cultures. But when under the specific cultural and social context, will participant’s
politeness strategies be affected? Especially when the participants in medical context
are with great power asymmetry, their communication is more complex because of the
social factors. Thus, we conduct our study in one medical center to understand the
communication the discourse between doctor, patient, and patient’s family companion
in order to understand the politeness strategies they used when making requests or
demand or showing medical preferences in the medical decision-making. Three
politeness strategies are mainly discussed in our study: (1) bald recommendations, (2)
collaborative plural, and (3) hedges. The process of how communication between doctor
and patient parties is negotiated and co-constructed is studied under politeness within
the social and cultural background in Taiwan.
1.1 Motivation
A growing interest in doctor-patient communication has arisen during the past few
decades. Many studies have investigated the communication of medical consultations.
However, the results from those studies have not yet shown the whole picture of
medical communication, probably due to the fact that among interpersonal relationships,
doctor-patient relationship is one of the most complicated ones. The interaction between
doctors and patients involves various power status, and is usually related to vital or
health issues, influenced by emotions and needed cooperation and negotiation (Ong,
1995; Chaitchik, 1992).
The doctor-patient relationship can be categorized into four models: (1) informative
model; (2) interpretive model; (3) deliberative model, and (4) paternalistic model
(Emanuel and Emanuel, 1992). Among these four models, the paternalistic model, also
known as parental or priestly model, is the most prominent one. (Emanuel and Emanuel,
1992; Levine et al., 1992; Beisecker and Beisecker, 1993; Deber, 1994; Coulter, 1997).
The paternalistic model assumes that patients could receive the best medical advice and
treatment decision from doctors to improve their health. This model is based on the
assumption that both doctors and patients have mutual objective criteria for defining the
best outcome. However, the fact is that most patients lack equal medical knowledge to
discuss their health problems with doctors under medical circumstances. (Waitzkin and
Waterman, 1974; Fisher and Groce, 1985).
According to Waitzkin and Waterman (1974), and Henley and Henley (1977),
doctor-patient interactions are social and micro political. Interactions are shaped and
constrained in cultural, structural and institutional features. Furthermore, the two parties
are not equal partners during their interaction since doctors have more medical
knowledge while patients usually do not. During the consultation, doctors are regarded
as the gatekeepers to control the process. This asymmetry leads doctors to take superior
roles while patients are perceived as subordinates.
Due to the disadvantages of the paternalistic model, that is the unequal status
between doctors and patients, patient-centered communication has been emphasized
greatly for decades. Patient-centered communication provides an environment for
patients to fully express their symptoms, feelings, concerns, and expectations during
consultation (Henbest and Stewart, 1989; Smith and Hoppe, 1991; Roter et al., 1988).
The main idea of the patient-centered method is “to follow patient’s leads, to understand
patient’s experiences from their point of view” (Weston et al, 1989), allowing the
doctor-patient relationship to become more equal and egalitarian. In addition, their
relationship would be empathic. This means that doctors would elicit patients’ feelings
and respond accordingly, remain silent to show support, listen carefully and try to
understand what they are unable to express, and provide support orally as well as
nonverbally (Lovett and Abou-Saleh, 1990; DiMatteo et al., 1980). In fact,
patient-centered communication is shown to have improved patients’ health (both
physically and mentally) and have increased the efficacy of health care and compliance
(Oates et al., 2000; Stewart, 2001; Epstein et al, 2005). The health care providers
nowadays try to follow the principles of patient-centered care in order to create a better
relationship with patients.
1.2 Research Questions
Previous studies in medical discourse mainly examine through turn-allocation
constraints to analyze doctors’ and patients’ participation (talking frequently or raising
questions) or through conversational constraints to study institutional authority. The
present study aims to examine the communication in medical consultations through
politeness constraints. In order to understand how communication is negotiated and
co-constructed under the asymmetry between doctors and patients in an institutional
authority structure, the research questions are:
1. What linguistic strategies are used in the negotiation of doctor-patient medical
decision-making to save each other’s faces?
2. In the triadic medical consultations, what linguistic strategies do the three parties
apply in medical decision-making process while saving each other’s faces?
1.3 Organization of the Thesis
The rest of the paper is structured as follows: Chapter 2 provides a quick review of
the related studies and basic ideas of medical communication, politeness, and power.
Chapter 3 contains the methodology used in this study, how the data is collected and
transcribed, the theoretical background and the analytical framework. In Chapter 4,
there are data and analyses of the politeness strategies used between two parties and
three parties during the medical consultation. The idea of politeness drawn from
Brown and Levinson’s (1987) politeness model. The main focuses are three politeness
strategies: (1) bald recommendations, (2) collaborative plural, and (3) hedges. Some of
the politeness strategies used by the participants are also discussed in the excerpts of the
consultations. Finally, Chapter 5 summarizes the major findings in the study and
provides suggestions for future studies.
Chapter 2. Literature Review
The study of language and doctor-patient relationship has drawn wide attention and
interests from cross-disciplinary researchers. Medical discourse provides insightful data
for us to understand the role of language in doctor-patient communication. It offers
first-hand data for analyzing the functional meaning of the utterances in medical
encounters since language is regarded as the vehicle of meaning. Medical encounters
are ideal for understanding institutional talk by investigating the imbalance of power
between doctors and patients and the outcome of their talk. In this chapter, we will
discuss previous studies related to sequential phases of medical consultation, medical
decision-making (mutual persuasion process), the power asymmetry between doctors
and patients, and how medical discourse is shaped by politeness.
2.1 Doctor-patient Communication
Medical consultation is one of the institutional talks that is ritualized and can be
studied by its fundamental organization – sequential phases (Helman, 1984). The
consultation is suggested to be composed of six phases: (1) relating to the patient, (2)
discovering the reason for attendance, (3) conducting a verbal and/or physical
examination, (4) considering the patient’s condition, (5) detailing treatment or further
investigation, and (6) termination (Byrne and Long, 1976; Waitzkin, 1991, Heath, 1992).
Ten Have (1989) generates a general ‘ideal sequence’ for the consultation which brings
together the three dimensions of medical consultations: sequential phase, its discourse
genre, and major speech activities. The sequence contains 6 phases: (1) opening, (2)
complaint, (3) examination or test, (4) diagnosis, (5) treatment or advice, and (6)
closing.
The cases of the study in the NTUH ophthalmology department mostly follow the
6 phases. The time period from (1) opening to (3) examination phase is relatively short.
The doctor and the patients spend more time discussing about (4) diagnosis and (5)
medical treatments. Sometimes, when the patient is still being examined (facing an
ocular slit lamp), the doctor gives the diagnosis and they start to discuss about the
causes of the disease or further treatments.
Doctor-patient communication can be regarded as the process of mutual persuasion.
The study of persuasion could be traced back to ancient Greece, where the term
“rhetoric” was used (Brake, 1969; McKeon, 2009). It is the process of adopting a series
of symbols to induce cooperation (Brock, Scott, & Chesebro, 1989). Rhetoric is also
defined as people persuading each other to make free choices (Hunt, 1955), and the
process of persuasion through rhetoric view is conveyed by discourse. One’s utterances
carry the information that would influence the other’s decision. In doctor-patient
communication, the persuasion is mutual. Doctors provide information to influence
patients’ decision-making. At the same time, patients also try to influence doctors’
medical choices for them, because they may want to have certain prescription or
medical treatment. In other words, medical communication is a persuasive process that
both doctors and patients are involved in and take the roles of persuader and persuadee
(Smith and Pettegrew, 1986). The mutual persuasion between doctors and patients
demonstrates the shared and negotiated decision-making.
Though decision-making is negotiated by doctors and patients, doctor-patient
communication is mainly doctor-initiated. During consultation, doctors actively ask
patients’ symptoms and prescribe medications for them. And because of their unequal
medical knowledge, patients could only understand their disease through doctors’
judgment and explanation. Doctors are regarded as the one with authority and power. In
fact, the study of power and domination and effective communication in medical
encounters has been emphasized greatly since the 1960s (Lupton, 1995). The power
doctors have during consultation was regarded as the aid to assist patients to make
better medical choices and gain compliance. Doctors were expected to not only listen to
patients but also to avoid the communicative gaps or obstacles during communication.
But the doctor-patient communication is in fact a process of mutual persuasion; though
with less medical knowledge, patients strive to “equalize the balance of power or gain
and maintain control over aspects of their healthcare” (Beisecker, 1990). When in
patients’ expertise (symptoms, preferences, concerns), they should take responsibility of
their health condition, and be encouraged to ask questions or be able to choose or refuse
different medical treatments. Hence, the patient is “empowered” during consultation
(Lupton, 1995).
2.2 Politeness
Brown and Levinson (1978) proposed a general model of politeness and showed
how discourse is shaped by politeness in different cultures and societies. The idea of
“face” from Goffman (1967) claims that people’s interaction is the cooperation of
maintaining each other’s face. From their point of view, everyday discourse contains
many face-threatening acts (FTAs) like critiques and requests. From Brown and
Levinson’s (1978) definition, the face is separated into (1) negative face: the want to be
unimpeded by others, and (2) positive face: the want to be desirable and close to others.
There are two distinctions of FTAs. The first one distinguishes acts that threaten the
hearer’s negative or positive face. Acts that threaten the hearer’s negative face are those
in which the speaker impedes the hearer’s action, such as: requests, suggestions,
promises (e.g. the speaker commits a future action that benefits the hearer, and the
hearer is under pressure to accept or reject it) and compliments (e.g. the speaker shows
desire in the hearer’s possession, so the hearer might feel like he has to give it to the
speaker), etc. Conversely, acts that threaten the hearer’s positive face are those in which
the speaker disregards the hearer’s wants, like: criticism, complaints, and disagreements.
However, there may also be an overlap in the distinctions of FTAs because some of
them threaten both the negative and the positive face, such as complaints and
interruptions. The second distinction focuses on acts that threaten the speaker’s negative
or positive faces. Because the speaker and the hearer work together to maintain each
other’s faces, the acts in the second distinction may threaten the hearer’s face as well.
Acts which threaten the speaker’s negative face include: expressing thanks (make
humble the speaker’s own face), acceptance of offers (the speaker is indebted and
threatens the hearer’s negative face), and making unwilling promises and offers (the
speaker is against his own will to commit to future actions, and it threatens the hearer’s
positive face if the speaker’s unwillingness is perceived). Other acts that threaten the
speaker’s positive face are: apologies (the speaker regrets doing an FTA), acceptance of
a compliment (the speaker may have to be humble or compliment the hearer in return),
and confession of guilt or responsibility.
In Brown and Levinson’s (1978) model, the possible strategies for doing FTAs are
proposed (See Figure 1). If a speaker goes on record, his action and communicative
intention are clear to the participants. For example, if a speaker says, “I promise to
come tomorrow” and all the participants have the idea that the speaker clearly commits
himself to be here tomorrow, this unambiguous intention is considered as “on-record”.
On the other hand, off record is when the speaker’s communicative act has more than
one intention. An example provided by Brown and Levinson (1987) is “Damn, I’m out
of cash, I forgot to go to the bank today” (Brown & Levinson, 1987:316). The speaker’s
intention is not clear here; He may want to borrow some money from the hearer or is
just plainly stating that he has run out of money. Off-record strategies contain metaphor,
irony, and rhetorical questions, etc. which causes the speaker’s intention to be
ambiguous.
Figure 1. Possible strategies for doing FTAs
When a speaker does a communicative act baldly without redress, it is direct and
unambiguous. For example, a request is bald if the speaker says, “Turn on the light!” In
Brown and Levinson’s (1978) analysis, an FTA done by a speaker without redress is
categorized into one of the following three conditions; the first condition is that both the
speaker and the hearer agree that the need to maintain face can be postponed due to
urgency. The second condition is when the degree of threat to the hearer’s face is very
small and the speaker does not need to sacrifice much, such as “Do sit down.” The final
condition is when the speaker has great power over the hearer, or can get support from
the audience to damage the hearer’s face but not his own.
Brown and Levinson (1978) define actions that “give face” to the hearer as
redressive actions in which an FTA is not intended or wanted. When the speaker
performs a redressive action, the hearer’s face is acknowledged and the speaker will try
to maintain the hearer’s face wants. There are two kinds of redressive actions – positive
redressive action and negative redressive action. A positive redressive action focuses on
the hearer’s positive face, and to a certain degree, the speaker is concerned with the
hearer’s wants. So the speaker may treat the hearer as his friend or an in-group. An FTA
is minimized because the speaker sympathizes with the hearer and tries to appeal to the
hearer’s positive face. On the contrary, negative redressive actions satisfy the hearer’s
negative face or his desire to maintain self-determination. Negative politeness strategies
are applied when the speaker acknowledges and respects the hearer’s negative face and
avoids to impede the hearer’s action.
Brown and Levinson considered the sociological variables which determine the
seriousness of a face-threatening act (FTA). There are three factors: (1) the ‘social
distance’ (D) (familiarity between S and H, a symmetric relation), (2) the relative
‘power (P) of S and H (an asymmetric relation), and (3) the absolute ranking (R) of
impositions in a particular culture (Brown and Levinson, 1978). (Brown and Levinson
even propose a formula for calculating the weightiness of an FTA, using “D,” “P,” and
“R” as variables. However, the weightiness is not our focus so we do not put emphasis
on it.) According to their definition, the seriousness of an FTA contains both risk to a
speaker’s face and risk to a hearer’s face depending on the type of the FTA. For
example, requests and offers tend to threaten both parties’ faces, while apologies
threaten a speaker’s face, and advice and orders typically threaten a hearer’s face. While
Brown and Levinson’s politeness model is not specific for doctor-patient
communication, the model can help provide an explanation for the facework between
doctors and patients under politeness constraints. According to the politeness model,
language is regarded as social practice and the means to negotiate. Though in Brown
and Levinson’s (1978) examples, the utterances they analyzed were collected from
different dialogues that were difficult to present the diversity of certain social
interactions.
Though the politeness model is not specialized for doctor-patient communication,
it provides the possibility to examine their communication under the politeness domain.
In fact, during consultation, doctors would raise questions and come up with
recommendations which may threaten patients’ face. On the other hand, when facing
doctors who have authority and power in an institutional structure, any active acts from
patients could be regarded as face threats (Aronsson and Sätterlund-Larsson, 1987).
During consultation, doctors sometimes raise questions that might threaten patients’
faces or give recommendations with implied criticisms. Aronsson and
Satterlund-Larsson (1987) investigated the dialogue between doctors, adult patients and
their family. They discovered that politeness and clarity may not always be satisfied at
the same time because doctors’ most face-threatening acts were softened by indirectness.
For instance, when a patient needs to get undressed for examination, the doctor might
say, “You could perhaps undress a little and then we’ll examine your thighs…” In this
request, the doctor softens the request through negative politeness by being
conventionally indirect, using hedges, and minimizing the level of imposition. On the
other hand, the request can also be applied through positive strategies like using the
plural form to imply collaboration. These strategies softened the face-threatening degree
of the doctor’s request but may be less clear. So in Aronsson and Satterlund-Larsson’s
study, after the doctor’s request, some of the patients were not certain with regards to
how much clothing they should take off or if they needed to get undressed at all.
2.3 Power
Doctor-patient relationship involves power relationship. Tannen (1987) suggests
that power is always metaphoric when related to interaction and discourse. That is
because there are different kinds of power and people take different roles. Between
doctors and patients, power determines their asymmetrical relationship; doctors take the
dominant role while patient the subordinate, which leads to an imbalanced status
(Tannen, 1994). Thus, under doctor-patient relationships, doctors could exercise power
to inform patients according to their medical knowledge and even persuade them to
accept their advice (Burgoon et al., 1990; Ryn, 1997). According to Kettunen and
Gerlander (2002), from the view of doctor-centered paternalistic, power is shown during
the health care process “by using jargon, dictating the topics, disregarding the patient’s
initiative, interrupting, questioning, and controlling the time” (Fisher and Groce, 1990;
Jarrett and Payne, 1995; Cegala, 1997; Chapple and May, 1997; Binbin, 1999; von
Friederichs-Fitzwater and Gilgun, 2001). However, in interpersonal communication,
power and solidarity at the same time, depending on the context (Tannen, 1994).
From the traditional paternalistic view, patients are regarded as the passive ones to
receive information with few questions or requests. They are not actively involved in
communication, and do not express the need for more information or show and clarify
their confusion (DiMatteo, 1991; Binbin, 1999; Lambert et al., 1997). On the other hand,
according to a study by Ainsworth-Vaughn (1995), though with different power statuses,
doctors and patients use the same power strategies but in different ways. For example,
doctors tend to ask direct questions while patients ask questions in a more indirect or
polite way. Moreover, patients are gentle while asking questions in order not to threaten
doctors’ domain. Thus, their questions would contain short pauses. During consultation,
patients would keep bringing up the questions or problems to continue the topic actively
or propose treatment options by themselves. (Ainsworth-Vaughn, 1995). Thus, power is
performed through individual action and interaction within the sequential organization,
not rooted in the characteristic or role of doctor and patient. During negotiation, doctors
and patients work together to build authority and power.
The medical consultations we collected are examined under the doctor and
patient’s asymmetry power status and different politeness strategies while they strike to
achieve their communicative goals. In Chapter 3, the methodology of conducting the
study is presented.
Chapter 3. Methodology
In this study, the talk exchange between doctor and patient parties in 45 medical
encounters in an ophthalmology clinic in National Taiwan University Hospital (NTUH)
were observed and analyzed. The age of the recruited patients ranged from 45 to 85
years. There were in total 45 patients (16 male, 29 female) and 6 family companions
included in our study. The family members who accompanied the patients were 2 wives,
1 husband, 2 daughters, and 1 son. The study was approved by the Institutional Review
Board (IRB) of National Taiwan University Hospital (NTUH) with the number:
201612117RINB. Our study was conducted according to the rules of IRB and the
participants’ right was fully protected by the researcher. If the patients or their family
companions were under 20 years old, they were excluded from the study because
according to the rules of IRB, they are vulnerable subjects who need extra-protection if
they are included in the study.
Because these patients’ eye conditions were chronic (the process of the disease is
over a period of time, such as cataract, glaucoma, age-related macular degeneration
AMD, etc.) but not urgent in nature, most of the patients visited the ophthalmologist on
a regular basis for three months, six months, to one year or so depending on the
condition of their eyes. Therefore most of the patients and their companions in the study
were well-acquainted with the doctor. Only 4 consultations were first-time visits and
most of them were referred by other specialists from other hospitals. The
ophthalmologist in our study is an expert in the retina-related field. The average number
of patients in each clinic session is around 90. There are many patients who live outside
the metropolitan areas of Taipei and would spend hours traveling just to see this doctor
at the National Taiwan University Hospital. Operating hours are in the morning or in the
afternoon. In the morning, the clinic begins at 9AM and ends around 2PM; in the
afternoon, it begins at 1:30PM and ends around 6PM. The average time for each
consultation is around 4 minutes. The Ophthalmology Department belongs to the
Surgical Department and ophthalmologists can diagnose the disease directly from the
patient’s eyes when their pupils are dilated (unlike interns who can only diagnose from
the patient’s description of symptoms or conduct basic examinations, and are unable to
perform any surgical treatment.)
3.1 Data Collection
In order to have a better view on the doctor-patient communication in Taiwan, the
face-to-face consultation between doctors and patients were investigated. The patients
and their families were invited to participate in this study by 1 doctor in the eye clinic
prior to their consultation. The goal and method of the study were explained by the
doctor. If the patient and their companion agreed to join this study, the entire
consultation would be recorded and later transcribed. The patients’ identities would be
delinked and their identities would not be revealed. The data collected could only be
used for academic purposes.
With regards to the setup of the clinic, patients were asked to sit on a chair near the
doctor for the examination while an ocular slit lamp was on the other chair. Usually,
there were two nurses in the clinic. One would face the table with a computer while
working on patients’ appointments and scheduling upcoming examinations. The other
would stand next to the door to help with the flow of patients going in and out of the
clinic, instructing the patients to sit on the right seats (facing the doctor or in front of the
ocular slit lamp) and give them the prescription sheet.
During the consultations, as a researcher, I sat on the chair farthest from the door
and behind the doctor, observing the entire sessions without interfering. When the
doctor invited the patients and their families to join the study and have them sign the
informed consent, I would start to record the consultation and later transcribe the
conversation.
3.2 Theoretical Background
The data in our study is transcribed and examined qualitatively under concepts of
Discourse Analysis (DA). “The main strength of the DA approach is that it promises to
integrate linguistic findings about intra-sentential organization with discourse structure.”
(Levinson, 1983:287). Discourse analysis is the study of language in context that
develops from linguistic studies and semiotics (Potter & Wetherell, 1987; Edwards &
Potter, 1992; Starks & Brown Trinidad, 2007). It focuses on language-in-use and
examines how participants achieve personal, social, and political communicative goals
through language (Tannen et al., 2015). From the viewpoint of discourse analysis,
language and words are basically meaningless but are a system of signs and meaning
that is generated through the shared and mutually agreed-on use of language (Starks &
Brown Trinidad, 2007). Human beings’ understanding and perception of reality is
constructed by language. In addition, language defines people’s social roles and they
means of our communication, discourse analysis examines how language shape and
reflect cultural, social, and political activities (Crowe, 1998; Gee, 2014).
Health communication provides a chance to study the relation between discourse
and healthcare. “Discourse” here is defined as “‘contextually sensitive written and
spoken language produced as part of the interaction between speakers and hearers and
writers and readers” (Candlin et al., 1999:321). For many linguists, language is
perceived not simply a reflection of relations in social life, but it actively contribute to
the construction and constitution (Kress, 1988; Fairclough, 1992; Candlin et al., 1999).
In healthcare and health communication, language plays a very important role in the
medical settings and discourse is the core of healthcare that reflects the communication
and patient satisfaction (Harvey & Adolphs, 2012).
3.3 Analytical Framework
The purpose of our study is to understand how linguistic strategies are used by the
participants in the decision-making process while saving each other’s faces during the
medical encounters. The linguistics cues are then compared with the politeness model
and show how the communication is negotiated and co-constructed by the participants
in institutional context. Because medical discourse is complex and influenced by the
participants’ social roles, the use of politeness strategies to save the participants’ faces
is marked. The cases of this study contain medical discourse between two parties
(doctor and patient) and three parties (doctor, patient, and companion).
First, we go through the transcription and pay attention to the decision-making
process between the doctor and patients. The linguistic strategies corresponding to the
distinction of Brown and Levinson’s (1978) politeness model are marked. Later, we
select three politeness strategies that used by the participants in both two parties and
three parties communication: (1) bald recommendations, (2) collaborative plural, and (3)
hedges. The three strategies are the main focuses of the analysis but because the
communication is dynamic, the excerpts are studied sequentially. The context of the
discourse plays a very important role in medical encounters. Though Brown and
Levinson (1978) proposed clear divisions of politeness strategies, the real application of
politeness by the participants in our study is influenced by specific social and cultural
factors. Some more detailed analysis of the three strategies is in Chapter 4.
3.4 Data Transcription
The dialogues between doctor, patients, and companions were tape-recorded and
transcribed in extenso. We listened to the conversation for each consultation and
checked the transcript many times to make sure the transcription can reveal the details
of the verbal communication between the participants. We focus on the politeness
strategies that the doctor and patient party use during the medical consultations and
draw the concepts from Discourse Analysis. The transcription contains the features
related to the possible politeness strategies appear in their consultations, so the
speaker’s emphasis, overlaps, and code-switching are marked but not other minor
linguistic features. (The transcription convention is in page iv.)1 In the transcription, the
participants’ names or addresses are fictionalized to protect their anonymity.
1[ ] Beginning and ending of overlap in speakers’ utterances
? Upward intonation
CAPITALS Relatively high amplitude (in Mandarin transcription: bold)
/ / Encloses description of how talk is delivered
_____ Code-switching (e.g. Taiwanese)
= Latching
.. Short pause
… Long pause
[…] Text omission
Chapter 4. Politeness Strategies in Medical Communication
This chapter presents the data and analyses of the politeness strategies used by two
role combinations during the medical consultations – two parties (doctor and patients)
and three parties (doctor, patient, and companion). The linguistic strategies they use
may threaten or save the hearer or the speaker’s faces depending on their
communicative goals. Most of the studies related to medical communication only focus
on two parties. When three parties are involved, the medical encounters are much more
complex and difficult to analyze not only because the dialogue is more complicated but
because the participants are constrained and influenced by others’ social power and
status. We select three politeness strategies that appear in both the consultations of two
parties and three parties in their medical decision-making to see how linguistic
strategies are applied when they seek to achieve their communicative goals while saving
each other’s faces. The results support that doctor-patient communication is a complex
process that is negotiated and co-constructed by the participants while they are under
power asymmetry in an institutional authority structure.
Nowadays, medical decision-making is often negotiated by both doctors and
negotiation is a process of mutual persuasion. In medical consultations, doctors give
recommendations and advices while patients make requests or express their preferences
for medical treatments. These communicative acts are regarded as face-threatening acts
in medical communication. Examples in this chapter are excerpts from the dialogues
between doctor, patients, and family companions to demonstrate how the two parties
and three parties save each other’s faces while achieving their respective
communicative goals with a power imbalance.
4.1 Strategies in Dyadic Interaction
In Brown and Levinson’s (1978) politeness model, the possible strategies for
performing FTAs are categorized and explained. When the speaker is performing an
on-record FTA with positive politeness strategies, he tries to maintain the hearer’s
positive face and considers himself to be in the same group with the hearer and thus the
face-threatening degree decreases. Some positive politeness strategies are: seeking
agreement, avoiding disagreement, and giving reasons, etc. In addition, if the speaker
includes both the hearer and himself in the activity equally, it is a positive politeness
strategy. For example, the requests may contain in-group identity markers, such as “we”
or “Let’s do something together.” On the other hand, when performing on-record FTAs
with negative politeness, the speaker shows respect or deference to the hearer and
maintains the hearer’s negative face by caring about his need to be unimpeded. Some
possible negative politeness strategies are: using questions or hedges, apologizing,
avoiding using pronouns, etc. In our study, we focus on three particular strategies used
in dyadic and triadic communication: bald recommendations, collaborative plural, and
hedges. These strategies are mainly used when the doctor and patients are discussing
about the diagnosis and medical treatments. The doctor provides medical advice while
the patients request their preferred treatment and asks questions. Taking into account the
circumstances during medical consultation, such as building rapport under limited time
and the asymmetry of power and medical authority, the politeness strategies applied by
the participants is able to reveal the interest of medical communication.
4.1.1 Bald Recommendations
The bald on-record strategy is most direct and unambiguous politeness strategy;
for example, the demand “Wash your hands” is a bald act (Brown & Levinson, 1978). A
bald act can be done when the speaker is not afraid of the hearer, the speaker has greater
power over the hearer, or when their social distance is close. These conditions are also
seen in the medical consultations.
In our study, the doctor has good communication skills and can usually create and
maintain a harmonious atmosphere in the clinic. Most of the patients visit on a regular
basis so to some degree they are familiar with the doctor. When the doctor gives
medical advice or requests, he usually tries to maintain the patient’s positive or negative
face. However, there are circumstances when the doctor or patients perform an act
baldly and without redress.
In Excerpt 1a, the doctor was surprised when he realized that the patient had the
nutrition supplements that were not scientifically tested. Therefore, he gave the
recommendation that the patient stop taking the supplements and spending money on
them.
Excerpt 1a
The doctor examines the test results on the screen.
1 DOC: 還是有一點點水誒 還是有一點點水
There is still some fluid inside the retina…. There is still some fluid inside your eye.
2 PAT: 又又有水了.. 右右眼?
There is still some fluid a..again… In the right right eye?
3 DOC: 恩..
Mmm..
4 PAT: 右邊有水
5 DOC: 對..
Yes..
6 PAT: 嗯.. 又有水 我之前吃那個幹細胞
Mmm.. there is fluid [in my eye] again. I had stem cells.
7 DOC: 你吃幹細胞?
YOU HAD STEM CELLS?
8 PAT: 恩我吃人人家介紹的
Yes. I did. Someone recommended them.
9 DOC: 阿呀不要浪費那個錢啦
Come on! Don’t waste your money on that!
10 PAT: 那個什麼胎盤 鹿胎盤
That so-called placenta, deer placenta.
11 DOC: 你絕對不要去亂吃 haa 拜託 haa
You should definitely not take any unproven remedies. Please!
12 PAT: 他說可以修復什麼
It is said that it can repair the…
13 DOC: 我絕對不相信那些 不要浪費錢
I absolutely do not believe in them at all. Don’t waste your money.
14 吃了一大堆雜七雜八的東西在身體 好 看正前方
Having those things in your body [may not be good]. OK. Look at the front.
Examination
In this excerpt, we see that there was some fluid in the patient’s right eye and the
problem could not be solved by the medicine or the eye drops. Usually such a problem
wouldn’t be solved until the eye starts absorbing the fluid by itself. The absorption
process might take weeks, months, or even years. The patient visits the doctor regularly
every four or six months and in this particular visit the doctor told him that there was
still some fluid in his right eye. The patient told the doctor that he had been taking stem
cells (Line 6). Hearing that the patient had stem cells which were not scientifically
tested, the doctor was very surprised and raised his voice in Line 7. The patient admitted
and said the practice was recommended by someone else. Starting from Line 9, the
doctor tried to persuade the patient not to take stem cells extracted from deer placenta.
Instead of using other politeness strategies in his recommendation, the doctor gave the
advice baldly to show his disproval. For instance, the doctor said “阿呀不要浪費那個
錢啦Come on! Don’t waste your money on that!” (Line 9) directly to show how much
he disagreed with the patient. This clear and unambiguous request that the patient was
just wasting money on buying unverified supplements was a bald act that threatened the
patient’s face. Usually, the doctor would try to save patient’s faces when he was giving
recommendations so the form of his request was rarely imperative. This time, however,
the doctor was really surprised and he hoped the patient could undergo proper
treatments.
As discussed here, the doctor took a clear stance that he disagreed with the
supplements whose medical effects were without scientific evidence. In Line 11, the
doctor even used “絕對 must not” and “拜託 Please!” to keep the patient from taking the
supplements. “拜託 Please!” in the request form is not commonly used by the doctor in
medical consultation. Sometimes, when one party used “Please!” as a request for the
other party, usually it is from the one with less power or between intimates. In this
example, “Please!” from the doctor was similar in tone to “Please do me a favor! Don’t
take those supplements which may not be good for your health!” The doctor treated his
conversation partner not only as a patient but like a friend. The use of “阿呀 Come on”
and “拜託 Please” shows the doctor and the patient have close social distance. And the
doctor can frankly express his genuine opinions. Otherwise, the doctor could just say
“Oh, if I were you I would think twice before I took stem cells.” Or “I do not consider
taking stem cells good for your eyes.”
However, the patient was not convinced by the doctor and he believed that the
supplements may have special curing effects. In Line 12, the patient tried to persuade
the doctor that the supplements were said to have curing effects, like repairing the cells
or the human body. The doctor immediately replied “我絕對不相信那些 不要浪費錢 I
absolutely do not believe in them at all. Don’t waste your money.” (Line 13) The doctor
strongly disagreed with the patient taking stem cells by using negation (don’t) and
intensifier (at all) and repeating “don’t waste the money” one more time. (The first time
the doctor told the patient not to waste money on the supplements is in Line 9.) Because
the stem cell extracts were not the supplements on prescription and not covered by
health insurance, the doctor kept saying “don’t waste the money” and that he personally
didn’t believe in the curing effect of the stem cells extracts. The idea of not wasting the
money is something beneficial to the patient. And the doctor did not want the patient to
waste his money on the extracts showing that the doctor cared for the patient.
In fact, during the consultation, the doctor’s recommendations were rarely bald
according to the politeness model. In most cases, the doctor tried to maintain the
patient’s faces when giving advice or making requests. This example of bald
recommendation here and the use of “阿呀 Come on” and “拜託 Please” showed the
intimacy between the doctor and the patient. Only when the doctor and the patient were
close enough, would their consultation contain these expressions. However, even
though the doctor showed his strong disapproval of the extraction, the patient still
seemed to believe in its curing effect near the end of their consultation.
Excerpt 1b
1 PAT: 沒有 那這邊要開眼藥水嗎 藥還沒用完
No. Then will [you] prescribe eye drops? There are still some left.
2 DOC: 好吧 那我看多久再幫你追蹤 半年再看好了 厚
Alright. Then I’ll see when your next appointment should be. Let’s meet
3 PAT: 好 OK.
4 DOC: 厚 半年 讓自己放輕鬆來 生活正常 不要熬夜 厚
OK. Half a year. Relax yourself. Have a regular lifestyle. Don’t stay up late. OK.
5 PAT: 鹿胎盤 他說什麼可以吃 修復身體
About the deer placenta. They said that it can repair the body.
6 DOC: 我從來都不相信這些 你就能吃能睡 頂多就吃一些什麼 什麼葉黃 素這樣
I never believe in those kinds of things at all. You just eat well and sleep well. Or at most try something like lutein.
7 PAT: 他說可以修復身體一下
They said I could try to repair my body.
8 DOC: 嘻嘻嘻
Hehehe /laughing/
9 PAT: 癌症都可以修復
That even cancer can be cured.
10 DOC: 世界上有這種藥的話 那就 就天下太平了 不用不用有這些醫生了 厚
If such kind of medicine exists, everything will be fine and all at peace.
No need to go to the doctors. Ok.
11 好 那就半年再追蹤 好不好 厚 好自己那個厚=
Alright. Then the follow-up will be in half a year. Is that ok? Ok. Ok you take care ok=
12 PAT: =半年 =half a year
13 DOC: 對 可以嗎? 還是 還是要四個月?
Yes. Ok? Or or four months?
14 PAT: 好半年可以
Ok half a year is fine.
15 DOC: 好 半年 Ok half a year.
In Line 4, after the doctor and the patient agreed for next follow-up, the doctor
gave the advice about having a regular lifestyle. But the patient mentioned the deer
placenta extract again and insisted that it can repair the body (Line 5). The doctor
restated his disagreement to oppose the patient directly in Line 6. (In excerpt 1a, the
doctor said “我絕對不相信那些 不要浪費錢 I absolutely do not believe in them at all.
Don’t waste your money.”) Here, he asserted that as a doctor he didn’t believe in the
curing effects of the placenta extract and emphasized by “從來 never”, which implied
that the patient should not believe in it either. In addition, the doctor gave some advice
about living a regular lifestyle. The doctor believed that the nutrition supplement that
the patient could take was lutein, which is already proven scientifically to improve
vision and eye health. But the patient was not convinced; besides Line 5, he mentioned
in Line 7 and 9 that the stem cells extracts can repair cells and even cure those with
cancer. The doctor found that the patient was not convinced due to his lack of medical
knowledge and couldn’t help but laugh (Line 8). However, instead of criticizing the
patient directly and threatening his positive face, the doctor replied indirectly and wisely
by saying “世界上有這種藥的話 那就 就天下太平了 不用不用有這些醫生了 厚
If such kind of medicine exists, everything will be fine and all at peace. No need to go
to the doctors. Ok.” (Line 9). The doctor was trying to tell the patient that there was no
such miracle elixir otherwise there would be no need for doctors. If that kind of
medicine really existed, people would only need to take the miracle elixir to cure all
diseases, since the patient claimed that even cancer could be cured by the extract. The
doctor used “厚 Ok” at the end of the sentence to seek the patient’s consent to end the
conversation. Without waiting for the patient’s response, the doctor shifted the topic
back to the follow-up appointment discussed earlier in Line 2 and 3. What is interesting
here is that when the patient repeated “半年 half a year” after the doctor in Line 12, the
doctor asked a yes/no question “可以嗎?Ok?” to seek for the patient’s agreement and
even provided an option. Usually, the follow-up is decided by the doctor because only
he knew the condition of the patient’s eyes and when the patient needed to come back
for the next examination. Most of the patients would simply agree or mention the date
which they would be available. But here the doctor provided the options of the next
follow-up for either 4 or 6 months later for the patient to make the final decision. In
Line 14, the patient made his choice and replied that half a year is fine. At the end, the
doctor confirmed by saying “yes” by repeating “half a year”.
The doctor involved the patient in the decision-making by using positive politeness