Case Report
Supratentorial solitary fibrous tumor / hemangiopericytoma in a 31-year-old man: A case report
Cho-Shun Li
1, 2, 3, Jeng-Dong Hsu
4, 5, Yu-Ting Wang
4, 5, 6, Wea-Lung Lin
4*, 51 School of Medicine, Chung-Shan Medical University
2 Department of Medical Education, Chung Shan Medical University Hospital
3 Department of Neurosurgery, Chung Shan Medical University Hospital
4 Department of Pathology, Chung Shan Medical University Hospital
5 Department of Pathology, Chung Shan Medical University
6 Institute of Medicine, Chung Shan Medical University
Introduction
Haemangiopericytoma (HPC) is a rare vascular mesenchymal neoplasm arising from the pericytes of Zimmerman, which are leiomyoblastic cells that spiral around capillaries and postcapillary venules (1,2). Extracranial HPC was first reported by Stout and Murray in 1942 (3). In 2007, HPCs were classified by the World Health Organization (WHO) as grade II neoplasms or, in the presence of anaplastic elements, grade III neoplasms (4,5).
Intracranial HPC comprises approximately 0.4% of all primary central nervous system (CNS) tumors (4,6), is more commonly located supratentorially, and tends to occur in younger patients, with average
age at presentation 38–42 years (7,8). Depending on the location of the lesion, symptoms commonly include seizure, headache, visual dysfunction, and motor weakness. Intracranial HPC has a strong tendency for local recurrence and extracranial metastases (9). The aim of this study was to emphasize the effectiveness of total tumor resection and adjuvant radiotherapy in achieving a maximal period free from recurrence.
Case report
A 31-year-old male was admitted to our hospital after presenting with sudden seizure. This patient had no personal or family history of seizures.
Over the previous three months, he had exprienced weakness and numbness in the right lower limb with progressive difficultywalking, without history of trauma or fever. Neurological examination revealed decreased power in the right lower limb (grade 3), with no obvious muscle atrophy.
* Correspondence Author: Wea-Lung Lin
Department of Pathology, Chung Shan Medical University Hospital, No. 110, Section 1, Chien-Kuo N. Road, Tel: +886-4-36009595
Fax: +886-4-24753987 E-mail: [email protected]
Intracranial haemangiopericytoma (HPC) is a rare vascular tumor, accounting for less than 1% of all primary central nervous system tumors. HPC closely mimics meningiomas in clinical and radiological features . However, it tends to occur in younger patients, with average age at presentation 38-42 years.
We report a rare case of histopathologically diagnosed HPC of the left frontal lobe in a 31-year-old man.
Craniotomy with gross total removal (GTR; Simpson grade 1 excision) of the mass was performed.
Postoperative radiotherapy was administered. We describe the clinical, radiological, and histological features of this tumor and its outcomes upon completion of treatment and 18 months of follow-up.
Keywords: haemangiopericytoma, surgery, TomoTherapy
Cranial computed tomography (CT) and magnetic resonance imaging (MRI) revealed a left frontal solid multi-cystic mass lesion measuring 6x6x5 cm (Figures 1 A-C).
Left frontal craniotomy with gross total removal (GTR; Simpson grade I excision) of the mass was performed with intraoperative monitoring (IOM) (Figure 1 D-F). During surgery, the mass grossly mimicked a hyper-vascular cystic meningioma and bled easily.
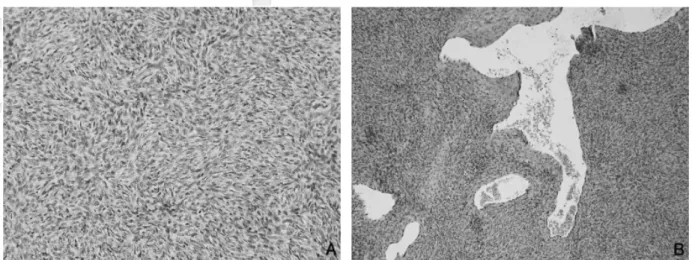
Microscopically, hematoxylin and eosin stain showed a patternless architecture with predominant hypercellular areas composed of closely apposed round-ovoid to spindle cells with scant cytoplasm.
Thin-walled, branching, staghorn-shaped vessels were also evident (Fig. 2 A, B). No necrosis was identified in prepared sections. Mitotic activity was 9 mitoses/10 HPF (high power fields). On immunohistochemical (IHC) analysis, EMA and PR were negative, while CD 34 was positive in vascular channels (Fig. 3A) and STAT6 (Signal Transducer and Activator of Transcription 6) was present in tumor cells (Fig. 3B). Ki-67 proliferative index was 10% (Fig. 3C). Light microscopic findings and IHC study confirmed the diagnosis of solitary fibrous tumor/HPC, WHO grade III.
This patient was treated postoperatively with adjuvant TomoTherapy with accumulated dose of 56 Gy in 30 fractions. Two years after treatment, Fig. 1 Magnetic resonance images show dural-based enhanced mass in the left frontal parasagittal convexity.
A-C: Axial (A), coronal (B), and sagittal (C) images show a round solid multi-cystic mass measuring 6x6x5 cm in the left convexity. D-F: Postoperative two-month axial (D), coronal (E), and sagittal (F) images show gross removal of the tumor.
the patient is disease free without any evidence of
local recurrence or distant extracranial metastases.
Discussion
Behavior:Fig. 2 Diffuse proliferation of polygonal and spindle tumor cells with round or ovoid nuclei (A). Thin-walled, branching, staghorn-shaped vessels (B).
Fig. 3 IHC study revealed CD 34 positivity in vascular channel (A) and STAT6 in tumor cells (B). EMA immunostain is negative (C). Ki-67 proliferative index is 10% (D).
Intracranial HPC is a rare neoplasm, but has a rather high rate of local recurrence. It is also a major brain tumor with the potential for extracranial metastasis. Even after complete removal, late local recurrence and distant extraneural metastases have been reported in 12% to 57% of cases. The mean survival is 84 months from diagnosis. (10,11).
Most primary brain tumors, such as glioma and meningioma, rarely exhibit extracranial metastasis, although malignant. However, the majority of intracranial HPCs eventually metastasize.
Imaging:
On imaging, most intracranial HPCs are supratentorial in distribution, with the most common location in the parasaggital area. Almost all tumors have lobulated margins and appear dense on CT.
HPCs appear with marked contrast enhancement on CT and MRI (12). Some studies have reported that intracranial HPCs are more multi-lobulated than benign meningiomas and have a narrow base of dural attachment on CT-scan and MR images, as in our patient (13,14). In previous studies on intracranial HPCs, the mean age at the time of diagnosis ranged from 38 to 50 years (15). In our case, the age was 31 years.
Histology-immunohistochemistry:
Histopathologically, HPC shows a staghorn- shaped vascular pattern of spindle cells (16). At times, the histopathologic features of HPC and meningioma can overlap. IHC analysis can be helpful in this situation. IHC staining for HPC shows intense reactivity to vimentin but not to epithelial membrane antigen (EMA), unlike meningioma which is positive for vimentin and EMA. CD34 and STAT6 are positive in HPC (17,18). Bcl-2 can be used to differentiate these two entities. CD99 seems to be a good marker for HPC with specificity of about 84%.
Genetic counseling:
Cytogenetic abnormalities have been found in some extracranial HPCs. Most HPCs are near- diploid and breakpoints in 12q13, 12q24, and 19q13 are common, with recurrent t(12;19)(q13;q13) translocations (19,20). Loss of chromosomal
material 10q and de novo chromosomal aberrations on chromosome 8 have also been reported in a case of recurrent infratentorial HPC. (21)
WHO classification:
The WHO classification of intracranial HPC has evolved over the past decades. The 2016 WHO classification of CNS tumors used phenotypic and genotypic parameters in addition to histology to define many tumor entities, formulating a concept for how CNS tumor diagnoses should be structured in the molecular era. In such an updated classification system, HPCs are classified as mesenchymal non-meningothelial tumors combined with solitary fibrous tumors (SFTs), graded I–III (22). It is likely that this nomenclature will further evolve.
Treatment:
Aggressive surgical resection remains the cornerstone of treatment. Adjuvant postoperative radiotherapy is indicated even in patients with completely resected tumor and who have been diagnosed with WHO grade II HPC. Radiation responses are dose dependent, with > 50 Gray (50 Gy–60 Gy) providing superior long-term disease- free survival (23). Chemotherapy has a limited role as reported in clinical series.
Conclusion
GTR is associated with the longest survival outcomes in patients with HPC. Radiation therapy is a recommended modality as adjuvant treatment even after GTR to achieve longer recurrence–free interval and overall survival. Extensive long-term follow up is necessary to rule out local recurrences and late extracranial metastases. Regular routine investigations should include liver function test, kidney function test, chest X-ray, ultrasound examinations of abdomen and pelvis, and radionuclide bone scan.
Acknowledgments
The authors would like to thank Pen-Hua SU, PhD, School of Medicine, Chung Shan Medical
University, Department of Pediatrics, Chung Shan Medical University Hospital, Taichung, Taiwan, for advising us on thegenetics section of this paper.
Conflicts of Interest
The authors have no financial conflicts of interest.
References
1. Muller J, Mealey J Jr. The use of tissue culture in differeniation between angioblastic meningioma and hemangiopericytoma. J Neurosurg 1971;34:341–
348.
2. Brunori A, Delitala A, Oddi G, Chiappetta F.
Recent experience in the management of meningeal hemangiopericytomas. Tumori 1997;83:856–861.
3. Stout AP, Murray MR. Hemangiopericytoma: a vascular tumor featuring Zimmermann's pericyts.
Ann Surg 1942;116(1):26–33.
4. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 2007;114(2):97–109.
5. Kleihues P, Burger PC, Scheithauer BW. The new WHO classification of brain tumours. Brain Pathol 1993;11:255–1268.
6. Tsou H, Wang Y, Yang D, et al. Intra-extracranial hemangiopericytoma: clinical manifestations, histopathological features, diagnosis, treatment and outcomes. Chin Med J 2002 (Taipei);65:314–319.
7. Perry A, Scheithauer BW, Nascimento AG. The immunophenotypic spectrum of meningeal hemangiopericytoma: a comparison with fibrous meningioma and solitary fibrous tumor of meninges. Am J Surg Pathol 1997;21(11):1354–
1360.
8. Liu G, Chen ZY, Ma L, Lou X, Li SJ, Wang YL. Intracranial hemangiopericytoma: MR imaging findings and diagnostic usefulness of minimum ADC values. J Magn Reson Imaging 2013;38(5):1146–1151.
9. Nakada S, Minato H, Takegami T, Kurose N, Ikeda H, Kobayashi M, et al. NAB2-STAT6 fusion gene analysis in two cases of meningeal solitary fibrous tumor/hemangiopericytoma with late distant
metastases. Brain Tumor Pathol Apr 18; 2015.
10. Kumar R, Wani AA: Unusual tumors of the posterior fossa skull base. Skull Base 16:75–
84,2006.
11. Guthrie BL, Ebersold MJ, Scheithauer BW, Shaw EG. Meningeal hemangiopericytoma:
histopathological features, treatment, and long- term follow-up of 44 cases. Neurosurgery 1989;25:514–522.
12. Chiechi MV, Smirniotopoulos JG, Mena H.
Intracranial hemangiopericytomas: MR and CT features. AJNR Am J Neuroradiol 1996;
17(7):1365–1371.
13. Rajaram V, Brat DJ. Anaplastic meningioma versus meningeal hemangiopericytoma: immunohistochemical and genetic markers. Hum Pathol 2004; 35:1413–
1418.
14. Wei G, Kang X, Liu X, Tang X, Li Q, Han J,et al. Intracranial meningeal hemangiopericytoma:
Recurrences at the initial and distant intracranial sites and extraneural metastases to multiple organs. Mol Clin Oncol 2015; 3(4):770–774.
15. Guthrie BL, Ebersold MJ, Scheithauer BW, Shaw EG. Meningeal hemangiopericytoma:
histopathological features, treatment, and long- term follow-up of 44 cases. Neurosurgery 1989;
25:514–522.
16. Han N, Kim H, Min SK, Paek SH, Park CK, Choi SH,et al. Meningeal Solitary Fibrous Tumors with Delayed Extracranial Metastasis. J Pathol Transl Med 2015; 14.
17. Noh SH, Lim JJ, Cho KG. I nt racranial Hemangiopericytomas: A Retrospective Study of 15 Patients with a Special Review of Recurrence.
J Korean Abdollahi et al. 285 Neurosurg Soc 2015; 58(3):211–216.
18. Trabelsi S, Mama N, Chourabi M, Mastouri MH, Ladib M, Popov S, et al. Meningeal Hemangiopericytomas and Meningomas: a Comparative Immunohistochemical and Genetic Study. Asian Pac J Cancer Prev 2015;16(16):6871–
6876.
19. Mandahl N, Orndal C, Heim S, Willen H, Rydholm A, Bauer HC, Mitelman F. Aberrations of chromosome segment 12q13-15 characterize a subgroup of hemangiopericytomas. Cancer
1993;71:3009–3013.
20. Hallen M, Parada LA, Gorunova L, Palsson B, Dictor M, Johansson B. Cytogenetic abnormalities in a hemangiopericytoma of the spleen. Cancer Genet Cytogenet 2002;136:62–65.
21. Heidrun H, Michela L, Peter A, et al. Intracranial hemangiopericytoma: Case study with cytogenetics and genome wide SNP-A analysis. Pathology -
Research and Practice 2011;207:310–316.
22. Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary.
Acta Neuropathol 2016;131:803–20.
23. Bastin KT, Mehta MP. Meningeal hemangiopericytoma:
defining the role for radiation therapy. Neurooncol 1992;14(3):277–287.