Yu Wen Chen ( 陳毓雯)M.D.
Department of Nuclear Medicine, Kaohsiung Medical University
Hospital; Department of Medicine, School of Medicine,
Kaohsiung Medical University, Kaohsiung, Taiwan
Introduction of radiopharmaceutics –
Concept of radiation biology- alpha emitter
History of radiopharmeceutics in Tx of prostate cancer with bone metas.
Concept of bone metastasis- prostate cancer
The phase III clinic trial of Ra 223- NEJM
Comparison with bone seeking
radiopharmaceutics- Sr89, Sm153
Most a combination of
(A) a radioactive molecule, a radionuclide
(放射核種),providing radiation eg. diagnosis (gamma
and X ray) and therapy ( betta and alpha).
(B) a biologically active molecule or drug providing a carrier and determining localization and
biodistribution (生物分佈).
Some radioactive atoms themselves confer the desired
localization properties, eg iodine, gallium, radium etc.
Antoine Henri Becquerel
The Nobel Prize in Physics 1903
• The becquerel (symbol Bq)
(pronounced: 'be-kə-rel) is the SI derived unit of radioactivity.
• 1 Bq is defined as the activity of a quantity of radioactive material in which one nucleus decays per
second.
• The becquerel succeeded the curie (Ci), an older, non-SI unit of
radioactivity based on the activity of 1 gram of radium-226.
1 Ci = 3.7×10
10Bq = 37 GBq 1 μCi = 37,000 Bq = 37 kBq
1 Bq = 2.7×10
−11Ci = 2.7×10
−5µCi
It is impossible to know at what time a certain radioactive nucleus will decay. It is, however possible to determine the probability l of decay in a certain time. In a sample of N nuclei the number of decays per unit time is then:
Rt = -dNt/ dt;
radioactivity: No. of disintegration of a sample of nuclei (atoms) per unit of time
Rt = λ Nt; λ: decay constant
ln 2= 0.693
2 T ln
e N
= N(t)
dt N dN
2 / 1
t - 0
Alpha
Beta
Gamma
X-ray X
Neutron n
E =MC 2
Linear Energy Transfer
LET
8
α radiation consists of helium (
4He) nuclei and is stopped by a sheet of paper or skin
β radiation, consisting of electrons, is halted by an aluminum plate or plastic
γ radiation, consisting of energetic photons, is
attenuated by dense material
Paper
or Skin Aluminum Lead or
Concrete Water or Polyethylene
α β γ
1. Kassis AI. Semin Nucl Med. 2008;38(5):358-366. 2. Brechbiel MW. Dalton Trans. 2007;43:4918- 4928. 3. Nilsson S, et al. Poster 2385 presented at: American Society for Radiation Oncology Annual
Meeting; October 31-November 4, 2010; San Diego, CA.
10-6 10-12
10-9 10-15
10-3
1 second
1 hour 1 day 1 year
100 years 1 ms
100
109 106 103
Energy deposition Excitation/ionization Initial particle tracks
Radical formation
PHYSICAL INTERACTIONS
PHYSICO-CHEMICAL INTERACTIONS
BIOLOGICAL RESPONSE
MEDICAL EFFECTS
Diffusion, chemical reactions Initial DNA damage
DNA breaks / base damage
Repair processes Damage fixation Cell killing
Promotion/completion
Teratogenesis Cancer
Hereditary defects
Proliferation of "damaged" cells Mutations/transformations/aberrations
TIME (sec)
Timing of events leading to radiation effects
Absorbed energy per mass unit
1 Gy (gray) 戈雷=1 J/kg
Harold Gray 1905-1965
H e = w r * D
D: absorbed dose (Gy), w
r: radiation weighting factor (1-20)
H eff =w T *H e
H
e: equivalent dose (Sv), w
T: tissue weighting factor (0.05-0.20)
Unit: 1 Sv (sievert) 西弗
E w T H
T
T
Rolf Sievert (1896-1966)
Radiation types Quality factors
Camma rays and X-rays 1
Electrons, beta particles 1
Neurtons 5-20
Protons 5
Alpha particles 20
Double-strand break(DSB) yield and repair
Traversal required for cell kill (LET)
Cell survival curve
Oxygen effect
Dose rate
Oncogenesis
Bystander effect, and bystander effect in vivo
Fractionation
Radiomodulation
DIRECT ACTION
DIRECT ACTION INDIRECT ACTION INDIRECT ACTION
Relative biological effectiveness
(RBE)
5.78 MeV
6.88 MeV
7.53 MeV
0.45 MeV
6.68 MeV
0.01MeV
0.49 MeV
Of the total decay energy1 93.5% emitted as - particles
< 4% emitted as - particles
< 2% emitted as γ- or x-rays
Measured on standard dose calibrators
PA-27
Role of the osteoclast in bone pathology
Growth factors
Osteoclast activity
Osteolysis Direct bone destruction
Bone Bone secondaries Primary
Local factors Systemic factors
Tumour cells
Bony complications
C
Activated
osteoclast
PA-28
C
Osteolytic bone disease Osteoblastic bone disease
Osteoclast
Osteoblast Unknown
GFs TGF-
Numerous bone metastases in 67-year-old man with prostate cancer.
A–D, Bone scintigraphy (A) and 18F-NaF PET/CT (B–D) images show more lesions in skull and ribs
than do whole body-bone MR images (E–G).
Range of alpha-particle
Radium-223
Bone surface
Mechanism of action for the targeting of osseous metastases by 223Ra.
Reprinted with permission from Algeta ASA, from 2012 ASCO GU Symposium
presentation.
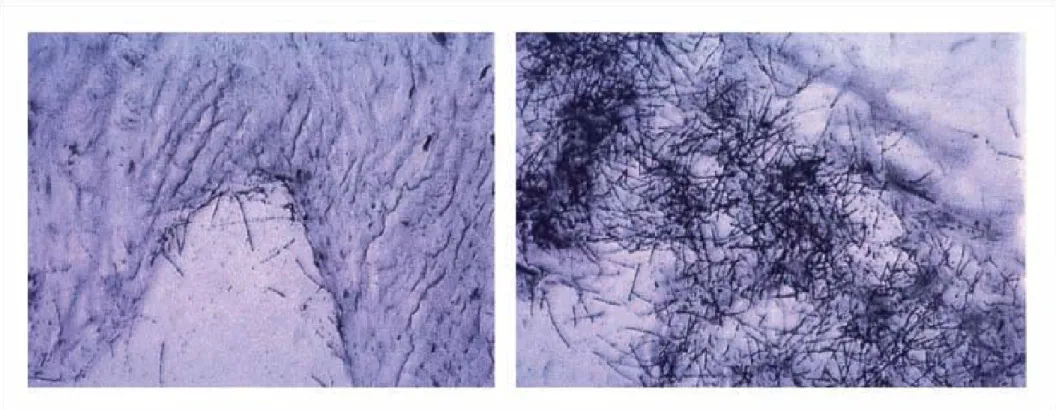
Fig. 2
. Microautoradiography from a dog injected with an a-emitting bone seeker. Distribution of a-particle tracks in normal spongious bone (A, left) and an osteoblastic zone (B, right).34
1. After intravenous injection, radium-223 is rapidly cleared from the blood and is distributed primarily into bone or is excreted into intestine.
2. The after injection of remaining blood radioactivity as 15 minutes, about 20%; 4 hours, about 4% and less than 1% at 24 hours.
3. At 10 minutes post-injection, radioactivity was observed in bone and in intestine. At 4 hours post-injection, the percentage of the radioactive dose present in bone and intestine was approximately 61% and 49%, respectively.
4. No significant uptake was seen in other organs such as heart, liver, kidneys, urinary bladder, and spleen at 4 hours post-injection.
FDA Package i
The whole body measurements indicated that approximately 63% of the administered radioactivity was excreted from the body within 7 days after injection (after correcting for decay). Fecal excretion is the major route of elimination from the body. At 48 hours after injection, the cumulative fecal
excretion was 13% (range 0 - 34%), and the cumulative urine excretion was 2%
(range 1 - 5%). There was no evidence of hepato-biliary excretion based on
imaging data.
FDA Package 36
Purpose 223Ra-Dichloride (223Ra) is a novel bone-seeking alpha-emitter that prolongs survival in patients with castration resistant metastatic prostate cancer. We conducted a study to better profile the pharmacokinetics, pharmacodynamics, and biodistribution of this agent. Methods Ten patients received either 50, 100, or 200 kBq of 223Ra per kilogram of body weight. Subsequently, six of these ten patients received a second dose of 50 kBq/kg. Pharmaco-kinetics and biodistribution were
assessed by serial blood sampling, planar imaging, and whole-body counting. Pharmacodynamic assessment was based on measurements of prostate-specific antigen, bone alkaline phosphatase, and serum N-telopeptide. Safety was also assessed. Results Pharmacokinetic studies showed rapid
clearance of 223Ra from the vasculature, with a median of 14 % (range 9– 34 %), 2 % (range 1.6–3.9
%), and 0.5 % (range 0.4–1.0 %) remaining in plasma at the end of infusion, after 4 h, and after 24 h, respectively. Biodistribution studies showed early passage into the small bowel and subsequent fecal excretion with a median of 52 % of administered 223Ra in the bowel at 24 h. Urinary excretion was relatively minor (median of 4 % of administered 223Ra). Bone retention was prolonged. No
doselimiting toxicity was observed. Pharmacodynamic effects were observed (alkaline phosphatase and serum N-telopeptides) in a significant fraction of patients. Conclusion 223Ra cleared rapidly from plasma and rapidly transited into small bowel, with fecal excretion the major route of
elimination. Administered activities up to 200 kBq/kg were associated with few side effects and appeared to induce a decline in serum indicators of bone turnover.
Serial dynamic images of anterior abdomen/pelvis obtained after intravenous administration of 7,585 kBq (0.205 mCi) of 223Ra-dichloride (patient 4). The images show prompt uptake throughout small bowel with mild uptake in liver and no gallbladder
visualization. The uptake in small bowel, although showing some changes, persists for 232 min. The activity moves intraluminally into ascending and transverse colon (1 day), then into descending colon (2 days), and there is significant clearing from bowel by 6 days.
The volume-rendered contrast CT shows bowel loops that
correspond to the early 223Rachloride images. A 99mTc-MDP
bone scan is available for reference. There is prompt uptake in the bone metastasis that persists and improves in contrast over time. Small amount of liver uptake is noted in the early dynamic images, but resolves in the later images
0-10 m 20-30 m 40-50 m
232 min post 1 d 2 d
6 d Volume rendered CT Bone scan –D13
Whole-body bone scan in left panel shows multiple metastatic disease to bone.
223Ra whole-body bone scan in right panel was taken 1 day after injection. Although 223Ra images have lower counts and are noisier than the bone scan, they clearly show focal
accumulation in the most obvious bone metastasis, e.g., left distal femur, right femur, left proximal humerus. In addition, excretion into the ascending and transverse colon is noted.
Tc-99m MDP Ra-223
anterior posterior anterior posterior
Representative biodistribution images. Serial posterior images
following injection of 4,366 kBq (0.118 mCi) of 223Ra-dichloride show initial accumulation in bone metastasis and normal bone that persists over time, compared to posterior 99mTc-MDP bone scan spot image of the same region. Early images will often show some mild uptake in the kidneys that decreases rapidly and is barely seen at 4 h and not seen beyond 1 day.
0-1 h 4 h
1 day Post-bone scan
50
Single-use vial at a concentration of 1,000 kBq/mL (27 microcurie/mL) at the
reference date with a total radioactivity of 6,000 kBq/vial (162 microcurie/vial) at the reference date (Day 0)
Half life: 11.4 days
52
• Ready to use
1• Long shelf life (28 days)
• Ready to use
1• Long shelf life (28 days)
• One visit per dose
• IV injection
• Outpatient treatment
2• One visit per dose
• IV injection
• Outpatient treatment
21. Nilsson et al. Presented at: American Society for Radiation Oncology annual meeting 2010; poster 2385.
2. Biggin. Eur J Nucl Med Mol Imag. 2007;34:S391 Abstract P646.
53
• Ready to use
1• Long shelf life (28 days)
• Easy to handle
2• Ready to use
1• Long shelf life (28 days)
• Easy to handle
2• One visit per dose
• IV injection
• Outpatient treatment
2• One visit per dose
• IV injection
• Outpatient treatment
2Phase III Dose: 50
kBq/kg × 4 injections at 4-week intervals3
Half-life is 11.4 days4, which allows for sufficient time for preparation, distribution (including long-distance shipment), and administration5
Radium-223 that is not rapidly taken up in bone is rapidly excreted into the small bowel6,7 Requires no additional
specialized detection equipment5
The ultra short penetration of α particles is easily
blocked (even by paper), allowing Radium-223 to be simply handled
without the requirement for complex shielding during shipping and administration2
Virtually no restrictions on patients after they leave the clinic2
Product is isotonic with physiological pH and is supplied as single-dose glass vials with
radioactivity
concentration of 1,000 kBq/mL (0.3 mCi/mL) at the reference date8
1. Nilsson S, et al. Poster 2385 presented at: American Society for Radiation Oncology Annual Meeting; October 31-November 4, 2010; San Diego, CA. 2. Biggin. C Eur J Nucl Med Mol Imag. 2007;34:S391. Abstract P646. 3. Parker C, et al. J Clin Oncol. 2012;30(Suppl). Abstract LBA4512. 4. McDevitt MR, et al. Eur J Nucl Med. 1998;25(9):1341-1351. 5. Nilsson S, et al. Clin Can Res. 2005;11(12):4451-4459. 6.
Lewington V, et al. Presented at: ASCO Genitourinary Cancers Symposium 2010: Poster 216. 7. Morris MJ, et al. Presented at: ASCO Genitourinary Cancers Symposium 2010: Poster 211. 8. Data on file, Algeta ASA.
1. Primary end point was overall survival.
2. Secondary efficacy end points included time to the first symptomatic
skeletal event and various Biochemical end points.