國立臺灣大學工學院應用力學研究所 碩士論文
Graduate Institute of Applied Mechanics College of Engineering
National Taiwan University Master Thesis
利用免疫螢光進行乳癌 mTOR 途徑藥物癌伏妥錠 (Everolimus)敏感度評估研究
Use of immunofluorescence to assess the efficacy of mTOR pathway therapeutic agent Everolimus in breast cancer
郭俊廷
Chun-Ting Kuo
指導教授:胡文聰 博士
Advisor: Andrew M. Wo, Ph.D.
中華民國 106 年 7 月
July 2017
i
致謝
時間真的過得好快,一下子兩年就到了。首先感謝我的口試委員盧彥伸醫師及 林季宏醫師在平時進度報告及口試的時候,一步步教導我,也讓我知道我還需努力 的地方,並謝謝我的指導教授 胡文聰博士,老師除了在研究方向與論文上的指導 外,也教育我待人接物和生活技能,尤其英文方面真的讓我受益良多。也感謝貞伶 學姐,在 mTOR 的研究上一直帶我,我們總是一起討論,當爭論不下時,我就去 做實驗以驗證孰是孰非,我的論文就這麼一點一滴建立起來了。感謝冠瑄學姐一直 教我細胞培養的細節跟訣竅,讓我在短時間裏自己維持五種細胞株的供應。除了在 研究上的幫助外,兩位學姐更是關心我的日常生活,也感謝芷琪學姐教我快速上手 Western blot,讓我能順利的做好實驗。這兩年真的對我自己來說進步好多,從一個 對生醫領域都不熟的人,慢慢努力的涉獵,進展到對於很多生化實驗及生化 pathway 都稍微懂一點點的研究生。感謝實驗室的各位夥伴,維遠、韋凡、華偉、
啟睿、展毓、韋傑、念文、恆允、沐承、博惟、立國、龔驛、博文的陪伴,也感謝 Angie 伴我一起修改論文字句。
我真的很幸運能進入實驗室跟大家一起努力,也非常感謝 Alice 姐總是在我心 裡沮喪及不知所措的時候為我禱告,讓我能用平靜的心情迎接在我面前一個又一 個的挑戰與難題。在實驗室裏,我就像一顆小小的螺絲釘,現在這個小釘子要畢業 了,真的不知道要如何表達我心裡的感動及感謝,阿們。也感謝一直在我身旁為我 打氣的人,威宇老師、揚文老師及冠德學長,你們總是在我生命中最脆弱、最不堪 一擊的時候陪著我,也跟著我一起面對艱難與考驗,沒有你們,就沒有現在的我!
最後,也感謝我的姐姐能在最後撰寫論文的時刻陪著我,跟我一同分享生活的點滴,
更謝謝在天上的父親:父親,我做到了!最後的最後,感謝主,真的感謝您讓我有 如此與別人不同的生涯,現在的我,人生才正要開始!
中文摘要
在許多癌症腫瘤中,PI3K/AKT/mTOR 路徑常被激勵活化並且掌控癌細胞的 主要功能。PI3K/AKT/mTOR 路徑的下游分子,磷酸化的 4EBP1 蛋白及磷酸化 的 S6K1 激酶更在細胞的生化功能裡扮演重要的角色。除此之外,mTOR 標靶治 療更是在乳癌病人對於賀爾蒙治療或化學治療產生抗藥性時進行治療。而讓 mTOR 中的專一性鍵結失效來達到調降 PI3K/AKT/mTOR 路徑的活化程度的癌 伏妥錠(Everolimus)則為 mTOR 標靶治療中常見的藥物。但在某些 mTOR 標靶 治療病人當中,癌伏妥錠卻沒有產生其應達到的治療效果。
本論文研究係以免疫螢光方式對於 Hs578T, MCF7, BT474, MDA-MB-231, 乳癌細胞株及 ABC-82T 及 ABC-16TX1 PDCC 細胞株進行 mTOR 抑制劑癌伏妥 錠(Everolimus)之敏感度測定。先以標準 MTT 測試及細胞生長率測試判別其細 胞株之藥物敏感度,而後則是利用磷酸化 4EBP1 Thr37/46 蛋白抗體及磷酸化 S6K1 Ser424 激酶抗體對細胞株進行免疫螢光亮值測定以和測出的敏感度加以 比較。
研究結果顯示利用免疫螢光之分析方法的確可指出其乳癌細胞株對於癌伏 妥錠(Everolimus)之敏感度。單獨的磷酸化 4EBP1 Thr37/46 蛋白抗體及磷酸化 S6K1 Ser424 激酶抗體之螢光表現可將乳癌細胞株及 PDCC 細胞株進行分群,
磷酸化 4EBP1 Thr37/46 及磷酸化 S6K1 Ser424 兩者綜合之螢光亮值則可代表其 藥物敏感度程度。當細胞對癌伏妥錠具有抗藥性潛力時,磷酸化 4EBP1 Thr37/46 及磷酸化 S6K1 Ser424 亦會產生動態變化,並且由實驗結果得知 mTOR 藥物的 抗藥性並不是只對於 AKT/mTOR 路徑有專一性,而是與其它特定蛋白如 LKB1 或其他路徑如 MAPK/ERK 路徑有關。
關鍵字:m TOR 路徑、癌伏妥錠、磷酸化 4EBP1、磷酸化 S6K1、mTOR 抗藥性、
MTT 測試
iii
Abstract
In many solid tumors, the PI3K/AKT/mTOR pathway is activated and is believed to play major roles in a range of cellular functions. Downstream of this pathway, pho-4EBP1 and pho-S6K1 perform critical role in controlling biological processes. In breast cancer, when patients start to exhibit resistance with hormonal therapy or chemotherapy, mTOR inhibitor, for example Everolimus, is often considered, which can deregulate the PI3K/AKT/mTOR pathway by allosteric binding the catalytic site of mTORC1. But in some mTOR-targeted therapy cases, Everolimus does not exhibit the desired efficacy. This work assesses the use of immunofluorescence analysis to predict the efficacy of the mTOR inhibitor Everolimus using breast cancer cell lines- Hs578T, MCF7, BT474, MDA-MB-231- and patient-derived cell culture (PDCC)-ABC-82T, and ABC-16TX1. These cells provided predictive information on the sensitivity of Everolimus using cell viability and MTT assays based on immunofluorescence intensities of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424. Results show that the immunofluorescence analyses can be used to indicate the efficacy of mTOR inhibitor Everolimus on cells tested.
Independently, pho-4EBP1 Thr37/46 and pho-S6K1 Ser424 immunofluorescence expression can classify into different groups based on their intensities for cell lines and PDCC. The combined immunofluorescence intensity of pho-4EBP1 Thr37/46 and
pho-S6K1 Ser424 is representative of the efficacy of Everolimus. Results also suggest that dynamitic change for pho-4EBP1 and pho-S6K1 occur when cells have resistance characteristic of Everolimus. Further, mTOR resistance is not only consequence of
AKT/mTOR but also by LKB1 or MAPK/ERK pathway. Furthermore, LKB1 and pho- GSK3β may also be potential markers to predict the efficacy of Everolimus therapy.
Keywords: mTOR, Everolimus, pho-4EBP1, pho-S6K1, mTOR resistance, MTT assay.
v
Contents
致謝 ……… i
中文摘要………...ii
Abstract……….iii
Contents………...v
List of Figures………...vii
List of Tables………...ix
Chapter 1. Introduction 1
1.1 Breast cancer and epithelial-mesenchymal transition………...1
1.2 The PI3K/AKT/mTOR pathway………3
1.2.1 Growth factors actuate the PI3K/AKT/mTOR pathway………...3
1.2.2 EIF4E-phosphorylated-4EBP1 protein and phosphorylated -S6K1 protein………4
1.3 Motivation of this work……….6
1.3.1 Targeted therapy and mTOR inhibitory drug sensitivity in breast cancer………...6
1.3.2 Clinical analysis method for phosphorylated protein—comparison between immunofluorescence, q-PCR , immunohistochemistry and western blot………7
1.4 The goal of this thesis……….8
Chapter 2. Materials and Methods 9
2.1 The experimental structure………..9
2.2 Cell culture, cell lines, and patient-derived cell culture (PDCC)………..9
2.3 Reagents………....11
2.4 Cell viability rate assay……….12
2.5 MTT and IC50 assays………..……….12
2.6 Immunofluorescence staining………...13
2.7 Western blots……….14
2.8 Statistical analysis……….15
Chapter 3 Results and Discussion 16
3.1 Immunofluorescence marker for Everolimus resistance in cell lines and PDCC………...16
3.1.1 Gene mutation and drug sensitivity………...16
3.1.2 Cell viability rate and IC50 value of cell lines and PDCC………..…...17
3.1.3 Immunofluorescence expression of mTOR markers and Everolimus sensitivity……..20
3.2 Pho-4EBP1 and pho-S6K1 do not have high specificity for AKT/mTOR………...28
3.3 Combined IF expression of pho-4EBP1 and pho-S6K1 before and after adding Everolimus………..33
3.4 Epithelial-mesenchymal transition state and Everolimus sensitivity………...35
3.5 The arrangement of IF marker in rare cancer cells detection………...36
Chapter 4 Conclusions 38
References 39
vii
List of Figures
Figure 1 Schematic representation of the PI3K/AKT/mTOR pathway………..4 Figure 2 The two-step phosphorylation of 4EBP1 protein……….………5 Figure 3 The calibration Curve of plate reader from MTT assay………....13 Figure 4 ABC-16TX1 PDCC exhibits stem cell characteristics (CD44 is high and CD24 is low),
which will likely lead to the ability of drug resistance.………..17 Figure 5 Cell proliferation under the 200 nM Everolimus after about 24hours. Some cells are Everolimus-sensitive cells, the others are Everolimus-resistant cells.………..18 Figure 6 Cell viability for cell lines and PDCC by MTT assay (a) Hs578T, BT474 and MCF7 (b)
ABC-16TX1 (c) IC50 values of Everolimus.………20 Figure 7 IF expression for BT474, MCF7, ABC-82T, and ABC-16TX1 cells without Everolimus
and the normalized IF intensity. (a) pho-S6K1 Ser424 (b) pho-4EBP1Thr37/46 (c) Pho-S6K1 Ser424 (d) Pho-4EBP1Thr37/46.……….23 Figure 8 Combined IF expression of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424 for cell lines.
(a) Everolimus-resistant cells will have high IF intensity. (b) the average expression of combined IF intensity of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424.
(c)Comparison between IC50 values, and combined signals.……….………...26 Figure 9 The ROC curve for Pho-S6K1, Pho-4EBP1, and this two combined markers. The
combined IF intensity has a better efficiency than pho-4EBP1 and pho-S6K1 individually.………..27 Figure 10 Pho-4EBP1 and pho-S6K1 might be impacted not only by AKT/mTOR, but also by
another target or pathway………...30
Figure 11 The expression of pho-GSK3β (a) IF relative intensity (b) western blot with ponceau s solution, which shows the total protein (c) western blot with beta-actin.It indicates that the expression of pho-AKT cannot represent the resistance of Everolimus.………...31 Figure 12 LKB1 expression for cell lines and PDCC (a) The IF image for MCF7 and ABC- 16TX1 cells (b) quantifies intensities for IF signals. (c) The western bolt expression of LKB1 for cell lines.It shows that Everolimus-sensitive cells has the higher LKB1
IF intensity than Everolimus-resistant
cells..………..33 Figure 13 Combined expression of pho-4EBP1 and pho-S6K1 for both control group and
Everolimus 500nM group for 24 hours (a) MCF7 cell line (b) BT474 cell line (c)
MDA-MB-231 cell line and ABC-16TX1
PDCC.……….35 Figure 14 The IF expression of vimentin for cell lines.Red ones represent Vimentin signals and
blue ones represent the nucleus signals. The positive relation between EMT state and the efficacy of Everolimus..……….36 Figure 15 The arrangement of IF expression. (a) White blood cells in healthy people (b) MCF7
cell line. The expression of CD45 will be arranged in FITC channel, the expression of pan cytokeratin C11+AE1/AE3 will be arranged in PE channel and the expression of pho-4EBP1+pho-S6K1 will be arranged in APC channel...37
ix
List of Tables
Table 1 Gene mutation for cell lines and PDCC………10 Table 2 Characteristics for cell lines and PDCC………10 Table 3 The group of cells by pho-S6K1 and pho-4EBP1………...24
Chapter 1 Introduction
1.1 Breast cancer and epithelial-mesenchymal transition
Breast cancer is the most common cancer for women, and metastasis is the main cause of motility. This disease can be divided into three subtypes: hormone receptors positive (luminal A, luminal B), HER2 enriched and triple negative.
According to the average statistics of U.S breast cancer cases for all ethnicity in 2015, about 74% of breast cancer patients were hormone receptors positive, 14% were HER2 enriched and 12% were triple negative. Among these patients, triple-negative breast cancers patients were regarded as more invasive and have poorer prognoses [1].
Besides, the final situation of breast cancer also depends on many biological features. The diagnosis and the therapy will be determined by these features. But in some patients, they have a similar features, yet they have different final outcomes.
So how to make the true diagnosis and find the biomarkers for breast cancer patients is important. Some studies showed that the number of rare cancer cells, for instance, circulating tumor cells (CTCs) could have a significant relationship with patient survival in breast cancer [2-3]. One reference also indicated that micro-RNA could
2
be a therapeutic tools for breast cancer [4].
Epithelial-mesenchymal transition (EMT) also plays an important role in cancer metastasis. EMT is the process that epithelial phenotype cells start to acquire mesenchymal phenotype characteristics thus potentially invasive and drug resistance.
EpCAM, pan cytokeratin, and E-CAD can represent epithelial markers. Vimentin, twist, and N-CAD are mesenchymal markers [5]. Cancer cells also can be classified into three parts by the expression of EMT: pure epithelial cells (E), intermediate epithelial and mesenchymal cells (E/M), and pure mesenchymal cells (M).
1.2 The PI3K/AKT/mTOR pathway
1.2.1 Growth factors actuate the PI3K/AKT/mTOR pathway
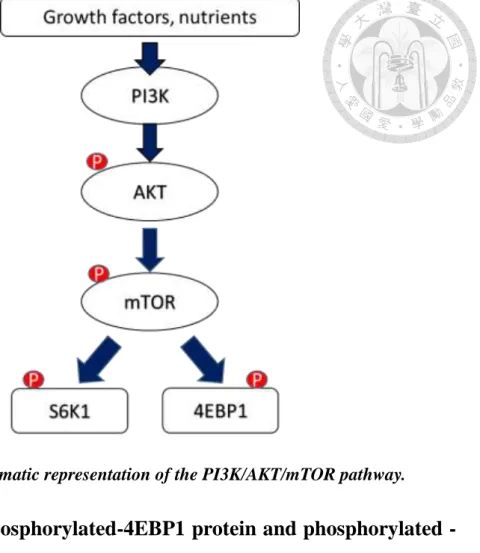
In breast cancer, PI3K/AKT/mTOR pathway is activated frequently and this pathway controls many major functions. For example, cellular proliferation, metastasis, growth, survival, and motility. When cells are stimulated by growth factors or hormones, phosphatidylinositol 3-kinase (PI3K) will be activated first. It will promote the phosphorylation of AKT, and the mechanistic target of rapamycin complex 1 (mTORC1) sequentially. And mTORC1 will phosphorylate its downstream substrate eukaryotic initiation 4E-binding protein 1 (4EBP1) and ribosomal protein S6 kinase beta-1 (S6K1) [6,7]. Besides, p53, KRAS, PI3CA and PTEN mutations also could have a relationship with the PI3K/AKT/mTOR pathway [8,9]. In many references, mTOR pathway could play a critical role in cancer, and phospho-4EBP1 and phospho-S6K1 also perform the critical role in controlling biological processes.
4
Figure 1 Schematic representation of the PI3K/AKT/mTOR pathway.
1.2.2 EIF4E-phosphorylated-4EBP1 protein and phosphorylated - S6K1 protein
As mentioned in section 1.2.1, there are two downstream markers for PI3K/AKT/mTOR pathway. One is phosphorylated-4EBP1 (Pho-4EBP1), the other is phosphorylated ribosomal protein S6 kinase 1 (Pho-S6K1). In the normal situation, 4EBP1 will combine with eIF4E and form 4EBP1-eIF4E complex. When mTORC1 is phosphorylated, it will phosphorylate 4EBP1 at Thr37/46, Thr70 and Ser65 four sites sequentially. But when 4EBP1 is phosphorylated at Thr37/46, the eIF4E does not release from 4EBP1 until it phosphorylate at Ser65. In other words, the phosphorylation of 4EBP1 protein has two steps, the first step is the phosphorylation
at Thr37/46, the 4EBP1-eIF4E complex still be combined together this moment. The second step is the phosphorylation at Thr70 and Ser65. Then eIF4E will be released from 4EBP1 and start the translation initiation. The second target is the phosphorylated ribosomal protein S6 kinase 1 (Pho-S6K1). Similarly, S6K1 will be phosphorylated at Thr389, Thr421, Ser371, and Ser424 when mTORC1 is phosphorylated, and it is also an important regulators of protein synthesis [10].
Figure 2 The two-step phosphorylation of 4EBP1 protein.
6
1.3 Motivation of this work
1.3.1 Targeted therapy and mTOR inhibitory drug sensitivity in breast cancer
Breast cancer therapy is composed of six approaches: surgery, radiation, hormonal therapy, chemotherapy, targeted therapy, and immunotherapy. For breast cancer, mTOR-targeted therapy is considered when patients are resistant to hormonal therapy or chemotherapy. In this event, Everolimus is one of mTOR inhibitors and can deregulate the PI3K/AKT/mTOR pathway by allosteric binding the catalytic site of mTORC1. In some studies, anti-proliferative effect of Everolimus is also determined in cancer cell lines [33]. For some patients, the efficacy of this therapeutic agent is not achieved yet side effects happened quality of life.
Many researchers have studied the efficacy of mTOR inhibitors. Some showed that it could distinguish drug sensitivity from gene expression and mutations [11,17,18,21]. Some studies pointed out that it could be classified by epithelial-mesenchymal transition (EMT) [12] and the others works indicated that the downstream of mTOR pathway could find some information by western blot for cell lines [13,14,15,17,19,22]or immunohistochemistry method for tumors [16,20,22]. But many of these studies are not conclusive. So how to check the
efficacy of mTOR inhibitors is very important for doctors to see how this drug is useful for patients.
1.3.2 Clinical analysis method for phosphorylated protein—
comparison between immunofluorescence, q-PCR, immunohistochemistry and western blot
As mentioned in section 1.3.1, many researches have studied in mTOR pathway and its inhibitors, for instance, Everolimus. These works use some analysis methods like q-PCR, immunohistochemistry and western blot to try to show the efficacy of mTOR inhibitors [19-24].
Immunohistochemistry is often used in patient’s tumors. It has to process the surgery for patients to get the tumors, and this method is also the most used method in clinical trials. Western blot and q-PCR is the process to observe the expression of target protein and RNA. Many researchers use these methods to investigate the situation of mTOR, but these methods cannot use in rare cells. For example, western blot cannot be detected by antibodies if the amount of proteins is too low.
Immunofluorescence (IF) is an easy technique by using specific antibodies which have been conjugated to fluorescent dyes. Besides, IF method is the convenient, quick method and can be detected for rare cancer cells compared with
8
immunohistochemistry, western blot, and q-PCR. The signals of IF can also be used in liquid biopsy and have the same expression for western blot. This is why that immunofluorescence is chosen to be the subject of the thesis.
1.4 The goal of this thesis
The purpose of this thesis is to build the immunofluorescence analysis and show the mTOR inhibitor Everolimus efficacy for breast cancer cell lines by IF expression.
Chapter 2
Materials and methods
2.1 The experimental structure
The experimental design would be divided into two parts. First part was to do cell viability rate assay and MTT assay for breast cancer cell lines and patient- derived cell culture (PDCC). The second part was to show how the immunofluorescence signals can predict the sensitivity of mTOR inhibitor, Everolimus.
2.2 Cell culture, cell lines, and patient-derived cell culture (PDCC)
Breast cancer cell lines MCF7, MDA-MB-231, BT474, Hs578T and two PDCC ABC-16TX1, ABC-82T were chosen to see whether the IF signals could predict the mTOR inhibitor Everolimus sensitivity or not.
MCF7 cell lines were cultured in 10% FBS DMEM/F12 medium. BT474 cell line were cultured in Hybricare medium, which EGF was added. MDA-MB- 231 cell line were cultured in 10% FBS DMEM HG medium. Hs578T cell line were cultured in 10%FBS DMEM HG medium, which insulin was added. Patient- derived cell culture (PDCC) ABC82T and ABC-16TX1 were unique cells, which were derived from breast cancer patient metastatic biopsy samples, and these two PDCC were cultured in IH medium. All cells were incubated in the culture dish
10
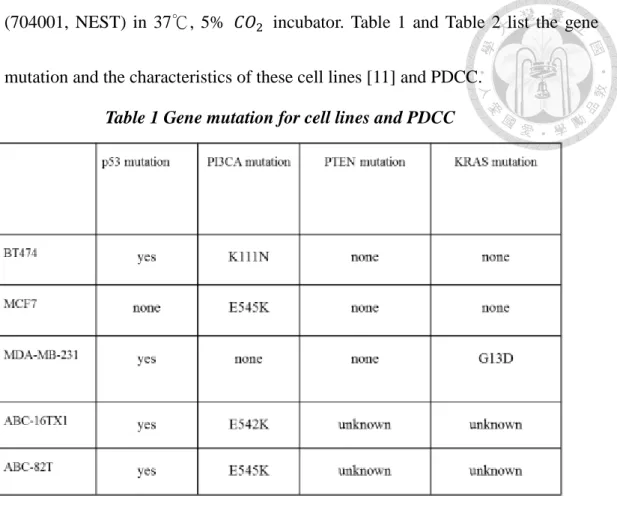
(704001, NEST) in 37℃, 5% 𝐶𝑂2 incubator. Table 1 and Table 2 list the gene mutation and the characteristics of these cell lines [11] and PDCC.
Table 1 Gene mutation for cell lines and PDCC
Table 2 Characteristics for cell lines and PDCC
2.3 Reagents
In this thesis, some reagents and buffers were used. Cell fixation buffer and Alexa Fluor 488 anti-human CD24 antibody were purchased from BioLegend.
Cell permeabilization kit were purchased from MiltenyiBiotec. Mouse anti-human CD45 conjugated with Alexa Fluor 488 and Hoechst33342 were purchased from Invitrogen. Pho-4EBP1 Thr37/46 antibody, vimentin antibody conjugated with Alexa Fluor 647 and pho-GSK3β Ser9 antibody were purchased from Cell Signaling Technology. Mouse anti-human CD44 antibody were purchased from BD Biosciences. Pho-S6K1 Ser424 antibody, pan cytokeratin C11 antibody, the donkey anti-rabbit and anti-mouse IgG H&L conjugated with Alexa Fluor 488 and 647 secondary antibody were purchased from Abcam. Pan cytokeratin AE1/AE3 antibody were purchased from Novus Biologicals. LKB1 antibody, goat anti- rabbit and anti-mouse IgG(H+L) superclonal secondary antibody, HRP conjugated were purchased from ThermoFisher. Everolimus were purchased from Selleckchem. 10X TGS buffer and 10X TG buffer for western blot were purchased from Omics Bio. MTT powder were purchased from Sigma-Aldrich.
12
2.4 Cell viability rate assay
MCF7, MDA-MB-231, BT474 cell lines, and ABC-82T, ABC-16TX1 two PDCCs were used. First, seeded cells in the 3.5 cm culture dish were grown to about 50-60% confluence. Second, 200 nM Everolimus were added into the dish. After about 24 hours, cells were harvested and the number of live cells were counted to determine cell viability rate. The MTT assay was also used to confirm
the cell sensitivity. The cell viability rate is defined as:
𝑐𝑒𝑙𝑙 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑑𝑟𝑢𝑔 𝑡𝑟𝑒𝑎𝑡𝑚𝑒𝑛𝑡 𝑎𝑓𝑡𝑒𝑟 24 ℎ𝑜𝑢𝑟𝑠 − 𝑐𝑒𝑙𝑙 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑐𝑜𝑛𝑡𝑟𝑜𝑙 𝑎𝑓𝑡𝑒𝑟 𝑎𝑏𝑜𝑢𝑡 24 ℎ𝑜𝑢𝑟𝑠 𝑐𝑒𝑙𝑙 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑐𝑜𝑛𝑡𝑟𝑜𝑙 𝑎𝑓𝑡𝑒𝑟 𝑎𝑏𝑜𝑢𝑡 24ℎ𝑜𝑢𝑟𝑠 × 100%
2.5 MTT and IC50 assays
About 5000-10000 cells were seeded in 100μl medium into the 96-well and incubated in 37℃, 5% 𝐶𝑂2 incubator overnight before the drug treatment.
Second, the same volume of the culture medium which contained different Everolimus concentration were replaced and were incubated for about 48 hours.
After Everolimus treatment for about 48 hours, the culture medium were replaced by 12mM MTT about 100μl and were placed for 3 hours in 37℃,
5% 𝐶𝑂2 incubator. Finally, the same amount DMSO were replaced for 20 minutes at 37℃ and the absorbance of DMSO at 570 nm were determined, which stood for the number of live cells by the plate reader (MQX 200, BioTek). the IC50
values were also determined for every cell lines. The accuracy of the plate reader would be done before the MTT assay.
Figure 3 The calibration Curve of plate reader from MTT assay.
2.6 Immunofluorescence staining
For immunofluorescence staining, cells were harvested first, the fixation buffer 200μl were added,incubated for 20 minutes at 4℃and washed with running buffer. Second, cells were permeabilized by adding the inside perm buffer, incubated for 20 minutes at 4℃ and washed with running buffer (some antibody did not use this process).
14
After cells were fixed and/or permeabilized, the primary antibodies were added, incubated for 25 minutes at 4℃ and washed with running buffer. When primary antibodies were bonded at cells, the secondary antibodies conjugated to Alexa Fluor 488 or 647 channels were added, incubated for 25 minutes at 4℃ and washed with running buffer. Immunofluorescence results were taken by the microscope.
2.7 Western blots
First, 105 cells were boiled with sample buffer for about 15 minutes and the cell samples which contained proteins were loaded into the wells of the Mini- PROTEAN Precast Gels which were purchased from Bio-Rad. Second, the gels were run with 200 volts for about 30 minutes. When the gels were run completely, proteins were transferred to PDVF membranes which were purchased from Merck Millpore with 100 volts for 30 minutes.
After running gels and blotting, the PDVF membranes were stained with Ponceau S solution for about 5 minutes to show the total proteins expression to check the equal amount protein and were washed with PBS-T three times. After this, the PDVF membranes were blocked with milk at room temperature for about 2 hours. After blocking, the primary antibody (1:1000) were added into the milk,
incubated at 4 ℃ overnight and were washed with PBS-T three times. The secondary antibody which HRP conjugated (1:5000) were added into the milk, incubated at room temperature for about 1 hours and washed with PBS-T six times.
Proteins were detected using UVP BioSpectrum 500 Imaging System.
2.8 Statistical analysis
The immunofluorescence pictures of the thesis were taken from Leica DMI 6000 B microscope and analyzed by MetaMorph software. In MetaMorph software, there were the counts nuclei function, which can count the cells IF intensity automatically. After taking the photos and counting the IF intensity, it was compiled statistics the by SigmaPlot 12.5 software and expressed as mean ± s. e. m.
16
Chapter 3
Results and discussion
3.1 Immunofluorescence marker for Everolimus resistance in cell lines and PDCC
3.1.1 Gene mutation and drug sensitivity
The goal of this work is to determine Everolimus sensitivity for these cell lines and PDCC by immunofluorescence (IF) markers. It is important to understand the relation between IF signals and the Everolimus sensitivity.
Doctors also can use them for patients to make the judgment on usage of Everolimus.
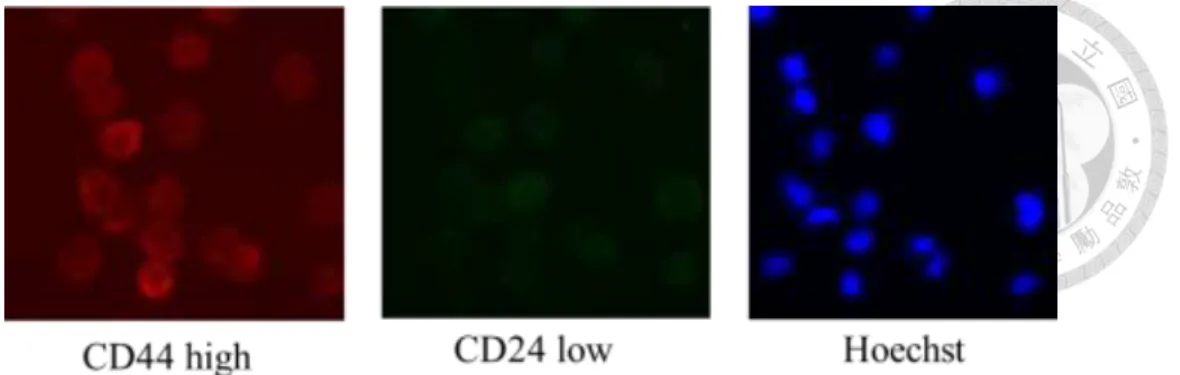
Although the expression of mTOR pathway is affected by regulation of p53, KRAS, PI3CA and PTEN gene mutation, these mutations do not provide reliable marker characteristics to predict Everolimus sensitivity. Hence, this work aims to use immunofluorescence method towards this end. And from Table 2 and figure 4, ABC-16TX1 cells show the stem cell expression, which CD44 expression is high and CD24 expression is low by immunofluorescence, stands for the high ability of drug resistance.
Figure 4 ABC-16TX1 PDCC exhibits stem cell characteristics (CD44 is high and CD24 is low), which will likely lead to the ability of drug resistance.
3.1.2 Cell viability and IC50 value of cell lines and PDCC
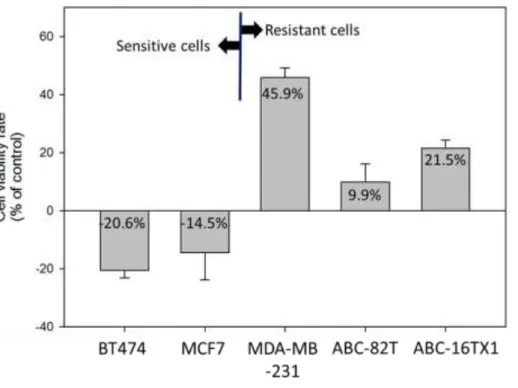
For cell viability asssay, the number of cells will be counted before and after adding Everolimus 200nM for 24 hours. Figure 5 represents cell viability rate for BT474, MCF7, MDA-MB-231 cell lines, and ABC-82T, ABC-16TX1 PDCC. The cell viability rate of BT474 and MCF7 are negative on sensitive to Everolimus, while the cell viability rate of MDA-MB-231, ABC-82T and ABC- 16TX1 are positive on resistant to Everolimus.
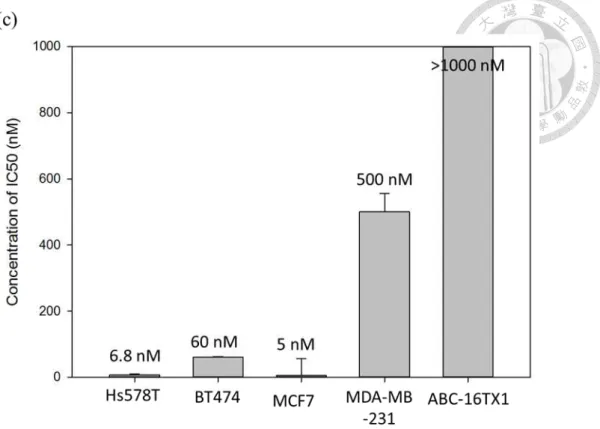
Figure 6 represents results for the MTT assay and IC50 values for breast cancer cell lines and PDCC. Figure 6(a) shows cell viability for Hs578T, BT474, MCF7 cell lines under different Everolimus concentration. Results show that the inhibition rate are over 50% when these cells are less than 100 nM, which can be regarded as Everolimus-sensitive cells. Figure 6(b) shows cell viability for ABC-16TX1 cells under different Everolimus concentration. Results show that
18
cell viability is still about 80% under high Everolimus concentration. It cannot find IC50 values which means high resistance of Everolimus. Figure 6(c) shows IC50 values for breast cancer cell lines and PDCC, which means the resistant characteristics for these cells. Every experiment is tested in triplicate.
Figure 5 Cell proliferation under the 200 nM Everolimus after about 24hours. Some
cells are Everolimus-sensitive cells, the others are Everolimus-resistant cells.
20
Figure 6 Cell viability for cell lines and PDCC by MTT assay (a) Hs578T, BT474 and MCF7 (b) ABC-16TX1 (c) IC50 values of Everolimus.
3.1.3 Immunofluorescence expression of mTOR markers and Everolimus sensitivity
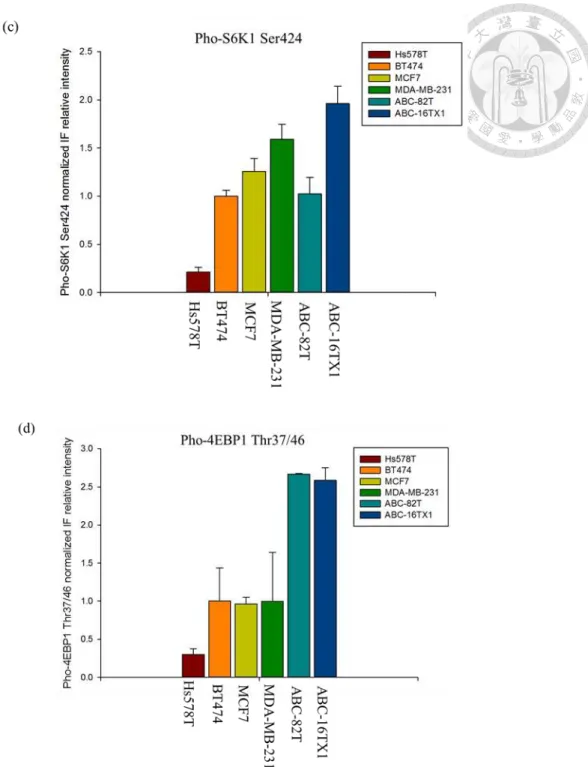
Figure 7 shows the baseline IF intensity for the cell lines and PDCC prior to adding of Everolimus. Figure 7(a) and 7(b) means the images of pho-S6K1 Ser424 and pho-4EBP1 Thr37/46 respectively. For ABC-16TX1 cells, both pho- 4EBP1 and pho-S6K1 have high IF intensity.
Figure 7(c) and 7(d) show the normalized IF intensity (by the intensity of BT474) for pho-4EBP1 Thr37/46 and pho-S6K1 Ser424 respectively. Data
suggest variation in IF intensity among these cells for both protein markers. In light of the results in figure 5 and 6, where sensitivity and resistance of each cell type is known, IF intensities for each of the protein marker do not correlate with known response to Everolimus. Results also display functional heterogeneity as mentioned in the reference [17] for some cells, like ABC-82T and MDA-MB-231, i.e., when IF signals of pho-4EBP1 are high, IF signals of pho-S6K1 are low, or when IF signals of pho-4EBP1 are low, IF signals of pho-S6K1 are high.
Results from figure 7(c) and 7(d) can be divided into three group of cells.
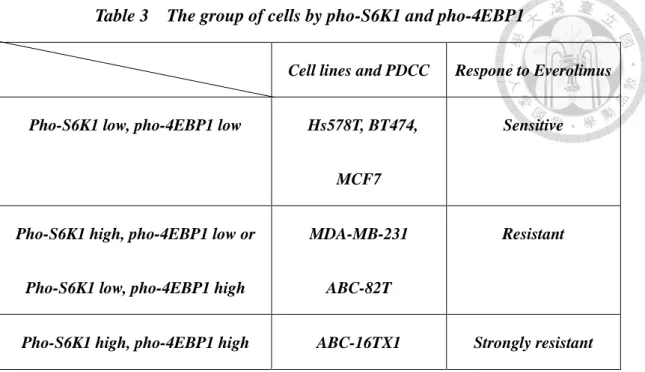
The first group contains Everolimus sensitive cells Hs578T, BT474 and MCF7, which both pho-S6K1 and pho-4EBP1 have low IF intensities. The second group is middle or resistant Everolimus sensitivity cells MDA-MB-231 and ABC-82T, which pho-S6K1 have low intensities and pho-4EBP1 have high intensities or pho-S6K1 have high intensities, and pho-4EBP1 have low intensities. The third group is ABC-16TX1 cells, in which both the pho-S6K1 and pho-4EBP1 are high, thus demonstrate high Everolimus resistance. Three these groups are listed in Table 3.
22
Figure 7 IF expression for BT474, MCF7, ABC-82T, and ABC-16TX1 cells without Everolimus and the normalized IF intensity. (a) pho-S6K1 Ser424 (b) pho-4EBP1
Thr37/46 (c) Pho-S6K1 Ser424 (d) Pho-4EBP1 Thr37/46.
24
Table 3 The group of cells by pho-S6K1 and pho-4EBP1
Cell lines and PDCC Respone to Everolimus
Pho-S6K1 low, pho-4EBP1 low Hs578T, BT474,
MCF7
Sensitive
Pho-S6K1 high, pho-4EBP1 low or
Pho-S6K1 low, pho-4EBP1 high
MDA-MB-231
ABC-82T
Resistant
Pho-S6K1 high, pho-4EBP1 high ABC-16TX1 Strongly resistant
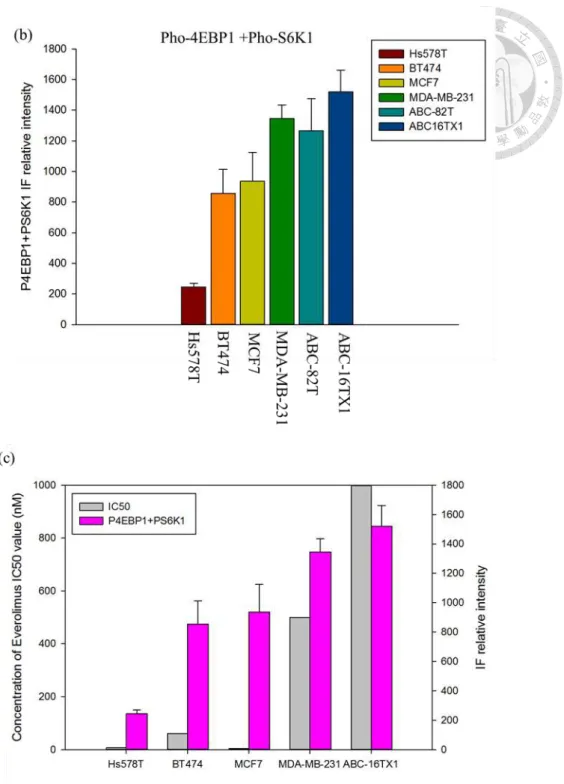
Figures 8(a) and figure 8(b) display the combined IF intensities of pho- S6K1 and pho-4EBP1 by adding results of figure 7(c) and 7(d). Unlike figure 7(c) and 7(d) for individual marker, combined intensities suggest a clear trend.
Hs578T has the lowest relative intensity of all, followed by BT474 and MCF7 with higher intensity. These three cell lines are sensitive to Everolimus therapy (Figure 5 and 6). MDA-MB-231, ABC-82T and ABC-16TX1 all have high relative intensity and they are resistant to Everolimus. Figure 8(c) represents the relationship between combined IF intensity and IC50 value (Figure 6). Results indicate that combined IF intensity is proportional to IC50 value in term of response to Everolimus. The high expression of pho-4EBP1 and pho-S6K1 in some cells may reflect mutation of mTOR. Two references [25,26] also provided
evidence that the expression of mTOR downstream marker will increase when the mTOR genes are mutated. Further studies suggested that high expression of pho-4EBP1 Thr37/46 due to resistant to rapamycin [32,33]. Moreover, pho- S6K1 Ser424 is also related to the MAPK/ERK pathway, which is another pathway in cell proliferation. In a gastric cell line study, expressions of pho- S6K1 Ser424 and pho-AKT Ser473 in rapamycin-resistant cells were higher than that in rapamycin-sensitive cells [31].
26
Figure 8 Combined IF expression of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424 for cell lines. (a) Everolimus-resistant cells will have high IF intensity. (b) the average expression of combined IF intensity of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424. (c)
Comparison between IC50 values, and combined signals.
Figure 9 shows ROC curves by for individual and combined protein markers of IF intensity. The area of ROC for pho-4EBP1 only is 0.69 and the area of ROC for pho-S6K1 only is 0.64.The area of ROC curve for combined protein markers is 0.85. This method has a better efficiency than pho-4EBP1 and pho-S6K1 individually to predict the Everolimus sensitivity. From results, we could make the conclusion that we can choose the better one to use. Every experiment is tested in triplicate.
Figure 9 The ROC curve for pho-S6K1, pho-4EBP1 and the two combined markers.
The combined IF intensity has a better efficiency than pho-4EBP1 and pho-S6K1
individually.
28
3.2 Pho-4EBP1 and pho-S6K1 do not have high specificity for AKT/mTOR
Although the IF approach can distinguish Everolimus sensitivity by
combining pho-4EBP1 Thr37/46 and pho-S6K1 Ser424, some studies suggest that if the cells were resistant for Everolimus, the expression of pho-4EBP1 would low and the expression of PI3K would be high [16]. This result, particularly the former part, is opposite from our experimental results (Figure 7(d)).
Figure 10 indicates other neighbor pathways and targets which might affect pho-4EBP1 and pho-S6K1 [27,28]. We suggest that mTOR pathway downstream targets pho-4EBP1 and pho-S6K1 might not have high specificity for AKT/mTOR. In other words, pho-4EBP1 and pho-S6K1 might be controlled not only by AKT/mTOR.
To test our hypothesis, another AKT downstream marker, pho-GSK3β Ser9 antibody, which stands for the activation of pho-AKT, and LKB1 antibody were chosen to observe whether pho-4EBP1 would be impacted only by AKT/mTOR or not.
Figure 11(a) represents the IF relative intensity (FITC) for pho-GSK3β.
Figure 11(b) and figure 11(c) show western blot for pho-GSK3β. ABC-16TX1,
ABC-82T, and BT474 cells have strong band corresponding to pho-GSK3β at 46 kDa. In contrast, MDA-MB-231 and MCF7 cells have weak band for pho- GSK3β. From results, the expression of pho-AKT cannot represent the resistance
of Everolimus. One reference [27] also indicated that the higher expression of pho-GSK3 in lung cancer cell lines, the higher the resistance of Everolimus. The results of this work confirm this phenomenon and show that the mTOR resistance might be impacted not only by the AKT/mTOR but also by LKB1 or another pathway like for instance, the MAPK/ERK pathway.
Figure 12(a) also shows the LKB1 IF signals (APC) for MCF7 and ABC- 16TX1 cells, where figure 12(b) quantifies intensities for all cell types studied.
Figure 12(c) represents the western blot for LKB1. Everolimus sensitive cells MCF7 is higher than Everolimus resistant cells ABC-16TX1 [29,30], means that LKB1 can affect Everolimus efficacy.
30
.
Figure 10 Pho-4EBP1 and pho-S6K1 might be impacted not only by
AKT/mTOR but also by another target or pathway.
Figure 11 The expression of pho-GSK3β (a) IF relative intensity (b) western blot with ponceau s solution, which shows the total protein (c) western blot with beta-actin. It
indicates that the expression of pho-AKT cannot represent the resistance of
Everolimus.
32
Figure 12 LKB1 expression for cell lines and PDCC (a) The IF image for MCF7 and ABC-16TX1 cells (b) quantifies intensities for IF signals. (c) The western bolt expression of LKB1 for cell lines. It shows that Everolimus-sensitive cells has the
higher LKB1 IF intensity than Everolimus-resistant cells.
3.3 Combined IF expression of pho-4EBP1 and pho-S6K1 before and after adding Everolimus
When staining some cell lines, for instance, MCF7, it will have the fundamental IF signals of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424. It is important to check these signals are the right signals we want. To prove this result, we add Everolimus 500 nM after about 24hours and stain with pho-4EBP1 and pho-S6K1 antibody.
Figure 13 shows the combined expression of pho-4EBP1 and pho-S6K1 for Everolimus-sensitive cells (MCF7, BT474) and Everolimus-resistant cells (MDA-MB-231, ABC-16TX1) for both control group and with Everolimus 500nM after 24 hours. Figure 13(a) represents the signals of MCF7 are decreased after adding Everolimus. Figure 13(b) represents the signals of BT474 cell line in Everolimus 500nM group are higher than control group. Figure 13(c) shows that the signals of Everolimus-resistant cells are the same and it is obvious that
34
MDA-MB-231 cell line and ABC-16TX1 cells are Everolimus-resistant cells.
BT474 cell line also has the higher resistance than MCF7 cell line. These results also maybe be related to the expression of pho-GSK3β and negative feedback of pho-AKT. If cells have some characteristics of resistance in Everolimus- sensitive cells, the dynamitic change for pho-4EBP1 and pho-S6K1 will happen.
For Everolimus-resistant cells, the expression of pho-4EBP1 and pho-S6K1 will almost unchanged. These results also show that signals are right in our research.
Figure 13 Combined expression of pho-4EBP1 and pho-S6K1 for both control group and Everolimus 500nM group for 24 hours (a) MCF7 cell line (b) BT474 cell line (c) MDA-
MB-231 cell line and ABC-16TX1 PDCC.
3.4 Epithelial-mesenchymal transition state and Everolimus sensitivity
The efficacy of Everolimus is believed to be affected by the cellular program EMT [12]. We used an EMT marker (vimentin) to interrogate this understanding.
Figure 14 represents results for four cell types. The expression of vimentin is negative for BT474 and MCF7, which are sensitive to Everolimus. The expression is positive for the other cells such as MDA-MB-231 and ABC-16TX1 which are resistant to Everolimus. This results explain the positive relation between EMT state and the efficacy of Everolimus. However, this vimentin results still do not list the sensitivity of Everolimus in order.
36
Figure 14 The IF expression of vimentin for cell lines. Red ones represent Vimentin signals and blue ones represent the nucleus signals. The positive relation between
EMT state and the efficacy of Everolimus.
3.5 The arrangement of IF marker in rare cancer cells detection
In order to use the pho-4EBP1 and pho-S6K1 IF marker into the application of rare cancer cells detection, we arrange the channels for these markers. In this section, MCF7 cell line will be the model of rare cancer cells.
The CD45 antibody will be placed in the location of the FITC channel, which distinguishes the white blood cells and rare cancer cells, meaning that the signals of white blood cells will be positive. The pan cytokeratin C11+AE1/AE3 antibody will be placed in the location of the PE channel, where it detects rare cancer cells. Pho-4EBP1-Thr37/46 add pho-S6K1 Ser424 antibody will be placed in the location of the APC channel. The stained Hoechst will also be used
to stand for the signal of the cell nucleus. Figure 15 shows the situation for MCF7 cell line in the blood and compares that for the white blood cells in healthy people. For white blood cells in healthy people, CD45 expression is positive, pan cytokeratin C11+AE1/AE3 expression is negative and the expression of pho- 4EBP1 and pho-S6K1 combined markers is positive. For MCF7 cell line, CD45 expression is negative, pan cytokeratin C11+AE1/AE3 expression is positive and the expression of pho-4EBP1 and pho-S6K1 combined markers is positive.
Figure 15 The arrangement of IF expression. (a) White blood cells in healthy people (b) MCF7 cell line. The expression of CD45 will be arranged in FITC channel, the expression of pan cytokeratin C11+AE1/AE3 will be arranged in PE channel and the
expression of pho-4EBP1+pho-S6K1 will be arranged in APC channel.
38
Chapter 4 Conclusions
This study shows that immunofluorescence analysis can be used to indicate the efficacy of mTOR inhibitor Everolimus on breast cancer cells (Hs578T, MCF7, BT474, MDA-MB-231) and patient-derived cell culture (ABC-82T, and ABC-16TX1). Immunofluorescence intensities of pho-4EBP1 Thr37/46 and pho-S6K1 Ser424 indicated that unlike each individual marker which does not correlate with efficacy in Everolimus, the combined IF intensity of these two proteins is representative of Everolimus efficacy. It also indicates that mTOR resistance might be affected not only by AKT/mTOR but also by LKB1 or MAPK/ERK pathway. In addition, the expression of LKB1 and pho- GSK3β might also be potential markers for efficacy of the therapeutic agent. In
many treatment cases, mTOR therapy is combined with hormonal drug e.g.
Tamoxifen. Hence it is important to understand the effect of Tamoxifen in the present IF analysis.
References
[1] DeSantis, C. E., et al. (2016). "Breast cancer statistics, 2015: Convergence of incidence rates between black and white women." CA Cancer J Clin 66(1): 31-42.
[2] Nole, F., et al. (2008). "Variation of circulating tumor cell levels during treatment of metastatic breast cancer: prognostic and therapeutic implications." Ann Oncol 19(5):
891-897.
[3] Nagrath, S., et al. (2007). "Isolation of rare circulating tumour cells in cancer patients by microchip technology." Nature 450(7173): 1235-1239.
[4] Bertoli, G., et al. (2015). "MicroRNAs: New Biomarkers for Diagnosis, Prognosis, Therapy Prediction and Therapeutic Tools for Breast Cancer." Theranostics 5(10):
1122-1143.
[5] Tomaskovic-Crook, E., et al. (2009). "Epithelial to mesenchymal transition and breast cancer." Breast Cancer Res 11(6): 213.
[6] Lamouille, S. and R. Derynck (2007). "Cell size and invasion in TGF-beta-induced epithelial to mesenchymal transition is regulated by activation of the mTOR pathway." Journal of Cell Biology 178(3): 437-451.
[7] Lamouille, S., et al. (2012). "TGF-beta-induced activation of mTOR complex 2 drives epithelial-mesenchymal transition and cell invasion." J Cell Sci 125(Pt 5): 1259-1273.
[8] Chao, S. K., et al. (2011). "Insights into 4E-BP1 and p53 mediated regulation of accelerated cell senescence." Oncotarget 2(1-2): 89-98.
[9] Feng, Z. and A. J. Levine (2010). "The regulation of energy metabolism and the IGF- 1/mTOR pathways by the p53 protein." Trends Cell Biol 20(7): 427-434.
[10] Polunovsky, Vitaly A., Houghton, Peter J. (2010). " mTOR Pathway and mTOR Inhibitors in Cancer Therapy. " Cancer Drug Discovery and Development.
40
[11] Weigelt, B., et al. (2011). "PIK3CA mutation, but not PTEN loss of function, determines the sensitivity of breast cancer cells to mTOR inhibitory drugs." Oncogene 30(29): 3222-3233.
[12] Holder, A. M., et al. (2015). "Epithelial to mesenchymal transition is associated with rapamycin resistance." Oncotarget 6(23): 19500-19513.
[13] Noh, W. C., et al. (2004). "Determinants of rapamycin sensitivity in breast cancer cells." Clin Cancer Res 10(3): 1013-1023.
[14] Hurvitz, S. A., et al. (2015). "In vitro activity of the mTOR inhibitor everolimus, in a large panel of breast cancer cell lines and analysis for predictors of response." Breast Cancer Res Treat 149(3): 669-680.
[15] Kang, S. A., et al. (2013). "mTORC1 phosphorylation sites encode their sensitivity to starvation and rapamycin." Science 341(6144): 1236566.
[16] Treilleux, I., et al. (2015). "Translational studies within the TAMRAD randomized GINECO trial: evidence for mTORC1 activation marker as a predictive factor for everolimus efficacy in advanced breast cancer." Ann Oncol 26(1): 120-125.
[17] Faes, S., et al. (2017). "Resistance to mTORC1 Inhibitors in Cancer Therapy: From Kinase Mutations to Intratumoral Heterogeneity of Kinase Activity." Oxidative Medicine and Cellular Longevity.
[18] Mohseni, M. and B. H. Park (2010). "PIK3CA and KRAS mutations predict for response to everolimus therapy: now that's RAD001." Journal of Clinical Investigation 120(8): 2655-2658.
[19] Choo, A. Y., et al. (2008). "Rapamycin differentially inhibits S6Ks and 4E-BP1 to mediate cell-type-specific repression of mRNA translation." Proc Natl Acad Sci U S A 105(45): 17414-17419.
[20] Gerdes, M. J., et al. (2013). "Highly multiplexed single-cell analysis of formalin-
fixed, paraffin-embedded cancer tissue." Proc Natl Acad Sci U S A 110(29): 11982- 11987.
[21] Leroy, C., et al. (2016). "Activation of IGF1R/p110beta/AKT/mTOR confers resistance to alpha-specific PI3K inhibition." Breast Cancer Res 18(1): 41.
[22] Karthik, G. M., et al. (2015). "mTOR inhibitors counteract tamoxifen-induced activation of breast cancer stem cells." Cancer Lett 367(1): 76-87.
[23] Satheesha, S., et al. (2011). "Response to mTOR inhibition: activity of eIF4E predicts sensitivity in cell lines and acquired changes in eIF4E regulation in breast cancer."
Mol Cancer 10: 19.
[24] Riquelme, I., et al. (2016). "The Gene Expression Status of the PI3K/AKT/mTOR Pathway in Gastric Cancer Tissues and Cell Lines." Pathol Oncol Res 22(4): 797-805.
[25] Rodrik-Outmezguine, V. S., et al. (2016). "Overcoming mTOR resistance mutations with a new-generation mTOR inhibitor." Nature 534(7606): 272-276.
[26] Xu, J., et al. (2016). "Mechanistically distinct cancer-associated mTOR activation clusters predict sensitivity to rapamycin." J Clin Invest 126(9): 3526-3540.
[27] Koo, J., et al. (2015). "GSK3 is required for rapalogs to induce degradation of some oncogenic proteins and to suppress cancer cell growth." Oncotarget 6(11): 8974-8987.
[28] McCubrey, J. A., et al. (2014). "GSK-3 as potential target for therapeutic intervention in cancer." Oncotarget 5(10): 2881-2911.
[29] Chen, I. C., et al. (2016). "Clinical Relevance of Liver Kinase B1(LKB1) Protein and Gene Expression in Breast Cancer." Scientific Reports 6.
[30] Li, J., et al. (2014). "Loss of LKB1 disrupts breast epithelial cell polarity and promotes breast cancer metastasis and invasion." J Exp Clin Cancer Res 33: 70.
[31] Liu, W., et al. (2017). "Quantitative proteomics profiling reveals activation of mTOR pathway in trastuzumab resistance." Oncotarget.
42
[32] Yoon, S. O. and P. P. Roux (2013). "Rapamycin resistance: mTORC1 substrates hold some of the answers." Curr Biol 23(19): R880-883.
[33] Saran, U., et al. (2015). "Cellular and molecular effects of the mTOR inhibitor everolimus." Clin Sci (Lond) 129(10): 895-914.