Retrospective Study using Magnetic Resonance Imaging (MRI) to Measure Depths of Acupuncture Points in Neck and Shoulder Region
Pei-Chi Chou
1,2, Yu-Chuen Huang
1,3, Chun-Jen Hsueh
4,5, Jaung-Geng Lin
1, Heng-Yi
Chu
*51
School of Chinese Medicine, College of Chinese Medicine, China Medical
University, Taichung, Taiwan.
2
Department of Traditional Chinese medicine, China Medical University Hospital
Eastern Branch, Taichung, Taiwan.
3
Department of Medical Research, China Medical University Hospital, Taichung,
Taiwan.
4
Department of Medical Imaging, Changhua Christian Hospital, Changhua, Taiwan.
5
Department of Physical Medicine and Rehabilitation, Tri-Service General Hospital,
National Defense Medical Center, Taipei, Taiwan.
Corresponding author: Heng-Yi Chu
No.325,Sec.2,Chenggong Rd.,Neihu District,Taipei City 114,Taiwan(R.O.C) [email protected]
Ph: +886-936276963
Ethics approval: Tri-Service General Hospital, National Defense Medical Center
Key words:
acupuncture, magnetic resonance imaging (MRI), acupuncture safety, needling depth Word count: 5008
ABSTRACT
Objectives
There are safety issues associated with acupuncture treatment. Previous studies
regarding needling depth of acupuncture points revealed inconsistent results due to vague depth definition, acupuncture point localization and measuring tools. The objective of this study is to find out and compare the differences of the mean depths of 11acupuncture points in the neck and shoulder region between subjects with
various variables including gender and body mass index (BMI).
Setting
This study was conducted at a single medical cernter in Taiwan.
Participants
Three-hundred and ninety four subjects were included in this study. Subjects were grouped according to gender and BMI. Acupuncture points were localized by WHO
standard and measured by MRI images.
Outcome measures
The distance from the needle insertion point (surface of the skin) to any tissues that
would cause possible/severe complications.
Results
Mean depths of 11 points were obtained in groups of different BMI and gender. Mean
depths of all subjects regardless of BMI and gender are as follows in centimeters: GB21=5.6,
SI14=5.2, SI15=8.8, GV15=4.9, GV16=4.6, GB20=5.0, ST9=1.6, SI16=1.8, SI17=2.4,
TE16=3.1, LI18=1.3. Subjects with higher BMI had greater measured depths in both gender
groups. Male subjects had larger mean depths than female subjects regardless of BMI except in
SI17 and LI18. When taking BMI into consideration, depths in male subjects are greater than in female subjects in most of the points except the following circumstances: GB21, TE16 in obesity group; ST9 in underweight and obesity group; SI16 in ideal body weight, overweight
and obesity group; SI17, LI18 in each group.
Conclusions
Subjects with higher BMI had greater measured depths and males tended to have greater depths in most of the points. Clinical practitioners are recommended to consider this
information to prevent complications when applying acupuncture treatment to their patients.
Article summary
Strengths of this study
※ The first study to investigate the depths of acupuncture points in neck and shoulder
regions using MRI
※ Acupuncture points were localized by WHO standard.
※ This study consists of the most subjects among similar existing studies regarding
measuring depths of acupoints Limitations of this study
※ Not able to analyze variables other than gender and BMI that may affect needling depth
such as age, diagnosis, neck girth and side difference.
INTRODUCTION
Acupuncture has generally been regarded as a relatively safe therapy method by many practitioners of complementary and alternative medicine (CAM) and most patients as Witt et al reported.[1] White et al meta-analyzed reports of adverse effects associated with acupuncture and concluded that the risk of serious events occurring in association with acupuncture is very low. [2]
However, numerous risks associated with this treatment method still exist and some of them could be clinically serious problems. Therefore, we should pay more attention to the safety issues of acupuncture treatment. [3]
Ancient Chinese classics and historical texts such as Huangdi Neijing have documented the adverse effects of acupuncture. For example, deep insertion at the acupuncture point Qupen (ST12) may cause dyspnea, cough, and even collapse of the lung.
Most of the reported adverse events were minor complications such as
needling pain, cutaneous disorders, hematoma, hypotension, nausea, vomiting, and fainting.[1] McPherson reported that a range of ‘negative’ reactions
including tiredness, drowsiness were frequently reported[4] but these do not
prevent most patients seeking further acupuncture and acupuncture is a
relatively safe intervention when practiced by regulated practitioners.[5]
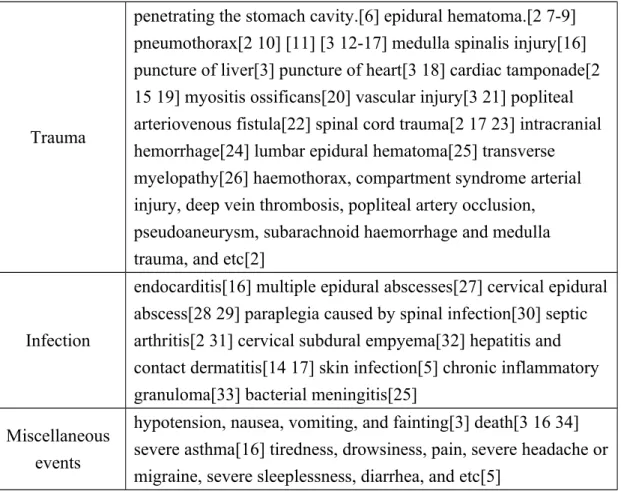
Complications in acupuncture practice may result from violations of sterile procedure and/or negligence of the practitioners. Common adverse events associated with acupuncture treatment are listed in table 1. Some events,
specifically trauma and infections, are likely to be avoidable.[2]
Table 1. Type of adverse events of acupuncture
Trauma
penetrating the stomach cavity.[6] epidural hematoma.[2 7-9]
pneumothorax[2 10] [11] [3 12-17] medulla spinalis injury[16]
puncture of liver[3] puncture of heart[3 18] cardiac tamponade[2 15 19] myositis ossificans[20] vascular injury[3 21] popliteal arteriovenous fistula[22] spinal cord trauma[2 17 23] intracranial hemorrhage[24] lumbar epidural hematoma[25] transverse myelopathy[26] haemothorax, compartment syndrome arterial injury, deep vein thrombosis, popliteal artery occlusion, pseudoaneurysm, subarachnoid haemorrhage and medulla trauma, and etc[2]
Infection
endocarditis[16] multiple epidural abscesses[27] cervical epidural abscess[28 29] paraplegia caused by spinal infection[30] septic arthritis[2 31] cervical subdural empyema[32] hepatitis and contact dermatitis[14 17] skin infection[5] chronic inflammatory granuloma[33] bacterial meningitis[25]
Miscellaneous events
hypotension, nausea, vomiting, and fainting[3] death[3 16 34]
severe asthma[16] tiredness, drowsiness, pain, severe headache or migraine, severe sleeplessness, diarrhea, and etc[5]
Pneumothorax has been reported as the most frequent adverse effect
associated with death. However, it is also the most frequent of all serious,
nonfatal complications of acupuncture. [14] Injuries of the organs and tissues
or even deaths would have been avoidable with a better understanding of
insertion, especially in points with higher needling frequency.
As many mentioned injuries of lung, heart, nerves and vessels occur in the points scattered in neck and shoulder regions. In this study, we focused on the investigation of 11 points with the depths actually measured on MRI in these areas. They are GV15(Yamen), GV16(Fengfu) , GB20(Fengchi),
GB21(Jianjing), SI14(Jianwaishu), SI15(Jianzhongshu), SI16(Tianchuang),
SI17(Tianrong), TE16(Tianyou), ST9(Renying) and LI18(Futu).
We would also like to understand how some variables such as body size and gender would affect the measured depth of each point, so we used Body mass
index (BMI) as the index for grouping of subjects in the current study.
Most of the previously conducted studies regarding acupuncture needling depth used computed tomography (CT) as the measuring tool[35]. In this
investigation, we used magnetic resonance imaging (MRI) as a measuring tool due to its excellent soft tissue contrast and multiplanar imaging capability.[36]
The objective of this study is to find out the mean distances from the skin
surface to the major organs of 11 acupoints which would cause no harm during
the treatment of each point and to compare the differences between subjects
with various variables including gender and BMI.
Subjects and Methods Subjects
The images of the subjects aged more than 18 years old who underwent MRI examination for neck and/or shoulder region that covered the points in this study from 7
thJune 1999 to 9
thApril 2014 were collected from the Tri-Service General Hospital, Taipei, Taiwan. This study was approved by the Tri-Service General Hospital, National Defense Medical Center Institutional Review
Board.
These subjects had undergone MRI to evaluate conditions such as herniated intervertebral discs, compression fracture of cervical vertebrae, degenerative joint diseases and acute conditions such as pain or surgical emergencies, accidental injuries, infections and oncology diseases. Subjects with severe clinical condition such as tumor invasion, fractures of the associated region that may affect the measuring definition or accuracy on MRI were excluded. We also excluded subjects whose MRI images failed to be obtained on both sides.
Subject data such as gender, age, body length and weight were retrieved from the medical records. Subjects were divided into 4 groups according to BMI:
underweight (BMI<18.5), ideal bodyweight (BMI=18.5-22.9), overweight
(BMI=23-24.9) and obesity (BMI≧25).[37]
Methods
As terms like safe needling depth or dangerous needling depth are very confusing due to lack of unanimous agreement between investigators, we hereby define the term of depth as the distance measured from the surface of the skin of the acupoint to the adventitia of major vessels (such as internal jugular vein/artery and common carotid artery for GB20,SI17, TE16, ST9, LI18 and SI16), nerves/spinal cord(such as dura mater for GV15 and 16) or pleural membrane (such as for GB21, SI14 and SI15) accordingly; i.e.; the distance from the needle insertion point (surface of the skin) to any tissues that would cause possible/severe complications such as hemorrhage (i.e. vessels),
nerve injury (i.e. spinal cord) or organ damage (i.e. lung) if punctured.
The needling angle is perpendicular to the surface of the skin of each point.
Both sides were measured in every subject except for GV15 and GV16.
The selected acupuncture points in the neck and shoulder region are depicted
in Figure 1.
The MRI machine used from 7th June 1999 to 9th April 2014 were the GE Signa EXCITE HDx 1.5T, GE Signa Discovery 750 3T (General Electric, Fairfield, MRI, USA) and PHILIPS Achieva 1.5T(Koninklijke Philips
Electronics N.V.). All MRI images had been taken in the sagittal, coronal and
axial planes. Neck images were obtained from the occipital level to two sections below the T2-3 vertebrae and the total field of view is about 25 cm.
The section thickness between each image was 1.1 to 5-6 mm on each plane.
Depth was measured on MRI images displayed on a PACS (Picture Archiving and Communication System; Centricity CSR4, General Electric,Fairfield, CT, USA) system for imaging. One of the authors who has been specialized in imaging of neural systems for 15 years was in charge of the measurement. The localization of each point was according to the suggestions from WHO
standard acupuncture locations.[38]
Statistical analysis
Demographic data of subjects were presented as mean ± standard deviation (SD) for continuous variables and percentage for categorical variables.
Student’s t test was used to determine the differences between the male and
female group. Analysis of variance (ANOVA) test or Brown-Forsythe test was
used to determine the differences among the four BMI groups (underweight,
ideal body weight, overweight, and obesity group). Simple linear regression
was used to predict the depth of needling acupoints by BMI. A p-value of <
0.05 was considered statistically significant. Statistical analyses were
done using the Statistical Package for the Social Sciences software package, v18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
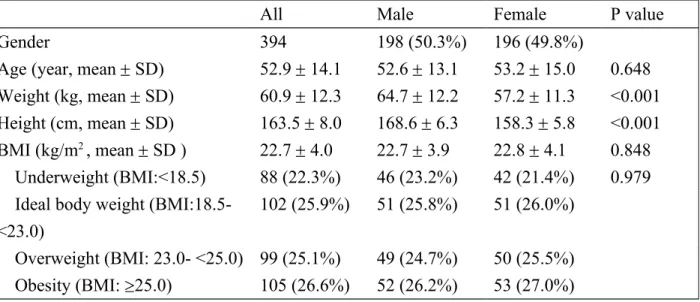
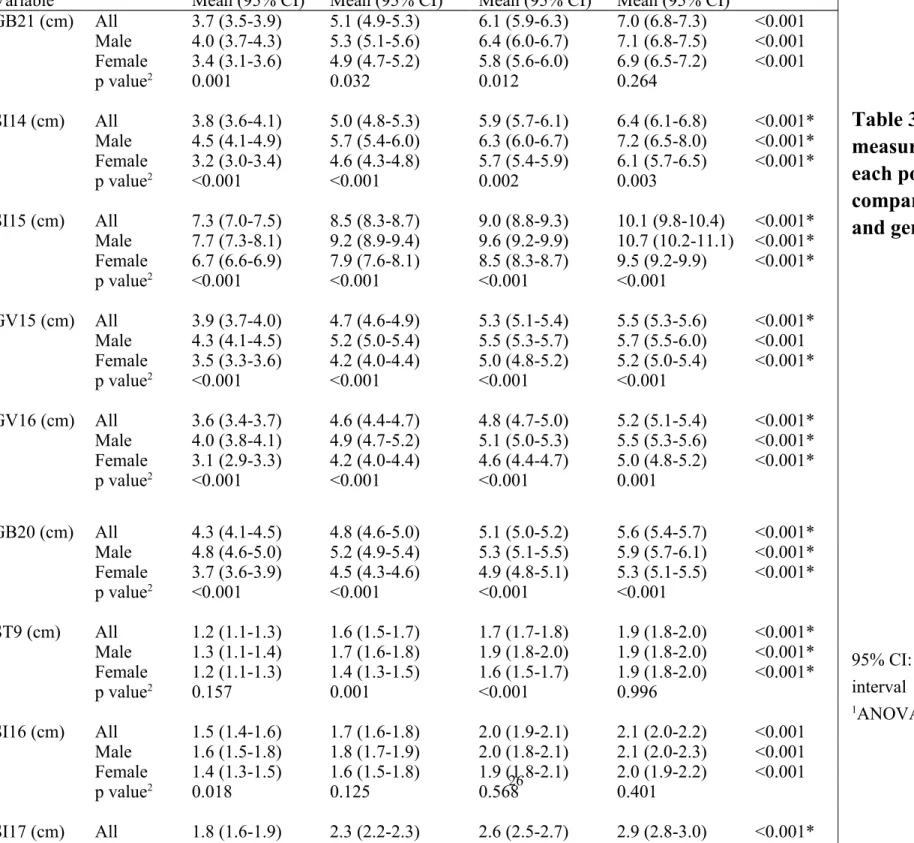
The images of 798 subjects were reviewed but only the images of 394 subjects were included in this study with 198 male subjects and 196 female subjects. Male subjects are taller and heavier than female ones. Mean age and BMI does not differ in 2 groups. There are 88 subjects in underweight group, 102 subjects in ideal bodyweight group, 99 subjects in overweight group and 105 subjects in obesity group. Details of demographic data are shown in table 2. Mean measured depth of each point among different BMI groups and
genders are shown in table 3. Mean measured depths of the 11 acupoints for all subjects regardless of BMI and gender are as follows in centimeters:
GB21=5.6, SI14=5.2, SI15=8.8, GV15=4.9, GV16=4.6, GB20=5.0, ST9=1.6, SI16=1.8, SI17=2.4, TE16=3.1, LI18=1.3. Generally speaking, male subjects had larger mean depths than female subjects regardless of BMI except in SI17 and LI18. From the perspective of BMI, the subjects with greater BMI had larger mean depths as details delineated in table 3.
. BMI is a very significant factor affecting measured depth in every point.
The measured depth of every point significantly correlated with the increase in
BMI. Depths in male subjects are greater than in female subjects in most of the
points except the following circumstances: GB21, TE16 in obesity group; ST9
in underweight and obesity group; SI16 in ideal body weight, overweight and
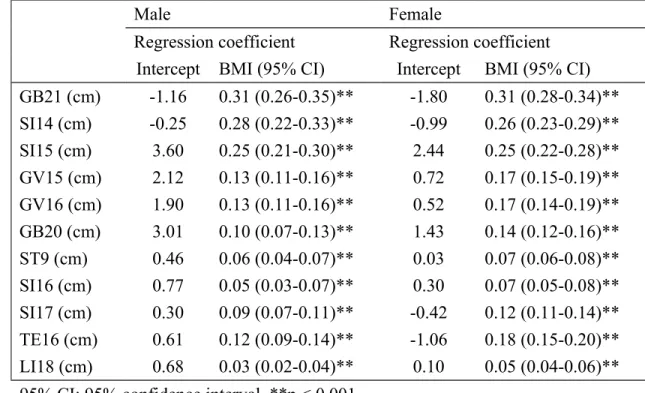
obesity group; SI17, LI18 in each group. We also show the results of regression
analysis on BMI and depth of each acupoint for male and female subjects
respectively in table 4 for prediction of the mean needling depth. The mean
predicted needling depth of each point in male subjects tends to be greater than
in female subjects.
DISCUSSION
To our knowledge, this is the first study to investigate the mean depths of acupuncture points in neck and shoulder regions using MRI and locating the acupoints according to the standard methods by WHO. This study also consists
of the most subjects among all existing studies regarding needling depth.
Most studies regarding safe/dangerous needling depth of acupuncture points used dissections from the cadavers which may be different from the real
situation.[35] Other investigations used CT scan as the imaging tool for depth measurement. There was a great inconsistency among those depths measured by different methods. For example, the suggested safe needling depths for GV16 are 27.73-33.39 mm(using CT images), 40.08 mm(using dissected specimens), and 43.46-57.42 mm(using dissected specimens) respectively.[35]
In this study, we selected MRI as the measuring tool. The major advantages of MRI over CT are primarily superior contrast resolution and better soft tissue
differentiation. [39] [40-42]
The other advantage of MRI is the ability to change the contrast of the images on PACS and possible to combine the different imaging planes for better acupuncture point localization.
We selected points in the neck and shoulder region and some are frequently
needled while with potential danger during needling. SI14 and SI15 were picked as not protected by scapula in the posterior shoulder region. The needling angle and direction also makes GB21 a candidate for lung injury.
Although external jugular vein can be easily dodged by careful inspection of the region close to points like GB20,SI17, TE16, ST9, LI18 and SI16, major vessels (such as internal jugular vein/artery and common carotid artery ) were
the main objects to avoid.
There is no unanimous definition of dangerous depth, safe depth or
therapeutic depth for each acupuncture point. Most of the authors chose 75% or 80% of the measured depths from their clinical experience. Moreover, from the clinical experience, most of the points are needled at the angle perpendicular to the skin surface, there is no universal needling angle in each point either, mostly resulting from the complex anatomical structures respectively.[35]
Different needling angle may actually cause different measured depth in each
point.
We hereby define the depth by documenting the measured distance from the
skin surface to major vessels, nerves or any organ such as lung under the
perpendicular needling angle. In the present study, we have successfully
reviewed and measured the MRI images of 394 patients; the mean depth of
each point was obtained. We also analyzed the variables including BMI and gender, and we obtained the corresponding mean depth in each subgroup. Both MRI and gender would affect the measured depth significantly. Regression analysis on BMI and depth of each point for male and female subjects was
done for further reference.
BMI is widely used as an international index for assessment of obesity of
adults in Taiwan and other Asian countries.[37] Its validity makes it an useful
tool for comparisons among subjects with different body sizes.[43 44]
Only one research used BMI to compare subjects’ needling depths. Nearly all parameters (interscapular distance, soft tissue thickness) correlated with the
BMI in acupoints BL25 and BL26 .[45]
Subjects with greater BMI had more adipose tissue in the body theoretically which results in thicker limbs and broader neck or shoulder girdle. As a result, in this study subjects with greater BMI had greater measured depth in all the points in this investigation. Neck circumference (NC) may play a role in
determining needling depth in points around the neck. Ben-Noun et al indicated a significant association between NC and: BMI, age, weight and waist
circumference. [46] Onat et al suggested that NC can be served as a useful
measure of central obesity, i.e., subjects with greater BMI may have greater NC
which leads to greater needling depth in the neck region.[47]
With the increase of BMI, lung volume may also be reduced and this probably leads to greater needling depth in the shoulder region such as in
GB21, SI14 and SI15.[48]
Male subjects had larger BMI than female subjects in this investigation. Male subjects were also heavier and higher even with the same BMI. In most of the points, regardless of BMI difference, male subjects tended to have greater measured depth as compared to female subjects. However, this lacks
consistency in points such as ST9, SI16, SI17 and LI18. This fact raises the
question: Why is there gender difference in certain points? Sexual dimorphism
of body composition should be taken into consideration. Several researches
revealed the difference of body fat distribution between different genders. They
may partially explain the observed facts. Whittle et al has pointed out that there
was no clear correlation between the volume of the soft tissue and fat in neck
region, especially when considering gender difference. [49] Wells et al
indicated that there are differences in terms of fat volume and distribution
between adult males and females. [50] There is also a sex difference in the
regional fat distribution. Women have more subcutaneous fat, whereas men
have more visceral fat. [51] So the depth in certain neck acupuncture points may
not show significant difference as expected in the limbs or the chest region
between different genders.[35]
Points with lesser mean values of measured depth such as SI16, SI17, SI18 and LI18 tend to have much less gender difference. Points of GV and CV tend to have less gender difference as well .[35] The measrued depths of points around the neck region were related to NC. Dancey et al indicated that men had significantly larger NC than women, but the difference became much less pronounced when normalized NC to body height.[52] This fact may reduce the gender difference to some extent. Another study also points out that there is an inverse association between upper airways size and both adiposity and visceral fat distribution in women which means that obesity is not necessarily the only factor affecting the distance from skin to major vessels inside the neck. [53] In addition, females have smaller carotid arteries even after adjusting for body and neck size, age, and blood pressure; this may also lead to the increase of the
measured depth.[54]
All these facts may cause some disparity of measured depth in certain points between different genders and among different body sizes. Clinical
practitioners should take more caution needling these points with less gender
difference. They could also refer to table 4 for predicted mean needling depth
of each point as predicted by regression analysis.
Limitations
In this study, we were not able to analyze the depth difference by different ages, diagnoses. Very few studies mentioned the side difference. One study indicated that right side BL13 points seems to be deeper, especially in thinner people.[35] BMI cut-off point for subjects grouping may need further
discussion and if we prefer FMI (fat mass index) or FFMI (fat-free mass index)
than BMI .
We can also take the measurement of neck and/or waist girth into
consideration for it is a simple anthropometric measure and a good indicator of
central obesity.
Measurement of more points of different region of body is undergoing and
will be disclosed later.
Future study design may be improved by the following suggestions:
Firstly, factors other than gender and BMI, such as age, body sides, diagnoses and different measuring methods should be controlled as much as possible.
Secondly, prospective in vivo research is better than retrospective images or
specimen dissections. Thirdly, multi-center collaboration should be encouraged
documented on ancient writings.
CONCLUSION
Mean measured depths of 11 acupuncture points around the neck and shoulder region were obtained in different groups of subjects classified according to BMI and sex. Subjects with higher BMI had greater depths and males tended to have greater depths in most of the points. Clinical practitioners are recommended to consider this information to prevent complications when applying acupuncture treatment to their patients.
Contributorship statement
Pei-Chi Chou came up with the idea of measuring the appropriate needling depth using MRI images. Pei-Chi Chou and Heng-Yi Chu were responsible for the study design, literature review, data collection and the writing of the manuscript. Chun-Jen Hsueh was responsible for the measurement of the needling depth via MRI images.
Yu-Chuen Huang was responsible for the statistical analysis of the data and wrote the statistics part of the manuscript. Jaung-Geng Lin was responsible for protocol
modification.
Competing interests: None
Funding
This study is supported by China Medical University, Taichung Taiwan (CMU102-N-10), and in part by Taiwan Ministry of Health and welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-
113002).
Data sharing statement: No additional data available.
Fig1. Selected Acupuncture points: the 11 selected acupuncture points in the neck and shoulder region.
REFERENCES
1. Witt CM, Pach D, Brinkhaus B, et al. Safety of acupuncture: results of a
prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forschende Komplementarmedizin (2006) 2009;16(2):91-7 doi: 10.1159/000209315[published Online First: Epub Date]|.
2. White A. A cumulative review of the range and incidence of significant adverse events associated with acupuncture. Acupunct Med 2004;22(3):122-33 3. Ernst E. Fatalities after CAM: an overview. Br J Gen Pract 2011;61(587):404-5
doi: 10.3399/bjgp11X578070[published Online First: Epub Date]|.
4. MacPherson H, Thomas K. Short term reactions to acupuncture--a cross-sectional survey of patient reports. Acupuncture in medicine : journal of the British Medical Acupuncture Society 2005;23(3):112-20
5. Macpherson H, Scullion A, Thomas KJ, et al. Patient reports of adverse events associated with acupuncture treatment: a prospective national survey. Qual Saf Health Care 2004;13(5):349-55 doi: 10.1136/qhc.13.5.349[published Online First: Epub Date]|.
6. Lee SW, Ahn JY, Choi WJ, et al. A needle penetrating the stomach cavity after
acupuncture. Clin Endosc 2014;47(3):258-61 doi:
7. Lee JH, Lee H, Jo DJ. An acute cervical epidural hematoma as a complication of dry needling. Spine (Phila Pa 1976) 2011;36(13):E891-3 doi:
10.1097/BRS.0b013e3181fc1e38[published Online First: Epub Date]|.
8. Eftekhar B, Ketabchi E, Ghodsi M, et al. Lumbar epidural hematoma due to lumbar acupunctures. Neurol India 2005;53(2):245-6
9. Chen JC, Chen Y, Lin SM, et al. Acute spinal epidural hematoma after acupuncture. J Trauma 2006;60(2):414-6; discussion 16 doi:
10.1097/01.ta.0000203541.49062.64[published Online First: Epub Date]|.
10. Conway N, Sreenivasan S. The acupunctured lung. Am J Emerg Med
2014;32(1):111.e1 doi: 10.1016/j.ajem.2013.08.026[published Online First:
Epub Date]|.
11. Tagami R, Moriya T, Kinoshita K, et al. Bilateral tension pneumothorax related to acupuncture. Acupunct Med 2013;31(2):242-4 doi: 10.1136/acupmed-2012- 010284[published Online First: Epub Date]|.
12. Ding M, Qiu Y, Jiang Z, et al. Acupuncture-associated pneumothorax. J Altern Complement Med 2013;19(6):564-8 doi: 10.1089/acm.2011.0495[published Online First: Epub Date]|.
13. Su JW, Lim CH, Chua YL. Bilateral pneumothoraces as a complication of acupuncture. Singapore Med J 2007;48(1):e32-3
14. Lao L, Hamilton GR, Fu J, et al. Is acupuncture safe? A systematic review of case reports. Altern Ther Health Med 2003;9(1):72-83
15. Peuker ET, White A, Ernst E, et al. Traumatic complications of acupuncture.
Therapists need to know human anatomy. Arch Fam Med 1999;8(6):553-8 16. Norheim AJ. Adverse effects of acupuncture: a study of the literature for the years
1981-1994. J Altern Complement Med 1996;2(2):291-7
17. Lao L. Safety issues in acupuncture. J Altern Complement Med 1996;2(1):27-31 18. Song BG, Park JR. Acupuncture needles over the myocardium. Heart Lung Circ
2010;19(8):480 doi: 10.1016/j.hlc.2009.10.010[published Online First: Epub Date]|.
19. Chun KJ, Lee SG, Son BS, et al. Life-threatening cardiac tamponade: a rare complication of acupuncture. J Cardiothorac Surg 2014;9:61 doi:
10.1186/1749-8090-9-61[published Online First: Epub Date]|.
20. Lee DG, Lee SH, Hwang SW, et al. Myositis ossificans in the paraspinal muscles of the neck after acupuncture: a case report. Spine J 2013;13(7):e9-e12 doi:
10.1016/j.spinee.2013.02.012[published Online First: Epub Date]|.
21. Wong YM, Hobara H. Hand acupuncture and vascular injury. J Nippon Med Sch
2012;79(4):246-7
fistula successfully treated with percutaneous endovascular intervention.
Kaohsiung J Med Sci 2010;26(3):158-62 doi: 10.1016/s1607-551x(10)70024- 3[published Online First: Epub Date]|.
23. Onda K, Honda H, Arai H, et al. [Dissociated sensory loss caused by acupuncture injury to the cervical spinal cord]. Brain Nerve 2008;60(10):1187-90
24. Choo DC, Yue G. Acute intracranial hemorrhage caused by acupuncture.
Headache 2000;40(5):397-8
25. Chen CY, Liu GC, Sheu RS, et al. Bacterial meningitis and lumbar epidural hematoma due to lumbar acupunctures: a case report. Kaohsiung J Med Sci 1997;13(5):328-31
26. Ilhan A, Alioglu Z, Adanir M, et al. Transverse myelopathy after acupuncture therapy: a case report. Acupunct Electrother Res 1995;20(3-4):191-4 27. Yu HJ, Lee KE, Kang HS, et al. Teaching NeuroImages: multiple epidural
abscesses after acupuncture. Neurology 2013;80(15):e169 doi:
10.1212/WNL.0b013e31828c2f1d[published Online First: Epub Date]|.
28. Lee JH, Cho JH, Jo DJ. Cervical epidural abscess after cupping and acupuncture.
Complement Ther Med 2012;20(4):228-31 doi:
10.1016/j.ctim.2012.02.009[published Online First: Epub Date]|.
29. Yazawa S, Ohi T, Sugimoto S, et al. Cervical spinal epidural abscess following acupuncture: successful treatment with antibiotics. Intern Med
1998;37(2):161-5
30. Bang MS, Lim SH. Paraplegia caused by spinal infection after acupuncture.
Spinal Cord 2006;44(4):258-9 doi: 10.1038/sj.sc.3101819[published Online First: Epub Date]|.
31. Daivajna S, Jones A, O'Malley M, et al. Unilateral septic arthritis of a lumbar facet joint secondary to acupuncture treatment--a case report. Acupunct Med 2004;22(3):152-5
32. Chen MH, Chen MH, Huang JS. Cervical subdural empyema following acupuncture. J Clin Neurosci 2004;11(8):909-11 doi:
10.1016/j.jocn.2004.02.011[published Online First: Epub Date]|.
33. Ha KY, Kim YH. Chronic inflammatory granuloma mimics clinical
manifestations of lumbar spinal stenosis after acupuncture: a case report.
Spine (Phila Pa 1976) 2003;28(11):E217-20 doi:
10.1097/01.brs.0000067278.67428.40[published Online First: Epub Date]|.
34. Ernst E. Deaths after acupuncture: A systematic review. The International Journal of Risk and Safety in Medicine 2010;22:131-36
35. Chou PC, Chu HY, Lin JG. Safe needling depth of acupuncture points. J Altern
Online First: Epub Date]|.
36. Li X, Ye Z. Magnetic resonance imaging features of alveolar soft part sarcoma:
report of 14 cases. World J Surg Oncol 2014;12:36 doi: 10.1186/1477-7819- 12-36[published Online First: Epub Date]|.
37. Anuurad E, Shiwaku K, Nogi A, et al. The new BMI criteria for asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. Journal of occupational health 2003;45(6):335-43
38. Organization WH. WHO Standard Acupuncture Point Locations in the Western Pacific Region, 2008.
39. Dirix P, Haustermans K, Vandecaveye V. The Value of Magnetic Resonance Imaging for Radiotherapy Planning. Semin Radiat Oncol 2014;24(3):151-59 doi: 10.1016/j.semradonc.2014.02.003[published Online First: Epub Date]|.
40. Totty WG, Murphy WA, Lee JK. Soft-tissue tumors: MR imaging. Radiology 1986;160(1):135-41
41. Sundaram M. MR Imaging of Soft Tissue Tumors: An Overview. Seminars in musculoskeletal radiology 1999;3(1):15-20 doi: 10.1055/s-2008-
1080048[published Online First: Epub Date]|.
42. Petasnick JP, Turner DA, Charters JR, et al. Soft-tissue masses of the locomotor system: comparison of MR imaging with CT. Radiology 1986;160(1):125-33 43. Mei Z, Grummer-Strawn LM, Pietrobelli A, et al. Validity of body mass index
compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. The American journal of clinical nutrition 2002;75(6):978-85
44. Komiya H, Masubuchi Y, Mori Y, et al. The validity of body mass index criteria in obese school-aged children. The Tohoku journal of experimental medicine 2008;214(1):27-37
45. Groenemeyer DH, Zhang L, Schirp S, et al. Localization of acupuncture points BL25 and BL26 using computed tomography. J Altern Complement Med 2009;15(12):1285-91 doi: 10.1089/acm.2007.7118-O[published Online First:
Epub Date]|.
46. Ben-Noun L, Sohar E, Laor A. Neck circumference as a simple screening measure for identifying overweight and obese patients. Obesity research
2001;9(8):470-7 doi: 10.1038/oby.2001.61[published Online First: Epub Date]|.
47. Onat A, Hergenc G, Yuksel H, et al. Neck circumference as a measure of central
obesity: associations with metabolic syndrome and obstructive sleep apnea
10.1016/j.clnu.2008.10.006[published Online First: Epub Date]|.
48. O'Donnell DE, Deesomchok A, Lam YM, et al. Effects of BMI on static lung volumes in patients with airway obstruction. Chest 2011;140(2):461-8 doi:
10.1378/chest.10-2582[published Online First: Epub Date]|.
49. Whittle AT, Marshall I, Mortimore IL, et al. Neck soft tissue and fat distribution:
comparison between normal men and women by magnetic resonance imaging.
Thorax 1999;54(4):323-8
50. Wells JC. Sexual dimorphism of body composition. Best practice & research Clinical endocrinology & metabolism 2007;21(3):415-30 doi:
10.1016/j.beem.2007.04.007[published Online First: Epub Date]|.
51. Nedungadi TP, Clegg DJ. Sexual dimorphism in body fat distribution and risk for cardiovascular diseases. Journal of cardiovascular translational research 2009;2(3):321-7 doi: 10.1007/s12265-009-9101-1[published Online First:
Epub Date]|.
52. Dancey DR, Hanly PJ, Soong C, et al. Gender differences in sleep apnea: the role of neck circumference. Chest 2003;123(5):1544-50
53. Busetto L, Calo E, Mazza M, et al. Upper airway size is related to obesity and body fat distribution in women. Eur Arch Otorhinolaryngol 2009;266(4):559- 63 doi: 10.1007/s00405-008-0773-y[published Online First: Epub Date]|.
54. Krejza J, Arkuszewski M, Kasner SE, et al. Carotid artery diameter in men and women and the relation to body and neck size. Stroke; a journal of cerebral circulation 2006;37(4):1103-5 doi:
10.1161/01.STR.0000206440.48756.f7[published Online First: Epub Date]|.
Table 2. Demographic data of subjects
All Male Female P value
Gender 394 198 (50.3%) 196 (49.8%)
Age (year, mean SD) 52.9 14.1 52.6 13.1 53.2 15.0 0.648 Weight (kg, mean SD) 60.9 12.3 64.7 12.2 57.2 11.3 <0.001 Height (cm, mean SD) 163.5 8.0 168.6 6.3 158.3 5.8 <0.001 BMI (kg/m
2, mean SD ) 22.7 4.0 22.7 3.9 22.8 4.1 0.848
Underweight (BMI:<18.5) 88 (22.3%) 46 (23.2%) 42 (21.4%) 0.979 Ideal body weight (BMI:18.5-
<23.0)
102 (25.9%) 51 (25.8%) 51 (26.0%)
Overweight (BMI: 23.0- <25.0) 99 (25.1%) 49 (24.7%) 50 (25.5%)
Obesity (BMI: 25.0) 105 (26.6%) 52 (26.2%) 53 (27.0%)
Table 3. Mean measured depth of each point
compared by BMI and gender
95% CI: 95% confidence interval
1
ANOVA test or Brown- Underweight Ideal body weight Overweight Obesity p value
1Variable Mean (95% CI) Mean (95% CI) Mean (95% CI) Mean (95% CI)
GB21 (cm) All 3.7 (3.5-3.9) 5.1 (4.9-5.3) 6.1 (5.9-6.3) 7.0 (6.8-7.3) <0.001 Male 4.0 (3.7-4.3) 5.3 (5.1-5.6) 6.4 (6.0-6.7) 7.1 (6.8-7.5) <0.001 Female 3.4 (3.1-3.6) 4.9 (4.7-5.2) 5.8 (5.6-6.0) 6.9 (6.5-7.2) <0.001
p value
20.001 0.032 0.012 0.264
SI14 (cm) All 3.8 (3.6-4.1) 5.0 (4.8-5.3) 5.9 (5.7-6.1) 6.4 (6.1-6.8) <0.001*
Male 4.5 (4.1-4.9) 5.7 (5.4-6.0) 6.3 (6.0-6.7) 7.2 (6.5-8.0) <0.001*
Female 3.2 (3.0-3.4) 4.6 (4.3-4.8) 5.7 (5.4-5.9) 6.1 (5.7-6.5) <0.001*
p value
2<0.001 <0.001 0.002 0.003
SI15 (cm) All 7.3 (7.0-7.5) 8.5 (8.3-8.7) 9.0 (8.8-9.3) 10.1 (9.8-10.4) <0.001*
Male 7.7 (7.3-8.1) 9.2 (8.9-9.4) 9.6 (9.2-9.9) 10.7 (10.2-11.1) <0.001*
Female 6.7 (6.6-6.9) 7.9 (7.6-8.1) 8.5 (8.3-8.7) 9.5 (9.2-9.9) <0.001*
p value
2<0.001 <0.001 <0.001 <0.001
GV15 (cm) All 3.9 (3.7-4.0) 4.7 (4.6-4.9) 5.3 (5.1-5.4) 5.5 (5.3-5.6) <0.001*
Male 4.3 (4.1-4.5) 5.2 (5.0-5.4) 5.5 (5.3-5.7) 5.7 (5.5-6.0) <0.001 Female 3.5 (3.3-3.6) 4.2 (4.0-4.4) 5.0 (4.8-5.2) 5.2 (5.0-5.4) <0.001*
p value
2<0.001 <0.001 <0.001 <0.001
GV16 (cm) All 3.6 (3.4-3.7) 4.6 (4.4-4.7) 4.8 (4.7-5.0) 5.2 (5.1-5.4) <0.001*
Male 4.0 (3.8-4.1) 4.9 (4.7-5.2) 5.1 (5.0-5.3) 5.5 (5.3-5.6) <0.001*
Female 3.1 (2.9-3.3) 4.2 (4.0-4.4) 4.6 (4.4-4.7) 5.0 (4.8-5.2) <0.001*
p value
2<0.001 <0.001 <0.001 0.001
GB20 (cm) All 4.3 (4.1-4.5) 4.8 (4.6-5.0) 5.1 (5.0-5.2) 5.6 (5.4-5.7) <0.001*
Male 4.8 (4.6-5.0) 5.2 (4.9-5.4) 5.3 (5.1-5.5) 5.9 (5.7-6.1) <0.001*
Female 3.7 (3.6-3.9) 4.5 (4.3-4.6) 4.9 (4.8-5.1) 5.3 (5.1-5.5) <0.001*
p value
2<0.001 <0.001 <0.001 <0.001
ST9 (cm) All 1.2 (1.1-1.3) 1.6 (1.5-1.7) 1.7 (1.7-1.8) 1.9 (1.8-2.0) <0.001*
Male 1.3 (1.1-1.4) 1.7 (1.6-1.8) 1.9 (1.8-2.0) 1.9 (1.8-2.0) <0.001*
Female 1.2 (1.1-1.3) 1.4 (1.3-1.5) 1.6 (1.5-1.7) 1.9 (1.8-2.0) <0.001*
p value
20.157 0.001 <0.001 0.996
SI16 (cm) All 1.5 (1.4-1.6) 1.7 (1.6-1.8) 2.0 (1.9-2.1) 2.1 (2.0-2.2) <0.001 Male 1.6 (1.5-1.8) 1.8 (1.7-1.9) 2.0 (1.8-2.1) 2.1 (2.0-2.3) <0.001 Female 1.4 (1.3-1.5) 1.6 (1.5-1.8) 1.9 (1.8-2.1) 2.0 (1.9-2.2) <0.001
p value
20.018 0.125 0.568
260.401
Forsythe test: determining the differences among different BMI groups.
*p-values were performed by Brown-Forsythe test
2