健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 摘要:
背景
影響睡眠的因素有許多,包含光線、醫療、噪音等因素,此種影響因素加護病房中皆有。研究指出約有 20%加護病房病人睡眠困難的原因為噪音,因噪音會抑制褪黑激素干擾睡眠,進而導致譫妄,譫妄會延長住 院時間,增加醫療負擔。亞急性呼吸照護中心,也出現相同的問題。
目的
探討將耳塞應用亞急性呼吸照護中心病人的睡眠品質照護。
方法
根據 PICO 的問題進行探討,提出 P:Intensive care unit patient(加護病房病人)、I:With earplugs
(使用耳塞)、C:Without earplugs(未使用耳塞)、O:Sleep quality and delirium incidence(睡眠品質 和譫妄發生),選用資料庫:Cochrance Library、Pub Med、CHINAL、華藝中文資料庫,年限為近五年,
文獻為最新,是一篇系統性回顧文章,將此篇評讀後運用在臨床,工具為耳塞,測量工具為查茲坎貝爾睡眠 量表(Richards-Campbell Sleep Questionnaire, RCSQ),測量時間包含四次,一次前測及三次後測。
結果
以 2011 年英國公共衛生資源部門發展的文獻評讀工具 Critical Appraisal Skills Programme (CASP)評 讀,10 項題目共有 7 項符合,並且將此應用在臨床,結果為使用耳塞後的三個晚上睡眠品質皆較前測(未使 用耳塞)的睡眠品質有明顯改善,但可以發現第一天晚上受測者使用耳塞睡眠品質有最顯著改善。
結論
日後的研究可以增加樣本數,或是使用不同材質的耳塞,將會造成不同的隔音效果,造成病人對睡眠品 質產生不同的差異。
關鍵字:亞急性呼吸照護中心、耳塞、睡眠品質
將耳塞應用亞急性呼吸照護中心病人的睡眠品質照護
施純瑩
1*、白香菊
21
中山醫學大學附設醫院護理部護理師
2中山醫學大學護理系副教授
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月
前言
睡眠在人類生命中扮演著極為重要的角色,具有 修復細胞及組織的功能(盧、解、陳、蘇、周、邱,
2014)。在加護病房中病人易有睡眠障礙的情形,影 響病人的睡眠型態,為加護病房中面臨頻繁的治療、
多種儀器的聲音、明亮的燈光,及心理壓力,都會造 成睡眠中斷(熊、張、周、邱,2009; Le et al., 2012;Alasad, Abu Tabar, & Ahmad, 2015)。有研 究顯示重症病人睡眠困難中約有 20%為噪音所引起 (Richard et al., 2003)。國際榮譽護理協會(Sigma Theta Tau International, 2004)曾提出對於實證護理 的定義,為涵蓋所有最佳證據及護理實務經驗,並重 視個人及所屬家庭及社區之價值及偏好的護理照護。
因此想藉由實證護理的應用,探討亞急性呼吸照護中 心病人夜間使用耳塞對譫妄及睡眠品質之影響。
重要文獻
(一) 噪音的介紹
噪音是指令人不悅耳、不舒服的聲音,甚至危害 人的身體健康,有文獻指出不愉快的聲音即為噪音
( 唐 、 董 、 羅 、 江 、 梁 , 2013 ; Johnson &
Thornhill, 2006 ; Pope, 2010) ,因此可了解噪音 為一種主觀的感受,及令人感到一種不安的聲音(黃、
黃、蕭、王,2004)。噪音對人體會造成很大的影 響,對於生理層面方面的影響,包含:聽力、心跳、
呼吸、睡眠、休息等。在心理層面方面也會造有諸多 負面影響。重症患者中約有 20%由睡眠中驚醒時為 由噪音而引發(Darbyshire &Young, 2013)。在 加護病房對於的噪音感受中,Aaron 等人 (1996)研 究顯示,加護病房中的噪音程度為 60 到 84 分貝,
當聲音超過 80 分貝,病人從睡眠中覺醒次數越多。
陳(2006)研究顯示,呼吸照護中心噪音為 60-63 分貝,約有 50%噪音來自於醫護人員的交談聲所致。
在加護單位中噪音為一種常見且不容忽視的問題,應 特別注意,需適當地處理,以避免對重症病人身心方 面帶來不好的感受(徐、黃,2007)。
(二)重症病人的睡眠品質
睡眠是人體生命中扮演著很重要的角色,是能量 的來源,及促進身體健康的要素(盧等,2014)。睡 眠品質為對於睡眠質性與量性綜合感受的自我評價,
並為判斷睡眠狀況的指標(邱、邱,2010)。由腦波 可了解,正常的睡眠週期可分為兩個階段,先由淺層 的 NREM 睡眠(第一、二期)開始,再進入深層的 REM 睡眠(第三、四期),此兩個階段會交替出現 (Carskadon & Rechtschaffen, 2005)。重症病人睡 眠時間,花費較多在 NREM 睡眠的第一期和第二期,
REM 的第三期及第四期的時間較短 (Freedman, Gazendam, Levan, Pack, & Schwab, 2001; Gabor Cooper, Crombach, Lee, Kadikar, Bettger, &
Hanley, 2003; Friese, Dias-Arrastia , McBride, Frankel , & Gentilello, 2007; Kudchadker, Sterni, Yaster, & Blaine Easley, 2009) ,此現象呈現出重症 病 人的睡 眠方 式為 淺 層睡 眠。 Simini(1991) 呈現 61% 的加護病房病人出現睡眠中斷,其睡眠中斷的 原因有許多,包含:陌生的醫院環境、疾病、情緒困 擾、疼痛,和需要 24 小時持續性的照護,而出現睡 眠剝奪的情形,且有 20%的加護病房病人造成睡眠 困難的因素為噪音(Williamson, 2002)。
(三)噪音對加護病房患者的影響
噪音會造成睡眠中斷、情緒感到緊張不安、工作 效率降低、疼痛的感受增加、傷口癒合不良等結果
(宋, 2012;唐等, 2013 ;Crawley & Emery,
2006; Pope, Gallun, & Kampel, 2013)。噪音為加 護病房環境中,干擾睡眠的最主要的因素,且有研究 顯示重症病患有 20%因為噪音的關係,亦讓病人由 睡眠中被驚醒 (Aaron et al.,1996; Darbyshire &
Young, 2013),因此顯示出噪音與睡眠有緊密的關係。
接受刊登:108 年 10 月 31 日
*通訊作者:施純瑩
機構:中山醫學大學附設醫院護理部 地址: 台中市南區建國北路一段 110 號
電話: 04-2473-9595 轉 32700 E-mail: [email protected]
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 Freedman 等人(1999)和方、王(2007)的研究顯示
,研究者自覺噪音與睡眠品質呈現負相關,表示噪音 越多,睡眠品質越差。加護病房中為了降低環境中的 噪音隔絕噪音的方法,由文獻查證中可以發現加護病 房中病人多以使用耳塞,當作降低噪音的方式,例如,
Hu 等人(2010)、Foreman 等人(2015)、Le 等人 (2014)的文獻中,皆呈現使用耳塞當作介入性的研究 中,可以改善睡眠品質。Van 等人(2012)此篇針對夜 間耳塞對重症單位病人的譫妄睡眠狀況的影響結果顯 示,於夜間第一個晚上使用耳塞相對於未使用耳塞病 人,近一半以上的病人呈現睡眠良好。
方法
(一)形成一個臨床可回答的問題
將 PICO 的關 鍵字, P:Intensive care unit patient(加護病房病人)、I:With earplugs(使用 耳 塞 ) 、 C:Without earplugs ( 未 使 用 耳 塞 ) 、 O:Sleep quality and delirium incidence(睡眠品質 和譫妄發生),組合排列成適當的關鍵字,先前因關 鍵 字 中 的 Sleep quality and delirium 和 Sleep quality and acute confusion 搜尋過程中,無法搜尋 到相關的文獻,因此將關鍵字修改為 Sleep and delirium 和 Sleep and acute confusion 。 利 用 MeSH terms 建立關鍵字,並且使用布林邏輯進行連 結 搜 尋 為 : ( P:Intensive care unit patient OR Critical care unit )AND (I 及 C: earplugs OR Ear protective devices OR Earmuffs)AND (O:Sleep and delirium OR Sleep and acute confusion)。
(二) 尋找最佳文獻證據
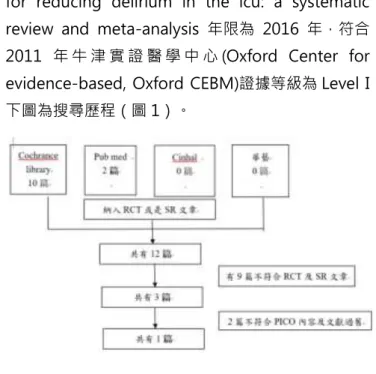
使用最佳搜尋資料庫,搜尋出來的文章為證據等 級較高的資料庫,為「Cochrance Library」,接下 來搜尋的資料庫分別為:Pub Med、CHINAL、華藝 中文資料庫。由 Cochrance Library 所搜尋出來的文 章因年現較舊,不予採用,由 Pub Med 搜尋出來的 文章共有兩篇其中一篇研究對象為小孩,最後搜尋為 Pub Med 資 料 庫 , 搜 尋 出 來 的 題 目 為 : The efficacy of earplugs as a sleep hygiene strategy
for reducing delirium in the icu: a systematic review and meta-analysis 年限為 2016 年,符合 2011 年 牛 津 實 證 醫 學 中 心 (Oxford Center for evidence-based, Oxford CEBM)證據等級為 Level I,
下圖為搜尋歷程(圖 1)。
圖 1 搜尋歷程
(三)評讀結果
採 用 英 國 公 共 衛 生 資 源 部 門 所 發 展 之 工 具 Critical Appraisal Skills Programme (CASP) 進行評 讀,2009 年至 2015 年間發表的九篇研究,共有 832 名參與者,由兩個森林圖呈現,使用耳塞導致譫 妄的情形較低,而且使用耳塞置導致死亡率也仍較低,
但此篇系統性回顧文獻中仍會擁有偏差的情形出現,
因為其中只有兩篇文獻納入儀器測量,呈現量化數據,
並且文獻中的研究都為小型的研究,較少為大型的研 究,這樣可能會高估治療效果及所呈現出來的研究結 果。以下表格為評讀結果如下表。
(四)將臨床專業與病人價值觀相結合
經過評論及分析統合後,發現有效的證據,並且 選用最佳的文獻證據,並經過臨床專家評估後,對於 選用耳塞的病人是否有危害,及評估病人的接受程度 後,對於病人做出最好的決策,因此決定使用耳塞當 作介入措施,並以中部某醫學中心亞急性呼吸照護中 心,我們使用耳塞當作介入措施,拿掉耳塞後進行後 測,共需連續監測病人三個晚上的睡眠狀況,總共需
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 要進行四次測量,並使用RCSQ量表當作測量工具。
表一 評讀結果
(五)評估執行效果及效用
此次於亞急性呼吸照護中心進行收案,但因亞 急性呼吸照護中心多為意識不清的患者,因此要符合 本研究的條件較少,因此最後只收了一名個案,總收 案人數為 1 人,運用 RCSQ 量表進行測量,此結果 採用 Excel 軟體進行繪製,我們可以發現使用 RCSQ 量表進行測量,發現前測各題的分數皆後測的分數為 低,我們可以由四次測量分數的群聚狀況(如圖 2)
發現,並且也可發現四次測量中的平均總分,以後測 的第一天分數最高,表示此病人在後測第一天的睡眠 品質較好(如圖 3)。
評讀項目 分析
評讀結果 Yes Can’t tell No 1. Did the review address a clearly
focused question?
裡面清楚呈現族群為加護病房病人、介入措施為耳塞、結果為譫妄、
死亡率。
v
2.Did the authors look for the right type of papers?
因裡面的文章中的表格呈現六篇 RCT 文章,但是內文裡面敘述中卻 只有 5 篇 RCT 文章,文中並未交代清楚。
v
3.Do you think all the important, relevant studies were included ?
裡面清楚的呈現關鍵字及資料庫的使用過程,但是裡面文章的收錄並 未有專家介入,而由兩位作者完完成,且裡面沒有詳細說明是否使用 其他語言,及尚未出版的文章。
v
4.Did the review’s authors do enough to assess the quality of the included studies?
裡面為使用 Cochrane Risk of Bias (RoB) Tool 將九篇文章進行評 讀。由兩位作者(E.L.,V.C.)完成。
v
5. If the results of the review have been combined was it reasonable to do so?
裡面以漏斗圖呈現合併後文章所分布的狀況,看起來分布過於鬆散。
文章中的第三個結果為使用耳塞是否能改善睡眠品質,因使用的睡眠 評估量表不同,因此異質性高為 99%。
v
6. What are the overall results of the review?
此篇文章作主要呈現的結果為譫妄,且結果使用相關風險評估 (relative risk,RR)。
v
7. How precise are the results? 所有的結果皆以信賴區間呈現。使用耳塞造成譫妄的相對風險 (relative risk,RR)為 0.59 異質性為 39%,95%信賴區間範圍為:
0.48-0.78,表示有顯著性。另一個結果為使用耳塞降低死亡率的相 對風險(RR)為 0.77,異質性為 48%,95%信賴區間範圍為:0.53- 1.11,表示無顯著性,此結果皆有清楚表達出。
v
8. Can the results be applied to the local population?
審查的患者可能與我所使用的人群無太大的差異,因此可以經此研究 結果做應用。
v
9. Were all important outcomes considered?
因文章中呈現死亡率,對於使用耳塞及未使用耳塞病人皆無顯著關 係,且文章 95%信賴區間為 0.53-1.11,表示仍可以思考是否有其他 臨床重要的因素,被排除。
v
10. Are the benefits worth the harms and costs?
此篇結果對於放置耳塞可以降低死亡率,無顯著差異,但改善睡眠品 質和降低入住加護病房的患者譫妄,減少進入加護病房的住院時間和 費用,這種方法可能是有價值的。
v
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 四、結論與討論
此次我們由臨床中找尋一個問題,並且經由實證 護理搜尋相關的文章。我們透過 PICO 呈現出問題,
並在資料庫中進行文獻搜尋,找出符合 PICO 問題的 文章,並檢視其內容,最後選定此篇文章後並進行評 讀,運用在臨床進行驗證。我們將此實證應用在一位 病人上,可以發現病人使用耳塞的三個晚上睡眠品質 平均分數均較高,表示睡眠品質皆有明顯的改善,與 Hu et al 等(2010)此篇耳塞和眼罩對重症單位環境中 夜間睡眠的影響,受病人的褪黑激素和皮質醇影響、
Foreman et al 等(2015)此篇睡眠在神經加護病房使 用環境和光補充褪黑激素,將睡眠量化及可行性、Le et al 等(2013)此篇耳塞和眼罩與常規護理可預防的睡
眠障礙在麻醉恢復室的狀況。我們應用的結果與以上 這些文章中所呈現的結果,使用耳塞後的睡眠品質較 沒有使用耳塞的睡眠品質狀況佳,因此可了解到結果 是一致的。且我們讓病人在夜間時使用耳塞觀察三個 晚上,可以發現使用耳塞後的第一天的睡眠品質較第 二天及第三天的睡眠品質為佳,此結果與 Van 等人 (2012) 此篇夜間使用耳塞對譫妄發作和睡眠知覺影 響的隨機對照試驗的結論是一致的。由此我們可以了 解到亞急性呼吸照護中心的患者使用耳塞,對於睡眠 品質的改善是有幫助的。日後我們建議讓在重症單位 的患者晚上睡覺時使用耳塞,增加睡眠品質。受限於 納入研究內之影響,未來擬提出更廣泛之具體應用,
需要未來執行更多嚴謹研究以豐富現存文獻。對於此 次使用耳塞可提升睡眠品質,進而減少譫妄,但因為 收案人數及收案地點的限制,無法對於使用耳塞減少 譫妄的部分進行評估,希望之後可以有較充足的收案 時間,擴大收案人數及收案地點,增加可信度。此次 介入措施為耳塞,且市面上的耳塞種類較多,且材質 的不同,皆會影響隔音效果,進而影響病人的睡眠品 質,希望未來可以探討及比較,不同材質的耳塞對於 病人的睡眠品質的狀況。
參考資料
方楸淑、王瑞霞(2007).外科加護病房病患睡眠品質 及其相關因素探討.實證護理,3(1),54-63。
宋秀琴、李敏靜、黃初雪 (2012).北部某醫學中心內科 病房環境噪音之改善方案.馬偕護理,6(2),37-47。
李淑燕(2008).睡眠臨床照護指引對改善外科重症加
護病房夜間睡眠環境與人睡眠品質之成效探討.國
立臺北護理健康大學護理研究所碩士論文,1-111。
林富美(2001).實證醫學與知識學習系統-實證護理發 展理念.取自 http://www1.wanfang.gov.tw/
ebm/03_ebn/01_intro.htm
邱曉彥、邱艷芬(2010).睡眠品質之概念分析.護理
雜誌,57(4),106-111。
唐秀燕、董婉君、羅映喬、江姿瑢、梁蕙芳 (2013).降 低某區域教學醫院外科病房噪音分貝量之行政專案.
長庚科技學刊,18,131-140。
徐愬美、黃秀梨 (2007).心臟手術後病人對加護單位 0
20 40 60 80 100
一 二 三 四 五 六
前測 後測第一天
後測第二天 後測第三天
0 10 20 30 40 50 60 70 80 90
前 測 後 測 第 一 天 後 測 第 二 天 後 測 第 三 天
平均分數 圖 2 四次測量的各項結果的比較
一:睡眠深度 五:睡眠品質
二:入睡狀況 六:昨晚病房噪音程度(護理人員) 三:被吵醒
四:回到睡眠
圖 3 四次測量的平均分數比較
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 噪音音量及來源之主觀感受.馬偕護理雜誌, 1(2),
31-40。
張靜雯(2005).重症單位老人壓力感受與相關因素及照
護需求之探討.中國醫藥大學護理研究所碩士論文,
1-125。
陳季涵、周幸生(2016).重症病人譫妄的群組照護.
領導護理雜誌,16(1),2-10。
陳靜如 (2006).呼吸照護中心呼吸器脫離訓練病患的睡
眠品質預測因素之探討.中國醫藥大學護理學系碩
士班學位論文,1-150。
黃麗玉、黃珊、蕭世槐、 王美文 (2004).南部某醫
學中心急診加護病房噪音改善方案.護理雜誌,
51(1), 58-69。
熊道芬、邱曉彥、邱艶芬(2007).加護單位病患睡眠 問題的護理挑戰.源遠護理,1(3),15-25。
熊道芬、張怡媛、周幸生、邱艶芬(2009).重症病人 睡眠品質及其影響因素之探討.榮總護理,26(3),
274-281。
盧淑芬、解玉珍、陳惠君、蘇惠文、周幸生、邱艷芬
(2014).某醫學中心音樂介入對於重症病人.榮 總護理,31(4),388-397。
Aaron, J. N., Carlisle, C. C., Carskadon, M. A., Meyer, T. J., Hill, N. S., & Millman, R. P. (1996). Environment noise as a cause of sleep disruption in an intermediate respiratory care unit. Sleep, 19(9), 707-710.
Alasad, J. A., Abu Tabar, N., & Ahmad, M. M. (2015).
Patients' experience of being in intensive care units.
Journal of Critical Care, 30(4), 859.e7-11.
Buysse, D. J., Reynolds III, C. F., Monk, T. H., Berman, S.
R., & Kupfer, D. J. (1989). The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry research, 28(2), 193- 213.
Carno, M. A., & Connolly, H. V. (2005). Sleep and sedation in the pediatric intensive care unit. Nursing Critical Care Clinics of North America, 17, 239-244.
Carskadon, M. A., & Rechtschaffen, A. (2005). onitoring and staging human sleep. In M. H.Kryger (Ed.), Principle and practice of sleep medicine, 2 ,1359-1377.
Çelik, S., Öztekin, D., Akyolcu, N., & İşsever, H.(2005).
Sleep disturbance: the patient care activities applied at the night shift in the intensive care unit. Journal of clinical nursing, 14(1), 102-106.
Cerejeira, J., Nogueira, V., Luis, P., Vaz-Serra, A., &
Mukaetova-Ladinska, E. B. (2012).The holinergic system and inflammation: common pathways in delirium pathophysiology. Journal of the American
Geriatrics society, 60(4), 669-675.
Chlan LL, Weinert CR, Heider scheit A, et al. (2013).
Effects of patient-directed music Intervention on anxiety and sedative exposure in critically ill patients receiving mechanical ventilator support: A randomized clinicaltrial. The Journal of the American Medical Association, 309, 2335-2344.
Critical Appraisal Skills Programme (2013). 10 questions to help you make sense of a review. Retrieved from http://www.caspuk.net/wp-
content/uploads/2011/11/CASPSystematic-Review- Checklist-31.05.13.pdf
Darbyshire, J. L., & Young, J. D. (2013). An investigation of sound levels on intensive care units with reference to the WHO guidelines. Critical Care, 17(5), R187.
Dines-Kalinowski, C. M. (2002). Nature s nurse: Promoting sleep in the ICU. Dimensions of Critical Care Nursing, 21(1), 32-35.
Ely, E. W., Shintani, A., Truman, B., Speroff, T., Gordon, S.
M., Harrell Jr, F. E., ... & Dittus, R. S. (2004).
Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. The Journal of the American Medical Association, 291(14), 1753-1762.
Foreman B, Westwood A J, Claassen J, et al. (2015). Sleep in the neurological intensive care unit: Feasibility of quantifying sleep after melatonin supplementation with environmental light and noise reduction. Journal of Clinical Neurophysiol, 32, 66-74.
Freedman, N. S., Kotzer, N., & Schwab, R. J. (1999).
Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit. American journal of respiratory and critical care medicine, 159(4), 1155-1162.
Francis, J., & Young, G. B. (2011). Diagnosis of delirium and confusional states. Up To Date, Rose, BD (Ed), Up To Date, Waltham, MA.
Freedman NS, Gazendam J, Levan L, Pack AI, Schwab RJ.
(2001). Abnormal sleep/wake cycles and the effect of environmental noise on sleep disruption in the intensive care unit. American Journal of Respiratory and Critical Care Medicine, 163, 451-457.
Friese RS, Dias-Arrastia R, McBride D, Frankel H,
Gentilello LM. (2007). Quantity and quality of sleep in the surgical intensive care unit: are our patients sleeping? The Journal of Trauma, 63, 1210-1214.
Gabor J, Cooper A, Crombach S, Lee B, Kadikar N, Bettger H, Hanley P. (2003). Contribution of the intensive care unit environment to sleep disruption in mechanically ventilated patients and healthy subjects. American journal respiratory critical care medicine, 167, 708- 715.
Gabor,J.Y.,Cooper,A.B.,Crombach,S.A.,Lee,B.,Kadikar,N., Bettger,H.E.,et al(2003).Contribution of the intensive care unit environment to sleep disruption in
mechanically ventilated patient and health subjects.
American journal of respiratory and critical care
健康照護科學雜誌 第 1 期 中華民國 109 年 2 月 medicine, 167(5),708-715.
Hu RF, Jiang XY, Zeng YM, et al. (2010). Effects of earplugs and eye masks on nocturnal sleep, melatonin and cortisol in a simulated intensive care unit
environment. Critical Care, 14, R66.
Johnson, P. R., & Thornhill, L. B. (2006). Noise reduction in the hospital setting. Journal of Nursing Care Quality, 21(4), 295-297.
Jones C, Dawson D. (2012). Eye masks and earplugs improve patient’s perception of sleep. Nursing in critical care, 17, 247-254.
Kamdar BB, King LM, Collop NA, et al (2013). The effect of a quality improvement Intervention on perceived sleep quality and cognition in a medical ICU. Critical care medicine, 41, 800-809.
Kamdar, B. B., Niessen, T., Colantuoni, E., King, L. M., Neufeld, K. J., Bienvenu, O. J., ... & Needham, D. M.
(2015). Delirium transitions in the medical ICU:
exploring the role of sleep quality and other factors. Critical care medicine, 43(1), 135.
Kress JP, Joffe AM. (2013). Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Critical care medicine; 41: 263-306.
Kudchadker S, Sterni L, Yaster M, Blaine Easley R. (2009).
Sleep in the intensive care unit. Contemporary critical care, 7, 1-12.
Le Guen M, Nicolas-Robin A, Lebard C, et al. (2013).
Earplugs and eye masks vs routine care prevent sleep impairment in post-anaesthesia care unit: A
randomized study. British journal of Anaesthesia, 112, 89-95. doi: 10.1093/bja/aet304
Le, A., Friese, R. S., Hsu, C. H., Wynne, J. L., Rhee, P., &
O'Keeffe, T. (2012). Sleep disruptions and nocturnal nursing interactions in the intensive care unit. Journal of Surgical Research, 177(2), 310-314.
Litton, E., Carnegie, V., Elliott, R., & Webb, S. A. (2016).
The efficacy of earplugs as a sleep hygiene strategy for reducing delirium in the ICU: a systematic review and meta-analysis. Critical care medicine, 44(5), 992- 999.
OCEBM Levels of Evidence Working Group. (2011). The Oxford 2011 levels of evidence. Retrieved from
http://www.cebm.net/index.aspx?o=5653
Olson, D. M., Borel, C. O., Laskowitz, D. T., Moore, D. T.,
& McConnell, E. S. (2001). Quiet time: a nursing intervention to promote sleep in neurocritical care units. American Journal of Critical Care, 10(2), 74.
Parthasarathy, S., & Tobin, M. J. (2004). Sleep in the intensive care unit. Intensive Care Medicine, 30, 197- 206.
Patel J, Baldwin J, Bunting P, et al. (2014). The effect of a multicomponent multidisciplinary bundle of interventions on sleep and delirium in medical and surgical intensive care patients. Anaesthesia, 69, 540- 549.
Pope, D. (2010). Decibel levels and noise generators on four medical/surgical nursing units. Journal of Clinical Nursing, 19, 2463-2470.
Pope, D. S., Gallun, F. J., & Kampel, S. (2013). Effect of hospital noise on patients’ ability to hear, understand, and recall speech. Research in Nursing & Health, 36(3), 228-241.
Richards, K., Nagel, C., Markie, M., Elwell, J., &Barone, C.
(2003). Use of complementary and alternative therapies to promote sleep in critically ill patient.
Nursing Critical Care Clinics of North America, 15(3), 329-340.
Scotto C J, Mc Clusky C, Spillan S, et al. (2009). Earplugs improve patients’ subjective experience of sleep in critical care. Nursing in critical care, 14, 180-184.
Simini, B. (1999). Patients’ perceptions of intensive care.
The Lancet, 354(9178), 571-572.
Thomas, H. F. (1991).Noise&health. New York: The New York Academy of Medicine.
Van Rompaey B, Elseviers M, Van Drom W, et al. (2012).
The effect of earplugs during the night on the onset of delirium and sleep perception: A randomized
controlled trial in intensive care patients. Critical care, 16, R73.
Williamson, S. N. (2002). Sleep deprivation in patients in critical care unit. Nursing Journal of India, 93(12), 267- 270.
Journal of Healthcare Science No. 1, February 2020
Effect of earplugs on the sleep quality of respiratory care center patients
Shih-Chun Ying*1、Hsiang-Chu Pai2
1 RN, Department of Nursing, Chung Shan Medical University Hospital
2 Associate Professor, School of Nursing, Chung Shan Medical University Abstract:
Background
There are many factors that can affect sleep quality including light, medical care, and noise. These factors exist in intensive care units (ICUs). According to the existing research, about 20% of ICU patients with sleep disorders are affected by noise. Noise can suppress the generation of melatonin and interfere with sleep patterns, which could cause delirium. Delirium can prolong hospitalization and increase the consumption of medical resources. This problem exists in respiratory care center (RCCs) as well.
Purpose
To discuss medical care in terms of sleep quality of patients with earplugs in RCCs.
Material and Methods
Following the PICO elements, P (patient) in this study stands for the ICU patient, I (intervention) represents those with earplugs, C (comparison) represents those without earplugs, and O (outcome) is measured in terms of sleep quality and incidence of delirium. Data of the past five years were obtained from the Cochrane Library, PubMed, CHINAL, and Airiti Library. The newest article is
a systematic review, which will be used after reading and will apply to clinical work. Earplugs constitute the main tool, while the measurement tool is the Richards-Campbell Sleep Questionnaire (RCSQ).Measurements are conducted four times including one pre-test and three post-tests.
Result
The article review tool, Critical Appraisal Skills Programme (CASP), was developed by the British Public Hygienic department in 2011. It consists of 10 questions, 7 of which are applied in clinics. The result shows that patients who use earplugs for three nights enjoy significantly better sleep quality as compared to the pre-test (no earplugs) patients. In addition, patients who use earplugs in the first night have the most significant change of sleep quality.
Conclusion
The simples will increase in further research. Earplugs made with different materials will cause different effects of sound insulation and variations in patients’ sleep quality.
Keywords: Respiratory Care Center, Earplugs, Sleep Quality
Accepted for publication October 31, 2019
*Address for correspondence to: Chun-Ying Shih, No.110, Sec. 1, Chien-Kuo N. Rd, Taichung 40201, Taiwan, ROC.
Tel:04-24739595-32700 E-mail: [email protected]