行政院國家科學委員會補助專題研究計畫 ■ 成 果 報 告
□期中進度報告
利用自組裝胜肽奈米纖維進行心血管再生的轉譯醫學研究
Translational research for cardiovascular regeneration using self-assembling peptide nanofibers
計畫類別:■ 個別型計畫 □ 整合型計畫 計畫編號:NSC97-2314-B-006-015-MY2
執行期間:2008 年 8 月 1 日至 2010 年 7 月 31 日
計畫主持人:楊友任
共同主持人:謝清河,羅傳堯
計畫參與人員:林意棟,蔡達慶,施雅云,朱婷鈺
成果報告類型(依經費核定清單規定繳交):□精簡報告 ■完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
■涉及專利或其他智慧財產權,□一年■二年後可公開查詢
執行單位:成功大學醫學院外科
中 華 民 國 99 年 10 月 31 日
計畫中英文摘要
奈米生物科技(nano-biotechnology)是生物醫學研究最新的利器之一。然而現今的應用仍 多侷限於醫學影像的診斷或癌症治療的研究二方面,甚少有被運用在"再生醫學"的研究 或應用上。再生醫學(regenerative medicine)是一門整合生物、醫學、與工程等多重領域的新 科學,其目的在促進人體組織器官的修復、維持、與功能的提升。之前的研究利用自組裝 胜肽奈米纎維(self-assembling peptide nanofibers)進行控制型藥物釋放,我們發現直接將胜肽 奈米纖維注入缺氧的老鼠心臟內,可以局部、緩慢、持續且有效的釋放具有治療效果的生 長因子,像是 PDGF 與 IGF,來達到保護心肌細胞、降低壞死程度,並且促進心肌再生的 效果,此實驗結果證明胜肽奈米纖維是一種極具臨床應用潛力的奈米生醫新科技。
本研究計畫的目的即在驗證是否經由這樣的新科技在缺氧的猪心也同樣具有治療的效 果,並結合其他生醫工程的研究技術改進此一系統,同時探究與開發新型奈米纖維藥物釋 放的最佳模式,以幫助心臟血管形成成熟而有用的新組織,使奈米生物科技與再生醫學的 研究更向前一步,以利將來邁向臨床應用。
關鍵詞: 奈米生物科技,再生醫學,自組裝胜肽奈米纎維,心臟,血管
Nanobiotechnology has emerged as a novel approach for biomedical research and applications in recent years. However, until now studies using nanobiotechnology mostly focus on diagnostic imaging or experimental cancer therapy, with very limited studies conducted in the field of regenerative medicine, an emerging multidisciplinary approach involving biology, medicine, and engineering to restore, maintain, or enhance tissue and organ function.
Recently, a new class of nanobiomaterials – the injectable self-assembling peptide nanofibers - has been developed. Previous studies have shown that these nanofibers support adhesion, growth and differentiation of many types of cells, with no increase of immunogenic response and rapid degrade following in vivo injection. These unique properties make peptide nanofibers exceptionally promising for use as biological scaffolds in regenerative medicine. Interestingly, we have found that for cardiac regeneration direct intramyocardial injection of peptide nanofibers induces microenvironmental neovascularization. Furthermore, peptide nanofibers can be
“custom-designed” to deliver platelet-derived growth factor (PDGF), insulin-like growth factor (IGF) and others for intramyocardial slow release, showing improvement of ventricular performance and cardiac cell therapy in a rat model of experimental myocardial infarction, suggesting a true potential of using nanofibers for cardiovascular regeneration. Accordingly, in the current proposal we propose a translational approach to test if controlled PDGF delivery using nanofibers may improve cardiovascular regeneration in large animals. Results from this work may not only provide important information in translational research, but also lead to clinically applicable therapy for cardiovascular diseases.
Key word:
Translational research, nanobiotechnology, regenerative medicine, self-assembling peptide nanofibers, cardiovascularISSN: 1524-4539
Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online 72514
Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
DOI: 10.1161/CIRCULATIONAHA.110.939512 2010;122;S132-S141
Circulation
C.H. Hsieh
Luo, Kung-Chao Chang, Jyh-Hong Chen, Hua-Lin Wu, Tin-Kan Hung and Patrick Shih, Min-Yao Chang, Yen-Wen Liu, Alan C.L. Tang, Tsai-Yun Chen, Chwan-Yau Yi-Dong Lin, Ming-Long Yeh, Yu-Jen Yang, Da-Ching Tsai, Ting-Yu Chu, Ya-Yun
Ventricular Remodeling and Efficacy of Bone Marrow Cell Therapy in Pigs Intramyocardial Peptide Nanofiber Injection Improves Postinfarction
http://circ.ahajournals.org/cgi/content/full/122/11_suppl_1/S132 located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprints
Reprints: Information about reprints can be found online at
[email protected] 410-528-8550. E-mail:
Fax:
Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050.
Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://circ.ahajournals.org/subscriptions/
Subscriptions: Information about subscribing to Circulation is online at
Intramyocardial Peptide Nanofiber Injection Improves Postinfarction Ventricular Remodeling and Efficacy of Bone
Marrow Cell Therapy in Pigs
Yi-Dong Lin, MS; Ming-Long Yeh, PhD; Yu-Jen Yang, MD, PhD; Da-Ching Tsai, MS;
Ting-Yu Chu, BA; Ya-Yun Shih, MS; Min-Yao Chang, MS; Yen-Wen Liu, MD; Alan C.L. Tang, MS;
Tsai-Yun Chen, MD; Chwan-Yau Luo, MD, MS; Kung-Chao Chang, MD, PhD;
Jyh-Hong Chen, MD, PhD; Hua-Lin Wu, PhD; Tin-Kan Hung, PhD; Patrick C.H. Hsieh, MD, PhD
Background—Growing evidence suggests that intramyocardial biomaterial injection improves cardiac functions after myocardial infarction (MI) in rodents. Cell therapy is another promising approach to treat MI, although poor retention of transplanted cells is a major challenge. In this study, we hypothesized that intramyocardial injection of self-assembling peptide nanofibers (NFs) thickens the infarcted myocardium and increases transplanted autologous bone marrow mononuclear cell (MNC) retention to attenuate cardiac remodeling and dysfunction in a pig MI model.
Methods and Results—A total of 40 mature minipigs were divided into 5 groups: sham, MI ⫹normal saline, MI⫹NFs, MI ⫹MNCs, and MI⫹MNCs/NFs. MI was induced by coronary occlusion followed by intramyocardial injection of 2 mL normal saline or 1% NFs with or without 1 ⫻10
8isolated autologous MNCs. NF injection significantly improved diastolic function and reduced ventricular remodeling 28 days after treatment. Injection of MNCs alone ameliorated systolic function only, whereas injection of MNCs with NFs significantly improved both systolic and diastolic functions as indicated by ⫹dP/dt and ⫺dP/dt (1214.5⫾91.9 and ⫺1109.7⫾91.2 mm Hg/s in MI⫹NS, 1693.7 ⫾84.7 and ⫺1809.6⫾264.3 mm Hg/s in MI⫹MNCs/NFs, respectively), increased transplanted cell retention (29.3 ⫾4.5 cells/mm
2in MI ⫹MNCs and 229.4⫾41.4 cells/mm
2in MI ⫹MNCs/NFs) and promoted capillary density in the peri-infarct area.
Conclusions—We demonstrated that NF injection alone prevents ventricular remodeling, whereas cell implantation with NFs improves cell retention and cardiac functions after MI in pigs. This unprecedented combined treatment in a large animal model has therapeutic effects, which can be translated to clinical applications in the foreseeable future. (Circulation. 2010;
122[suppl 1]:S132–S141.)
Key Words: biomaterials 䡲 bone marrow mononuclear cells 䡲 cardiac tissue engineering 䡲 myocardial infarction
C ongestive heart failure is a leading cause of death in the United States and other developed countries. The dom- inant cause of heart failure is loss of myocardium due to coronary artery disease and the limited regeneration potential of cardiomyocytes. Cardiac tissue engineering is a promising and actively developing area of research aiming to repair, replace, and regenerate the myocardium. Several studies have demonstrated the feasibility of this approach and indicated that direct injection of biomaterials into the infarcted myo- cardium may be beneficial in preventing deleterious remod- eling and reducing cardiac dysfunction.
1– 4Previous studies using intramyocardial injection of self-assembling peptide nanofibers (NFs), a highly biocompatible
5,6and biodegrad-
able
7material, have also revealed their therapeutic potentials for angiogenesis, controlled drug/growth factor release, cell delivery, and stem cell recruitment.
5–10These results indicate that NFs may impact a broad spectrum of applications in myocardial tissue engineering.
Cell therapy is another promising approach to heart disease treatments; however, there are many challenges that call for attention such as the extremely low retention and survival rates of implanted cells.
11This issue is especially apparent in cardiac therapy due to the forbidding microenvironment of a high blood flow rate in the heart and a high degree of ventricular remodeling after myocardial infarction (MI).
12Thus, it may be necessary to inject cells contained within
From the Institute of Biomedical Engineering (Y.D.L., M.L.Y., M.Y.C., P.C.H.H.), Institute of Clinical Medicine & Research Center of Clinical Medicine (Y.D.L., D.C.T., T.Y.C., Y.Y.S., M.Y.C., Y.W.L., A.C.L.T., P.C.H.H.), Department of Surgery (Y.J.Y., C.Y.L., P.C.H.H.), Department of Medicine (Y.W.L., T.Y.C., J.H.C.), Department of Pathology (K.C.C.), and Department of Biochemistry and Molecular Biology (H.L.W.), National Cheng Kung University & Hospital, Tainan, Taiwan; the Institute of Biomedical Sciences (P.C.H.H.), Academia Sinica, Taipei, Taiwan; and the Department of Bioengineering (T.K.H.), University of Pittsburgh, Pittsburgh, Pa.
The online Data Supplement can be found with this article at http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.110.939512/DCI.
Correspondence to Patrick C.H. Hsieh, MD, PhD, Institute of Clinical Medicine & Research Center of Clinical Medicine, National Cheng Kung University & Hospital, 35 Xiao-Dong Road, Room 7063, Tainan 70428, Taiwan. E-mail [email protected]
© 2010 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.110.939512
at BPLUS/CHEKM on September 13, 2010 S132 circ.ahajournals.org
Downloaded from
vehicles or biomaterials coupled with nutritional factors to increase cell retention and cell survival rates.
13Lastly, the lack of angiogenesis in the MI zone is also a critical concern regarding support, survival, and grafting of implanted cells into the host tissue.
14Small animal models have been used to attain exciting and promising achievements by different combinations of the mentioned approaches. In contrast, large animal model stud- ies have not been widely performed
15,16but are crucial to further investigation of clinical applications. Therefore, we carried out experiments to test the hypothesis that intramyo- cardial injection of NFs thickens the infarcted myocardium and increases cell retention such that attenuation of post-MI cardiac remodeling and dysfunction can be achieved in a pig model of experimental MI.
Methods
A total of 40 sexually mature minipigs (approximately 5 months old, acquired from National Taitung Animal Propagation Station and housed at NCKU Animal Center.) were divided into 5 groups: sham
operation, which was performed by opening the chest without coronary artery ligation (sham), MI⫹normal saline (NS), MI⫹NFs, MI⫹autologous bone marrow mononuclear cells (MNCs), and MI⫹MNCs along with NFs (MNCs/NFs; n⫽8 in each group). MI was induced by permanent occlusion of the midleft anterior descend- ing coronary artery immediately followed by injection of a total of 2 mL NS or 1% NFs divided among approximately 40 injections into the infarcted area. Freshly isolated 1⫻108autologous MNCs were mixed in 2 mL NS or NFs for injection. Cardiac functions were assessed by echocardiography before and immediately after MI and together with hemodynamic measurements through catheter- ization 4 weeks later (Supplemental Figure I, II). For additional information, see online Supplemental Material (available at http://circ.ahajournals.org).
Results
Injection of Peptide NFs Alone Increases
Interventricular Septum Thickness and Prevents Ventricular Remodeling After Infarction
The successful induction of MI was confirmed by a comparably decreased left ventricular ejection fraction (LVEF) immediately postinfarction among groups (LVEF: 62.1 ⫾1.0% in sham,
Figure 1. Injection of peptide NFs increases interventricular septum thickness, and injection of bone marrow MNCs improves systolic functions after infarction. A, Histogram of LVEF before, immediately after, and 28 days after MI in sham and experimental groups. B, Statistical analysis of interventricular septum thickness at systole and diastole. *P⬍0.05, **P⬍0.01, ***P⬍0.001 versus MI⫹NS;†††P⬍0.001 versus MI⫹NFs; ‡P⬍0.05 versus MI⫹MNCs.
Lin et al Nanofibers for Bone Marrow Cell Therapy in Pig MI S133
45.1 ⫾1.7% in MI⫹NS, 46.3⫾3.7% in MI⫹NFs, 44.0⫾5.0% in MI ⫹MNCs, 44.5⫾1.6% in MI⫹ MNCs/NFs; all P⬍0.001 versus sham; Figure 1A).
At 28 days after MI, 68.5 ⫾2.3% NFs were retained in the injected regions as determined by high-performance liquid chromatography (Supplemental Figure III). Injection of NFs alone significantly increased both systolic and diastolic inter- ventricular septum thickness (systole: 0.54 ⫾0.02 cm and diastole: 0.46 ⫾0.03 cm in the MI⫹NS group; and systole:
0.73 ⫾0.05 cm and diastole: 0.57⫾0.02 cm in the MI⫹NFs group; Figure 1B). Furthermore, both left ventricular left ventricular end diastolic volume and left ventricular end systolic volume were improved by NF injection (Table), suggesting that this significantly prevented post-MI left ventricular dilatation. NF injection significantly increased the ratio of scar thickness and decreased the ratio of scar length in the infarct (scar thickness ratio: 66.8 ⫾2.6% and scar length ratio: 26.0 ⫾1.1% in the MI⫹NS group, and scar thickness ratio: 85.1 ⫾5.4% and scar length ratio: 21.0⫾1.5% in the MI ⫹NFs group; Figure 2). Together these findings imply that the scar expansion and left ventricular remodeling after infarction were prevented by NF injection.
In addition, the post-MI diastolic function was significantly improved after NF injection ( ⫺dP/dt: ⫺1109.7⫾91.2 mm Hg/s in the MI ⫹NS group, and ⫺1751.0⫾86.9 mm Hg/s in the MI ⫹NFs group; Table). Consistently, the collagen content at the remote zone (collagen content: 22.5 ⫾0.7% in the MI⫹NS group and 13.0 ⫾0.9% in the MI⫹NFs group; Figure 3) and the global
elasticity (as assessed by arterial elastance and maximum cham- ber elasticity; Table) both significantly revealed improvement of cardiac compliance by NF injection. However, estimation of LVEF by echocardiography and ⫹dP/dt by catheterization showed no improvement by NF injection (Figure 1A; Table).
Combining the finding that there was no significant difference in the ratio of necrotic area between MI ⫹NS and MI⫹NFs groups (Figure 2C), these results suggest that NF implantation alone may not be sufficient for recovery of cardiac performance and cell implantation may be required to increase the contractile component for the improvement of systolic function.
Injection of Peptide Nanofibers Along With Autologous Bone Marrow MNCs Improves Both Systolic and Diastolic Functions After Infarction At 28 days after infarction, injection of autologous bone marrow MNCs alone significantly increased LVEF, systolic interventricular septum thickness, and ⫹dP/dt (Figure 1;
Table), suggesting that MNC injection improved systolic function after MI. However, neither diastolic interventricular septum thickness nor ⫺dP/dt showed improvement by MNC injection (Figure 1B; Table). Combining the finding that there was no improvement in the maximum chamber elasticity between MI ⫹NS and MI⫹MNCs groups (Table), these results suggest that MNC implantation alone may not be sufficient for prevention of ventricular remodeling after MI, and NF implantation may be required to increase cardiac compliance and diastolic function.
Table. Hemodynamic Parameters at 1 Month After MI Parameter
Sham (n⫽8)
MI⫹NS (n⫽8)
MI⫹NFs (n⫽8)
MI⫹MNCs (n⫽8)
MI⫹MNCs/NFs (n⫽8) Heart rate, beats/min 102.4⫾6.3 94.0⫾4.4 94.0⫾6.7 95.6⫾8.1 99.4⫾6.8
LVESP, mm Hg 89.0⫾4.1 69.6⫾2.6 77.5⫾3.4 77.1⫾5.7 79.1⫾4.5
LVEDP, mm Hg 8.3⫾0.7 12.7⫾0.9 8.6⫾1.0† 8.6⫾0.7† 8.5⫾0.5†
LVESV, mL 35.6⫾3.6 103.0⫾7.0 73.7⫾3.6‡ 58.7⫾2.4‡§ 51.7⫾4.6‡㛳
LVEDV, mL 96.8⫾6.4 147.5⫾7.0 120.3⫾7.0† 115.0⫾5.7† 113.6⫾6.1†
SV, mL 64.9⫾8.6 44.5⫾5.8 52.0⫾5.0 56.2⫾4.8 61.8⫾5.0
CO, mL/min 6636.0⫾959.1 4133.3⫾482.2 5084.6⫾535.2 5247.0⫾433.3 5879.9⫾654.8 SW, mm Hg䡠 mL 4870.5⫾532.4 2527.0⫾414.2 3689.1⫾511.4 4114.5⫾533.6 4567.0⫾809.4
AE, mm Hg/mL 1.52⫾0.12 0.89⫾0.07 1.26⫾0.08* 1.12⫾0.09* 1.29⫾0.10*
⫹dP/dt, mm Hg/s 1852.7⫾82.9 1214.5⫾91.9 1419.4⫾71.8 1602.1⫾135.6* 1693.7⫾84.7†
⫺dP/dt, mm Hg/s ⫺2048.8⫾293.1 ⫺1109.7⫾91.2 ⫺1751.0⫾86.9* ⫺1401.4⫾127.6 ⫺1809.6⫾264.3*
(Weiss method), ms 30.8⫾0.8 42.1⫾3.4 33.0⫾1.9* 34.5⫾0.9* 32.1⫾1.7*
PRSW, mm Hg 65.1⫾8.4 42.2⫾5.6 55.8⫾6.8 60.5⫾5.9 65.1⫾13.8
ESPVR, mm Hg/mL 1.6⫾.2 0.7⫾0.1 1.2⫾0.2 1.3⫾0.2 1.5⫾0.2
EDPVR, mm Hg/mL 0.05⫾0.02 0.06⫾0.02 0.05⫾0.02 0.06⫾0.02 0.05⫾0.02
Emax, mm Hg/mL 3.6⫾0.4 1.4⫾0.2 2.9⫾0.2* 2.5⫾0.5 3.3⫾0.4†
⫹dP/dt-EDV, mm Hg/s/mL 14.3⫾4.5 6.5⫾1.6 9.4⫾3.0 9.5⫾2.1 12.0⫾2.9
Values are mean⫾SEM.
*P⬍0.05 versus MI⫹NS.
†P⬍0.01 versus MI⫹NS.
‡P⬍0.001 versus MI⫹NS.
§P⬍0.05 versus MI⫹NFs.
㛳P⬍0.01 versus MI⫹NFs.
LVESP indicates left ventricular end systolic pressure; LVEDP, left ventricular end diastolic pressure; LVESV, left ventricular end systolic volume; LVEDV, left ventricular end diastolic volume; SV, stroke volume; CO, cardiac output; SW, stroke work; AE, arterial elastance;, time constant of left ventricular pressure decay; PRSW, preload recruitable stroke work; ESPVR, end diastolic pressure–volume relationship;
EDPVR, end systolic pressure–volume relationship; Emax, maximum chamber elasticity; EDV, end diastolic volume.
S134 Circulation September 14, 2010
at BPLUS/CHEKM on September 13, 2010 circ.ahajournals.org
Downloaded from
Confirming this hypothesis, we found that the LVEF (66.0 ⫾1.0% in the sham group, 45.2⫾1.8% in the MI⫹NS group, 48.2 ⫾2.0% in the MI⫹NFs group, 52.6⫾2.1% in the MI ⫹MNCs group, 58.7⫾1.6% in the MI⫹MNCs/NFs group;
Figure 1A), left ventricular end diastolic pressure, left ven- tricular end systolic volume, left ventricular end diastolic volume, AE, ⫹dP/dt, ⫺dP/dt, , and maximum chamber elasticity were all significantly improved as a result of MNC/NF injection (Table). Although injection of MNCs alone without NFs also improved systolic function after MI,
only injection of MNCs combined with NFs improved both systolic and diastolic functions.
Injection of Peptide NFs Along With Autologous Bone Marrow MNCs Decreases Necrotic Tissue and Collagen Content in the Remote Area After Infarction
Consistent with the finding that MNC/NF injection improved both systolic and diastolic functions after MI, the necrotic tissue was significantly reduced after infarction (18.6 ⫾1.1%
Figure 2. Injection of peptide NFs prevents infarct expansion, and injection of bone marrow MNCs improves tissue viability after infarc- tion. A, Representative cross-section images at the level of papillary muscle insertion of left ventricle from each group. B, Magnified images of nonnecrotic tissue in the peri-infarct zone indicated by the dashed boxes in A. C, Percentages of scar thickness ratio, scar length ratio, and necrotic area ratio determined using computer image analysis. *P⬍0.05, **P⬍0.01, ***P⬍0.001 versus MI⫹NS;
†P⬍0.05 versus MI⫹NFs; ‡P⬍0.05 versus MI⫹MNCs.
Lin et al Nanofibers for Bone Marrow Cell Therapy in Pig MI S135
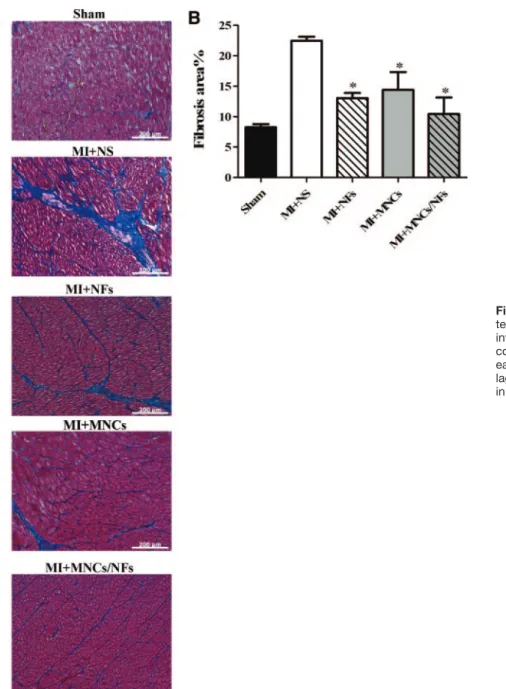
in the MI ⫹NS group, 17.5⫾1.9% in the MI⫹NFs group, 13.2 ⫾2.2% in the MI⫹MNCs group, and 11.3⫾1.5% in the MI ⫹MNCs/NFs group; Figure 2C). Furthermore, injection of MNCs/NFs significantly attenuated collagen content in the remote area after infarction, but a similar effect was also detected in the other 2 groups of NFs injection alone and MNCs injection alone (22.5 ⫾0.7% in the MI⫹NS group, 13.0 ⫾0.9% in the MI⫹NFs group, 14.4⫾3.0% in the MI ⫹MNCs group, and 10.5⫾2.7% in the MI⫹MNCs/NFs group; Figure 3).
Injection of Peptide NFs Along With Bone Marrow MNCs Increases Transplanted Cell Retention and Differentiation as Well as Angiogenesis After Infarction
At the border or infarct zone of treated myocardium, our results showed a higher DiI
⫹cell density in the MI ⫹MNCs/
NFs group than in the MI ⫹MNCs group (29.3⫾4.5 /mm
2in
the MI ⫹MNCs group and 229.4⫾41.4/mm
2in the MI ⫹MNCs/NFs group, P⬍0.001; Figure 4). This result indicates that NFs also serve as a delivery vector to improve the retention of transplanted cells after intramyocardial injection.
To confirm the differentiation fate of the injected MNCs, we used costaining of primary antibodies with DiI signal to trace these cells. To rule out the cytoplasmic autofluores- cence, the DiI signal was checked on multiple wavelengths and was detectable only under red wavelength (Supplemental Figure IVA); serial sections with DiI staining only were also used to confirm that the detected signals were dependent on the primary antibodies to these epitopes (Supplemental Fig- ure IVB–C). Surprisingly, we found that 28 days after injection, the surviving MNCs mainly differentiated into endothelial cells as indicated by von Willebrand factor, VE-cadherin, isolectin, and CD31 staining and few into smooth muscle cells (SM myosin heavy chain, SM22 ␣, and
Figure 3. Injection of peptide NFs pro- tects the remote zone from fibrosis after infarction. A, Representative images of collagen content at the remote zone from each group. B, Statistical analysis of col- lagen content from images such as those in A. *P⬍0.05 versus MI⫹NS.
S136 Circulation September 14, 2010
at BPLUS/CHEKM on September 13, 2010 circ.ahajournals.org
Downloaded from
SM ␣-actin staining), whereas no evidence of differentiation into cardiomyocytes (stained by cardiac tropomyosin, Nkx2.5, and GATA4; Figure 5; Supplemental Figure V and data not shown). We also detected MNC differentiation into hematopoietic lineage cells (stained by CD45 and an antibody against macrophage; Supplemental Figure VI). Interestingly, when NFs were injected along with MNCs, we found a higher differentiation ratio of MNCs into endothelial cells and smooth muscle cells and still no evidence of cardiomyocytes (MNCs: ratio of endothelial cell differentiation, 56.3 ⫾8.8%
and ratio of smooth muscle cell differentiation, 3.3 ⫾2.1%;
MNCs/NFs: ratio of endothelial cell differentiation, 83.0 ⫾4.9% and ratio of smooth muscle cell differentiation, 14.5 ⫾3.5%; Figure 5). These results indicated that one of the benefits of MNC treatment is angiogenesis and this effect is enhanced by injection of MNCs along with NFs. Supporting the results of MNC differentiation into endothelial cells, there was significant additional increase of capillary density in the peri-infarct zone after treatment with NFs along with MNCs (capillary density: 190.4 ⫾20.8 number/mm
2in the MI ⫹NS group, 352.6 ⫾33.5 number/mm
2in the MI ⫹NFs group, 533.8 ⫾53.9 number/mm
2in the MI ⫹MNCs group, and 644.8 ⫾64.6 number/mm
2in the MI ⫹MNCs/NFs group;
Figure 6).
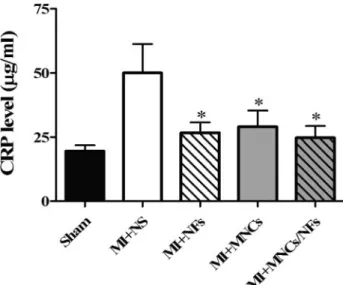
Injection of NFs Reduces C-Reactive Protein Levels After Infarction
Although the biocompatibility of NFs is well established,
5it has not yet been confirmed in pigs, so we measured C-reactive protein (CRP) levels in the plasma to detect chronic inflammation. There was no CRP level increase at 28 days after NF injection compared with the control. However, CRP is known to rise as a result of MI itself,
17and our results
confirmed this (sham versus MI only). Surprisingly, all treatment groups showed markedly reduced CRP levels, and the combined NF ⫹MNC group showed the greatest decrease (CRP: 19.5 ⫾2.2 g/mL for sham, 50.0⫾11.2 g/mL in the MI ⫹NS group, 26.7⫾4.0 g/mL in the MI⫹NFs group, 29.0 ⫾6.4 g/mL in the MI⫹MNCs group, and 24.7⫾4.6
g/mL in the MI⫹MNCs/NFs group; Figure 7). Interest- ingly, we also detected significantly decreased leukocyte infiltration in the NF injection area, suggesting that NF injection may not stimulate inflammatory reaction in the infarcted myo- cardium, which is consistent with a previous study in rats (Supplemental Figure VII).
5Discussion
The outcome of intramyocardial biomaterial injection has been investigated in only a few studies. In contrast, cell therapy is a more commonly explored approach, but cell retention is an issue and is often briefly addressed or ignored.
Although both these treatments have potential uses in therapy for cardiac diseases, they have rarely been tested in large animal models, an essential step before proceeding to clinical trials. In this study, we describe a novel approach that combines biomaterial injections with cell therapy and dem- onstrate that cardiac functions are regained in a large animal model of MI.
Local Repair by Biomaterial Injection Preserves Cardiac Geometry and Function
Jugdutt suggested that although extracellular matrix expres- sion increases in the entire heart after MI, this increase is only beneficial in the infarct zone at the same time as being detrimental in the noninfarct zone.
18In this study, we showed that NF treatment increased interventricular septum thickness
Figure 4. Injection of peptide NFs along with bone marrow MNCs improves transplanted cell retention after infarc- tion. A, Representative pictures of DiI⫹ cells (red) in the area injected with cells alone (left panel) or with cells and NFs (right panel). Nuclei were stained by 4⬘,6-diamidino-2-phenylindole (blue). B, Cell retention rates as reflected by DiI⫹ cell counts. ***P⬍0.001 versus MI⫹MNCs.Lin et al Nanofibers for Bone Marrow Cell Therapy in Pig MI S137
after MI, restrained scar extension, and prevented further harmful fibrosis at the remote zone. Moreover, reduction in global cardiac remodeling and diastolic dysfunction after MI was achieved. Interestingly, these results were very similar to a numeric simulation model proposed by Wall et al, which indicated that intramyocardial noncontractile material injec- tion had all of these effects as well as a reduction in elevated myofiber stresses.
2Landa et al reported that intramyocardial biomaterial in- jection preserves cardiac systolic function 2 months after MI in a rodent model.
3In contrast, we found that NF injection did not improve systolic function at 28 days after MI in pigs. This inconsistency may be due to the different materials, time points, and animal models chosen for the 2 studies. Because the heart failure indices atrial natriuretic peptide and B-type natriuretic peptide showed no difference between the sham and MI ⫹NS groups (data not shown), the heart of a large animal like the pig may still undergo remodeling beyond 28 days after MI, so long-term studies of the effects of NF injection are needed.
Cell Retention Determines Cardiac Functional Improvement by Cell Therapy
Bone marrow MNC transplantation has been reported to benefit the infarcted myocardium.
19We demonstrated similar contributions to cardiac functional improvement after MNC
implantation in pigs. Beyond direct MNC injection alone, injection of MNCs along with NFs showed even better amelioration of cardiac function. We believe these beneficial results were mainly due to the ability of NFs to increase cell retention. Furthermore, consistent with our previous stud- ies,
6,20the presence of NFs did not alter the viability of MNCs, which remained approximately 95% viable before injection (Supplemental Methods). NF injection may also increase the cell survival rate due to the increase in capillary density at the border zones 28 days after MI. From this point of view, coinjection of cells with NFs may be highly beneficial for both cell engraftment and angiogenesis effects due to increases in cell retention and survival rates.
Beyond cell retention and survival, evidence from our results also showed an increase in MNC differentiation into endothelial cells and smooth muscle cells after injection of MNCs/NFs compared with injection of MNCs alone. The NFs may act as a scaffold that provides a suitable microen- vironment for the MNCs to adhere and perform normal cellular functions.
6Furthermore, differentiation of MNCs into endothelial cells and smooth muscle cells promotes angiogenesis and prevents further apoptosis of cardiomyo- cytes within the infarct zone, leading to the preservation of cardiac function.
21These results demonstrate the synergistic effect of NF and MNC injection.
Figure 5. Injection of peptide NFs along with bone marrow MNCs improves transplanted cell differentiation into vascular cells. A–C, Representative images of red DiI fluorescence overlapped with green immunostaining for von Willebrand factor (vWF, A), SM myosin heavy chain (B), and cardiac tropomyosin (C). Nuclei were stained with 4⬘,6-diamidino-2-phenylindole (blue). The image (right panel) was magnified from left panel indicated in the boxes and costained cells were arrowed. The cell integrated into the vessel was indi- cated by an arrowhead in B. D, Quantification of ratio of cells stained with endothelial cell (EC), smooth muscle cell (SMC), and cardio- myocyte (CM) markers.
S138 Circulation September 14, 2010
at BPLUS/CHEKM on September 13, 2010 circ.ahajournals.org
Downloaded from
Combined MNC/NF Injection Has Complementary Effects for Clinical Application
MNC injection alone significantly increased systolic but not diastolic function after MI, whereas NF injection alone increased diastolic but not systolic function. Importantly, the combined injection of MNCs and NFs improved both systolic and diastolic function. This combination thus acts in a complementary fashion to synergistically benefit cardiac function and is now shown to be feasible in a large animal model with induced acute MI. Because most cardiac patients have chronic heart disease, whether this treatment is applica- ble for chronic MI cases as well the appropriate time window requires further investigation.
The different conditions of the treatments in this study such as dosage, timing, and location of injections were tuned to be optimal for 25-kg minipigs. Modification is necessary for clinical trial models. However, one exception is the require- ment for spread-out injections to achieve a well dispersed administration of the cells and NFs. In the future, open-chest intramyocardial injection may be replaced by a catheter transendocardial approach or minimally invasive thoracot- omy for clinical use to minimize the risk and harm of surgery itself.
From a safety perspective, introduction of foreign materials into the body may be seen as hazardous, possibly leading to
mechanical failure or arrhythmia caused by change in con- ductance of the heart. In our study, 2 of 42 animals died with intractable ventricular fibrillation on the operating table before any treatments were administered. There were no negative side effects due to NF treatments.
Mechanisms of MNC Therapy Remain to Be Determined
The mechanisms of cardiac functional improvement by bone marrow cell therapy are still under investigation.
12,13Contro- versies exist concerning myocyte differentiation,
22,23para- crine effects,
24and whether stimulation causes endogenous cardiac repair.
25Another interesting question is if the trans- planted bone marrow cells may integrate into the pre-existing vessels or form entirely new vessels. As shown in Figure 5B and Supplemental Figure VIII, we observed not only integra- tion of MNC-derived smooth muscle cells into pre-existing vessels, but also new vessels formed entirely from the injected MNCs. However, to what extent these effects con- tribute to the increase of functional improvement after MI remains unknown. Therefore, the specific pathways and mechanisms by which bone marrow cells act require further investigation.
Quevedo et al reported that 14% bone marrow cells differentiate into cardiomyocytes, but our data did not con-
Figure 5 (Continued).Lin et al Nanofibers for Bone Marrow Cell Therapy in Pig MI S139
firm this.
16The major difference is that the cells they used were allogeneic bone marrow mesenchymal stem cells, which were conditioned by in vitro culture. On the other hand, the cells we used were autologous bone marrow MNCs, which are nonadherent and mainly consist of hematopoietic cells. In
dealing with the controversies surrounding the various results and explanations of bone marrow cell therapy effects, a more stringent approach or confirmation by double experimental methods should be carried out for more convincing results.
For example, genetic linage tracking could be considered for tracing the injected cells in future studies.
25Here, we at- tempted to simulate the clinical situation of a single proce- dure, rather than a sequence of steps, so DiI-labeled MNCs were chosen to allow convenient cell isolation and cell labeling concurrently in MI without a complicated and precarious preprocess.
In conclusion, the present study reveals that intramyocar- dial injection of NFs alone prevents pathological left ventric- ular remodeling, whereas injection of cells along with NFs helps raise the cell retention rate and improve cardiac performance 28 days after MI in pigs. To our knowledge, this is the first study to use this novel combined treatment approach in a large animal model and demonstrate positive therapeutic effects. We believe these methods and results can be translated to clinical applications in the foreseeable future.
Acknowledgments
We gratefully acknowledge Iain C. Bruce, PhD (Zhejiang University School of Medicine) for manuscript preparation and the Taitung Animal Propagation Station and the NCKU Animal Center for assistance with pig experiments.
Figure 6. Injection of peptide NFs along with bone marrow MNCs improves capillary density in the peri-infarct area. A, Representative immunostaining of isolectin (green) overlapped with cardiomyocytes stained with cardiac tropomyosin (red) at the border zone from each group. Nuclei were stained by 4⬘,6-diamidino-2-phenylindole (blue). B, Quantification of capillary density in the peri-infarct zone.
*P⬍0.05, ***P⬍0.001 versus MI⫹NS; †P⬍0.05, ††P⬍0.01 versus MI⫹NFs.
Figure 7. Injection of peptide NFs decreases CRP level after infarction. Statistics of CRP levels. *P⬍0.05 versus MI⫹NS.
S140 Circulation September 14, 2010
at BPLUS/CHEKM on September 13, 2010 circ.ahajournals.org
Downloaded from
Sources of Funding
This work was supported by the National Science Council (97IR082, 96-2314-B-006-021, 97-2314-B-006-015), the National Health Re- search Institutes (EX97-9722SI), and the National Cheng Kung University Integrated Landmark Project (98I006).
Disclosures
None.
References
1. Dai W, Wold LE, Dow JS, Kloner RA. Thickening of the infarcted wall by collagen injection improves left ventricular function in rats: a novel approach to preserve cardiac function after myocardial infarction. J Am Coll Cardiol. 2005;46:714 –719.
2. Wall ST, Walker JC, Healy KE, Ratcliffe MB, Guccione JM. Theoretical impact of the injection of material into the myocardium: a finite element model simulation. Circulation. 2006;114:2627–2635.
3. Landa N, Miller L, Feinberg MS, Holbova R, Shachar M, Freeman I, Cohen S, Leor J. Effect of injectable alginate implant on cardiac remodeling and function after recent and old infarcts in rat. Circulation.
2008;117:1388 –1396.
4. Karen LC, Randall JL. Biomaterials for the treatment of myocardial infarction. J Am Coll Cardiol. 2006;48:907–913.
5. Hsieh PCH, Davis ME, Gannon J, MacGillivray C, Lee RT. Controlled delivery of PDGF-BB for myocardial protection using injectable self- assembling peptide nanofibers. J Clin Invest. 2006;116:237–248.
6. Davis ME, Motion JPM, Narmoneva DA, Takahashi T, Hakuno D, Kamm RD, Zhang S, Lee RT. Injectable self-assembling peptide nano- fibers create intramyocardial microenvironments for endothelial cells.
Circulation. 2005;111:442– 450.
7. Davis ME, Hsieh PCH, Takahashi T, Song Q, Zhang S, Kamm RD, Grodzinsky AJ, Anversa P, Lee RT. Local myocardial insulin-like growth factor 1 (IGF-1) delivery with biotinylated peptide nanofibers improves cell therapy for myocardial infarction. Proc Natl Acad Sci U S A. 2006;
103:8155– 8160.
8. Davis ME, Hsieh PCH, Grodzinsky AJ, Lee RT. Custom design of the cardiac microenvironment with biomaterials. Circ Res. 2005;97:8 –15.
9. Engel FB, Hsieh PCH, Lee RT, Keating MT. FGF1/p38 MAP kinase inhibitor therapy induces cardiomyocyte mitosis, reduces scarring, and rescues function after myocardial infarction. Proc Natl Acad Sci U S A.
2006;103:15546 –15551.
10. Hsieh PCH, MacGillivray C, Gannon J, Cruz FU, Lee RT. Local con- trolled intramyocardial delivery of platelet-derived growth factor improves postinfarction ventricular function without pulmonary toxicity.
Circulation. 2006;114:637– 644.
11. Hofmann M, Wollert KC, Meyer GP, Menke A, Arseniev L, Hertenstein B, Ganser A, Knapp WH, Drexler H. Monitoring of bone marrow cell homing into the infarcted human myocardium. Circulation. 2005;111:
2198 –2202.
12. Segers VF, Lee RT. Stem-cell therapy for cardiac disease. Nature. 2008;
451:937–942.
13. Laflamme MA, Murry CE. Regenerating the heart. Nat Biotechnol. 2005;
23:845– 856.
14. Sekine H, Shimizu T, Hobo K, Sekiya S, Yang J, Yamato M, Kurosawa H, Kobayashi E, Okano T. Endothelial cell coculture within tissue- engineered cardiomyocyte sheets enhances neovascularization and improves cardiac function of ischemic hearts. Circulation. 2008;118:
S145–S152.
15. Johnston PV, Sasano T, Mills K, Evers R, Lee ST, Smith RR, Lardo AC, Lai S, Steenbergen C, Gerstenblith G, Lange R, Marban E. Engraftment, differentiation, and functional benefits of autologous cardiosphere- derived cells in porcine ischemic cardiomyopathy. Circulation. 2009;120:
1075–1083.
16. Quevedo HC, Hatzistergos KE, Oskouei BN, Feigenbaum GS, Rodriguez JE, Valdes D, Pattany PM, Zambrano JP, Hu Q, McNiece I, Heldman AW, Hare JM. Allogeneic mesenchymal stem cells restore cardiac function in chronic ischemic cardiomyopathy via trilineage differentiating capacity. Proc Natl Acad Sci U S A. 2009;106:14022–14027.
17. Park DW, Yun SC, Lee JY, Kim WJ, Kang SJ, Lee SW, Kim YH, Lee CW, Kim JJ, Park SW, Park SJ. C-reactive protein and the risk of stent thrombosis and cardiovascular events after drug-eluting stent implan- tation. Circulation. 2009;120:1987–1995.
18. Jugdutt BI. Ventricular remodeling after infarction and the extracellular collagen matrix: when is enough enough? Circulation. 2003;108:
1395–1403.
19. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RV, Kogler G, Wernet P. Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans.
Circulation. 2002;106:1913–1918.
20. Narmoneva DA, Vukmirovic R, Davis ME, Kamm RD, Lee RT. Endo- thelial cells promote cardiac myocyte survival and spatial reorganization:
implications for cardiac regeneration. Circulation. 2004;110:962–968.
21. Hsieh PCH, Davis ME, Lisowski LK, Lee RT. Endothelial– cardiomyo- cyte interactions in cardiac development and repair. Annu Rev Physiol.
2006;68:51– 66.
22. Balsam LB, Wagers AJ, Christensen JL, Kofidis T, Weissman IL, Robbins RC. Haematopoietic stem cells adopt mature haematopoietic fates in ischaemic myocardium. Nature. 2004;428:668 – 673.
23. Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima HO, Rubart M, Pasumarthi KBS, Ismail Virag J, Bartelmez SH, Poppa V, Bradford G, Dowell JD, Williams DA, Field LJ. Haematopoietic stem cells do not transdifferentiate into cardiac myocytes in myocardial infarcts. Nature.
2004;428:664 – 668.
24. Kinnaird T, Stabile E, Burnett MS, Lee CW, Barr S, Fuchs S, Epstein SE.
Marrow-derived stromal cells express genes encoding a broad spectrum of arteriogenic cytokines and promote in vitro and in vivo arteriogenesis through paracrine mechanisms. Circ Res. 2004;94:678 – 685.
25. Hsieh PCH, Segers VFM, Davis ME, MacGillivray C, Gannon J, Molkentin JD, Robbins J, Lee RT. Evidence from a genetic fate-mapping study that stem cells refresh adult mammalian cardiomyocytes after injury. Nat Med. 2007;13:970 –974.