中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/23818
6
0
0
全文
(2) Wen-Hong Lee, et al.. study. The average duration of plantar fasciitis was 20 months (range, 6 to 72 mo). Eight patients had bilateral heel pain; therefore the total number of painful heels was 45 (right heel, n = 23; left heel, n = 22). The inclusion criteria included proximal plantar fasciitis which could not be cured after 6 months of conservative treatment. Patients were excluded if they were younger than 18 years, if they had less than 6 months of symptoms, if they had systemic or local infection, malignancy, diabetes mellitus, gout, neurologic abnormalities, peripheral vascular disease, implanted plates or screws in the area, or a cardiac pacemaker, and if they were pregnant or taking anti-coagulants. Under local anesthesia, 6 patients received one session of ESWT, 30 patients received two sessions of ESWT, and 1 patient received three sessions of ESWT. Each session consisted of 1000 acoustic shock wave pulses with an energy density of 0.55 mJ/mm2 (MTS OrthoWave®, at level 5). After treatment, the patients were instructed to ice the heel. Full weight bearing was allowed immediately after treatment. Follow-up. 231. examinations were completed at 6 weeks, 12 weeks, 6 months, and 12 months. Patients' general data, pain assessment with a visual analog pain scale and satisfaction and a functional score (The Mayo Clinical Scoring System [7], Table 1) were measured and analyzed pre-treatment and at 6 weeks, 12 weeks, 6 months, and 12 months post-treatment. Data were analyzed by Excel 2003 software (Microsoft Office). Comparison of pre-treatment status with outcome was made by Student's t test with a level of significance at p < 0.05. RESULTS The body weights of the 37 patients ranged from 45 to 87.5 kg (average, 66.5 10.6 kg). The body heights of the 37 patients ranged from 140 to 180 cm (average, 161.9 9.4 cm). The body mass index (BMI) ranged from 18.7 to 32.6 kg/m2 (average, 25.4 5.4 kg/m2). Nineteen heels (42%) had heel spurs on X-ray, ranging in length from 1 to 7 mm (average, 3.6 1.9 mm). All of the spurs were found incidentally on X-ray. There was no relationship between the heel spurs and the degree or duration of heel pain.. Table 1. The Mayo clinical scoring system (Total 100 points) [7] Characteristic Pain None Mild, occasional Moderate, frequent Severe, constant Activity limitations None Minor, no limitation of daily activities limitation of daily and recreational activities Footwear or orthotic requirement No footwear limitations, orthosis not required Minor limits of footwear, orthosis occasionally used Modified shoes reauired, orthosis Plantar heel tenderness Absent Present Neuropathy None, sensation intact Present, hyperthesia, Tinel's sign Antalgic gait Absent Present Excellent results 90-100 points, good results 80-89, fair results 70-79, poor results < 70.. Points 50 40 30 0 10 5 0 10 5 0 10 0 10 0 10 0.
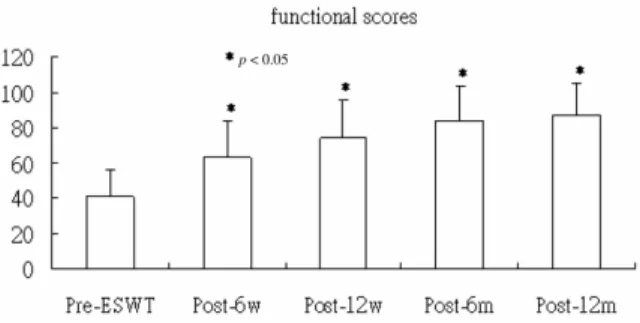
(3) 232. Extracorporeal Shock Wave Therapy. Two patients (2 heels) were lost to followup. Among the remaining 35 patients (43 heels), there were no systemic or local complications such as redness, bruising, swelling or hematoma formation. There were significant statistical differences (p < 0.05) between pre-ESWT and post-ESWT as early as 6 weeks. The visual analog pain scales, functional scores and overall results are listed in Figs. 1, 2 and Table 2.. The etiology of plantar fasciitis is multifactorial but most commonly involves inflammation and degeneration of the proximal plantar fascia caused by overloading. The development of plantar fasciitis is associated with overweight patients, female gender, increased activity levels, and inappropriate shoe wear [14,8,9]. In our study, females represented 48.6% (18/37) of the study population. The BMI data revealed 14 normal weight (BMI = 18.5 to 24.9), 20 overweight (BMI = 25.0 to 29.9), and 3 obese patients (BMI ≥ 30.0); the average BMI was 25.5 3.3. Therefore, 23 patients (62%) were overweight or obese in our study. About 50% to 70% of patients have heel spurs on X-ray films. [1,2]. However, many times they are incidental radiographic findings and are asymptomatic. The relationship between heel spurs and heel pain is still unclear, but it may be a secondary consequence of chronic plantar fasciitis. In our study, heel spurs were found in 19 heels (42%), but they were not related to the symptoms of the disorders. However, the goal of ESWT is relief of pain not fragmentation of heel spurs. Rompe et al used visual analog scales and satisfaction rates to measure outcome in a singleblind study of 30 patients with chronic plantar fasciitis. The patients were divided equally into an ESWT treatment group and a control group. They noted that there was a significant alleviation of pain and improvement of function at all follow-ups in the treatment group [10]. Ogden et al evaluated the effectiveness of extracorporeal shock wave treatment in 297 patients with plantar fasciitis who had failed to respond to conservative measures. The authors noted that 76% of the patients in the treatment group reported pain relief and were satisfied with the outcome of the procedure [6]. Wang et al, in a one-year follow-up study of 79 patients with 85 painful heels, reported that 75.3% were complaint-free and. Fig. 1. VAS for pain scale decreased from 6.87 2.00 preESWT to 3.73 2.68 (6 wk, p < 0.001), 2.59 2.57 (12 wk, p < 0.001), 1.43 1.89 (6 mo, p < 0.001) and 1.05 1.73 (12 mo, p < 0.001) post-ESWT.. Fig. 2. Functional scores (MCSS) increased from 40.5 15.4 pre-ESWT to 62.7 21.0 (6 wk, p < 0.001), 73.4 22.6 (12 wk, p < 0.001), 84.3 19.1 (6 mo, p < 0.001) and 86.9 18.2 (12 mo, p < 0.001) post-ESWT.. DISCUSSION. Table 2. Overall results (post-ESWT). 6 wk 27.9 Pain relief (VAS decreased ≥ 5), % 20.0 Good or excellent result (MCSS ≥ 80), % 72.1 Satisfaction rate, % VAS = visual analog scale; MCSS = Mayo clinic scoring system.. 12 wk 46.5 48.6 74.4. 6 mo 65.1 74.3 81.4. 12 mo 67.4 85.7 72.1.
(4) Wen-Hong Lee, et al.. 18.8% were significantly better. They noted that shockwave therapy seemed to have positive cumulative effects in treating plantar fasciitis [1113]. In our study, there was a 67.4% reduction of pain relief, 85.7% good or excellent results in functional scores and 72.1% of patients were satisfied with the treatment at one-year follow-up. The symptoms seemed to continue improving past 12 months; therefore, the effects of shockwaves may be time-dependent. The results were similar to those reported in the literature [11-13]. Wang et al reported that shock wave therapy relieved pain symptoms by alternating focal circulation and regeneration. They demonstrated that shock wave therapy enhanced neovascularization at the tendon-bone junction in dog and rabbit models [14,15]. Their studies also revealed that shock waves cause neovascularization at the tendon junction by inducing early release of angiogenesis-mediating growth and proliferating factors, including endothelial nitric oxide synthase, vascular endothelial growth factor, and proliferating cell antinuclear antigen; all of these hormones are known to improve blood supply and tissue regeneration [16,17]. Therefore, they concluded that shock wave therapy relieved pain symptoms by alternating focal circulation and regeneration. Rompe et al, in an animal study, noted dose-dependent changes in the tendon and paratenon after ESWT, and they concluded that 2 energy flux densities over 0.28 mJ/m should not be used in the treatment of tendon disorders [18]. However, we used an energy flux density of 0.55 mJ/mm 2, which was between the medium and high range (0.28 to 0.60 mJ/mm2) and there were no complications. Rompe et al also reported that repetitive lower-energy shock waves were successful in treating chronic plantar fasciitis [19,20]. Recently they used repetitive lowerenergy shock waves without local anesthesia to treat the chronic plantar fasciitis, and the result seemed better than that with local anesthesia [21]. In our study, we used the medium energy (0.55 mJ/mm 2 ) shock wave in 1 to 3 sessions of. 233. treatment for each patient. All the patients needed local anesthesia. To achieve better results, we should try the repetitive lower energy level shock waves without local anesthesia. Local steroid injection may have a negative effect on ESWT. In our study, ESWT failed to relieve pain in 14 heels at 12-month follow-up. Ten of the 14 heels had had local steroid injection before ESWT. A total of 19 heels had had local steroid injection before ESWT. The pain was relieved in 47.4% (9/19) of heels with local steroid injection, and 83.3% (20/24) in those without local steroid injection. In conclusion, ESWT is safe and effective for the treatment of chronic plantar fasciitis. It is a non-invasive therapy with a low complication rate and a high success rate. It should be considered before any surgical treatment for intractable pain. Long-term investigation is necessary for further clinical applications. REFERENCES 1. Glenn BF. Plantar heel pain. In: Franklin HS, ed. Instructional Course Lectures, Vol 50: AAOS. Rosemont: Illinois, 2001:521-31. 2. Richardson EG. Chapter 43 disorders of tendons and fascia--painful heel. In: Canale ST, ed. Campbell's Operative Orthopaedics, 9th edition. St. Louis: Mosby, 1998:1912-9. 3. Schepsis AA, Leach RE, Gorzyca J. Plantar fasciitis. Etiology, treatment, surgical results, and review of the literature. Clin Orthop Relat Res 1991;266:185-96. 4. Juliano PJ, Harris TG. Plantar fasciitis, entrapment neuropathies, and tarsal tunnel syndrome: current up to date treatment. Curr Opin Orthop 2004; 15:49-54. 5. Ogden JA, Alvarez RR. Extracorporeal shock wave therapy in orthopaedics. Clin Orthop Relat Res 2001; 387:2-3. 6. Ogden JA, Alvarez R, Levitt R, et al. Shock wave therapy for chronic proximal plantar fasciitis. Clin Orthop Relat Res 2001;387:47-59. 7. Daly PJ, Kitaoka HB, Chao EY. Plantar fasciotomy for intractable plantar fasciitis: clinical results and biomechanical evaluation. Foot Ankle 1992;13:18895. 8. Hill JJ Jr, Cutting PJ. Heel pain and body weight. Foot Ankle 1989;9:254-6..
(5) 234. 9. Foot and ankle Joint. In: Bachmann CE, Gruber G, Konermann W, et al, eds. ESWT and Ultrasound Imaging of the Musculoskeletal System, 2nd revised and translation edition. Germany: Steinkopff Verlag Darmstadt, 2001:99-118. 10.Rompe JD, Hopf C, Nafe B, et al. Low-energy extracorporeal shock wave therapy for painful heel: a prospective controlled single-blind study. Arch Orthop Trauma Surg 1996;115:75-9. 11.Wang CJ, Chen HS, Huang TW. Shockwave Shockwave therapy for patients with plantar fasciitis: a one-year follow-up study. Foot Ankle Int 2002;23: 204-7. 12. Wang CJ, Chen HS, Chen WS, et al. Treatment of painful heels using extracorporeal shock wave. J Formos Med Assoc 2000;99:580-3. 13. Chen HS, Chen LM, Huang TW, et al. Treatment of painful heel syndrome with shock waves. Clin Orthop Relat Res 2001;387:41-6. 14. Wang CJ, Huang HY, Pai CH. Shock wave-enhanced neovascularization at the tendon-bone junction: an experiment in dogs. J Foot Ankle Surg 2002;41:16-22. 15.Wang CJ, Wang FS, Yang KD, et al. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J Orthop Res 2003;21: 984-9.. Extracorporeal Shock Wave Therapy. 16.Wang CJ. An overview of shock wave therapy in musculoskeletal disorders. [Review] Chang Gung Med J 2003;26:220-32. 17. Wang FS, Wang CJ, Huang HJ, et al. Physical shock wave mediates membrane hyperpolarization and Ras activation for osteogenesis in human bone marrow stromal cells. Biochem Biophys Res Commun 2001; 287:648-55. 18. Rompe JD, Kirkpatrick CJ, Kullmer K, et al. Doserelated effects of shock waves on rabbit tendo Achillis. A sonographic and histological study. J Bone Joint Surg Br 1998;80:546-52. 19. Rompe JD, Schoellner C, Nafe B. Evaluation of lowenergy extracorporeal shock-wave application for treatment of chronic plantar fasciitis. J Bone Joint Surg Am 2002;84:335-41. 20. Rompe JD, Decking J, Schoellner C, et al. Shock wave application for chronic plantar fasciitis in running athletes. A prospective, randomized, placebocontrolled trial. Am J Sports Med 2003;31:268-75. 21. Rompe JD, Meurer A, Nafe B, et al. Repetitive lowenergy shock wave application without local anesthesia is more efficient than repetitive low-energy shock wave application with local anesthesia in the treatment of chronic plantar fasciitis. J Orthop Res 2005;23:931-41..
(6) 235. 1990 2002. 7. 2003. 3. 37 1. 0.55 mJ/mm2 2. 12 (2. 12. 6.87 15.4. ). 6. 3. 1000 6. 40.5. (45. 86.9. 6. 12. ) 2.00. 35 1.05. 18.2. 1.73 85.7%. (43. ) 67.4% 72.1%. 2006;11:230-5. 404. 2. 2006. 4. 15. 2006. 9. 27. 2006. 7. 20.
(7)
數據
![Table 1. The Mayo clinical scoring system (Total 100 points) [7]](https://thumb-ap.123doks.com/thumbv2/9libinfo/8941984.270967/2.892.96.783.741.1127/table-mayo-clinical-scoring-total-points.webp)
相關文件
臺大機構典藏NTUR (National Taiwan University 二 Repository, http://ntur.lib.ntu.edu.tw) 經驗與協助推 動臺灣學術機構典藏TAIR (Taiwan Academic Institutional Repository,
In terms of contracted foreigners with work duration greater than 90 days, foreigner status and application process should be handled in accordance with regulations relevant to
But due to the careful construction of the middle state solution for the contact discontinuity, which is extremely important for many difficult multicomponent problems with strong
Weak solution for problems with shock & rarefaction waves Interface indicator H I takes value zero away from interfacs, yielding standard compressible Euler equations
A constant state u − is formed on the left side of the initial wave train followed by a right facing (with respect to the velocity u − ) dispersive shock having smaller
An elementary energy method is introduced in [18] based on a macro-micro decomposition of the equation into macroscopic and microscopic components to analyze the
different spectral indices for large and small structures Several scintil- lation theories including the Phase Screen, Rytov, and Parabolic Equa- tion Method
Other instruments and appliances, used in dental sciences, with low-frequency, high-frequency, ultrasonic and ultra-short wave
