Name of journal: World Journal of Obstetrics and Gynecology
ESPS Manuscript NO: 2827
Individualized Misoprostol Dosing for Labor Induction or Augmentation: A Review
Cheng SY
Individualized Misoprostol Dosing for Laboring women
Shi-Yann Cheng, MD, Department of Obstetrics and Gynecology, China Medical
University Beigang Hospital, 123 Shinder Road, Beigang Town, Yunlin County 65152, Taiwan.
Author contributions: Cheng SY solely contributed to this paper.
Correspondence to: Shi-Yann Cheng, MD, Department of Obstetrics and
Gynecology, China Medical University Beigang Hospital, 123 Shinder Road, Beigang Town, Yunlin County 65152, Taiwan. [email protected]
Telephone: +886-5 -783-7933 Fax: +886-5-783-6439 Received: March 18, 2013 Revised: April 30, 2013 Accepted:
Abstract
Cesarean birth rates are greater than 20% in many developed countries. The main diagnoses contributing to the high rate of cesarean births in nulliparous women are dystocia and prolonged labor. Traditionally, a policy of vaginal dinoprostone for the treatment of unripe cervix or early amniotomy with oxytocin administration for a ripened cervix has been associated with a modest reduction in the rate of cesarean births due to arrest disorders. However, the course of vaginal dinoprostone is tedious and oxytocin should be administered through an infusion pump, which may be inconvenient in certain settings. Because misoprostol has powerful uterotropic and uterotonic effects, and has become a common agent used in the practice of obstetrics and gynecology, the U.S. Food and Drug Administration (FDA) removed the absolute contraindication of the drug during pregnancy from its label in April 2002. However, excessive uterine contractility resulting in tachysystole or fetal distress is always a concern with the oral or vaginal use of fixed-dosage misoprostol. Therefore, misoprostol should be administered with caution to ensure that fetal hypoxia does not occur. A pilot trial of examining the use of very small, frequent, titrated oral misoprostol dosages administered every 2 hours was first conducted by Hofmeyr et al in 2001. Given women’s different metabolisms and responses to misoprostol, another method of titrating individualized oral
misoprostol with dosing administered every hour relative to uterine response was then developed by Cheng in 2006. Based on previous studies, this titration method is potentially an ideal alternative to traditional dinoprostone, oxytocin or the previously established misoprostol dosing method for labor induction or augmentation.
Key words: cervix; misoprostol; oxytocin; labor induction; labor augmentation
Core tip:
Cheng SY
Avoiding uterine tachysystole and fetal hypoxia is the critical consideration when implementing labor induction or augmentation with misoprostol. Titrated oral misoprostol is potentially an ideal alternative to traditional dinoprostone, oxytocin or the previously established misoprostol dosing method for labor induction or augmentation.
INTRODUCTION
There are many indications for term labor inductions and more than 15% of all gravid women require aid in cervical ripening. A labor course longer than that of spontaneous labor is the most commonly encountered problem associated with labor induction. Additionally, prolonged spontaneous labor in nulliparous women is another common problem, that can result in a negative birth experience[1,2] and can
be associated with a non-reassuring fetal heart rate (FHR) resulting in emergency cesarean delivery[3,4]. Considering the root cause of these problems, the unripe
cervix is the greatest barrier to spontaneous birth, which results in great concern and unnecessary cesarean deliveries. Therefore, overcoming an unripe cervix is a critical issue. Misoprostol, a synthetic prostaglandin E1 analogue, was initially used to treat peptic ulcers caused by prostaglandin synthetase inhibitors. Because misoprostol has been used off-label for a variety of indications in the practice of obstetrics and gynecology, including medication abortion, medical management of miscarriage, induction of labor, cervical ripening before surgical procedures, and the treatment of postpartum hemorrhage, the absolute contraindication of the use of misoprostol during pregnancy was removed from the label by the U.S. Food and Drug Administration (FDA) in April 2002[5]. Because misoprostol has
since 1992 to learn how to administer the drug while taking into consideration safety during labor induction[6-9]. Fetal hypoxia resulting from uterine tachysystole is
always an obstetrical concern[10-16]. The recommended dosage of misoprostol is 50
µg every 4 hours via the oral route or 25 µg every 4 hours via the vaginal route[17]
until adequate labor commences, but the induction duration is prolonged. Because the risk of inducing fetal hypoxia is incurred by using a fixed dosage of misoprostol, a pilot trial using very small, frequent, titrated oral misoprostol doses every 2 hour was first conducted by Hofmeyr et al in 2001[18,19]. It was concluded that this new
approach to oral misoprostol administration was successful in minimizing the risk of uterine hyperstimulation, which has been a feature of misoprostol use for labor induction, at the expense of a somewhat slower response in women with intact membranes and unfavorable cervices[19]. Given women’s different metabolic rates
and responses, another method of titrating individualized oral misoprostol with dosing administered every hour relative to uterine response was developed[20-23]. It
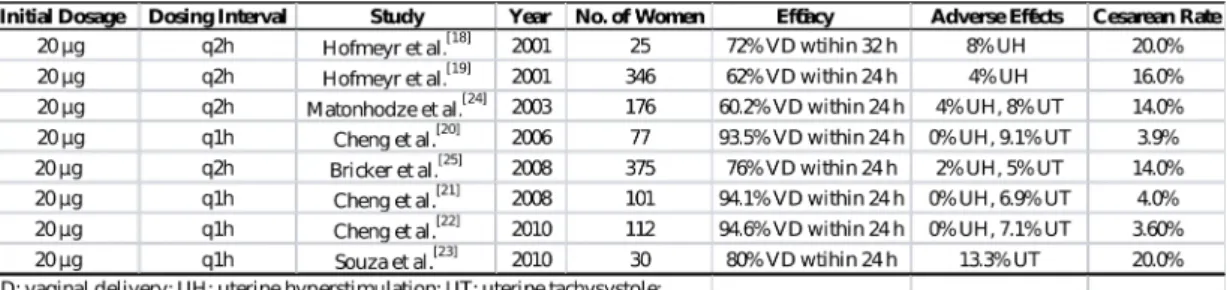
was observed that a higher success rate of vaginal delivery within 24 hours, not accompanied by a higher rate of uterine hyperstimulation, was achieved using the 1-hour oral misoprostol titration method (Table1). According to the results of titration studies, misoprostol is the ideal candidate agent for labor induction and augmentation due to its convenience of administration and cervical ripening
characteristics.
PRINCIPLE OF TITRATED ORAL MISOPROSTOL ADMINISTRATION
After misoprostol is absorbed, it undergoes rapid de-esterification to its free acid, which is responsible for its clinical activity and is detectable in the blood plasma[26].
Because misoprostol’s effects on and toxicity to the uterus based on serum concentrations of misoprostol acid at term are unknown, the rationale for titrated administration stems from the proven efficacy and pharmacokinetics of misoprostol, and the extreme inter- and intra-individual variation in uterine sensitivity[20]. To avoid uterine hyperstimulation and shorten the labor course,
misoprostol should be administered in small, frequent doses (one dose per hour, generally) titrated against the uterine response. This approach is analogous to the conventional, titrated use of oxytocin. Currently, misoprostol is available as an oral tablet of 100 or 200 µg and is water-soluble. Oral administration is easier and has greater acceptability among women than vaginal administration. Because the drug absorption is more rapid and more predictable, with a peak serum concentration after oral administration of 34 minutes and a half-life of 20–40 minutes[26], a 1-hour
interval between oral administrations and an increase in dosage of 20 µg every 4 hours from the initial 20-µg dosage were determined to be optimal based on a
mathematical model that takes these drug characteristics into consideration[20].
This method maintains a virtually steady serum level of misoprostol acid, thus avoiding large fluctuations and increases the peak serum concentration of the 20-µg absorptive misoprostol dose every 4 hours by a factor of 1.33. This mathematical model is described in Table 2.
CLINICAL PHARMACOLOGY OF MISOPROSTOL
Misoprostol does not affect the hepatic mixed-function oxidase enzyme systems. In patients with varying degrees of renal impairment, there is an approximate doubling of the T1/2, peak serum concentration (Cmax), and area under the serum concentration curve compared with those of normal patients, but no clear correlation between the degree of impairment and area under the serum concentration curve has been shown. No routine dosage adjustment is recommended in older patients or patients with renal impairment[27,28]. Misoprostol
does not produce clinically significant effects on the serum levels of prolactin, gonadotropin, thyroid-stimulating hormone, growth hormone, thyroxine, cortisol, gastrointestinal hormones, creatinine, or uric acid. Furthermore, gastric emptying, immunological competence, platelet aggregation, pulmonary function, and the cardiovascular system are not modified by the recommended doses of
misoprostol[28].Therefore, the use of misoprostol is not contraindicated in patients
with renal disease, severe anemia, systemic lupus erythematosus, hypertension, or heart disease.
RISKS OF MISOPROSTOL ADMINISTRATION
Uterine rupture is an unwanted risk of labor regardless of whether a woman has had a previous caesarean delivery. Most studies suggest that the use of misoprostol in women with a previous caesarean delivery increases the frequency of uterine scar disruption, either described as uterine dehiscence or overt uterine rupture[29-31].
There are even sporadic reports of uterine rupture in women without prior cesarean surgeries[32,33]. Grand multiparity appears to be a risk factor for uterine rupture in
the presence of misoprostol, although there is a report of uterine rupture in a primigravida[34]. Therefore, the indications for labor induction or augmentation must
be carefully evaluated prior to misoprostol administration.
PREPARING ORAL MISOPROSTOL SOLUTIONS AND GUIDELINES FOR ADMINISTRATION
Misoprostol is manufactured as an oral tablet and is water-soluble. The uterine activity produced by an oral solution is faster and stronger than that produced by an oral tablet or when administered via the rectal or vaginal route[35]. One 200-µg
bottle. The misoprostol solution needs to be used completely within 24 hours after preparation or discarded. Women are induced with one basal unit of 20 ml of misoprostol solution (1 µg/ml) prepared as described above. The determined volume of misoprostol solution is poured according to the obstetrician’s discretion at each dosing, following the guidelines of labor induction[21] or augmentation[22].
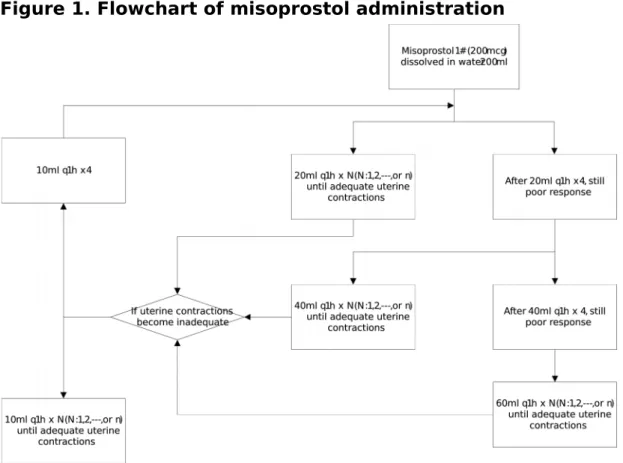
Initially, the determined volume may be given upon request by an obstetrician according to the guidelines when regular uterine contractions are not achieved. Once regular uterine contractions are achieved, the obstetrician is called to visit the patient and make a decision regarding the next dose or dosage adjustment, if any. Such individualized administration of misoprostol decreases the accidental fetal hypoxia resulting from uterine hyperstimulation. The flowchart of administration is shown in the Figure 1. The general misoprostol administration guidelines are as follows:
1. An initial dose of 20 µg/hour is administered and repeated hourly until adequate uterine contractions are achieved. If contractions do not occur after 4 doses, the dosage is increased to 40 µg/hour and repeated hourly until uterine contractions are achieved, for a maximum of 4 more doses. If the response still remains poor after 8 h, the dosage can be increased to 60 µg/hour until adequate contractions occur or a maximum cumulative dosage of 1600 µg is reached.
2. Adequate uterine contractions are defined as 3 or more contractions in a 10-minute period, over 30-10-minute windows. Once uterine activity is adequate for a 1-hour period, no further misoprostol is administered.
3. If the contractions subsequently become inadequate, hourly doses of misoprostol solution are started at 10 µg/hour and can be increased to 20 µg/hour, and perhaps 40 µg/hour, based on uterine responsiveness. This process is repeated until adequate uterine contractions occur or a maximum cumulative dosage of 1600 µg is reached.
4. Fetal heart rate and uterine activity are continuously monitored throughout the active phase of the labor course.
5. Induction failure is defined as not entering the active phase of labor after 36 hours of misoprostol treatment, with a maximum cumulative dosage of 1600 µg. Failure to progress is defined as cervical dilation or fetal descent without any progress for 3 hours after entering the active labor phase.
6. Intravenous magnesium sulfate (4 g over 30 minutes) or any other tocolytic agent available should be given at the physician’s discretion if uterine hyperstimulation occurs.
7. When the cervix achieves a Bishop score of 9, the artificial rupture of the membrane can be performed at the physician’s discretion.
contractions with a cervical dilatation of greater than 3 cm.
9. Supplemental oxytocin can be used at the physician’s discretion when uterine contractions are inadequate or when entering into the active phase of labor with a favorable cervix (Bishop score > 8) because of poor response to misoprostol. 10. Cesarean delivery is offered to all patients after induction failure, after failure of labor to progress, or when non-reassuring FHR patterns occur.
INDICATIONS AND CONTRAINDICATIONS FOR MISOPROSTOL ADMINISTRATION
The indications for labor induction with titrated oral misoprostol are the same as those for labor induction with oxytocin, including post-term pregnancy, preeclampsia, diabetes mellitus, oligohydramnios, intrauterine fetal growth restriction, and abnormal antepartum fetal surveillance results. However, to avoid adverse events, it is important for practitioners to be alert to contraindications, including a non-reassuring FHR pattern, uterine scarring, grand multiparity (≥ 5), any contraindication for labor or vaginal delivery or both, suspected placental abruption with an abnormal FHR pattern, and hypersensitivity to misoprostol or prostaglandin analogues.
In published case reports[36-38], accidental overdosing with misoprostol resulted in
pyrexia, hypoxia, and rhabdomyolysis; all occurred with a single drug intake at a dosage exceeding 3,000 μg. These adverse effects are signs of misoprostol toxicity and can be easily monitored when administering misoprostol. The other common side effects are nausea, vomiting, and diarrhea, but these side effects rarely occur in the course of labor induction or augmentation with titrated oral misoprostol. Furthermore, these side effects are easily relieved by medication.
First trimester exposure to misoprostol is associated with facial paralysis[39],
limb defects or vascular disruption defects[40,41] in newborns. In the Latina
American Collaborative Study of Congenital Malformations of 4673 malformed infants and 4980 control infants, increased frequencies of transverse limb defects, ring-shaped constrictions of the extremities, arthrogryposis, hydrocephalus, holoprosencephaly, and bladder exstrophy, but not Mobius syndrome, were observed in the infants exposed to misoprostol in utero[42]. There are no known
reports of teratogenicity upon misoprostol ingestion when taken after the first trimester.
EFFICACY OF TITRATED ORAL MISOPROSTOL
The 1-hour interval between titrated oral misoprostol administration based on pharmacokinetics has been proven to be effective in previous studies. One
randomized controlled trial of titrated misoprostol compared titrated oral with vaginal misoprostol for labor induction[21]. Women between 34 and 42 weeks of
gestation with an unfavorable cervix (Bishop score ≤ 6) and an indication for labor induction were randomly assigned to receive titrated oral or vaginal misoprostol. The titrated oral misoprostol group received a basal unit dose of 20 ml of misoprostol solution (1 µg/ml) every hour for 4 doses, then with titration based on individual uterine responses. The vaginal group received 25 µg every 4 hours until attaining a more favorable cervix. Vaginal delivery within 12 hours was the primary outcome. The data were analyzed on an intention-to-treat basis. Titrated oral misoprostol and vaginal misoprostol were given to 101 (48.8%) and to 106 (51.2%) women, respectively. Completed vaginal delivery occurred within 12 hours in 75 (74.3%) women in the titrated oral group and 27 (25.5%) women in the vaginal group (P < 0.01; relative risk [RR], 8.44; 95% confidence interval [CI], 4.52–15.76). Four women (4.0%) in the titrated oral group and 18 (17.0%) women in the vaginal group underwent cesarean deliveries (P < 0.01; RR, 0.20; 95% CI, 0.07–0.62). The incidence of hyperstimulation was 0.0% in the titrated oral group compared with 11.3% in the vaginal group (P < 0.01; RR, 0.08; 95% CI, 0.01– 0.61). Although more women experienced nausea (10.9%) in the titrated oral group (P < 0.01; RR, 27.07; 95% CI, 1.57–465.70), fewer infants had Apgar scores
of less than 7 at 1 minute in the titrated oral group compared with the vaginal group (P < 0.01; RR, 0.10; 95% CI, 0.01–0.76). The conclusion was that titrated oral misoprostol was associated with a lower incidence of uterine hyperstimulation and a lower cesarean delivery rate than vaginal misoprostol for labor induction in patients with unfavorable cervix.
Another randomized controlled trial compared oral titrated misoprostol with intravenous oxytocin for labor augmentation in women at 36-42 weeks of gestation with spontaneous onset of active labor[22]. Women meeting the general
selection criteria of having regular contractions, an effaced cervix dilated between 3 and 9 cm, and inadequate uterine contractions (2 or fewer contractions every 10 minutes) during the first stage of labor, were randomly assigned to titrated oral misoprostol or intravenous oxytocin. The augmentation-to-vaginal delivery interval and occurrence of vaginal delivery within 12 or 24 hours were the primary outcomes. The data were analyzed on an intention-to-treat basis. Of the 231 women, 118 (51.1%) and 113 (48.9%) were randomized to titrated oral misoprostol and titrated intravenous oxytocin, respectively. The median interval from the start of augmentation to vaginal delivery was 5.22 hours (3.77–8.58 hours, 25th–75th percentile) in the misoprostol group, and 5.20 hours (3.23–6.50 hours, 25th–75th percentile) in the intravenous oxytocin group (P = 0.019).
Complete vaginal delivery occurred within 12 hours for 92 (78.0%) women in the misoprostol group and 97 (85.8%) women in the oxytocin group (P = 0.121; RR, 0.91; 95% CI, 0.80–1.03). There were no significant differences between the 2 groups who delivered vaginally within 24 hours. Twelve (10.2%) women in the misoprostol group and 13 (11.5%) women in the oxytocin group underwent cesarean deliveries (P = 0.744; RR, 0.88; 95% CI, 0.42–1.85). The side effects and neonatal outcomes also did not differ between the two groups. The conclusion was that labor augmentation with titrated oral misoprostol or intravenous oxytocin resulted in similar rates of vaginal delivery within 12 and 24 hours.
A retrospective review of the medical records of all patients between 37 and 42 weeks of gestation with a Bishop score ≤ 6 who underwent labor induction with titrated oral misoprostol solution[43] has also been conducted. The women were
allocated into two groups: nulliparous and multiparous. The women received one basal unit of misoprostol solution (20 ml, 1 µg/ml) every hour for four doses; additional doses were titrated based on individual uterine responses. The latent and active phase intervals and occurrence of vaginal delivery within 12 hours were the primary outcomes. Of the 112 women included in the study, 49 (43.8%) nulliparae and 63 (56.2%) multiparae underwent labor induction with titrated oral misoprostol solution. Although fewer women delivered vaginally within 12 hours in
the nulliparous group than in the multiparous group (42.9% vs 85.7%; P < 0.01; RR, 0.54; 95% CI, 0.39–0.76), there was no significant difference between the two groups regarding vaginal delivery within 24 hours (87.8% vs 100.0%; P = 0.09; RR, 0.96; 95% CI, 0.90–1.02). Four (8.2%) women in the nulliparous group and none (0.0%) of the women in the multiparous group underwent caesarean deliveries (P = 0.02; RR 1.09; 95% CI, 1.00–1.18). All induction durations, including the latent and active phases, were significantly shorter in the multiparous group (P < 0.01). Induction failure did not occur in any patient in either of the groups. There was no instance of hyperstimulation, which was defined as tachysystole or hypertonus with a non-reassuring FHR pattern, although tachysystole , which was defined as the presence of at least 6 contractions in 10 minutes over at least 2 10-minute windows, occurred in 4 (8.2%) nulliparous women and 4 (6.3%) multiparous women. Hypertonus, defined as a single contraction lasting more than 2 minutes, did not occur in either group. None of the neonates in either group had Apgar scores of < 7 at 1 minute. The conclusion was that titrated oral misoprostol solution was a promising method of labor induction for both nulliparous and multiparous women.
Cesarean birth rates are greater than 20% in many developed countries[44]. The
main diagnoses contributing to the high rate of cesarean births in nulliparous women are dystocia and prolonged labor. Traditionally, a policy of vaginal dinoprostone for the treatment of an immature cervix or early amniotomy with oxytocin administration for mature cervices for the prevention of a delay in labor progress is associated with a modest reduction in the rate of cesarean births[45].
However, the course of vaginal dinoprostone or misoprostol is tedious, and excessive uterine contractility resulting in fetal distress is always a concern with the oral or vaginal use of fixed-dosage misoprostol. Oxytocin administration through the intravenous route needs to be under the control of an intravenous pump and may be inconvenient in certain settings. Because titrated oral misoprostol solution is easier to administer than titrated intravenous oxytocin, it is worth conducting these treatment regimens for labor induction or augmentation. In addition, misoprostol offers several advantages over dinoprostone and oxytocin, including a longer shelf life, stability at room temperature, and easy administration. It is an ideal alternative to traditional dinoprostone or oxytocin for labor induction or augmentation. In consideration of inter- and intra-individual variations of drug response during the dosing course, it is reasonable that the titrated oral misoprostol solution may replace fixed-dosage misoprostol via the vaginal or oral
route for labor induction or augmentation. In addition, the use of titrated oral misoprostol is superior to the traditional use of vaginal misoprostol in completing vaginal deliveries to reduce the cesarean rate, based on previous randomized controlled trials[21]. However, further studies are needed to determine the minimal
plasma misoprostol concentration necessary to induce a uterine response during labor induction at term and to validate the mathematical model of titrated oral misoprostol. This information will help ensure the obstetric use of misoprostol.
BIOGRAPHY
Shi-Yann Cheng received his MD degree from National Yang-Ming University, Taipei, Taiwan. He completed an extensive five-year obstetrics residency in Taiwan in the Department of Obstetrics and Gynecology, Veteran General Hospital, Kaohsiung. He is presently the Director of the Department of Obstetrics and Gynecology and Medical Education and Research at Medical China University Beigang Hospital and Lecturer in the School of Medicine at Medical China University, Taichung, Taiwan. His research interests cover clinical obstetrics and interdisciplinary collaborative care education, and his most notable contribution is the development of the concept of labor induction with titrated misoprostol solution with a focuse on dosing interval and uterine responses according to the pharmacokinetics of misoprostol. His CV lists 16 peer-reviewed publications, 2 book chapters,
prestigious medical education devotion awards, and presentations at national and international meetings.
REFERENCES
1 Waldenstrom U, Hildingsson I, Rubertsson C, Radestad I. A negative birth
experience: prevalence and risk factors in a national sample. Birth 2004;31:17-27. [PMID: 15015989 DOI: 10.1111/j.0730-7659.2004.0270.x] 2 Nystedt A, Hogberg U, Lundman B. Some Swedish women's experiences
of prolonged labour. Midwifery 2006;22:56-65. [PMID: 16488810 DOI: 10.1016/j.midw.2005.05.003]
3 Bugg GJ, Stanley E, Baker PN, Taggart MJ, Johnston TA. Outcomes of
labours augmented with oxytocin. Eur J Obstet Gynecol Reprod Biol 2006;124:37-41. [PMID: 15955617 DOI:10.1016/j.ejogrb.2005.04.015] 4 Florica M, Stephansson O, Nordstrom L. Indications associated with
increased cesarean section rates in a Swedish hospital. Int J Gynaecol Obstet 2006;92:181-5. [PMID: 16364324 DOI:10.1016/j.ijgo.2005.10.016] 5 ACOG Committee Opinion. Number 283, May 2003. New U.S. Food and
Drug Administration labeling on Cytotec (misoprostol) use and pregnancy. Obstet Gynecol 2003;101:1049-50. [PMID: 12738178]
6 Keirse MJ. Prostaglandins in preinduction cervical ripening. Meta-analysis
of worldwide clinical experience. J Reprod Med 1993;38:89-100. [PMID: 8429533]
Briones DK. Labor induction with the prostaglandin E1 methyl analogue misoprostol versus oxytocin: a randomized trial. Obstet Gynecol 1993;81:332-6. [PMID: 8437780]
8 Hofmeyr GJ, Gulmezoglu AM, Alfirevic Z. Misoprostol for induction of
labour: a systematic review. Br J Obstet Gynaecol 1999;106:798-803. [PMID: 10453829 DOI : 10.1111/j.1471-0528.1999.tb08400.x ]
9 Wing DA. Labor induction with misoprostol. Am J Obstet Gynecol
1999;181:339-45. [PMID: 10454679 DOI : 10.1016/S0002.9378(99)70558-2]
10 Bennett KA, Butt K, Crane JM, Hutchens D, Young DC. A masked randomized comparison of oral and vaginal administration of misoprostol for labor induction. Obstet Gynecol 1998;92:481-6. [PMID: 9764615 DOI : 1016/S0029-7844(98)00226-9]
11 Kolderup L, McLean L, Grullon K, Safford K, Kilpatrick SJ. Misoprostol is more efficacious for labor induction than prostaglandin E2, but is it associated with more risk? Am J Obstet Gynecol 1999;180:1543-50. [PMID: 10368502]
12 Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Database Syst Rev 2001:CD000941.
13 Shetty A, Danielian P, Templeton A. A comparison of oral and vaginal misoprostol tablets in induction of labour at term. BJOG 2001;108:238-43. [PMID: 11281461 DOI : 10.1111/.1471-0528.2001.00073.x]
14 Shetty A, Danielian P, Templeton A. Sublingual misoprostol for the induction of labor at term. Am J Obstet Gynecol 2002;186:72-6. [PMID: 11810088 DOI : 10.1067/mob.2002.118917]
15 Shetty A, Martin R, Danielian P, Templeton A. A comparison of two dosage regimens of oral misoprostol for labor induction at term. Acta Obstet Gynecol Scand 2002;81:337-42. [PMID: 11952465 DOI : 10.1034/j.1600-0412.2002.810411.x]
16 Alfirevic Z, Weeks A. Oral misoprostol for induction of labour. Cochrane Database Syst Rev 2006:CD001338. [PMID: 16625542 DOI: 10.1002/14651858.CD001338.pub2]
17 Weeks A, Alfirevic Z. Oral misoprostol administration for labor induction. Clin Obstet Gynecol 2006;49:658-71. [PMID: 16885670]
18 Hofmeyr GJ, Matonhodze BB, Alfirevic Z, Campbell E, de Jager M, Nikodem C. Titrated oral misoprostol solution--a new method of labour induction. S Afr Med J 2001;91:775-6. [PMID: 11680329]
19 Hofmeyr GJ, Alfirevic Z, Matonhodze B, Brocklehurst P, Campbell E, Nikodem VC. Titrated oral misoprostol solution for induction of labour: a
multi-centre, randomised trial. BJOG 2001;108:952-9. [PMID: 11563466 DOI: 10.1111/j.1471-0528.2001.00231.x]
20 Cheng SY, Chen TC. Pilot study of labor induction with titrated oral misoprostol. Taiwan J Obstet Gynecol 2006;45:225-9. [PMID: 17175468 DOI : 10.1016/S1028-4559(09)60229-1]
21 Cheng SY, Ming H, Lee JC. Titrated oral compared with vaginal misoprostol for labor induction: a randomized controlled trial. Obstet Gynecol 2008;111:119-25. [PMID: 18165400 DOI: 10.1097/01.AOG.0000297313.68644.71]
22 Ho M, Cheng SY, Li TC. Titrated oral misoprostol solution compared with intravenous oxytocin for labor augmentation: a randomized controlled trial. Obstet Gynecol 2010;116:612-8. [PMID: 20733443 DOI: 10.1097/AOG.0b013e3181ed36cc]
23 Souza AS, Scavuzzi A, Rodrigues DC, Oliveira RD, Feitosa FE, Amorim MM. [Titrated oral solution of misoprostol for labour induction: a pilot study]. Rev Bras Ginecol Obstet 2010;32:208-13. [PMID: 21085749 DOI : / 10.1590/S0100-72032010000500002]
24 Matonhodze BB, Hofmeyr GJ, Levin J. Labour induction at term--a randomised trial comparing Foley catheter plus titrated oral misoprostol
Med J 2003;93:375-9. [PMID: 12830603]
25 Bricker L, Peden H, Tomlinson AJ, et al. Titrated low-dose vaginal and/or oral misoprostol to induce labour for prelabour membrane rupture: a randomised trial. BJOG 2008;115:1503-11. [PMID: 18752586 DOI:10.1111/j.1471-0528.2008.01890.x]
26 Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorption kinetics of misoprostol with oral or vaginal administration. Obstet Gynecol 1997;90:88-92. [PMID: 9207820 DOI: 10.1016/S0029-7844(97)00111-7] 27 Foote EF, Lee DR, Karim A, Keane WF, Halstenson CE. Disposition of
misoprostol and its active metabolite in patients with normal and impaired renal function. J Clin Pharmacol 1995;35:384-9. [PMID: 7650228]
28 Searle: Cytotec (misoprostol)–full Revised Label 14 April, 2002 Available at:
[http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHu manMedicalProducts/ucm154498.htm] Accessed on 22 May, 2009.
29 Wing DA, Lovett K, Paul RH. Disruption of prior uterine incision following misoprostol for labor induction in women with previous cesarean delivery. Obstet Gynecol 1998;91:828-30. [PMID: 9572178]
30 Choy-Hee L, Raynor BD. Misoprostol induction of labor among women with a history of cesarean delivery. Am J Obstet Gynecol 2001;184:1115-7.
[PMID: 11349173 DOI: 10.1067/mob.2001.115177]
31 Blanchette HA, Nayak S, Erasmus S. Comparison of the safety and efficacy of intravaginal misoprostol (prostaglandin E1) with those of dinoprostone (prostaglandin E2) for cervical ripening and induction of labor in a community hospital. Am J Obstet Gynecol 1999;180:1551-9. [PMID: 10368503 DOI : 10.1016/S0002-9378(99)70051-7 ]
32 Bennett BB. Uterine rupture during induction of labor at term with intravaginal misoprostol. Obstet Gynecol 1997;89:832-3. [PMID: 9166339 DOI : 10.1016/S0029-7844(97)00036-7 ]
33 Khabbaz AY, Usta IM, El-Hajj MI, Abu-Musa A, Seoud M, Nassar AH. Rupture of an unscarred uterus with misoprostol induction: case report and review of the literature. J Matern Fetal Med 2001;10:141-5. [PMID: 11392596]
34 Thomas A, Jophy R, Maskhar A, Thomas RK. Uterine rupture in a primigravida with misoprostol used for induction of labour. BJOG 2003;110:217-8. [PMID: 12618171 DOI : 10.1046/1471-0528.2003.t01-2-02005.x]
35 Chong YS, Chua S, Shen L, Arulkumaran S. Does the route of administration of misoprostol make a difference? The uterotonic effect and
Eur J Obstet Gynecol Reprod Biol 2004;113:191-8. [PMID: 15063959 DOI : 10.1016/j.ejogrb.2003.09.011]
36 Graber DJ, Meier KH. Acute misoprostol toxicity. Ann Emerg Med 1991;20:549-51. [PMID: 1902633 DOI: 10.1016/S0196-0644(05)91614-2] 37 Bond GR, Van Zee A. Overdosage of misoprostol in pregnancy. Am J
Obstet Gynecol 1994;171:561-2. [PMID: 8059844]
38 Austin J, Ford MD, Rouse A, Hanna E. Acute intravaginal misoprostol toxicity with fetal demise. J Emerg Med 1997;15:61-4. [PMID: 9017489 DOI : 10.1016/S0736-4679(96)00257-0]
39 Pastuszak AL, Schuler L, Speck-Martins CE, et al. Use of misoprostol during pregnancy and Mobius' syndrome in infants. N Engl J Med 1998;338:1881-5. [PMID: 9637807 DOI:10.1056/NEJM199806253382604] 40 Gonzalez CH, Marques-Dias MJ, Kim CA, et al. Congenital abnormalities in
Brazilian children associated with misoprostol misuse in first trimester of pregnancy. Lancet 1998;351:1624-7. [PMID: 9620717 DOI:10.1016/S0140-6736(97)12363-7]
41 Vargas FR, Schuler-Faccini L, Brunoni D, et al. Prenatal exposure to misoprostol and vascular disruption defects: a case-control study. Am J Med Genet 2000;95:302-6. [PMID: 11186881 DOI : 10.1002/1096-8628(20001211)]
42 Orioli IM, Castilla EE. Epidemiological assessment of misoprostol teratogenicity. BJOG 2000;107:519-23. [PMID: 10759272 DOI : 10.1111/j.1471-0528.2000.tb13272.x]
43 Cheng SY, Hsue CS, Hwang GH, Chen W, Li TC. Comparison of labor induction with titrated oral misoprostol solution between nulliparous and multiparous women. J Obstet Gynaecol Res 2010;36:72-8. [PMID: 20178530 DOI: 10.1111/j.1447-0756.2009.01118.x]
44 Betran AP, Merialdi M, Lauer JA, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol 2007;21:98-113. [PMID: 17302638 DOI:10.1111/j.1365-3016.2007.00786.x]
45 O'Driscoll K, Foley M, MacDonald D. Active management of labor as an alternative to cesarean section for dystocia. Obstet Gynecol 1984;63:485-90. [PMID: 6700893]
Table 1. Comparison of Titrated Oral Misoprostol in Labor
Induction between Studies
Times t = 34 + 60n, n = 0,1,2,3, --- (minutes) Dosag e (mcg) 34 94 154 214 274 20 P 20 P(1/40+1/4 1) 20 P(1/40+1/41+1/4 2) 20 P(1/40+1/41+1/42+1/ 43) 40 P+P(1/40+1/41+1/42+1/43+1 /44) …
Set the function C = f(t), where
C: concentration of misoprostol acid (pg/ml) in plasma
t: times during the whole process, t = 34 + 60n (minutes), when taking misoprostol at n = 0, 1, 2, 3, ---(hours)
Tmax (the time to peak plasma concentration of misoprostol acid after absorption): 34 minutes
T1/2 (the half-life of misoprostol acid): 30 minutes as determined by a pharmacokinetics study
When n = 0, intake 20 µg, t = 34 minutes, set the peak plasma concentration of misoprostol acid, C = P
When n = 1, intake 20 µg, t = 34+(60×1) = 94 minutes, and C = P(1/40+1/41) When n = 2, intake 20 µg, t = 34+(60×2) = 154 minutes, and C = P(1/40+1/41+ 1/42)
When n = 3, intake 20 µg, t = 34+(60×3) = 214 minutes, and C = P(1/40+1/41+ 1/42+1/43)
When n = 4, intake 40 µg, t = 34+(60×3) = 214 minutes, and C = P+P(1/40+1/41 +1/42+1/43+1/44)
and so on.
Therefore, C = f(t) is a convergent series in which the upper limit = P/(1-1/4)+P/