中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/32401
117
0
0
全文
(2) . 中國醫藥大學碩士班研究生 論文指導教授推薦書. 針灸研究所,Pascale Schmied 鐵雲 君所提之論 文 A Study of Acupuncture Practice in Taiwan Today 台灣針灸使用現況調查研究,係由本人指導撰述, 同意提付審查。. 指導教授. 中. . 華. 民. 國. 九. 十. (簽章). 九. ii. 年. 七. 月. 一. 日.
(3) . 中 國 醫 藥 大 學 碩 士 班 研 究 生 論文口試委員審定書. 針灸研究所,Pascale Schmied 鐵雲 君所提之 論 文 A Study of Acupuncture Practice in Taiwan Today 台灣針灸使用現況調查研究,經本委員會審 議,認為符合碩士資格標準。. 論文口試委員會. 委員. (簽章). 所長. 中 華 民 國 九 十 九 年 七 月 十 四 日. . iii.
(4) . Contents Abstract. ..................................................................................................... 1. 1. Introduction.................................................................................................. 3 1.1 Practice of acupuncture in Taiwan......................................................... 3 1.2 Purpose of the research .......................................................................... 4 2. Literature review.......................................................................................... 5 2.1 Chinese Medicine in Taiwan.................................................................. 5 2.2 Plurality of Chinese Medicine................................................................ 8 Historical and Anthropological perspectives............................................ 8 Acupuncture clinical trial design ............................................................ 11 3. Methodology.............................................................................................. 13 3.1 Questionnaire contents ......................................................................... 13 3.2 Analysis methods ................................................................................. 15 Descriptive statistics ............................................................................... 15 Comparative statistics ............................................................................. 15 Questionnaire reliability ......................................................................... 17 4. Results ….................................................................................................. 19 4.1 Questionnaire distribution.................................................................... 19 4.2 Profile of the questionnaire respondents.............................................. 19 4.3 Use of acupuncture in general.............................................................. 25 Acupuncture in Chinese Medicine practice............................................ 25 Diseases treated by acupuncture............................................................. 32 4.4 Specific use of acupuncture for low back pain .................................... 44 Diagnosis of low back pain..................................................................... 44 Theory.................................................................................................. 44 Diagnosis methods .............................................................................. 47 Treatment of low back pain .................................................................... 52 Choice of acupuncture points.............................................................. 52 . iv.
(5) . Needles and needle technique ............................................................. 62 Retention time of the needles............................................................... 68 Frequency of the treatment ................................................................. 69 Co treatment ........................................................................................ 70 5. Discussion.................................................................................................. 72 5.1 Limitation of the research .................................................................... 72 5.2 Research method .................................................................................. 73 5.3 Questionnaire analysis ......................................................................... 74 Comparison of the factors....................................................................... 74 Correlation of the factors ........................................................................ 77 Example of the influence of the factors.................................................. 79 5.4 Integration in acupuncture practice...................................................... 80 6. Conclusion ................................................................................................. 82 Appendix: Questionnaire ........................................................................... 83 Bibliography............................................................................................... 94 Abstract in Chinese .................................................................................. 100 Notes......................................................................................................... 101. . v.
(6) . Tables Table 3.2.1 Factor 1: Education course .........................................................................15 Table 3.2.2 Factor 2: Age of the Chinese medicine physicians....................................15 Table 3.2.3 Factor 3: Years of practice..........................................................................16 Table 3.2.4 Factor 4: Type of hospitals..........................................................................16 Table 3.2.5 Factor 5: Geographical situation................................................................16 Table 3.2.6 Factor 6: Urbanisation ................................................................................16 Table 4.2.1 Age of the respondents ................................................................................19 Table 4.2.2 Chinese medicine course .............................................................................20 Table 4.2.3 Publications ..................................................................................................23 Table 4.2.4 Participation and contribution regarding the age of the physicians.......24 Table 4.2.5 Participation and contribution regarding the years of practice of the physicians .....................................................................................................24 Table 4.2.6 Participation and contribution regarding education course of the physicians .....................................................................................................25 Table 4.3.1 Factors associated with the treatment methods (1st Page) .......................30 Table 4.3.1 Factors associated with the treatment methods (Page 2) .........................31 Table 4.3.2 Factors associated with the categories of diseases treated by acupuncture (1st Page) .......................................................................................................41 Table 4.3.2 Factors associated with the categories of diseases treated by acupuncture (Page 2) .........................................................................................................42 Table 4.3.2 Factors associated with the categories of diseases treated by acupuncture (Page 3) .........................................................................................................43. . vi.
(7) . Table 4.4.1 Factors associated with the importance accorded to pattern identification.................................................................................................46 Table 4.4.2 Diagnosis tools: Percentage of “Not familiar with” regarding the years of practice .........................................................................................................49 Table 4.4.3 Diagnosis tools: Percentage of “Very important” regarding the type of hospitals ........................................................................................................50 Table 4.4.4 Diagnosis tools: Percentage of “Very important” regarding the type of hospitals ........................................................................................................50 Table 4.4.5 Factors associated with the importance accorded to the diagnosis tools .......................................................................................................................51 Table 4.4.6 Factors associated with the rational for choosing acupuncture points...59 Table 4.4.7 Factors associated with the importance accorded to the categories of acupuncture points (1st Page) ....................................................................60 Table 4.4.7 Factors associated with the importance accorded to the categories of acupuncture points (Page 2) ......................................................................61 Table 4.4.8 Factors associated with the importance accorded to the needles stimulation....................................................................................................65 Table 4.3.9 Factors associated with the respiratory supplementation and draining method ..........................................................................................................67. . vii.
(8) . Figures. Figure 1 Purpose of the research......................................................................................4 Figure 4.2.1 Degree obtained by the physicians............................................................20 Figure 4.2.2 Years of practice.........................................................................................21 Figure 4.2.3 Place of practice..........................................................................................22 Figure 4.2.4 Hospitals geographical situation ...............................................................22 Figure 4.3.1 Therapeutic methods used.........................................................................26 Figure 4.3.2 Frequency of the therapeutic methods used according the geographical situation .....................................................................................................27 Figure 4.3.3 Frequency of the therapeutic methods used regarding the cities and districts areas ............................................................................................28 Figure 4.3.4 Diseases categories treated by acupuncture.............................................32 Figure 4.3.5 Most common diseases treated by acupuncture ......................................33 Figure 4.3.6 Diseases categories treated by acupuncture according to the education course .........................................................................................................35 Figure 4.3.7 Treatment of the diseases of the respiratory system in relation to the age of the physicians.................................................................................36 Figure 4.3.8 Treatment of rheumatoid and immune diseases, neoplasm and diseases of the blood in relation to the age of the physicians ..............................37 Figure 4.3.9 Treatment of rheumatoid and immune diseases in relation to the years of practice ..................................................................................................37 Figure 4.3.10 Treatment of diseases in relation to the type of hospitals.....................40 Figure 4.4.1 Patterns identification 1.............................................................................44 Figure 4.4.2 Patterns identification 2.............................................................................45 . viii.
(9) . Figure 4.4.3 Diagnosis tools.............................................................................................47 Figure 4.4.4 Chinese medicine diagnosis tools ..............................................................48 Figure 4.4.5 Western medicine diagnosis tools .............................................................48 Figure 4.4.6 Most frequent acupuncture points used to treat low back pain ............53 Figure 4.4.7 Most used acupuncture points for the treatment of acute low back pain ....................................................................................................................54 Figure 4.4.8 Most used acupuncture points for the treatment of chronic low back pain ............................................................................................................55 Figure 4.4.9 Rationale for choosing acupuncture points..............................................56 Figure 4.4.10 Categories of acupuncture points ...........................................................56 Figure 4.4.11 Method of needle’s insertion ...................................................................62 Figure 4.4.12 Stimulation of the needles........................................................................63 Figure 4.4.13 Electrical stimulation of the needles regarding geographical situation ...................................................................................................................63 Figure 4.4.14 Supplementation and draining methods ................................................66 Figure 4.4.15 Retention time of the needles for acute and chronic low back pain ....68 Figure 4.4.16 Frequency of the visits for acute and chronic low back pain ...............69 Figure 4.4.17 Questionnaire results for co treatments used in the treatment of low back pain ..................................................................................................70. . ix.
(10) . A Study of Acupuncture Practice in Taiwan Today Post-Graduate Student: Pascale Schmied Advisor: Professor Yi-Shang Su Graduate Institute of Acupuncture Science, China Medical University. Abstract Acupuncture as a part of Chinese medicine is not a uniform field of knowledge and practice but known for its plurality. Historians of Chinese medicine, medical anthropologists or physicians conducting clinical trials, all underlined the plurality of diagnosis and practices in the field of Chinese Medicine. Although some literature analysed the case of Chinese medicine in Taiwan, mentioning the scope of acupuncture use, little is known about acupuncture practice particularly. The purpose of this research was to determine how education, the age and the years of practice of the Chinese medicine physicians and as well as the direct environment influence in their practice of acupuncture. In order to understand what leads to different practices, we designed a questionnaire. The questionnaire contained three parts. The first part gathered demographic data, the second part addressed questions about the general use of acupuncture and the third part concerned the diagnosis and treatment of low back pain. The questionnaire was sent to 403 Chinese medicine physicians practicing in Western and Chinese medicine hospitals and 177 physicians responded (44%). The results obtained trough the questionnaire showed that the geographical situation and the education course had a strong influence on the therapeutic methods used by the Chinese medicine physicians and on the categories of diseases treated by acupuncture. The age and the years of practice of the physicians were also correlated and the different type of hospitals showed some differences too. In the north of the island acupuncture . 1.
(11) . was more frequently used and physicians used to treat a larger scope of diseases categories with acupuncture. Special licence qualified physicians treated more categories of diseases with acupuncture than the physicians graduated of the school of Chinese medicine and the school of Post baccalaureate Chinese medicine. Older physicians having a long clinical experience also used acupuncture to treat a large variety of diseases. Then physicians working in Chinese medicine hospitals used to treat a larger scope of diseases categories with acupuncture and they founded more important to use Chinese medicine diagnosis tools than physicians working in Western medicine hospitals. The plurality found in acupuncture practice is a complex process where different factors interact at different levels. The geographical situation and the education background were the two main factors influencing acupuncture practice. However, further studies are needed to understand the situation of acupuncture practice in private clinic and examine the role played by the health insurance coverage.. Keywords: Taiwan, acupuncture, questionnaire, western medical hospital, Chinese medical hospital. . 2.
(12) . 1. Introduction 1.1 Practice of acupuncture in Taiwan Acupuncture is widely practiced in Taiwan. Most of the time it is used with other therapeutic techniques of Chinese medicine (prescription of Chinese medicinal, manipulation techniques, etc.), there are very few Chinese medicine practitioners who rely solely in acupuncture. Nevertheless in some hospital there is a specialized department of acupuncture, where the physicians practice mainly acupuncture. In Taiwan, only licensed Chinese medicine physicians can legally dispense acupuncture. There are two distinct ways of being legally recognized as a Chinese medicine physician in Taiwan: through the Chinese Medicine Physician Licence Examination and through the Chinese Medicine Physician Special Licence Qualifying Examination. The former is only open to the students issued from the courses dispensed at China Medical University (undergraduate course or Post baccalaureate course) or at Changgung1 University while the latter do not require a Chinese medicine institutional background. Chinese medicine physicians practice mainly in private clinics but also in Chinese medicine hospitals and in Western medicine hospitals that possess a Chinese medicine unit or a specialised department of acupuncture. Non-recognized practitioners also practice acupuncture, but we choose not to take in account this part of the Taiwanese reality. Therefore the present research is limited to the field of legal acupuncture practice and do not take into account other forms of popular practice used in Taiwan.. . 3.
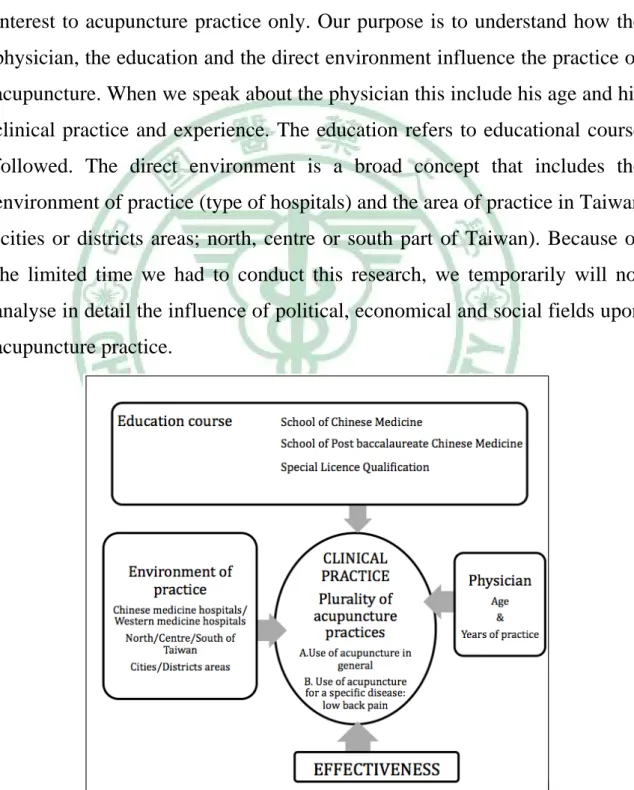
(13) . 1.2 Purpose of the research Acupuncture as a part of Chinese medicine is not a uniform field of knowledge and practice but known for its plurality. The purpose of this research was to determine what leads to the plurality of acupuncture practice we observed. We wanted to focus on Taiwan area and chose to take an interest to acupuncture practice only. Our purpose is to understand how the physician, the education and the direct environment influence the practice of acupuncture. When we speak about the physician this include his age and his clinical practice and experience. The education refers to educational course followed. The direct environment is a broad concept that includes the environment of practice (type of hospitals) and the area of practice in Taiwan (cities or districts areas; north, centre or south part of Taiwan). Because of the limited time we had to conduct this research, we temporarily will not analyse in detail the influence of political, economical and social fields upon acupuncture practice.. Figure 1 Purpose of the research . 4.
(14) . 2. Literature review 2.1 Chinese Medicine in Taiwan The recent history of acupuncture as a part of Chinese medicine in Taiwan differs considerably of what happen in mainland China this past century. In Taiwan, before the Japanese colonization, Chinese medicine was the predominant medical system used. The education of Chinese medicine was assured in the most usual way it has been held under the past centuries: through apprenticeship and self-study2. When the Japanese arrived to Taiwan in 1895 they began to replace Chinese medicine by Western medicine, and established the first school of modern Western medicine, which was also in charge for the training of Chinese medicine practitioners 3 . During the Japanese colonisation (1885-1945), Western medicine became the leading medical system and even Chinese medicine was still practiced, the Japan’s hostile policy towards Chinese medicine had a devastating effect that lead to a tremendous drop of Chinese medicine physicians4. When the Japanese left Taiwan in 1945 only a few dozen of physician remained (from the initial 1903 Chinese medicine physicians recognized by the Japanese7 government in. 1901) 5. .. The Chinese nationalist government came to Taiwan in 1945 and pursued the policy held in mainland China. During 1945 to 1954, because of the massive arrival of immigrants from Mainland China, coupled by a loosened governmental regulations and control of Chinese medical practice, the number of licensed Chinese medicine practitioners suddenly increase from two dozen physicians in 1945 to 1545 physicians in 1954. As Chi remarked this was both beneficial and treacherous for the sake on Chinese medicine. In one hand, it allowed the Taiwanese population to have a wider . 5.
(15) . access to Chinese Medicine. In another hand, because of the poor quality of some practitioners the public trust toward licensed Chinese Medicine physicians was reduced6. A licensure system examination was established by the nationalist government in 1946 and was open to anybody without a specific educational background. This licensure is named Chinese Medicine Physician Special Licence Qualifying Examination (referred as special licence qualification) and is still in effect today. It is organized in a more or less regular basis of every one or two years7. In 1958 the China Medical College (named China Medical University CMU until 1999) was establish but it is only in 1966 that the institutionalized education of Chinese medicine really began with the establishment of the department of Chinese medicine, whose aim was to “develop Chinese Medical science, catch up with modern Western medical sciences, and to combine Chinese and Western medical science in order to establish a new system of medical science”4. In this department, the students took a seven years course (the course was extended to eight years until 1996) and study jointly Chinese and Western medicine. At the end of their studies and internship they can take the examinations to have a licence both in Chinese Medicine and in Western Medicine, but they are not allowed to practice under the both licence at the same time. Until 1995 a lot of students issued from this courses chose to be registered as Western medicine physicians principally because of the higher income and the social prestige conferred by this position8. In 1975, the university established a graduate school of Chinese medicine (a master degree in 1975 and a doctoral degree in 1987) in order “to combine ancient, current, domestic and foreign medical knowledge, to develop Chinese medicine in general and to train teacher of Chinese medicine”4. Ten years later, in 1984, the university created a school of Post baccalaureate Chinese medicine. It offered a five years course to. . 6.
(16) . train graduate students to become Chinese medicine physicians. Then in 1996, Changgung University opened a seven years course in Chinese medicine more or less similar as China Medical University. The teaching and practice of acupuncture is a part of the whole course of a Chinese medicine physician. It is a therapeutic technique among others and does not require specialised course. Nerveless, it exist a specific course of acupuncture open to Western medicine physicians and dentists that offer them a quick formation (a hundred of hours). From 2005, the China Medical University opened a master degree in acupuncture research whose aim is “to cultivate the qualified acupuncture teachers and specialists for research and development purpose”. In the beginning of the seventies, political policy engaged to encourage Chinese medicine and particularly acupuncture. The Chinese Acupuncture association (中國針灸學會) was created in 1957 but it is only in 1972 that a centre for acupuncture research was created. Following his creation, the first symposium on acupuncture and moxibustion was held. The international recognition of acupuncture abroad helping this process led, in 1982, to the first international symposium organized by the Department of Health and the China Medical College. This symposium gathered over 1000 experts and the aim of this meeting was to unify the academic theories and concepts and therefore enabling scholars to communicate and to promote the interaction between Chinese and Western medicine9. A. Kleinman has explored the case of Chinese medicine in Taiwan from an anthropological perspective10. He offered a broad description of the health care system in Taiwan at the end of the seventies. He distinguished three sectors into the health care system: the popular one, the professional one and the folk sector. He explained how popular, professional and folk culture shape illness and therapeutic experiences in distinct ways. He showed that . 7.
(17) . the professional sector as an institution posses a large power « to create illness and treatment as social phenomena, to legitimate a certain construction of reality, as the only clinical reality » 11 . From this point of view he showed that Western Medicine control most of the power letting few place to other therapeutic systems, including Chinese medicine. Some other studies focused more on Chinese Medicine, like C.C. Chi, who offers a condensed description of the education, training and licensure system of Chinese medicine physicians in Taiwan3. L.D. Chen, in his doctoral thesis, explored in detail the characteristics of the Chinese Medicine practitioners linked to different educational backgrounds5. Other articles about the uses of Chinese medicine in Taiwan have demonstrated the general increase of use of Chinese Medicine the last decades especially until its inclusion in the heath care system12,13,14. All these studies help us to understand the actual trends of Chinese Medicine in Taiwan. Nevertheless very few studies have addressed the case of acupuncture. The few articles related to acupuncture focused on the pattern of acupuncture use and the characteristics of the patients12.. 2.2 Plurality of Chinese Medicine The plurality found in Chinese Medicine has been subject to much interest and has been approach under different point of views. Historical and Anthropological perspectives From an historical perspective, P. Unschuld15 has underlined the variety of Chinese medicine trends and corrected the common idea in the West understanding Chinese Medicine as an homogeneous tradition. Kuriyama16 in his comparison between the history of ancient Greek and Chinese medicine has noted some essential differences between the two medicines. He . 8.
(18) . explained clearly how the perception of and theories about the body differed in the two cultures and therefore in the two medicines. Even if his book is about ancient medicine it still give us some interesting clue to reflect about the particular features of Chinese medicine and to understand the position of a Chinese medicine actually embed in a health care system dominated by the paradigm of Western medicine. The multiplicity of Chinese medicine has been under the scope of medical anthropologists. J. Farquhar, focusing her research on the clinical encounter in Chinese medicine, underlined the fact that in Chinese medicine the knowledge are directly related to the practice and therefore to the physician. She also showed how, in Chinese medicine, illness is transformed into an actionable pattern with the help of a classificatory logic. This logic allows some flexibility and improvisation in the process of diagnosis and treatment17. She therefore described the central position of the physician in mastering Chinese medicine, as well as a certain range of freedom he had making diagnosis and treatment. E.Hsu has examined the variation of key concepts of Chinese medicine under different mode of transmission (secret, personal and standardized mode of transmission)18. She underlined that different ways of learning also implied different ways of knowing. Therefore she demonstrated the difficulties for the actual standardized way of teaching Chinese medicine to match with the clinical practice reality, a problem that didn’t exist before the standardization the knowledge. She explained how “Chinese medicine uses word meanings to manipulate reality in a very different way from that the twentieth century Western science” that is to say the Chinese character has a multiplicity of meaning 19 that allow flexibility and helps the physician to deal with the clinical reality20. . 9.
(19) . V. Scheid, in his impressive work, has offered an outstanding explanation of the plurality of Chinese medicine 21 . He used ethnographic methods as well as theories from the Science and Technology Studies (STS) to understand field of human practices. For him three interrelated features define this plurality. The first one is the heterogeneity found in Chinese medicine, that is to say the fact that different domains (like biomedicine, calligraphy, painting among others) and various periods of time permeate Chinese medical tradition and practitioners. The second feature is the multiplicity, it is a consequence of heterogeneity and a product of outside influences that leads to a variety of ways of thinking about body, diagnosis and treating illnesses. Both features are descriptive concepts emphasizing the plural constitution of the field of Chinese medicine practice. The last feature is the synthesis, it is a result or product of the interaction of different infrastructures. It is more a concept employed to understand the constitution of Chinese medicine practice as “a process of simultaneous emergence and disappearance”22 of concepts and practices. His account offers a detailed and helpful explanation of the plurality found in Chinese Medicine. In another article, V. Scheid described how Chinese medicine physicians use to combine knowledge issued from Chinese and Western medicine without major problem because of the openness, flexibility and adaptability, that are some key characteristics of Chinese Medicine23. His account shows how physicians in their daily practice synthesize two different kinds of medicine without conflict or contradiction. Both historical and anthropological approaches offer a solid and broad view of the essence and specificity of Chinese Medicine. They show some key features of Chinese medicine that can help us to understand the plurality we found in acupuncture practice. These approaches also offer reflexions about Chinese Medicine development, assimilation and adaptation process . 10.
(20) . from the past until today. Therefore it is possible to distinguish how Chinese medicine and particularly acupuncture has been transformed and adapted to fit the modern Taiwanese health care system. Acupuncture clinical trial design More specific, some other studies about acupuncture were conducted by physicians worried to find a unity to conduct clinical trial. These studies focused on differential diagnosis and variety of treatment of the low back pain (in the United States and in United Kingdom). In their literature review of Chinese medicine treatment of low back pain, Birch and Sherman concluded that there are many explanatory models, approaches to practice and techniques used by acupuncturists24. In another study, Sherman and al. showed the influence of the practitioner identity on recorded diagnosis as well as on acupuncture point prescriptions 25 . The result of a survey conducted by the same researchers demonstrated that Chinese medicine physicians used several different diagnoses for the same Western medical diagnosis and used a great variety of Chinese medicine treatments 26 . In another paper, Hogeboom et al. showed that the teaching and practice of acupuncture was heterogeneous and that the variations in training contributed to the variability of styles of diagnosis and treatments 27 . MacPherson et al. stated the diversity found in acupuncture practice shows that this medical tradition is not static, “there are no clear boundaries as to what constitutes the practice of acupuncture as it continues to adapt and evolve over time”28. In an article, Kalauokalani et al. showed that despite a difference of theory in the choice of acupuncture points between physician and non physician acupuncturists in the US, the final selection of acupuncture points to treat low back pain was almost the same for the two types of physicians29. The last article put in light an interesting point that is. . 11.
(21) . even the theory for choosing the acupuncture points sometimes differ, the selection of points is often quite similar at the end. Almost all these studies stated the variety of diagnosis and treatment used by different acupuncturists to cure low back pain but they didn’t try to explain the plurality found in acupuncture practice.. . 12.
(22) . 3. Methodology In order to understand what’s lead to the plurality found in acupuncture practice, we conducted several fieldworks and interviews. A questionnaire was designed from our observations and literature review about acupuncture practice. Besides, our involvement to China Medical University master degree courses gives us access to many useful information. From the discussions with professors and classmates to the participation to undergraduate courses inside and outside the university, we gathered very different points of view about acupuncture practice.. 3.1 Questionnaire contents The questionnaire contained nine pages and took twenty minutes to complete. It was pretested among the students and professors of the acupuncture research department. Then it was also distributed in two meetings organized by Chinese medicine physicians association in Tainan and Taichung. Finally we asked five professors and clinically experimented physicians of China Medical University to give their advice about the content and the design of the questionnaire. We amended the questionnaire with regards to the reaction and advices of the professors, physicians and students. The questionnaire contained three parts: 1.. The first part contained items about demographic data (age, sex,. clinical experience, type of practice), learning and mastering processes, participation and contribution of the physician to medical world and about the environment of practice (medical structure of practice, location of professional practice, NHI participation).. . 13.
(23) . 2.. The second part concerned the general use of acupuncture. We. measured the place of acupuncture treatment among other therapeutic methods used in Chinese medicine. Then we evaluated the scope of acupuncture use, that is to say, for which category of diseases Chinese medicine physicians frequently use acupuncture. The evaluation of the second part of the questionnaire was done by using a range of five gradations: 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Every items corresponded to an approximate number of patients: Never used = no patients; Rarely = if 100 patients, used on 1 to 25 patients; Occasionally = if 100 patients, used on 25 to 50 patients; Frequently = if 100 patients, used on 50 to 75 patients; Very frequently = if 100 patients, used on 75 to 100 patients. 3.. The third part was specifically about the diagnosis and. treatment of low back pain. In the first sub part the physician were asked to explain which kind of diagnosis tools he will use to diagnose low back pain. The second sub part concerned the treatment of low back pain. We asked question about needles techniques, stimulation of the needles and acupuncture points. We evaluated the importance the physician accorded to each item by his reply within a four gradations answer: 1. Not familiar with; 2. Not important; 3. Important; 4. Very important. Then doctors were asked to describe three acupuncture points they frequently use to treat acute and chronic low back pain, the retention time of the needles and the frequency of the treatment. Finally, we enquired about the co treatment methods they will frequently use to cure low back pain.. . 14.
(24) . 3.2 Analysis methods The data collected though questionnaire were entered to Microsoft Excel then exported and analysed through SPSS. Descriptive statistics We first analysed the data using simple descriptive statistics. The results are reported through the analyses of frequencies and we used valid percent to present the data in the figures and tables. Comparative statistics Our aim was to understand how the physician, his Chinese medicine education course and the environment influenced his acupuncture practice. Therefore we chose six groups of factors, which were the age of the physician, his years of clinical practice, his education course, the type of hospital he works in, the geographical situation of the hospital and the density of urbanisation. The different groups were subdivided into different variables and we performed the chi-square test to determine if there were notable differences between the variables into each group with regards to acupuncture practice. Table 3.2.1 Factor 1: Education course Variable 1. School of Chinese medicine. Variable 2. School of Post baccalaureate Chinese medicine. Variable 3. Special license qualification examination. Table 3.2.2 Factor 2: Age of the Chinese medicine physicians. . Variable 1. Under 30 years. Variable 2. 30 to 39 years. Variable 3. 40 to 49 years. 15.
(25) . Variable 4. 50 and more years. Table 3.2.3 Factor 3: Years of practice Variable 1. 1 to 5 years. Variable 2. 6 to10 years. Variable 3. 11 to 20 years. Variable 4. More than 20 years. Table 3.2.4 Factor 4: Type of hospitals Variable 1. Teaching hospital. Variable 2. Regional hospital. Variable 3. Rural hospital. Variable 4. Chinese medicine hospital. Table 3.2.5 Factor 5: Geographical situation Variable 1. North. Variable 2. Centre. Variable 3. South. For the distinction between North, Centre and South, we used the National Health Insurance district boundaries that divided the countries in six regions30. The North referred to the northern region and the Taipei area, the Centre to the central region and the South to the southern region and the Kaoping region. We didn’t include the eastern region because the sample was too small to be computed in the statistics.. Table 3.2.6 Factor 6: Urbanisation. . Variable 1. Cities area. Variable 2. Districts area. 16.
(26) . The cities and districts areas are administrative boundaries planned out by the Taiwanese government. We assumed that cities areas were more urbanized than districts areas. The cities areas included Taipei city, Keelung city, Hsinchu city, Taichung city, Chiayi city, Tainan city and Kaohsiung city. The districts areas included all the districts in the north, central and south part of the island. For the questions 2.1 and 2.2 in the second part of the questionnaire, which included a frequency rating (Never used=0; Rarely=1; Occasionally=2; Frequently=3; Very frequently=4), we also performed the one-way Anova test (the T test for the comparison between cities and districts areas) to determine the differences of frequencies between the different variables. Then we used the post hoc analysis Tukey’s test to determine which variable were significantly different and which were not. Finally in order to test the potential association of the different groups of factors with the items of our questionnaire we performed a multiple linear regression analysis for the questions concerning the treatment methods (question 2.1), the diseases categories treated by acupuncture (question 2.2), the importance accorded to the diagnosis tools (question 3A1), the importance accorded to the pattern identifications (question 3A2), questions about needles techniques (questions 3B4 and 3B5) and the rational for choosing acupuncture points as well as the importance accorded to acupuncture points categories (question 3B6). Questionnaire reliability We tested the validity of the questionnaire on 14 physicians. After of the reception of the first questionnaire we sent back two weeks later the same questionnaire and analysed the reliability of the answers. We tested the main questions of the questionnaire: 2.1 (15 items); 2.2 (16 items); 3A1 (16 items); 3A2 (4 items); 3B4 (4 items); 3B5(6 items) and 3B6 (12 items). If . 17.
(27) . we reported the average measure of ICC (Intraclass correlation) we obtained an average of 0.7 that signify a very good reproducibility. If we reported the single measure of ICC, we obtained an average of 0.53, which still indicate a fair reproducibility 31 . The two main questions which obtained the lower alpha value were the question 3A1 (Alpha= 0.49) and 3A2 (Alpha= 0.46), which concerned the diagnosis tools.. . 18.
(28) 4. Results 4.1 Questionnaire distribution The questionnaire was send to 403 Chinese medicine physicians working in hospitals. We selected Chinese medicine hospitals and Western medicine hospitals32 with a department of Chinese medicine. The physicians that received the questionnaire were asked to carefully fill it, in return they will obtain 2 credit points from the Chinese Medical Association of Acupuncture 33 (中華針灸醫學會). From the 403 questionnaire sent, 177 physicians returned the questionnaire (44%). However, only 160 questionnaires were used for this study (39.9%). We excluded 17 questionnaires because 11 were blank with sometimes a note explaining that the Chinese medicine physician didn’t use acupuncture as a therapeutic method. The 6 other questionnaires were excluded because they contained too much missing data.. 4.2 Profile of the questionnaire respondents The age range of the respondents of the questionnaire was from 28 to 75 years, the average age was 39 years. Table 4.2.1 Age of the respondents Age of the respondents (n=159). . Under 30 years. 6.9%. 30 to 39 years. 44.7%. 40 to 49 years. 43.0%. 50 years and more. 14.5%.
(29) . A majority of respondents were male (67%). The results showed a female predominance in younger physicians (group age: “under 30 years” and “30 to 39 years”). This result was also correlated with the years of clinical practice where we found less female physicians with a long clinical experience. Most of the physicians obtained a bachelor degree in Taiwan. A lot of them also had a master degree. A few possessed a PhD but one third of these PhD were issued from mainland China.. Figure 4.2.1 Degree obtained by the physicians. A majority of the respondents were graduated from the school of Chinese medicine and the school of Post baccalaureate Chinese medicine. Table 4.2.2 Chinese medicine course Chinese medicine course (n=160) School of Chinese medicine. 51.3%. School of Post baccalaureate Chinese medicine. 44.4%. Special licence qualification. 4.4%. In the school of Post baccalaureate Chinese medicine, we found a larger proportion of female physicians (41.5%) than in the other groups (25.7% for . 20.
(30) . the school of Chinese medicine and 14.3% for the special licence qualification group). The special licence qualified physicians were older than the physicians in the two other groups, 86% of them fell in the categories of “40 to 49 years” and “50 and more years” (49% for the physicians of the school of Chinese medicine and 45% for the physicians of the school of Post baccalaureate Chinese medicine). Furthermore, they were working only in regional hospitals (71.4%) and teaching hospitals (28.6%). For the two other groups, the physicians were distributed in all the different hospitals. The majority of the respondents didn’t have a lot of clinical experience. Their average years of practice was 7 years (from 1 to 36 years). A large proportion of the physicians of the school of Chinese medicine and the school of Post baccalaureate Chinese medicine fell in the category of “1 to 5 years” of clinical practice. In comparison the special licence qualified physicians had more clinical experience, 43% of them had more than 10 years of clinical experience (37% for the physicians of the school of Chinese medicine and 19% for the physicians of the school of Post baccalaureate Chinese medicine).. Figure 4.2.2 Years of practice . 21.
(31) . Most of the physicians worked in a teaching hospital or a regional hospital. The location of the hospitals within cities areas or a districts areas was well balanced. 56% of the hospitals were situated in cities areas and 46% in districts areas.. Figure 4.2.3 Place of practice. Figure 4.2.4 Hospitals geographical situation. . 22.
(32) . There were a majority of hospitals situated in the North, but the three regions were well represented. The teaching hospitals were distributed in the three parts of the island. A majority of rural hospitals were located in the central part of the island and the Chinese medicine hospitals were mainly situated in the North and in the South. The rural hospitals were more likely to be located in districts areas and the Chinese medicine hospitals were mainly located in cities areas. Teaching and regional hospitals were almost equally distributed between cities and districts areas. We found a high rate of teaching experience as well as publication that showed an active participation and contribution of the physicians to the medical field. 60.6% of the physicians had teaching experience and 60% of the physicians published articles. Most of the publications were in Chinese. Table 4.2.3 Publications Publication. Chinese journal 48.8%. SCI journal 6.9%. Chinese & SCI journals 4.4%. This participation was related to the age, the years of practice and the education background. In general, teaching experience, publications and participation of international meeting showed a higher rate for the older physicians and for physicians with a long clinical practice. Statistical evidences demonstrated that the teaching experience was correlated to the age and years of practice of the physicians and that the age was also related to the publication’s rate.. . 23.
(33) . Table 4.2.4 Participation and contribution regarding the age of the physicians Age. Under 30 years. 30 to 39 years. 40 to 49 years. 50 years and more. Teaching experience*. 18.2%. 53.5%. 78.2%. 60.9%. Publication*. 18.2%. 49.3%. 78.2%. 69.6%. Participation to international meetings. 27.3%. 20.3%. 31.5%. 36.4%. Table 4.2.5 Participation and contribution regarding the years of practice of the physicians Years of practice. 1 to 5 years. 6 to 10 years. 11 to 20 years. More than 20 years. Teaching experience*. 44.1%. 68.9%. 79.4%. 77.8%. Publication. 50.0%. 62.2%. 73.5%. 77.8%. Participation to international meetings. 27.9%. 16.7%. 35.3%. 37.5%. It is interesting to note that younger physicians and physicians with less years of clinical practice were more used to teach in students or public associations as older physicians and physicians with more years of clinical practice were teaching in universities, hospitals, medical associations or opening their own classes. The education background also played a role even there was no statistical evidence for it. Special licence qualified physicians showed a higher rate of participation and contribution. They were mainly teaching in medical associations, student or public associations or having their own class. Physicians from the school of Chinese Medicine were more likely to teach in the universities and finally physicians of school of Post baccalaureate Chinese medicine were less involved in teaching than the two other groups. . 24.
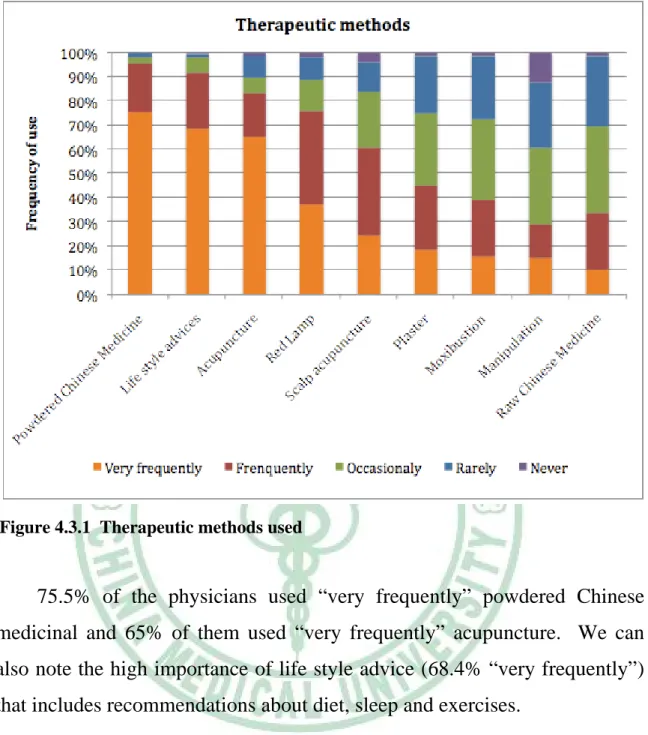
(34) . Table 4.2.6 Participation and contribution regarding education course of the physicians Special licence qualification. 66.2%. School of Post baccalaureate Chinese medicine 53.7%. Publication. 67.6%. 52.4. 71.4%. Participation to international meetings. 30.0%. 22.8%. 49.2%. Education background. School of Chinese medicine. Teaching experience. 85.7%. 4.3 Use of acupuncture in general Acupuncture in Chinese Medicine practice Chinese Medicine is characterized by its multiplicity of therapeutic methods, the main ones are the medicinal treatment and the acupuncture and moxibustion treatments, besides comes the manipulations techniques 34 including massage or tuina and the prevention techniques that optimize the circulation of Qi like Qigong. Finally other minor techniques as cupping, guasha, bloodletting, the application of plasters and fumigations are also frequently used. In Taiwan, one Chinese medicine physician usually relies on many therapeutic methods35. Nevertheless some choose to specialize only in the field of medicinal treatment, some others use both acupuncture and medicinal treatment and add others techniques like manipulation, cupping, guasha and so on. Therefore acupuncture is one of the therapeutic methods used by Chinese Medicine physicians. The data obtained through the questionnaire showed that the most used therapeutic method was the powdered Chinese medicinal, followed by life style advices and then acupuncture.. . 25.
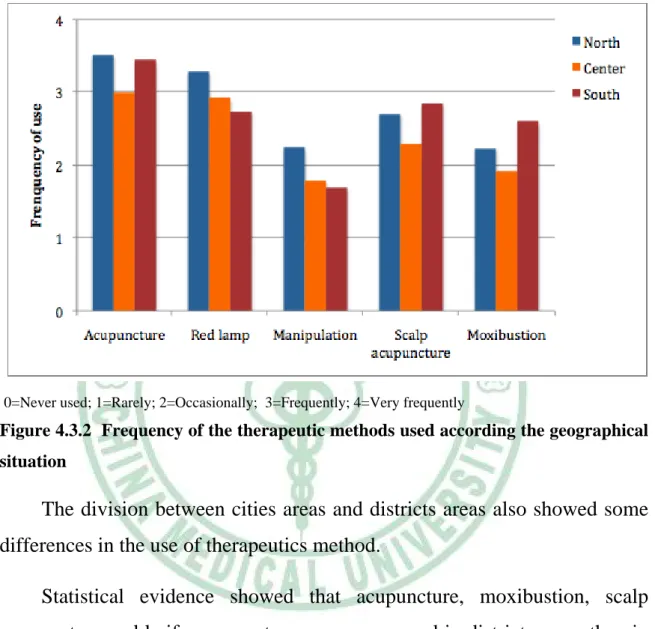
(35) . Figure 4.3.1 Therapeutic methods used. 75.5% of the physicians used “very frequently” powdered Chinese medicinal and 65% of them used “very frequently” acupuncture. We can also note the high importance of life style advice (68.4% “very frequently”) that includes recommendations about diet, sleep and exercises. Statistical evidence demonstrated that the different therapeutic methods were strongly correlated with geographical and urban environment. There were evidences that acupuncture was more widely used in the North than in the centre of Taiwan. The manipulations methods and the use of red lamp were also more popular in the North of the island. On the contrary, moxibustion and scalp acupuncture are more used in the south than in the centre of the country. A similar trend was also observed for the fumigations, which were more used in the south of the island, even there was . 26.
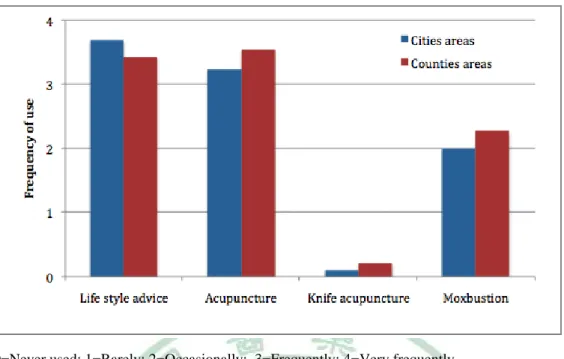
(36) . no statistical evidence. There were no differences of the frequency uses of powdered Chinese medicinal and raw Chinese medicinal between the different geographical locations.. 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.2 Frequency of the therapeutic methods used according the geographical situation. The division between cities areas and districts areas also showed some differences in the use of therapeutics method. Statistical evidence showed that acupuncture, moxibustion, scalp acupuncture and knife acupuncture were more used in districts areas than in cities areas. By contrast, life style advices were more important into cities areas. In general we found a larger use of therapeutics methods in districts areas than in cities areas.. . 27.
(37) . 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.3 Frequency of the therapeutic methods used regarding the cities and districts areas. Regarding the therapeutic methods there was only one statistical evidence related to the years of clinical practice. Statistics demonstrated that raw Chinese medicinal were more used by physicians with a longer clinical experience. We found the same tendencies for the bloodletting technique. In contrast, the use of powdered Chinese medicinal was more frequently use by the physician with 6 to 10 years of clinical experience. The use of raw Chinese medicinal and bloodletting technique was also correlated with age. Older physicians favoured more the use of these two therapeutic methods than younger physicians. That also was the case for the use of ear acupuncture, which was more popular for the group age between 40 to 49 years and 50 and more years. The use of powdered Chinese medicinal was predominant for the physicians between 30 to 49 years old. Statistical evidences also showed that the bloodletting technique was correlated to educational background. Special licence qualified physicians used considerably more this techniques than the two other groups. The. . 28.
(38) . special licence qualified physicians also stand out of the other groups by the fact they used more raw Chinese medicinal and didn’t used at all knife acupuncture nor Qigong techniques. We can note that if bloodletting technique and the use of raw Chinese medicinal were strongly correlated with special licence qualified physicians that could be due to the fact that in this group the physicians were older than the physicians from the school of Chinese medicine and the school of Post baccalaureate Chinese medicine (see profile of the respondent p. 20-1). There were no evidences for the correlation between the different hospitals and the therapeutics methods. However we can distinguish some tendencies especially concerning rural hospitals and Chinese medicine hospitals. In the rural hospitals we found a higher rate of moxibustion and fumigation use. On the contrary, we found less use of raw Chinese medicinal and knife acupuncture than in the other type of hospitals. We also found some similarity between rural hospitals and Chinese medicine hospitals were the use of manipulations and plasters were higher than in teaching and regional hospitals. Through the multiple linear regression analysis, we found that the group of factors that influenced strongly the use of the treatment methods was those correlated with the environment. There were four evidence of association related to geographical areas (moxibustion, knife acupuncture, manipulations and the use of red lamp). Two evidences were related to the cities/districts areas (manipulations and life style advice) and finally one was related to the type of hospitals (manipulations). The age was also influencing the choice of therapeutic methods (two evidences for the use of acupuncture and the use of red lamp). Finally, one evidence was related to the education background of the physicians and it concerned the use of the bloodletting technique. . 29.
(39) . Table 4.3.1 Factors associated with the treatment methods (1st Page) Acupuncture. Factors B. School of CM School of PB of CM Special licence Under 30 years old 30 to 39 years old 40 to 49 years old More than 50 years old 1 to 5 years of practice 6 to 10 years of practice 11 to 20 years of practice More than 20 years of practice Teaching hospital Regional hospital Rural hospital Chinese medicine hospital North of Taiwan Centre of Taiwan South of Taiwan Cities areas Districts areas. -.03 .32 0a -.59 -.55 -.76 0a .37 .61 .37 0a -.11 -.34 -.37 0a .12 -.37 0a -.30 0a. Sig.. .95 .45 . .28 .20 .05* . .49 .52 .42 . .71 .29 .46 .58 .12 . .11 .. 95% Confidence interval Lower Upper Bound Bound -.89 .84 -.52 1.16 . . -1.67 .49 -1.38 .29 -1.52 -.01 . . -.68 1.42 -.44 1.66 -.53 1.27 . . -.69 .47 -.97 .29 -1.33 .60 . . -.30 .54 -.83 .10 . . -.68 .07 . .. Moxibustion. B. Sig.. .51 .29 0a .01 .16 .06 0a -.31 .00 -.14 0a .18 -.11 .09 0a -.09 -.54 0a -.66 0a. .27 .53 . .99 .70 .87 . .57 .99 .77 . .55 .72 .86 . .67 .02* . .00** .. 95% Confidence interval Lower Upper Bound Bound -.40 1.42 -.61 1.19 . . -1.06 1.08 -.66 .97 -.68 .80 . . -1.38 .76 -1.06 1.06 -1.06 .78 . . -.40 .76 -.74 .51 -.88 1.06 . . -.50 .33 -.99 -.08 . . 1.03 -.29 .. Manipulation. B. -.18 -.16 0a -.09 -.32 -.42 0a .91 .90 .55 0a -1.03 -1.25 -1.29 0a .72 .53 0a -.47 0a. Sig.. .73 .76 .90 .54 .37 .17 .17 .33 .01* .00** .03* . .01* .07 . .04* .. 95% Confidence interval Lower Upper Bound Bound -1.22 .86 -1.18 .87 . . -1.41 1.24 -1.34 .71 -1.35 .51 . . -39 2.20 -39 2.20 -.56 1.67 . . -1.75 -.31 -2.03 -.47 -2.48 -.10 . . .21 1.23 -.03 1.10 . . -.92 -.03 . .. Bloodletting. B. -.98 -.98 0a -.31 -.08 .12 0a -.10 -.06 -.10 0a -.14 -.09 .17 0a -.03 -.29 0a -.08 0a. Sig.. .01* .01* . .46 .81 .69 .82 .89 .78 . .52 .70 .66 . .84 .11 . .59 .. 95% Confidence interval Lower Upper Bound Bound -1.68 -.29 -1.67 -.29 . . -1.13 .51 -.71 .56 -.45 .69 . . -.91 .72 -.87 .76 -.81 .60 . . -.59 .30 -.57 .39 -.57 .91 . . -.35 .29 -.64 .07 . . -.36 .21 . .. Data were analysed through Multiple Linear Model analysis and we chose to represent only the factors that attained statistical evidences. The factors didn't showed a difference with the following treatment methods: ear acupuncture, scalp acupuncture, raw Chinese medicinal, powdered Chinese medicinal, plaster, fumigations, cupping, guasha, qigong a . This parameter is set to zero because it is redundant * P<.05 **P<.001. 30 .
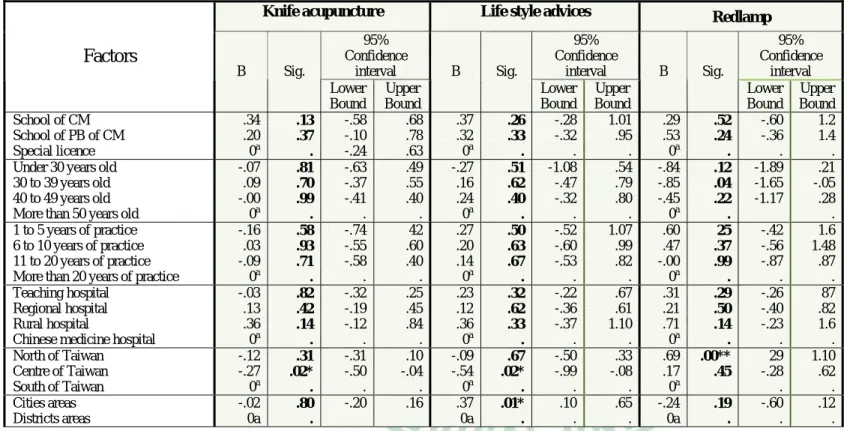
(40) . Table 4.3.1 Factors associated with the treatment methods (Page 2) Knife acupuncture. Factors B. School of CM School of PB of CM Special licence Under 30 years old 30 to 39 years old 40 to 49 years old More than 50 years old 1 to 5 years of practice 6 to 10 years of practice 11 to 20 years of practice More than 20 years of practice Teaching hospital Regional hospital Rural hospital Chinese medicine hospital North of Taiwan Centre of Taiwan South of Taiwan Cities areas Districts areas. .34 .20 0a -.07 .09 -.00 0a -.16 .03 -.09 0a -.03 .13 .36 0a -.12 -.27 0a -.02 0a. Sig.. .13 .37 . .81 .70 .99 . .58 .93 .71 . .82 .42 .14 . .31 .02* . .80 .. 95% Confidence interval Lower Upper Bound Bound -.58 .68 -.10 .78 -.24 .63 -.63 .49 -.37 .55 -.41 .40 . . -.74 42 -.55 .60 -.58 .40 . . -.32 .25 -.19 .45 -.12 .84 . . -.31 .10 -.50 -.04 . . -.20 .16. Life style advices. B. .37 .32 0a -.27 .16 .24 0a .27 .20 .14 0a .23 .12 .36 0a -.09 -.54 0a .37 0a. Sig.. .26 .33 . .51 .62 .40 . .50 .63 .67 . .32 .62 .33 . .67 .02* . .01* .. 95% Confidence interval Lower Upper Bound Bound -.28 1.01 -.32 .95 . . -1.08 .54 -.47 .79 -.32 .80 . . -.52 1.07 -.60 .99 -.53 .82 . . -.22 .67 -.36 .61 -.37 1.10 . . -.50 .33 -.99 -.08 . . .10 .65 . .. Redlamp. B. Sig.. .29 .53 0a -.84 -.85 -.45 0a .60 .47 -.00 0a .31 .21 .71 0a .69 .17 0a -.24 0a. .52 .24 . .12 .04 .22 . 25 .37 .99 . .29 .50 .14 . .00** .45 .19 .. 95% Confidence interval Lower Upper Bound Bound -.60 1.2 -.36 1.4 . . -1.89 .21 -1.65 -.05 -1.17 .28 . -.42 1.6 -.56 1.48 -.87 .87 . . -.26 87 -.40 .82 -.23 1.6 . . 29 1.10 -.28 .62 . . -.60 .12 . .. Data were analysed through Multiple Linear Model analysis and we chose to represent only the factors that attained statistical evidences. The factors didn't showed a difference with the following treatment methods: ear acupuncture, scalp acupuncture, raw Chinese medicinal, powdered Chinese medicinal, plaster, fumigations, cupping, guasha, qigong a . This parameter is set to zero because it is redundant * P<.05 **P<.001. . 31.
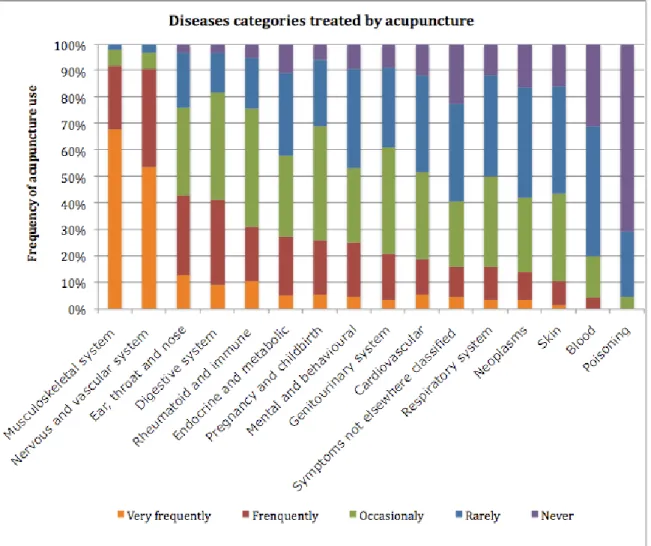
(41) . Diseases treated by acupuncture Acupuncture is used to improve the communication and circulation between the meridians and regulate the flow of the Qi and the blood in the meridians36. Therefore it can treat many diseases. Results issued from the questionnaire data showed that the most common kind of diseases treated by acupuncture were mainly diseases of the musculoskeletal system and nervous and vascular system37. Then came the ear, throat and nose diseases, digestive system disease and rheumatoid and immune diseases.. Figure 4.3.4 Diseases categories treated by acupuncture. 32 .
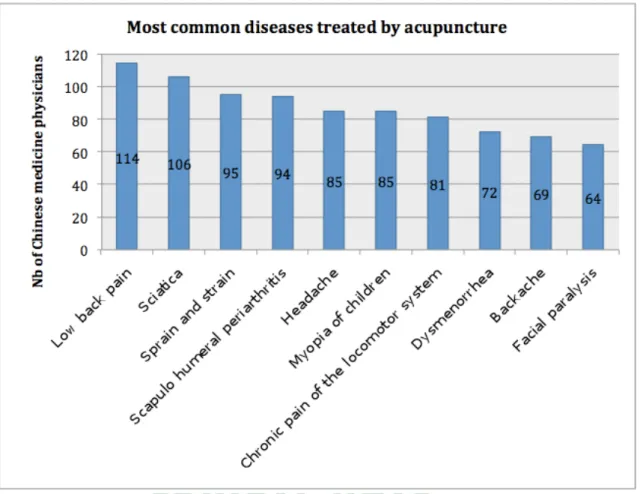
(42) . Besides the ten major diseases picked up among the list of 64 diseases recommended by the WHO for acupuncture treatment were: low back pain, sciatica, sprain and strain, scapulo humeral periarthritis, headache, myopia of children, chronic pain of the locomotor system, dysmenorrhea, backache and facial paralysis38.. Figure 4.3.5 Most common diseases treated by acupuncture. Apart these ten first common diseases commonly treat with acupuncture, Chinese medicine physicians are also used to treat cervical spondylopathy (60 physicians), hemiplegia (58 physicians), tennis elbow (55 physicians), insomnia (55 physicians), rhinallergosis (53 physicians), migraine (36 physicians), tonic headache (32 physicians), nausea and vomiting (32 physicians), oppilation (27 physicians), prosopalgia (25 physicians)and simple obesity (20 physicians).. . 33.
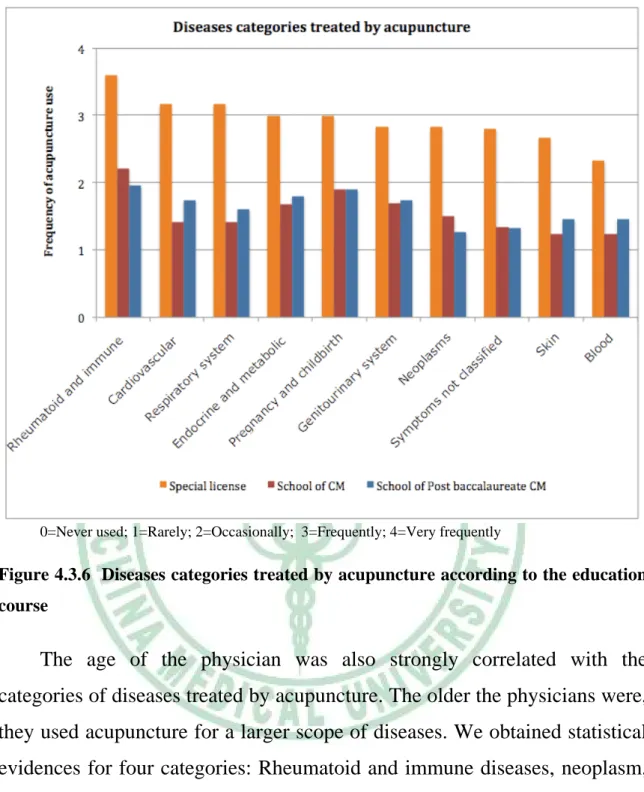
(43) . Comparative statistics showed some interesting features on how diseases categories treated by acupuncture were related to the physicians educational background, age and years of clinical practice as well as to the geographical environment. Furthermore some evidences also showed some links between the different kind of hospitals and the diseases treated. The most striking statistical evidences were linked to the educational background. The special licence qualified physicians used acupuncture for a lager scope of diseases than physician graduated from the school of Chinese medicine and the school of Post baccalaureate Chinese medicine. For the 16 different diseases categories mentionned in the questionnaire, 10 showed evidences of the differences between the special licence qualified physicians with the two other groups (table 4.3) and 3 showed evidences of the differences between the special licence qualified physicians and one of the other groups. Special licence qualified physicians displayed always a higher rate of acupuncture use except for musculoskeletal, neurological diseases and poisoning where there were no differences between the three groups.. . 34.
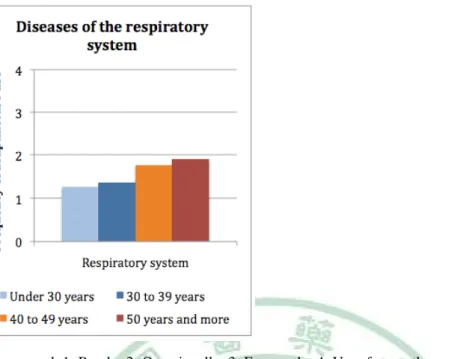
(44) . 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.6 Diseases categories treated by acupuncture according to the education course. The age of the physician was also strongly correlated with the categories of diseases treated by acupuncture. The older the physicians were, they used acupuncture for a larger scope of diseases. We obtained statistical evidences for four categories: Rheumatoid and immune diseases, neoplasm, diseases of the respiratory system and diseases of the blood. We observed two kinds of tendencies. The first one was a progressive increase of the frequency use proportional to the group age. This tendency is represented by the use of acupuncture for rheumatoid and immune diseases. We found the same tendencies for musculoskeletal diseases, endocrine and metabolic diseases and diseases of the respiratory system.. . 35.
(45) . 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.7 Treatment of the diseases of the respiratory system in relation to the age of the physicians. The second tendencies found was an augmentation of acupuncture use proportional to the age if we merged the age of the physician into two groups: “Under 30 to 39 years” and “40 and more years” (sometimes the differences between the group of physicians “Under 30 years” and “30 to 39 years” wasn’t very clear). This allowed us to see the same tendency, that is to say, the older physicians used acupuncture for a larger scope of diseases. This tendency was found for neoplasm, rheumatoid and immune diseases and diseases of the blood with statistical evidence. The same trend was also found for mental and behavioural disorders, diseases of the digestive system, diseases of the ear, throat and nose, diseases of the genitourinary system and symptoms and signs not elsewhere classified.. . 36.
(46) . 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.8 Treatment of rheumatoid and immune diseases, neoplasm and diseases of the blood in relation to the age of the physicians. Regarding the years of clinical practice and the scope of acupuncture use the tendencies were less apparent. We found one statistical evidence for the rheumatoid and immune diseases that was proportionally related to the years of practice.. 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.9 Treatment of rheumatoid and immune diseases in relation to the years of practice. . 37.
(47) . This tendency was unique. The other trend we found was a higher rate of acupuncture use for the musculoskeletal diseases, mental and behavioural disorders, endocrine and metabolic diseases and diseases of the skin by the group of physicians with “more than 20 years” of practice. For the other categories, there were no clear differences between the different groups. The general trend we found relating geographical situation and the kind of disease treated was that in the north of the island, the physicians used acupuncture for a larger scope of diseases than in the centre of the island. In the centre, acupuncture use was limited to certain categories of diseases (diseases of the musculoskeletal system and diseases of the nervous and vascular system). The south of the island was in between the results found for the north and the centre of the country. However we only found one statistical evidence for the category of “symptoms and signs not elsewhere classified”, the physicians practicing in the north of the country showed an evident prevalence of acupuncture use under both the centre and the South. The same trend was found for neoplasm, cardiovascular diseases and diseases of the respiratory system. The other tendency concerned mainly differences between the north and the centre of the island in the treatment of the diseases with acupuncture. This was the case for mental and behavioural disorders, pregnancy and childbirth, diseases of the skin and diseases of the blood, endocrine and metabolic diseases, diseases of the digestive system, diseases of the ear, throat and nose and diseases of the genitourinary system that displayed a higher use rate in the North. For the other categories of disease there were no specific differences according to the geographical situation. Regarding the division of the physician between cities and district areas, one evidence of difference was found between the two groups for the endocrine and metabolic diseases. This category of disease was more likely . 38.
(48) . to be treated by acupuncture in cities areas. Though the tendencies between cities and district areas were not clearly distinct therefore it is difficult to draw conclusion. Comparing the different hospitals and the categories of disease treated by acupuncture we found a general trend, that was that the rural hospitals tend to have a limited scope of disease treated by acupuncture. In contrast physicians working in Chinese medicine hospital used to treat a larger scope of disease with acupuncture. Chinese medicine hospital showed a higher rate of acupuncture use for rheumatoid and immune diseases, diseases of the digestive system as well as endocrine and metabolic diseases. Regional hospital more frequently used acupuncture for treating questions regarding pregnancy, childbirth and diseases of the nervous and vascular system than the other hospitals. Finally the teaching hospital displayed a more homogeneous use of acupuncture for all the categories of diseases. Now if we separated the hospitals into two groups (Chinese medicine hospitals and Western medicine hospitals), we find an interesting tendency event there are no statistical evidences. Physicians working in Chinese medicine hospitals used acupuncture to treat a larger scope of diseases than those practicing in Western medicine hospitals. This was specially marked for endocrine and metabolic diseases, diseases of the respiratory system as well as for rheumatoid and immune diseases and diseases of the digestive system.. . 39.
(49) . 0=Never used; 1=Rarely; 2=Occasionally; 3=Frequently; 4=Very frequently. Figure 4.3.10 Treatment of diseases in relation to the type of hospitals. The multiple linear regression analysis showed that the strongest association of the categories of diseases treated by acupuncture was related to the educational background. Nine items showed an evidence of association with the educational background (rheumatoid and immune diseases, neoplasms, endocrine and metabolic diseases, cardiovascular diseases, diseases of the respiratory system, pregnancy and childbirth, diseases of the skin, diseases of the blood and symptoms, signs not elsewhere classified). Three items showed a correlation with the age (rheumatoid and immune diseases, diseases of the ear, nose and throat and injury and poisoning). Three items showed an evidence of association with the geographical area (neoplasms, mental and behavioural diseases and symptoms, signs not elsewhere classified). Finally the type of hospitals was associated with two items (endocrine and metabolic diseases and diseases of the respiratory system), and the cities/districts areas were associated with one item (neoplasm). . 40.
(50) . Table 4.3.2 Factors associated with the categories of diseases treated by acupuncture (1st Page). Poisoning. Factors B. School of CM School of PB of CM Special licence Under 30 years old 30 to 39 years old 40 to 49 years old More than 50 years old 1 to 5 years of practice 6 to 10 years of practice 11 to 20 years of practice More than 20 years of practice Teaching hospital Regional hospital Rural hospital Chinese medicine hospital North of Taiwan Centre of Taiwan South of Taiwan Cities areas Districts areas. -.27 -.08 0a -.84 -.71 -.50 0a .66 .70 .44 0a .05 -.09 -.15 0a -.03 -.06 0a -.08 0a. Sig.. .34 .79 . .01* .01* .03* . .04* .03* .11 . .79 .64 .63 . .82 .70 . .51 .. 95% Confidence interval Lower Upper Bound Bound -.83 .29 -.63 .48 . . -1.49 -.18 -1.22 -.21 -.95 -.05 . . .02 1.30 .06 1.33 -.10 .99 . . -.31 .40 -.47 .29 -.74 .45 . . -.28 .23 -.34 .23 . . -.30 .15 . .. Neoplasm. B. -1.06 -1.16 0a -.74 -.75 .01 0a -.15 -.16 -.57 0a .17 -.11 -.33 0a .46 .19 0a -.40 0a. Sig.. .02* .01* . .16 .07 .99 . .77 .76 .20 . .54 .71 .48 . .03* .41 . .03* .. 95% Confidence interval Lower Upper Bound Bound -1.93 -.20 -2.02 -.31 . . -1.77 .30 -1.56 .05 -.72 .73 . . -1.16 .86 -1.17 .85 -1.44 .30 . . -.38 .72 -.71 .48 -1.25 .60 . . .06 .86 -.26 .63 . . -.76 -.05 . .. Endocrine and metabolic diseases B. -1.23 -1.05 0a .02 -.36 .05 0a -.12 -.07 -.46 0a -.71 -.72 -.83 0a -.07 -.25 0a -.03 0a. Sig.. .01* .03* . .97 .42 .91 . .83 .91 .34 . .03* .03* .11 . .77 .32 . .90 .. 95% Confidence interval Lower Upper Bound Bound -2.23 -.30 -2.00 -.09 . . -1.12 1.15 -1.24 .52 -.74 .83 . . -1.23 .99 -1.17 1.04 -1.41 .49 . . -1.32 -.09 -1.38 -.06 -1.86 .20 . . -.51 .38 -.75 .25 . . -.42 .37 . .. Diseases of the respiratory system B. Sig.. -1.45 -1.26 0a -.55 -.70 -.25 0a .17 .16 -.15 0a -.56 -.43 -.63 0a .13 -.14 0a -.18 0a. .00** .00** . .27 .07 .48 . .72 .75 .71 . .04* .14 .17 . .49 .53 . .31 .. 95% Confidence interval Lower Upper Bound Bound -2.29 -.60 -2.10 -.43 . . -1.54 .44 -1.46 .07 -.93 .44 . . -.79 1.14 -.81 1.12 -.98 .67 . . -1.10 -.02 -1.01 .15 -1.52 .27 . . -.25 .52 -.56 .29 . . -.52 17 . .. Data were analysed through Multiple Linear Model analysis and we chose to represent only the factors that attained statistical evidences. The factors didn't showed a difference with the following categories of diseases: musculoskeletal diseases, diseases of the nervous and vascular system, diseases of the digestive system and diseases of the genitourinary system. a . This parameter is set to zero because it is redundant * P<.05 **P<.001. 41 .
(51) . Table 4.3.2 Factors associated with the categories of diseases treated by acupuncture (Page 2). Factors Factors. School of CM School of PB of CM Special licence Under 30 years old 30 to 39 years old 40 to 49 years old More than 50 years old 1 to 5 years of practice 6 to 10 years of practice 11 to 20 years of practice More than 20 years of practice Teaching hospital Regional hospital Rural hospital Chinese medicine hospital North of Taiwan Centre of Taiwan South of Taiwan Cities areas Districts areas. Rheumatoid and immune diseases B B. -.79 -1.00 0a -1.08 -.99 -.45 0a -.44 -.42 -.57 0a -.37 -.12 -.24 0a .27 .10 0a -.27 0a. Sig. Sig.. .09 .03* . .04* .02* .22 . .39 .41 .19 . .18 .69 .60 . .19 .64 . .13 .. 95% Confidence interval Lower Upper Bound Bound -1.72 .14 -1.91 -.09 . . -2.10 -.06 -1.78 -.20 -1.16 .26 . . -1.44 .57 -1.41 .58 -1.43 .29 . . -.92 .18 -.71 .47 -1.16 .67 . . -.13 .66 -.33 .54 . . -.62 .08 . .. Symptoms and signs not elsewhere classified B B. Sig. Sig.. -1.14 -1.16 0a -.22 -.71 -.26 0a .77 .69 .54 0a .09 -.23 .14 0a .78 .13 0a -.21 0a. .04* .03* . .72 .15 .57 . .22 .27 .34 . .80 .54 .79 . .00** .62 . .34 .. 95% Confidence interval Lower Upper Bound Bound -2.23 -.04 -2.21 -.10 . . -1.47 1.02 -1.68 .26 -1.16 .64 . . -.47 2.01 -.54 1.92 -.57 1.64 . . -.59 .77 -.96 .51 -.94 1.23 . . .29 1.27 -.40 .66 . . -.64 .22 . .. Diseases of the skin B. Sig.. 1.20 -.96 0a .01 .07 .14 0a -.86 -.75 -.68 0a -.26 -.05 -.29 0a -.03 -.22 0a. . .05 0a. .01* .02* . .99 .85 .69 . .08 .12 .10 . .32 .86 .52 . .88 .31 . .79 .. 95% Confidence interval Lower Upper Bound Bound -2.02 -.38 -1.78 -.15 . . -.96 .97 -.68 .81 -.53 .80 . . -1.80 .09 -1.69 .19 -1.48 .13 . . -.79 .26 -.61 .51 -1.16 .59 . . -.40 .35 -.63 .20 . . -.29 .38 . .. Cardiovascular diseases B. Sig.. -1.42 -1.19 0a -.33 -.52 -.07 0a .25 .07 -.18 0a -.49 -.09 -.84 0a .28 .17 0a -.24 0a. .00** .01* . 54 .21 .84 . .64 .89 .69 . .09 .78 .08 . .18 .46 . .19 .. 95% Confidence interval Lower Upper Bound Bound -2.32 -.52 -2.08 -.30 . . -1.38 .73 -1.33 .30 -.80 .66 . . -.79 1.28 -.96 1.10 -1.06 .70 . . -1.06 .08 -.70 .53 -1.80 .12 . . -.13 .69 -.29 .63 . . -.61 .13 . .. Data were analysed through Multiple Linear Model analysis and we chose to represent only the factors that attained statistical evidences. The factors didn't showed a difference with the following categories of diseases: musculoskeletal diseases, diseases of the nervous and vascular system, diseases of the digestive system and diseases of the genitourinary system. a . This parameter is set to zero because it is redundant * P<.05 **P<.001. . 42.
數據
+7
相關文件
On another level, though, the similarities to the research world are strong: you succeed by building networks, the glue that holds relationships together is the values that you
臺大機構典藏NTUR (National Taiwan University 二 Repository, http://ntur.lib.ntu.edu.tw) 經驗與協助推 動臺灣學術機構典藏TAIR (Taiwan Academic Institutional Repository,
了⼀一個方案,用以尋找滿足 Calabi 方程的空 間,這些空間現在通稱為 Calabi-Yau 空間。.
• ‘ content teachers need to support support the learning of those parts of language knowledge that students are missing and that may be preventing them mastering the
volume suppressed mass: (TeV) 2 /M P ∼ 10 −4 eV → mm range can be experimentally tested for any number of extra dimensions - Light U(1) gauge bosons: no derivative couplings. =>
• Formation of massive primordial stars as origin of objects in the early universe. • Supernova explosions might be visible to the most
Monopolies in synchronous distributed systems (Peleg 1998; Peleg
Salas, Hille, Etgen Calculus: One and Several Variables Copyright 2007 © John Wiley & Sons, Inc.. All
