CASE REPORT
Monozygotic twins with trisomy 18 of paternal origin: prenatal diagnosis and
molecular cytogenetic characterization in a pregnancy with one structurally
abnormal living fetus and one intrauterine fetal demise
Chih-Ping Chen a,b,c,d,e,f,g*, Schu-Rern Chern c, Yi-Yung Chen b, Pei-Chen Wu b, Dai-Dyi Town b, Wen-Lin Chen b and Wayseen Wang c,h
a Department of Medicine, Mackay Medical College, New Taipei City, Taiwan
b Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan c Department of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan
d Department of Biotechnology, Asia University, Taichung, Taiwan
e School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan f Institute of Clinical and Community Health Nursing, National Yang-Ming University, Taipei, Taiwan g Department of Obstetrics and Gynecology, School of Medicine, National Yang-Ming University, Taipei,
Taiwan
h Department of Bioengineering, Tatung University, Taipei, Taiwan
* Correspondence to: Chih-Ping Chen, MD
Department of Obstetrics and Gynecology, Mackay Memorial Hospital 92, Section 2, Chung-Shan North Road, Taipei, Taiwan
Tel: +886-2-25433535
Fax: +886-2-25433642, +886-2-25232448 E-mail: [email protected]
Abstract
Objective: To present prenatal diagnosis and molecular cytogenetic characterization of trisomy 18 in a monozygotic twin pregnancy with one structurally abnormal living fetus and one intrauterine fetal demise.
Case Report: A 38-year-old woman was referred for amniocentesis at 16 weeks of gestation because of advanced maternal age. Prenatal ultrasound revealed a monozygotic twin pregnancy with one structurally abnormal living fetus and one fetal demise. The body structure details of the dead fetus could not be identified, whereas holoprosencephaly and omphalocele were identified in the living fetus on prenatal ultrasound. Quantitative fluorescent polymerase chain reaction assays using polymorphic DNA markers specific for chromosome 21 and chromosome 18 were applied to the uncultured amniocytes in the amniotic cavity of the living fetus and the cultured amniocytes in the amniotic cavity of the fetus with intrauterine fetal demise. The specimen showed a dosage ratio of 2:1 (paternal: maternal) for chromosome 18-specific markers in both twins. The result was consistent with monozygosity and trisomy 18, and the trisomy 18 was possibly caused by a paternal second meiotic division non-disjunction error or a postzygotic mitotic error. Conventional cytogenetic analysis revealed a karyotype of 47,XY,+18 in both twins. The pregnancy was terminated at 19 weeks of gestation, and a 2-g small-for-date macerated twin A and a 166-g malformed asphyxiated twin B were delivered. Twin A manifested cebocephaly and omphalocele, and twin B manifested premaxillary agenesis and omphalocele.
Conclusion: The present case provides evidence that fetal wastage may occur in one of the co-twins in monozygotic co-twins associated with trisomy 18, and this may in part explain the very rare occurrence of living monozygotic twins with trisomy 18.
Key words: intrauterine fetal death, monozygotic twins, prenatal diagnosis, rapid aneuploidy diagnosis, trisomy 18
Introduction
Trisomy 18 in monozygotic twins is very rare with a predicted incidence of 1 in one million births based on the calculation of 0.3 per 1,000 newborn babies in trisomy 18 and 3.5-4 per 1,000 births in monozygotic twins [1]. To date, only 6 cases of trisomy 18 in monozygotic twins have been reported [1-6]. Here, we present our experience of prenatal diagnosis and molecular cytogenetic characterization of trisomy 18 in a monozygotic twin pregnancy with one structurally abnormal living fetus and one intrauterine fetal demise. To our knowledge, such a case has not been previously described.
Case Report
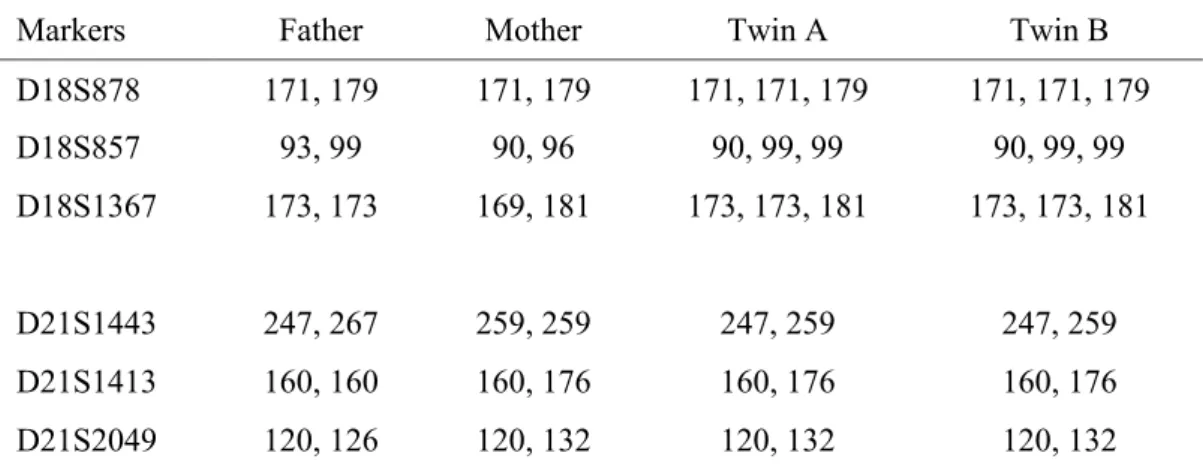
A 38-year-old, gravida 5 para 2, woman was referred for amniocentesis at 16 weeks of gestation because of advanced maternal age. The woman had not undergone any assisted reproductive technology and did not have diabetes mellitus. Her husband was 40 years old. She and her husband were healthy and non-consanguineous. There was no family history of congenital malformation. Prenatal ultrasound revealed a monozygotic twin pregnancy with one structurally abnormal living fetus and one fetal demise. The dead co-twin had a crown-rump length (CRL) of 3.4 cm equivalent to 10.1 weeks, and the living co-twin had a CRL of 7.5 cm and a biparietal diameter of 2.6 cm equivalent to 13.2 weeks. The amniotic sac was monochorionic and diamniotic. The amniotic fluid amounts in both amniotic cavities were normal. The body structure details of the dead fetus could not be identified, whereas holoprosencephaly (HPE) and omphalocele were identified in the living fetus on prenatal ultrasound (Figure 1). The woman underwent amniocentesis at 16 weeks of gestation. Quantitative fluorescent polymerase chain reaction (QF-PCR) assays using polymorphic DNA markers specific for chromosome 21 and chromosome 18 were applied to the uncultured amniocytes in the amniotic cavity of the living fetus and the cultured amniocytes in the amniotic cavity of the fetus with intrauterine fetal demise. The specimen showed a diallelic pattern with a dosage ratio of 1:1 (paternal: maternal) for chromosome 21-specific markers but a diallelic pattern with a dosage ratio of 2:1 (paternal: maternal) for chromosome 18-specific markers in both twins (Table 1, Figure 2). The twin fetuses inherited two copies of a single paternal allele in chromosome 18. The result was consistent with monozygosity and trisomy 18, and the trisomy 18 was possibly caused by a
error. Conventional cytogenetic analysis revealed a karyotype of 47,XY,+18 in both twins. The pregnancy was terminated at 19 weeks of gestation, and a 2-g small-for-date macerated twin A and a 166-g malformed asphyxiated twin B were delivered. The twins manifested concordant phenotype of HPE and omphalocele. Twin A manifested cebocephaly and omphalocele, and twin B manifested premaxillary agenesis (PMA) and omphalocele (Figures 3 and 4). Postnatal QF-PCR analysis using the umbilical cord tissues from the twins confirmed the prenatal diagnosis. Discussion
Rapid aneuploidy diagnosis (RAD) by array comparative genomic hybridization (aCGH) using uncultured amniocytes in pregnancy with fetal structural abnormalities has been well described [7]. In this report, we demonstrate the application of QF-PCR in RAD of trisomy 18 using uncultured and cultured amniocytes in a monozygotic twin pregnancy with one structurally abnormal living fetus and one fetal demise. RAD refers to the applications of aCGH, multiplex ligation-dependent probe amplification (MLPA), interphase fluorescence in situ hybridization (FISH) and QF-PCR without the need of cell culture [8]. The aCGH has the advantage of rapid genome-wide analysis but the disadvantages of difficulty in detecting low-level mosaicism, balanced translocation, inversion and polyploidy. MLPA, FISH and QF-PCR have the advantage of being less expensive than aCGH but the disadvantages of limitation to the detection of numerical aneuploidies of chromosomes 13, 18, 21, X and Y. Whenever prenatally detected ultrasound abnormalities raise suspicions of common aneuploidies such as trisomies 13, 18 and 21, and Turner syndrome, the application of MLPA, FISH or QF-PCR may be considered as a choice of RAD with less expensive cost than aCGH. In addition to RAD, QF-PCR is able to determine zygosity, parental origin of the aneuploidy as well as meiotic or mitotic non-disjunction. The information acquired by QF-PCR is very useful in genetic counseling of prenatally detected chromosome abnormalities in twins.
The present case was associated with structural abnormalities of omphalocele and HPE which are not uncommon in fetuses with trisomy 18 or trisomy 13. Therefore, we first selected trisomy 18-specific markers for RAD in addition to the trisomy 21-specific markers. Both omphalocele and HPE can be associated with trisomies 18 and 13 [9-10]. Omphalocele is more frequently observed in fetuses with trisomy 18, but HPE is more frequently observed in fetuses with trisomy 13. Snijders et al. [11] found that omphalocele was diagnosed in 31% of fetuses with trisomy 18
(n = 137) and in 17% of the fetuses with trisomy 13 (n = 54). Chen [12] found that among 1,148 fetuses with prenatally detected omphalocele, 415 cases (36.1%) had chromosome abnormalities including trisomy 18 (n = 277) in 66.7% (277/415) of the cases and trisomy 13 (n = 72) in 17.3% (72/415) of the cases. Snijders et al. [11] found that HPE occurred in 39% of fetuses with trisomy 13 (n = 54) and 3% of the fetuses with trisomy 18 (n = 137). They also reported that among 132 fetuses with prenatally detected HPE, 33% of the cases had chromosome abnormalities including trisomy 13 (n = 30) and trisomy 18 (n = 7). In a study of 59 fetuses with HPE, Chen et al. [13] found 34 cases (57.6%) had chromosome abnormalities including trisomy 13 (n = 19) and trisomy 18 (n = 4).
The present case was associated with a paternal origin of the extra chromosome 18. Studies on the extra chromosome in trisomy 18 have shown that 91% are of maternal origin with 60% due to a meiosis II error, 30% due to a meiosis I error and about 8% due to a mitotic error [14-16]. Trisomy 18 has a low paternal error rate. In a study of 31 cases of fetal trisomy 18, Chen et al. [17] found a result of maternal disjunction in 90.3% of the cases and of paternal non-disjunction in only 9.7%. Clinical reports of trisomy 18 in monozygotic twins are uncommon. Lapi et al. [2] first reported a case of presumptive monozygotic trisomy 18 twins with only one liveborn twin who died at 15 minutes of age. Bhatnagar et al. [3] reported trisomy 18 in monozygotic twins associated with a viable co-twin and a holoacardius. Mulder et al. [4] reported a case of a pair of monozygotic twins with trisomy 18 discordant for major anomalies, with left diaphragmatic hernia and a small ventricular septal defect in one twin, and bilateral diaphragmatic hernias, hydrocephalus, radial aplasia and complex congenital heart defects in the other twin. Shah et al. [5] reported prenatal diagnosis of trisomy 18 in monozygotic twins by cordocentesis in a twin pregnancy with fetal growth lag and structural abnormalities detected by ultrasound. The liveborn monozygotic twins differed in phenotype, with omphalocele in one twin and clitoromegaly in the other twin. Schlessel et al. [1] reported a case of trisomy 18 in liveborn monozygotic twins with prenatal ultrasound findings of intrauterine growth restriction and structural malformations in one of the twins. Phenotypic discordance in the trisomic twins included complex congenital heart defects in one twin and myelomeningocele, hydrocephalus and omphalocele in the other twin. Lee et al. [6] reported trisomy 18 in a pair of liveborn
esophageal fistula but were discordant for types of congenital heart defects, cleft lip and choanal atresia.
In conclusion, we have presented prenatal diagnosis and molecular cytogenetic characterization of trisomy 18 in monozygotic twins in a pregnancy with one structural abnormal living fetus and one intrauterine fetal demise. Our presentation provides evidence that fetal wastage may occur in one of the co-twins in monozygotic twins associated with trisomy 18, and this may in part explain the very rare occurrence of living monozygotic twins with trisomy 18.
Acknowledgements
This work was supported by research grants NSC-97-2314-B-195-006-MY3 and NSC-99-2628-B-195-001-MY3 from the National Science Council, and MMH-E-100-04 from Mackay Memorial Hospital, Taipei, Taiwan.
References
1. Schlessel JS, Brown WT, Lysikiewicz A, Schiff R, Zaslav AL. Monozygotic twins with trisomy 18: a report of discordant phenotype. J Med Genet 1990; 27: 640-2.
2. Lapi E, Benedetti A, Biondi A. Sindrome di Edwards in una coppia gemellare. Minerva Ginecol 1981; 33: 1151-4.
3. Bhatnagar KP, Sharma SC, Bisker J. The holoacardius: a correlative computerized tomographic, radiologic, and ultrasonographic investigation of a new case with review of literature. Acta Genet Med
Gemellol (Roma) 1986; 35: 77-89.
4. Mulder AFP, van Eyck J, Groenendaal F, Wladimiroff JW. Trisomy 18 in monozygotic twins. Hum
Genet 1989; 83: 300-1.
5. Shah DM, Jeanty P, Dev VG, Ulm JE, Phillips J. Diagnosis of trisomy 18 in monozygotic twins by cordocentesis. Am J Obstet Gynecol 1989; 160: 214-5.
6. Lee J-T, Chou H-C, Tsao P-N, Hsieh W-S, Hwu W-L. Trisomy 18 in monozygotic twins with discordant phenotypes. J Formos Med Assoc 2004; 103: 314-6.
7. Chen C-P, Su Y-N, Wu P-C, Lee C-C, Pan C-W, Wang W. Rapid aneuploidy diagnosis by array comparative genomic hybridization using uncultured amniocytes in a pregnancy with fetal nuchal edema and mild ascites. J Med Ultrasound 2011: 19; in press
8. Bui TH. Prenatal cytogenetic diagnosis: gone FISHing, BAC soon! Ultrasound Obstet Gynecol 2007; 30: 247-51.
9. Chen C-P. Prenatal sonographic features of fetuses in trisomy 13 pregnancies (II). Taiwan J Obstet
Gynecol 2009; 48: 218-24.
10.Chen C-P. Prenatal sonographic features of fetuses in trisomy 13 pregnancies (III). Taiwan J Obstet
Gynecol 2009; 48: 342-9.
11.Snijders RJM, Farrias M, von Kaisenberg C, Nicolaides KH. Fetal abnormalities. In: Snijders RJM, Nicolaides KH, eds. Ultrasound Markers for Fetal Chromosomal Defects. New York: Parthenon Publishing Group, 1996; 1-62.
12.Chen C-P. Chromosomal abnormalities associated with omphalocele. Taiwan J Obstet Gynecol 2007; 46: 1-8.
13.Chen C-P, Chern S-R, Tsai F-J, Lin C-Y, Lin Y-H, Wang W. A comparison of maternal age, sex ratio and associated major anomalies among fetal trisomy 18 cases with different cell division of error .
Genet Couns 2005; 16: 49-57
14.Fisher JM, Harvey JF, Morton NE, Jacobs PA. Trisomy 18: studies of the parent and cell division of origin and the effect of aberrant recombination of nondisjunction. Am J Hum Genet 1995; 56: 669-75. 15.Eggermann T, Nöthen MM, Eiben B, Hofmann D, Hinkel K, Fimmers R, et al. Trisomy of human
chromosome 18: molecular studies on parental origin and cell stage of nondisjunction. Hum Genet 1996; 97: 218-23.
16.Nicolaidis P, Petersen MB. Origin and mechanisms of non-disjunction in human autosomal trisomies.
Hum Reprod 1998; 13: 313-9.
17.Chen C-P, Chern S-R, Lin C-J, Lee C-C, Wang W, Tzen C-Y. A comparison of maternal age, sex ratio and associated anomalies among numerically aneuploid, structurally aneuploid and euploid holoprosencephaly. Prenat Diagn 2005; 25: 327-30.
Figure Legends
Figure 1. Prenatal ultrasound at 16 weeks of gestation shows (A) twin A with intrauterine fetal death, (B) twin B with omphalocele (O) and holoprosencephaly, and (C) holoprosencephaly in twin B. Figure 2. Representative electrophoretograms of quantitative fluorescent polymerase chain reaction assays
show monozygotic twinning and trisomy 18. The marker D21S1443 shows two peaks (247bp: 259bp; paternal and maternal, respectively) of equal fluorescent activity from two different parental alleles indicating disomy 21 in the amniocytes of monozygotic twins. The marker D18S1367 shows two peaks (173bp: 181bp; paternal and maternal, respectively) of unequal fluorescent activity from two different parental alleles in the amniocytes of monozygotic twins with a ratio of 2:1 (paternal: maternal) indicating a paternal origin of trisomy 18.
Figure 3. (A) Amplified image of twin A with intrauterine fetal demise. (B) Twin A and twin B at birth. Figure 4. The phenotypes of twin B: (A) holoprosencephaly and premaxillary agenesis, (B) omphalocele,
(C) clenched hand and (D) rocker-bottom foot.
Table 1. Molecular results using polymorphic markers specific for chromosomes 18 and 21*
Markers Father Mother Twin A Twin B
D18S878 171, 179 171, 179 171, 171, 179 171, 171, 179 D18S857 93, 99 90, 96 90, 99, 99 90, 99, 99 D18S1367 173, 173 169, 181 173, 173, 181 173, 173, 181 D21S1443 247, 267 259, 259 247, 259 247, 259 D21S1413 160, 160 160, 176 160, 176 160, 176 D21S2049 120, 126 120, 132 120, 132 120, 132
* Alleles (basepair sizes) are listed below each individual. Twin A: the twin with intrauterine fetal death.