Introduction
In 1998, we reported on the use of the T2sympathetic block (ESB2) by the clipping method for 326 cases of hyperhidrosis palmaris (HP) [1].
Recently, indications of sympathetic surgery ex-panded to include hyperhidrosis craniofacialis (HCF) and facial blushing (FB) [2–4]. In 2001, we set up the Lin–Telaranta classification (Table1) for sympathetic surgery [3] in order to reduce the rate of reflex sweating, which is the most troublesome side effect of this procedure [1,5, 6].
In this series, we report the best level of blockade for HP, the advantages of the clipping method, and the possibility of unilaterally clipping the wrong ganglion. We also explain why we believe ‘‘reflex sweating’’ rather than ‘‘compensatory hyperhidrosis’’ is a more appropriate term.
Materials and methods
Between June 2001 and June 2003 data from 114 patients who underwent surgery for various sympathetic disorders were col-lected. In total, 73 patients had a history of HP, 27 HCF, and 14
FB. They all underwent sympathetic block by the clipping method using the principles of the Lin–Telaranta classification (Table1).
The surgical procedures used were the endoscopic sympathetic block (ESB) and the reverse procedure (removal of clips). These two procedures have been previously described [1].
Results
ESB4gave the best results (i.e., normal facial and hand sweating without reflex sweating) in patients with HP. After ESB4, normal physiological sweating, during hot environment exposure, occurred in the popliteal area and lower back. All FB subsided after ESB2. One pa-tient experiencing intolerable reflex sweating, and clipping was reversed. ESB3 produced satisfactory results in all patients with HCF, none reported intol-erable side effects.
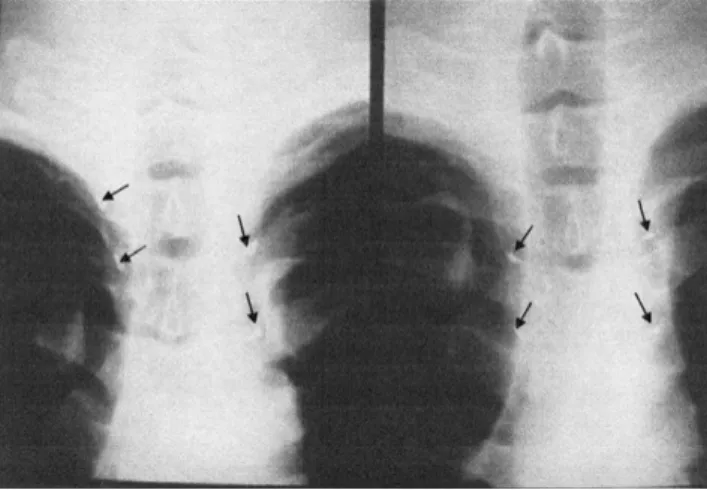
During the follow-up period, we surprisingly dis-covered that five patients (4.4%) were unilaterally clipped at the wrong level (Fig. 1). Three patients underwent ESB3 for HCF. Post-operatively, they experienced hemi-facial anhydrosis. By reviewing the chest roentgenograph, one side was ESB2 while the Shah-Hwa Chou
Eing-Long Kao Chien-Chih Lin Meei-Feng Huang
The outcome of ganglion clipping
in hyperhidrosis and blushing
Received: 25 January 2005 Accepted: 23 March 2006 Published online: 12 May 2006
j Abstract A total of 114 patients with various sympathetic disor-ders underwent endoscopic sym-pathetic block over different thoracic ganglions by the clipping method. The advantages of this method include the recognition of the clipped level, changeability, and reversibility. However, 4.4% of patients were unilaterally clipped at the wrong level.
j Key words sympathetic block Æ ganglion clipping Æ
hyperhidrosis Æ sweating Æ autonomic nervous system
RESEARCH LETTER
Clin Auton Res (2006) 16:240–242 DOI 10.1007/s10286-006-0347-2
CAR
347
S.-H. Chou Æ E.-L. Kao Æ C.-C. Lin (&) M.-F. Huang
Dept. of Surgery
Kaohsiung Medical University 100 Shih Chuan 1st Road Kaohsiung 80708, Taiwan Tel.: +886-7/3121101 ext. 6305 Fax: +886-7/3127056
other side was ESB3. Another two patients underwent ESB4 for HP. Post-operatively, one side had normal hand sweating while the other side was ‘‘too dry’’. Again, on chest X-ray, one side was EB4and the other side was ESB3. They received a second operation in which the clip was re-applied to the appropriate ganglion, and achieved satisfactory results. All of the patients had no recurrence after an average follow-up period of 28 ± 10.5 months.
Discussion
We use the term ‘‘reflex sweating’’ instead of ‘‘com-pensatory hyperhidrosis’’ because the latter has been misused as a medical term and several observations have been noted in actual practice. First, there is no increased sweating over the face and upper body after lumbar sympathectomy for plantar sweating. Second, different degrees of post-operative sweating were found after different levels of sympathetic block. Lastly, there has been abnormal sweating induced after sym-pathetic procedures for a non-sweating symsym-pathetic disorder (e.g., FB). Hence, post-operative sweating is
not a sort of compensation but due to the feedback mechanism of the autonomic nervous system [5].
The triggering factors of hyperhidrosis are emotion and anxiety, rather than a hot environment [7, 8]. These factors stimulate the sweating center located in the hypothalamus, releasing efferent signals that are positive sympathetic tones to the target organs (e.g., the hands and feet). From the target organs, some afferent signals, which serve as negative feedback tones, return to the hypothalamus for the control of sweating (Fig.2).
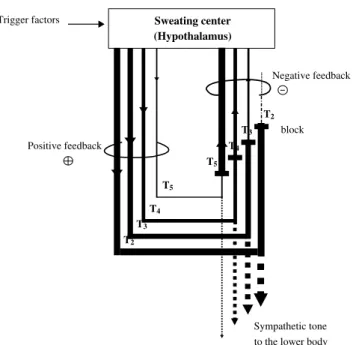
If the afferent negative feedback signals are mostly blocked, such as in T2 sympathectomy, the efferent positive signals from the hypothalamus will not be inhibited, thereby causing severe sweating in the lower body. This never happens in the upper body since the nerves to the upper body no longer exist (T2 was blocked). Consequently, if the negative feedback signals are only partially blocked, such as in T3or T4 sympathectomy, positive feedback signals are also partially inhibited, causing less post-operative sweat-ing over the lower body (Fig.3). This is why ‘‘reflex sweating’’ is a more precise term. As in hyperhidrosis, reflex sweating is emotion- and not climate-related.
Table 1 Lin–Telaranta Classification
(2004) Disorders Procedure
Group 1 Facial blushing ESB2
Group 2 Facial sweating, facial sweating with blushing ESB3
Group 3 Palmar sweating ESB4
Group 4 Axillary sweating (Bromidrosis) ESB5
Abbreviations: ESB2, endoscopic sympathetic block of T2; ESB3, endoscopic sympathetic block of T3; ESB4, endoscopic
sympathetic block of T4; ESB5, endoscopic sympathetic block of T5
Fig. 1 Chest roentgenographs during sympathetic blockade using the clipping method. Chest roentgenographs taken from a 20-year-old man undergoing T3
sympathetic block for HCF. Arrows indicate the location of clips. The initial sympathetic block (left film) was clipped at the wrong (T2) ganglion.
Post-operatively the patient experienced right face anhydrosis. The clip was corrected (right film) and all side effects were resolved
Trigger factors Efferent, positive tone Sweating center Hand sweating (Hypothalamus) negative feedback sympathetic ganglion To lower body Afferent,
Fig. 2 The possible mechanisms of emotional sweating as a negative feedback loop. Triggering factors (e.g., anxiety) activate ‘‘the sweating’’ area of the hypothalamus. This increases in efferent sympathetic activity to the target organs (e.g., to the hands) result in an increase in sweat production. Afferent signals from the target organs return back to the hypothalamus, and feedback to inhibit subsequent efferent output, creating a negative feedback loop
Many specialists still treat HP with a T2 and T3 level surgery [9]. As experience has shown, this
causes serious reflex sweating [10–12]. In our pre-vious study, 1.6% experienced regret towards the operation due to intolerable reflex sweating after ESB2 for HP [1]. Although the number does not seem great, a lot more patients actually experienced abnormally excessive sweating over the lower body. Ramicotomy [11,13], which includes division of the T2 and T3 rami only, theoretically reduces reflex sweating. However, the recurrence was high. In this study, we verified T4 as the target ganglion for HP. Nonetheless, further studies have to be done in order to understand the actual etiology of reflex sweating.
Although the authors of this study have the experience of over 1,000 cases, 4.4% were unilater-ally clipped at the wrong level. If sympathicotomy is the procedure of choice, it is difficult to evaluate the error. As a result, the blame is often laid on temperamental nature of the patient. The endoclip has become a good marker indicating whether the sympathetic procedure performed at the same location as in the pre-operative plan. As such, if the clipping was erroneously located, it can be re-ap-plied.
Conclusion
The advantages of clipping are the immediate recog-nition of location, its changeability, and its revers-ibility. It serves as a good marker for post-operative assessment and as an excellent pre-operative infor-mation for repeat operations.
Trigger factors
Positive feedback
Sympathetic tone to the lower body Sweating center (Hypothalamus) Negative feedback block T2 T3 T4 T5 T5 T4 T3 T2
Fig. 3 The proposed effect of the level of blocking on emotional sweating control. The magnitude of nerve activity is proportional to the width of the lines. If we consider the regulation of emotional sweating as a negative feedback loop (see Fig.2): if the inhibitory afferent signals are blocked (e.g., T2
block), then the hypothalamic (excitatory) efferent signals will not be inhibited. This will result in increased sweating in the lower body. Increased sweating in the upper body cannot occur as the nerves (e.g., T2) have been blocked.
However, if the inhibitory afferent signals are only partially blocked (e.g., T3or
T4block), there is some negative feedback control to the hypothalamus, and
inhibition of the excitatory efferent activity, therefore less inappropriate post-operative sweating in the lower body
References
1. Lin CC, Mo LR, Lee LS, Ng SM, Hwang MH (1998) Thoracoscopic T2-sympathec-tomy block by clipping – a better and reversible operation for treatment of hyperhidrosis palmaris: experience with 326 cases. Eur J Surg 580:13–16 2. Lin CC (1992) Extended thoracoscopic
T2-sympathectomy in treatment of hyperhidrosis: experience with 130 consecutive cases. J Laparoendoscopic Surg 2:1–6
3. Lin CC, Telaranta T (2001) Lin–Tela-ranta classification: the importance of different procedures for different indi-cations in sympathetic surgery. Annal Chirur Gynae 90:161–166
4. Rex LO, Drott C, Claes G, Gothberg G, Dalman P (1998) The boras experience of endoscopic thoracic sympathectomy for palmar, axillary, facial hyperhidro-sis and facial blushing. Eur J Surg Suppl 580:23–26
5. Loewy AD, Spyer KM (1990) Central regulation of autonomic functions. University Press, Oxford
6. Chou SH, Lee SH, Kao EL (1993) Tho-racic endoscopic T2-T3 sympathec-tomy in palmar hyperhidrosis: Experience of 112 cases. Jpn J Surg 23:105–107
7. Ogawa T (1975) Thermal influence on palmar sweating and mental influence on generalized sweating in man. Jpn J Physiol 25:525–536
8. Vetrugno R, Liguori R, Cortelli P, Montagna P (2003) Sympathetic skin response – basic mechanisms and clinical applications. Clin Auton Res 13:256–270
9. Arnold WS, Daniel TM (2005) Tho-racoscopic sympathectomy. In: Shield TW (ed) General thoracic sur-gery. 6th edn. Lippincott Williams & Wilkins, Philadelphia, pp 698–702
10. Edmondson RA, Banerjee AK, Rennie JA (1992) Endoscopic trans-thoracic sympathectomy in the treat-ment of hyperhidrosis. Ann Surg 215:289–293
11. Gossot D, Toledo L, Fritsch S, Celerier M (1997) Thoracoscopic sym-pathectomy for upper limb hyperhi-drosis: looking for the right operation. Ann Thorac Surg 64:975–978
12. Krasna MJ, Jiao X, Sonett J, Gamliel Z, King K (2000) Thoracoscopic sympa-thectomy. Surg Laparosc Endosc Perc-utan Tech 10:314–318
13. Wittmoser R (1992) Thoracoscopic sympathectomy and vagotomy. In: Cuschieri A, Buess G, Perissat J (eds) Operative manual of endoscopic sur-gery. Springer, New York, pp 110–133 242