2012/July/3
Libyan Journal of Medicine ID:18830 (Revision 1) Title Page
Type of manuscript: original paper
Manuscript title: Atorvastatin correlates with decreased risk of esophageal
cancer: a population-based case-control study from Taiwan
Running head: esophageal cancer and atorvastatin Shih-Wei Lai, MD1,2; Kuan-Fu Liao, MD and MS 3,4,5;
Hsueh-Chou Lai, MDand MS6,7; Chih-Hsin Muo, MPH8,9;
Fung-Chang Sung, PhD, MPH 8,9
(The first two authors contributed equally to this study.)
1School of Medicine, 6School of Chinese Medicine, and 8Department of Public
Health, China Medical University, Taichung, 404, Taiwan
2Department of Family Medicine, 7Department of Internal Medicine, and
9Management Office for Health Data, China Medical University Hospital, Taichung,
404, Taiwan
3Department of Internal Medicine, Taichung Tzu Chi General Hospital, Taichung,
427, Taiwan
4School of Medicine, Tzu Chi University, Hualien, 970, Taiwan
5Department of health care administration, Central Taiwan University of Science and
Technology, Taichung, 406, Taiwan Corresponding author:
Fung-Chang Sung, PhD, MPH
Professor, Department of Public Health, China Medical University, 91 Hsueh-Shih Road, Taichung 404, Taiwan
Phone: 886-4-2205-4070 Fax: 886-4-2201-9901
ABSTRACT
Objectives. The aim of this study was to explore the association between statins use
and esophageal cancer in Taiwan. Methods. We designed a case-control study using the database from Taiwan National Health Insurance. In all, 549 patients aged 20 years or older with newly diagnosed esophageal cancer as cases, and 2196 subjects without esophageal cancer as controls, from 2000 to 2009. The association between esophageal cancer and statins use and other co-morbidities were measured. Results. After adjustment for covariates, multivariate logistic regression showed patients with a cumulative duration of using atorvastatin ≥ 12 months might have a reduced risk of esophageal cancer, compared to those with non-use of statins (OR 0.14, 95% CI 0.04-0.56). The other statins could not show a significant association with esophageal cancer. Age (OR 1.01, 95% CI 1.00-1.01), alcoholism (OR 3.83, 95% CI 3.01-4.89), and esophageal diseases (OR 4.60, 95% CI 3.46-6.12) were independent factors significantly associated with esophageal cancer.
Conclusions. Use of atorvastatin ≥ 12 months may correlate with decreased risk of
esophageal cancer.
INTRODUCTION
In global estimates, esophageal cancer was the eighth commonly diagnosed cancer (482,300 new cases) and was the sixth leading cause of cancer deaths (406800 death cases) in the world in 2008 . In 2010, esophageal cancer was the eighth leading cause of cancer deaths in Taiwan, with a mortality rate of 6.8 per 100,000 persons (1563 death cases, 3.8% of the total) .
The etiology of esophageal cancer remains inconclusive, but a number of risk factors have been reported to be associated with esophageal cancer in previous literature, including Barrett's esophagus, gastroesophageal reflux disease, obesity, cigarette smoking, excess alcohol consumption, use of hot foods and drinks, and low intake of fresh fruit and vegetables . On the other hand, Helicobacter pylori infection and use of aspirin and non-steroidal anti-inflammatory drugs correlate with decreased risk of esophageal cancer .
HMG-CoA reductase inhibitors, usually known as statins, are commonly used to reduce the cholesterol level and further to decrease the risk of cardiovascular disease. Recently, two in vitro studies demonstrated that statins have the effects of inhibiting proliferation and further increasing apoptosis of esophageal adenocarcinoma cells . A case-control study by Nguyen et al in US showed that statins use correlates with 45% risk reduction of esophageal cancer in patients with existing Barrett's esophagus (95%
CI 0.36-0.86) .
To date, no study is found about the association between statins use and esophageal cancer in Taiwan. With comprehensive understanding of esophageal cancer, newer preventive strategies can be developed to help improve its outcomes and reduce its burden. Therefore, we conducted this case-control study using the National Health Insurance (NHI) program database in Taiwan to explore the following questions: (i) Is there an association between statins use and esophageal cancer? (ii) What are the effects of other co-morbidities and medications on the risk of esophageal cancer?
MATERIALS AND METHODS Data sources
This case-control study used data from The NHI program in Taiwan. The insurance program details can be found in previous studies . In order to secure patient privacy, all types of personal identification on files connected with this study were scrambled using surrogate identification numbers. This study was exempt from full review by the Institutional Review Board .
Inclusion criteria
We selected the subjects as cases who were newly diagnosed with esophageal cancer (International Classification of Diseases 9th Revision-Clinical Modification, ICD-9
codes 150.X and A-code A090) during the period of 2000-2009 and aged 20 years or older at the date of diagnosis. We defined the index date of each case as the date of diagnosis with esophageal cancer. For each esophageal cancer case, we randomly selected 4 subjects as controls from the same dataset who were frequency matched for sex, age (per 5 years) and index date. We excluded the subjects with esophageal cancer or any other cancer (ICD-9 codes 140-208 and A-code A08x-A14x) before the index date.
Potential co-morbidities and medications associated with esophageal cancer risk
risk of esophageal cancer, co-morbidities before the index date included were as follows: obesity (ICD-9 codes 278.00, 278.01, and A-code A183), esophageal diseases (ICD-9 codes 530.x and 947.2), Helicobacter pylori infection (ICD-9 codes 041.86), alcoholism (ICD-9 codes 303, 305.00, 305.01, 305.02, 305.03,and V11.3, and A-code A215), and tobacco use (ICD-9 codes 305.1). Medication history of six commercially available statins before the index date, including simvastatin, lovastatin, pravastatin, fluvastatin, atorvastatin, and rosuvastatin, were included. The other medications included were as follows: non-statin lipid-lowering drugs, proton pump inhibitors, histamine-2 receptor antagonists, aspirin, other non-steroidal anti-inflammatory drugs (NSAIDs), and cyclooxygenase-2 inhibitors (COX-2 inhibitors).
Statistical analysis
We demonstrated the differences in demographic factors, co-morbidities, and
medications between the esophageal cancer cases and the controls by the Chi-square test, t-test, and Fisher’s exact test. The significant variables were further included in the multivariate logistic regression analysis to measure odds ratio (OR) and 95% confidence interval (CI) for esophageal cancer. The statistical significance level was set at probability value of < 0.05 (SAS software version 9.1, SAS Institute Inc., Cary, North Carolina, USA).
RESULTS
Baseline characteristics of the study population
There were 549 cases of esophageal cancer and 2196 subjects without esophageal cancer as controls. Table 1 compares the demographic characteristics, co-morbidities, and medications between esophageal cancer cases and controls. The cases had higher proportions of alcoholism, esophageal diseases, use of proton pump inhibitors, use of histamine-2 receptor antagonists, use of other NSAIDs, and use of COX-2 inhibitors.
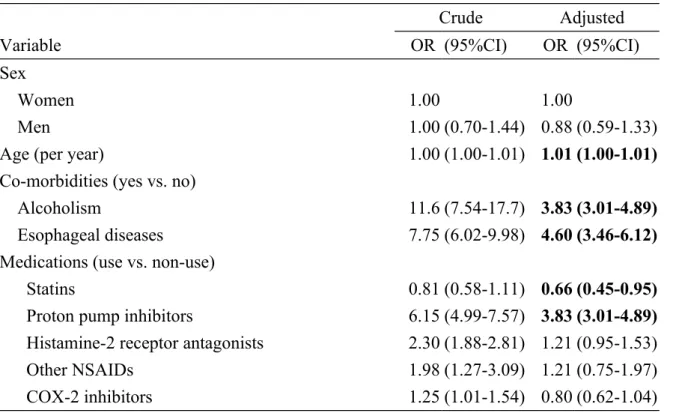
Esophageal cancer associated with statins use and covariates
After adjustment for covariates, multivariate logistic regression showed the adjusted OR of esophageal cancer was 0.66 (95% CI 0.45-0.95) for the group with statins use, when compared to the group with non-use of statins. Age (OR 1.01, 95% CI 1.00-1.01), alcoholism (OR 3.83, 95% CI 3.01-4.89), esophageal diseases (OR 4.60, 95% CI 3.46-6.12), and use of proton pump inhibitors (OR 3.83, 95% 3.01-4.89) were independent factors significantly associated with esophageal cancer (Table 2).
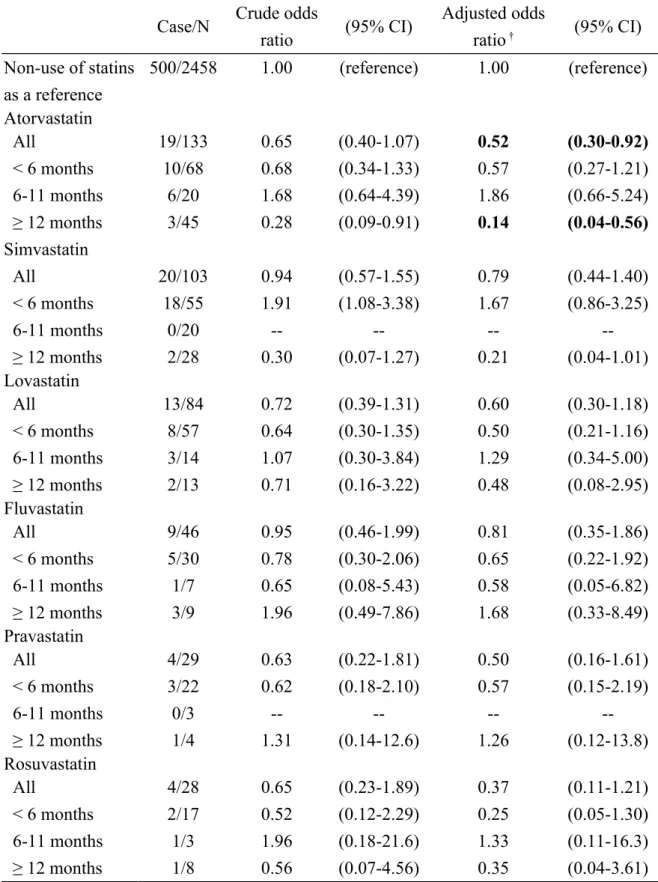
Sub-analysis of the association between six types of statins and esophageal cancer
In sub-analysis, patients with a cumulative duration of using atorvastatin ≥12 months had a reduced risk of esophageal cancer, compared to those with non-use of statins (OR 0.14, 95% CI 0.04-0.56). The other statins did not show a significant association with esophageal cancer (Table 3).
DISCUSSION
A growing body of epidemiologic evidence has shown that statins use can correlate with risk reduction of some digestive cancers, including stomach, colon-rectum, liver, and pancreas . To the best of our knowledge, the association between statins use and esophageal cancer is still under investigation. In this present study, we found patients with statins use had an overall 34% risk reduction of esophageal cancer, when
compared to the group with non-use of statins. In sub-analysis, atorvastatin could reduce 86% risk of esophageal cancer when used for ≥ 12 months. These results are consistent with a previous study . In that study by Nguyen et al, using statins for more than 12 months can correlate with 48% risk reduction of esophageal cancer in patients with existing Barrett's esophagus (95% CI 0.30-0.91) . Although the mechanism behind the correlation of statins use with decreased risk of esophageal cancer is not well elucidated, in vitro studies have demonstrated that statins have the effects of decreasing viability, decreasing proliferation, and increasing apoptosis of human esophageal adenocarcinoma cells . More studies are needed to explore the links between esophageal cancer and statins use to gain a better understanding of whether there are protective or harmful effects of statins on esophageal cancer risk.
Contrary to previous studies , we found that proton pump inhibitors might be associated with increased risk of esophageal cancer (OR 3.83). In our opinion, this
does not mean that proton pump inhibitors potentially cause esophageal cancer. Instead, we should point out that patients treated with proton pump inhibitors might be those with early undiagnosed esophageal cancer but initially presenting with esophageal symptoms and using proton pump inhibitors. That is, proton pump inhibitors may mask the diagnosis of esophageal cancer. We also found that
esophageal diseases also correlate with increased risk of esophageal cancer (OR 4.60). Thus, these findings alert clinicians to be more cautious of the potential risk of
esophageal cancer when patients present with esophageal symptoms.
There are a number of limitations in this study. The first concern is that we can not separately examined squamous cell cancer from adenocarcinoma of the esophagus due to inherent limitation of the dataset we used. This is a fundamental issue for analysis because these two cancers may be associated with some different risk factors . This indicates a future direction for research into the effects of statins on squamous cell cancer and adenocarcinoma of the esophagus. Second, lack of control for potentially confounding factors, including use of hot foods and drinks, and low intake of fresh fruit and vegetables, is also due to inherent limitation of this dataset. Third, the number of subjects for each of the individual statins is relatively small. Particularly, only 19 cases suffered from esophageal cancer in atorvastatin-use group
should be interpreted carefully because this figure is really too small to draw firm conclusions.
CONCLUSION
This study shows that use of atorvastatin ≥ 12 months may correlate with an 86% risk reduction of esophageal cancer. Age, alcoholism, and esophageal diseases are
Specific author contributions:
Shih-Wei Lai and Kuan-Fu Liao: (1) substantial contributions to the conception of this article; (2) planned and conducted the study; (3) initiated the draft of the article and critically revised the article;
Hsueh-Chou Lai and Chih-Hsin Muo: (1) conducted data analyses and participated in data interpretation; (2) critically revised the article;
Fung-Chang Sung: (1) conducted data analysis and participated in data interpretation; (2) critically revised the article.
Funding
This study was supported in part by grants from Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH101-TD-B-111-004), the Cancer Research Center of Excellence (DOH 101-TD-C-111-005), and the National Science Council (NSC 100-2621-M-039-001). The funding agencies did not
influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements
The authors thank the National Health Research Institute in Taiwan for providing the insurance claims data.
Conflict of Interest Statement
REFERENCES
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893-917.
2. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69-90.
3. Department of Health. Taiwan: Main Causes of Death in 2010. http://www.doh.gov.tw. [cited in 2012 February].
4. Pera M, Manterola C, Vidal O, Grande L. Epidemiology of esophageal adenocarcinoma. J Surg Oncol. 2005;92:151-9.
5. Falk GW. Risk factors for esophageal cancer development. Surg Oncol Clin N Am. 2009;18:469-85.
6. Hongo M, Nagasaki Y, Shoji T. Epidemiology of esophageal cancer: Orient to Occident. Effects of chronology, geography and ethnicity. J Gastroenterol Hepatol. 2009;24:729-35.
7. Kamangar F, Chow WH, Abnet CC, Dawsey SM. Environmental causes of esophageal cancer. Gastroenterol Clin North Am. 2009;38:27-57.
8. Ogunwobi OO, Beales IL. Statins inhibit proliferation and induce apoptosis in Barrett's esophageal adenocarcinoma cells. Am J Gastroenterol. 2008;103:825-37.
9. Sadaria MR, Reppert AE, Yu JA, Meng X, Fullerton DA, Reece TB, et al. Statin therapy attenuates growth and malignant potential of human esophageal adenocarcinoma cells. J Thorac Cardiovasc Surg. 2011;142:1152-60.
10. Nguyen DM, Richardson P, El-Serag HB. Medications (NSAIDs, statins, proton pump inhibitors) and the risk of esophageal adenocarcinoma in patients with Barrett's esophagus. Gastroenterology. 2010;138:2260-6.
11. Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC. Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore). 2010;89:295-9.
12. Lai SW, Muo CH, Liao KF, Sung FC, Chen PC. Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in taiwan. Am J Gastroenterol. 2011;106:1697-704.
13. Lai SW, Su LT, Lin CH, Tsai CH, Sung FC, Hsieh DP. Polypharmacy increases the risk of Parkinson's disease in older people in Taiwan: A population-based study.
Psychogeriatrics. 2011;11:150-6.
14. Lai SW, Chen PC, Liao KF, Muo CH, Lin CC, Sung FC. Risk of hepatocellular carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: a population-based cohort study. Am J Gastroenterol. 2012;107:46-52. 15. Poynter JN, Gruber SB, Higgins PD, Almog R, Bonner JD, Rennert HS, et al. Statins
and the risk of colorectal cancer. N Engl J Med. 2005;352:2184-92.
16. Khurana V, Sheth A, Caldito G, Barkin JS. Statins reduce the risk of pancreatic cancer in humans: a case-control study of half a million veterans. Pancreas. 2007;34:260-5.
17. El-Serag HB, Johnson ML, Hachem C, Morgana RO. Statins are associated with a reduced risk of hepatocellular carcinoma in a large cohort of patients with diabetes. Gastroenterology. 2009;136:1601-8.
18. Chiu HF, Ho SC, Chang CC, Wu TN, Yang CY. Statins are associated with a reduced risk of gastric cancer: a population-based case-control study. Am J
Gastroenterol. 2011;106:2098-103.
19. El-Serag HB, Aguirre TV, Davis S, Kuebeler M, Bhattacharyya A, Sampliner RE. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett's esophagus. Am J Gastroenterol. 2004;99:1877-83.
20. de Jonge PJ, Steyerberg EW, Kuipers EJ, Honkoop P, Wolters LM, Kerkhof M, et al. Risk factors for the development of esophageal adenocarcinoma in Barrett's esophagus. Am J Gastroenterol. 2006;101:1421-9.
Table 1. Comparison by demographic factors and other medical conditions between esophageal cancer cases and controls
Esophageal cancer No N= 2196 Yes N= 549 n (%) n (%) P value Sex 1.00 Women 156 (7.10) 39 (7.10) Men 2040 (92.9) 510 (92.9)
Age (Mean and SD, years)* 60.3 (13.3) 60.9 (12.9) 0.33 Co-morbidities
Alcoholism 31 (1.41) 78 (14.2) <0.0001
Tobacco use disorder 37 (1.68) 9 (1.64) 0.94
Obesity† 4 (0.18) 3 (0.55) 0.15
Esophageal diseases 128 (5.83) 178 (32.4) <0.0001
Helicobacter pylori infection 10 (0.46) 3 (0.55) 0.78 Medications
Use of statins 238 (10.8) 49 (8.93) 0.19
Use of non-statin lipid-lowering drugs
209 (9.52) 58 (10.6) 0.46 Use of proton pump inhibitors 284 (12.9) 262 (47.7) <0.0001
Use of histamine-2 receptor antagonists
1139 (51.9) 391 (71.2) <0.0001
Use of aspirin 715 (32.6) 187 (34.1) 0.50
Use of other NSAIDs 2021 (92.0) 526 (95.8) 0.002
Use of COX-2 inhibitors 534 (24.3) 157 (28.6) 0.04
Data are presented as the number of subjects in each group, with percentages given in parentheses. Chi-square test,*t-test and †Fisher’s exact test comparing subjects with
Table 2. Crude and adjusted odds ratios and 95% confidence intervals of esophageal cancer associated with statins use and covariates
Crude Adjusted
Variable OR (95%CI) OR (95%CI)
Sex
Women 1.00 1.00
Men 1.00 (0.70-1.44) 0.88 (0.59-1.33)
Age (per year) 1.00 (1.00-1.01) 1.01 (1.00-1.01)
Co-morbidities (yes vs. no)
Alcoholism 11.6 (7.54-17.7) 3.83 (3.01-4.89)
Esophageal diseases 7.75 (6.02-9.98) 4.60 (3.46-6.12)
Medications (use vs. non-use)
Statins 0.81 (0.58-1.11) 0.66 (0.45-0.95)
Proton pump inhibitors 6.15 (4.99-7.57) 3.83 (3.01-4.89) Histamine-2 receptor antagonists 2.30 (1.88-2.81) 1.21 (0.95-1.53)
Other NSAIDs 1.98 (1.27-3.09) 1.21 (0.75-1.97)
COX-2 inhibitors 1.25 (1.01-1.54) 0.80 (0.62-1.04)
Adjusted for sex, age, alcoholism, esophageal diseases, statins, proton pump inhibitors, histamine-2 receptor antagonists, other NSAIDs and COX-2 inhibitors
Table 3. Odds ratios and 95% confidence intervals of esophageal cancer by duration of statins use
Case/N Crude odds
ratio (95% CI) Adjusted odds ratio † (95% CI) Non-use of statins as a reference 500/2458 1.00 (reference) 1.00 (reference) Atorvastatin All 19/133 0.65 (0.40-1.07) 0.52 (0.30-0.92) < 6 months 10/68 0.68 (0.34-1.33) 0.57 (0.27-1.21) 6-11 months 6/20 1.68 (0.64-4.39) 1.86 (0.66-5.24) ≥ 12 months 3/45 0.28 (0.09-0.91) 0.14 (0.04-0.56) Simvastatin All 20/103 0.94 (0.57-1.55) 0.79 (0.44-1.40) < 6 months 18/55 1.91 (1.08-3.38) 1.67 (0.86-3.25) 6-11 months 0/20 -- -- -- --≥ 12 months 2/28 0.30 (0.07-1.27) 0.21 (0.04-1.01) Lovastatin All 13/84 0.72 (0.39-1.31) 0.60 (0.30-1.18) < 6 months 8/57 0.64 (0.30-1.35) 0.50 (0.21-1.16) 6-11 months 3/14 1.07 (0.30-3.84) 1.29 (0.34-5.00) ≥ 12 months 2/13 0.71 (0.16-3.22) 0.48 (0.08-2.95) Fluvastatin All 9/46 0.95 (0.46-1.99) 0.81 (0.35-1.86) < 6 months 5/30 0.78 (0.30-2.06) 0.65 (0.22-1.92) 6-11 months 1/7 0.65 (0.08-5.43) 0.58 (0.05-6.82) ≥ 12 months 3/9 1.96 (0.49-7.86) 1.68 (0.33-8.49) Pravastatin All 4/29 0.63 (0.22-1.81) 0.50 (0.16-1.61) < 6 months 3/22 0.62 (0.18-2.10) 0.57 (0.15-2.19) 6-11 months 0/3 -- -- -- --≥ 12 months 1/4 1.31 (0.14-12.6) 1.26 (0.12-13.8) Rosuvastatin All 4/28 0.65 (0.23-1.89) 0.37 (0.11-1.21) < 6 months 2/17 0.52 (0.12-2.29) 0.25 (0.05-1.30) 6-11 months 1/3 1.96 (0.18-21.6) 1.33 (0.11-16.3) ≥ 12 months 1/8 0.56 (0.07-4.56) 0.35 (0.04-3.61)
†Adjusted for age, sex, esophageal diseases, alcoholism, statins, proton pump inhibitors, histamine-2 receptor