BRIEF REPORT
Nationwide surveillance of antimicrobial resistance
among
Enterobacteriaceae in intensive care units in Taiwan
S.-S. Jean
&P.-R. Hsueh
&W.-S. Lee
&H.-T. Chang
&M.-Y. Chou
&I.-S. Chen
&J.-H. Wang
&C.-F. Lin
&J.-M. Shyr
&W.-C. Ko
&J.-J. Wu
&Y.-C. Liu
&W.-K. Huang
&L.-J. Teng
&C.-Y. Liu
Received: 30 April 2008 / Accepted: 25 July 2008 / Published online: 21 August 2008 # Springer-Verlag 2008
Abstract To determine the antimicrobial resistance profiles
among clinical isolates of Enterobacteriaceae in Taiwanese
intensive care units (ICUs), a national surveillance of
antibiotic resistance among important Enterobacteriaceae
was conducted from September 2005 through November
2005 at the ICUs of ten major teaching hospitals in Taiwan.
A total of 574 Enterobacteriaceae isolates recovered from
various clinical samples of our ICU patients were submitted
for in vitro test. Minimum inhibitory concentrations (MICs)
of these isolates to 18 antimicrobial agents were determined
by the broth microdilution method. The prevalences of
Enterobacteriaceae isolates with phenotypic
extended-spectrum
β-lactamase (ESBL) production were 26% in
Klebsiella pneumoniae, 16% in Serratia marcescens, 14%
in Escherichia coli, and 13% in Proteus mirabilis, in which
a significantly rising prevalence of ESBL production
among K. pneumoniae was noted (p=0.002) when
com-pared with a previous Taiwanese survey in 2000.
Hetero-S.-S. Jean
Departments of Intensive Care Units and Internal Medicine, Min-Sheng General Hospital,
Taoyuan County, Taiwan P.-R. Hsueh (*)
Departments of Laboratory Medicine and Internal Medicine, National Taiwan University Hospital,
National Taiwan University Medical College, 7 Chung-Shan South Road,
100 Taipei, Taiwan e-mail: [email protected] W.-S. Lee
Department of Internal Medicine, Taipei Municipal WanFang Hospital, Taipei, Taiwan
H.-T. Chang
Department of Internal Medicine, Far Eastern Memorial Hospital, Taipei County, Taiwan
M.-Y. Chou
Department of Internal Medicine, Cheng Hsin Rehabilitation Medical Center, Taipei, Taiwan
I.-S. Chen
Department of Internal Medicine, Cardinal Tien Hospital, Taipei County, Taiwan
J.-H. Wang
Department of Internal Medicine, China Medical College Hospital, Taichung, Taiwan
C.-F. Lin
Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
J.-M. Shyr
Department of Clinical Pathology, Taichung Veterans General Hospital, Taichung, Taiwan
W.-C. Ko
Departments of Internal Medicine, National Cheng-Kung University Hospital, Tainan, Taiwan
J.-J. Wu
School of Medical Technology,
National Cheng-Kung University College of Medicine, Tainan, Taiwan
Y.-C. Liu
Department of Clinical Pathology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
geneous resistance to various fluoroquinolones was found
among our Enterobacteriaceae isolates, except for
Ente-trobacter cloacae. Emergence of ertapenem-resistant
iso-lates of E. coli, K. pneumoniae, E. cloacae, and S.
marcescens was noted. Gradually increasing rates of
drug-resistant Enterobacteriaceae were noted in Taiwanese
ICUs. Periodic surveillance of the evolutionary trend of
antimicrobial resistance among ICU isolates is crucial for
starting appropriately empirical antimicrobial therapy in the
future.
Antimicrobial resistance is an increasing threat in
hospital-ized patients experiencing sepsis caused by
Enterobacter-iaceae, and it has resulted in increased illnesses, mortality,
and healthcare costs, particularly in patients admitted to
intensive care units (ICUs) [
1
,
2
]. National programs about
monitoring the trends of endemic resistance and comparing
the data with those of other countries are warranted to
guide optimal empirical antibiotics for selected infections.
Surveillance of Multicenter Antimicrobial Resistance in
Taiwan (SMART), initiated in 2000, is a nationwide
programme in Taiwan designed to monitor antimicrobial
resistance among clinically important bacteria.
From September 2005 through November 2005, the ICU
wards of ten major teaching hospitals in different regions of
Taiwan were involved in this study. A total of 574
non-duplicated isolates (one isolate per patient) of
Enterobac-teriaceae were collected. Identification of species was
performed with conventional biochemical methods and the
Vitek system (bioMérieux Vitek, St Louis, MO, USA). The
isolates that were recovered from various clinical specimens
included Escherichia coli (160 isolates), Klebsiella
pneu-moniae (162 isolates), Enterobacter cloacae (75 isolates),
Serratia marcescens (68 isolates), Citrobacter freundii (12
isolates), Morganella morganii (33 isolates), and Proteus
mirabilis (64 isolates). Antimicrobial susceptibility testing
was performed using the broth microdilution method
according to Clinical and Laboratory Standards Institute
(CLSI) recommendations [
3
]. A total of 18 antimicrobial
agents (Table
1
) were tested. Reference strains E. coli
ATCC 25922, K. pneumoniae ATCC 700603, and
Pseudo-monas aeruginosa ATCC 27853 were used as quality
control strains for each batch of MIC tests. Susceptibility
categories of these isolates were determined based upon
CLSI MIC breakpoints, except for moxifloxacin,
isepami-cin, and tigecycline in that their MIC breakpoints are not
available [
4
].
For phenotypic identification of extended-spectrum
β-lactamase (ESBL) production for E. coli, K. pneumoniae,
and P. mirabilis, CLSI guidelines using the confirmatory
disk diffusion methods were applied [
4
]. For other
Enter-obacteriaceae species, ESBL production was defined based
on the MICs of ceftazidime, ceftriaxone, or cefepime that
were equal to or greater than 2
μg/ml. If the MIC of
cefepime in the presence of clavulanic acid (10
μg) was at
least eight-fold less than that of cefepime, the isolate was
regarded to have ESBL production as previously described
[
5
].
Among these Enterobacteriaceae isolates, the most
common source (45.1%) was respiratory tract, 14.6% were
from patients with bloodstream infection, and 7.8% from
other sterile sites (pleural effusion, ascites, cerebrospinal
fluid, and synovial fluid). E. coli (27.9%) and K.
pneumo-niae (28.2%) were the two predominant bacteria of all
Enterobacteriaceae.
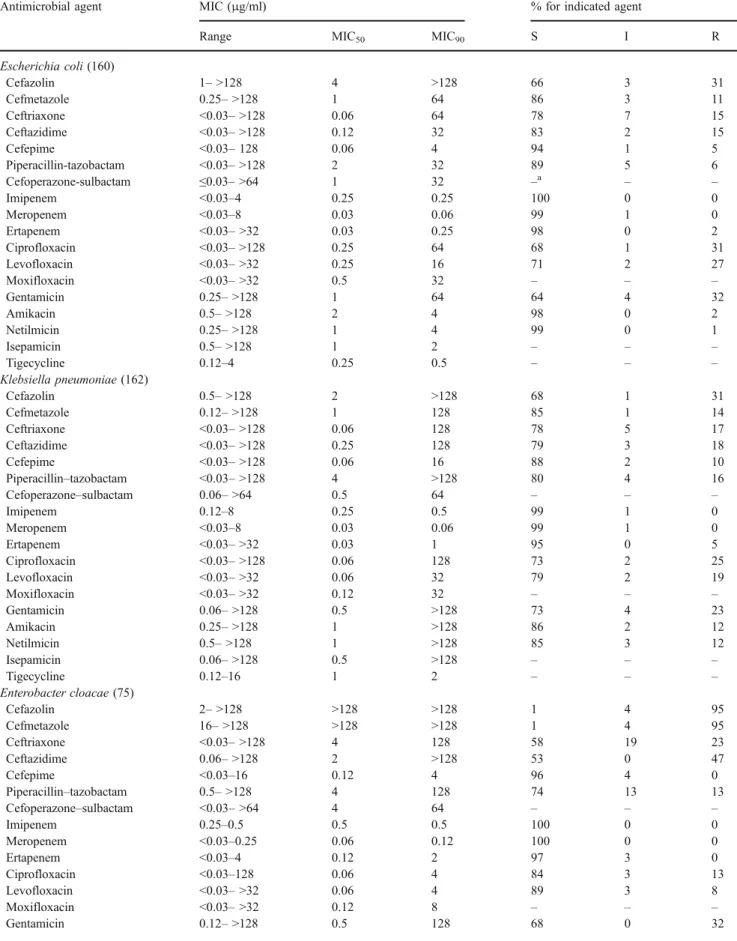
The results of antimicrobial susceptibilities for the
isolates are shown in Table
1
. With the exception of E.
cloacae and C. freundii, cefmetazole retained acceptable in
vitro activities (>75% susceptibilities) against the other
isolates. Ceftazidime and ceftriaxone exhibited good
activ-ities against Enterobacteriaceae isolates tested except E.
cloacae and C. freundii. Cefepime had rather low resistant
rates (<10%) for all isolates tested. Piperacillin-tazobactam
displayed fair (60–80%) susceptibility against E. cloacae,
C. freundii, and S. marcescens. In contrast, all carbapenems
exhibited excellent activities against all isolates tested.
However, eight K. pneumoniae isolates, two E. cloacae
isolates, and two S. marcescens isolates were not
suscep-tible to ertapenem. Additionally, one isolate of K.
pneumo-niae with intermediate susceptibility to imipenem and
meropenem was noted. Of note, levofloxacin has better in
vitro activity than ciprofloxacin against all these isolates.
The MIC
90levels of moxifloxacin was two-fold higher than
those of levofloxacin for most of our enterobacterial
isolates. Netilmicin and isepamicin showed similar in vitro
susceptibilities to amikacin, and these three agents had
remarkably better in vitro activity than gentamicin. All of
the isolates tested, except the P. mirabilis isolates (MIC
90,
32
μg/ml), were inhibited by 2 μg/ml of tigecycline.
It is noteworthy that in this survey K. pneumoniae
(26%), S. marcescens (16%), E. coli (14%), and P. mirabilis
W.-K. HuangDepartment of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
L.-J. Teng
School of Medical Technology, National Taiwan University Hospital,
National Taiwan University College of Medicine, Taipei, Taiwan
C.-Y. Liu
Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
Table 1 Antimicrobial susceptibilities of 574 clinical Enterobacteriaceae isolates recovered from patients treated at ICUs of ten major teaching hospitals in Taiwan in 2005
Antimicrobial agent MIC (μg/ml) % for indicated agent
Range MIC50 MIC90 S I R
Escherichia coli (160) Cefazolin 1– >128 4 >128 66 3 31 Cefmetazole 0.25– >128 1 64 86 3 11 Ceftriaxone <0.03– >128 0.06 64 78 7 15 Ceftazidime <0.03– >128 0.12 32 83 2 15 Cefepime <0.03– 128 0.06 4 94 1 5 Piperacillin-tazobactam <0.03– >128 2 32 89 5 6 Cefoperazone-sulbactam ≤0.03– >64 1 32 –a – – Imipenem <0.03–4 0.25 0.25 100 0 0 Meropenem <0.03–8 0.03 0.06 99 1 0 Ertapenem <0.03– >32 0.03 0.25 98 0 2 Ciprofloxacin <0.03– >128 0.25 64 68 1 31 Levofloxacin <0.03– >32 0.25 16 71 2 27 Moxifloxacin <0.03– >32 0.5 32 – – – Gentamicin 0.25– >128 1 64 64 4 32 Amikacin 0.5– >128 2 4 98 0 2 Netilmicin 0.25– >128 1 4 99 0 1 Isepamicin 0.5– >128 1 2 – – – Tigecycline 0.12–4 0.25 0.5 – – – Klebsiella pneumoniae (162) Cefazolin 0.5– >128 2 >128 68 1 31 Cefmetazole 0.12– >128 1 128 85 1 14 Ceftriaxone <0.03– >128 0.06 128 78 5 17 Ceftazidime <0.03– >128 0.25 128 79 3 18 Cefepime <0.03– >128 0.06 16 88 2 10 Piperacillin–tazobactam <0.03– >128 4 >128 80 4 16 Cefoperazone–sulbactam 0.06– >64 0.5 64 – – – Imipenem 0.12–8 0.25 0.5 99 1 0 Meropenem <0.03–8 0.03 0.06 99 1 0 Ertapenem <0.03– >32 0.03 1 95 0 5 Ciprofloxacin <0.03– >128 0.06 128 73 2 25 Levofloxacin <0.03– >32 0.06 32 79 2 19 Moxifloxacin <0.03– >32 0.12 32 – – – Gentamicin 0.06– >128 0.5 >128 73 4 23 Amikacin 0.25– >128 1 >128 86 2 12 Netilmicin 0.5– >128 1 >128 85 3 12 Isepamicin 0.06– >128 0.5 >128 – – – Tigecycline 0.12–16 1 2 – – – Enterobacter cloacae (75) Cefazolin 2– >128 >128 >128 1 4 95 Cefmetazole 16– >128 >128 >128 1 4 95 Ceftriaxone <0.03– >128 4 128 58 19 23 Ceftazidime 0.06– >128 2 >128 53 0 47 Cefepime <0.03–16 0.12 4 96 4 0 Piperacillin–tazobactam 0.5– >128 4 128 74 13 13 Cefoperazone–sulbactam <0.03– >64 4 64 – – – Imipenem 0.25–0.5 0.5 0.5 100 0 0 Meropenem <0.03–0.25 0.06 0.12 100 0 0 Ertapenem <0.03–4 0.12 2 97 3 0 Ciprofloxacin <0.03–128 0.06 4 84 3 13 Levofloxacin <0.03– >32 0.06 4 89 3 8 Moxifloxacin <0.03– >32 0.12 8 – – – Gentamicin 0.12– >128 0.5 128 68 0 32
Table 1 (continued)
Antimicrobial agent MIC (μg/ml) % for indicated agent
Range MIC50 MIC90 S I R
Amikacin 0.5– >128 1 8 97 0 3 Netilmicin 0.25– >128 1 4 98 0 2 Isepamicin 0.5– >128 1 2 – – – Tigecycline 0.5–8 1 1 – – – Serratia marcescens (68) Cefazolin 32– >128 >128 >128 0 0 100 Cefmetazole 4– >128 16 128 76 9 15 Ceftriaxone 0.06– >128 4 >128 70 9 21 Ceftazidime 0.12– >128 1 8 90 1 9 Cefepime 0.04–64 0.25 16 84 13 3 Piperacillin-tazobactam 1– >128 8 64 63 34 3 Cefoperazone–sulbactam 0.25– >64 8 >64 – – – Imipenem 0.12–2 0.5 0.5 100 0 0 Meropenem <0.03–2 0.03 0.12 100 0 0 Ertapenem <0.03–16 0.12 0.5 97 0 3 Ciprofloxacin 0.06–128 2 32 43 16 41 Levofloxacin 0.06– 32 1 8 66 9 25 Moxifloxacin 0.06– >32 2 16 – – – Gentamicin 0.5– >128 8 >128 47 10 43 Amikacin 1– >128 2 >128 87 0 13 Netilmicin 0.5– >128 2 >128 85 0 15 Isepamicin 0.5– >128 2 >128 – – – Tigecycline 1–8 2 2 – – – Citrobacter freundii (12) Cefazolin 2– >128 128 >128 33 0 67 Cefmetazole 0.5–128 32 128 25 25 50 Ceftriaxone 0.06–64 0.25 32 59 33 8 Ceftazidime 0.25–128 0.5 128 50 0 50 Cefepime <0.03–1 0.06 1 100 0 0 Piperacillin–tazobactam 2– >128 4 >128 67 0 33 Cefoperazone–sulbactam 0.5– >64 1 >64 – – – Imipenem 0.12–0.5 0.25 0.5 100 0 0 Meropenem <0.03–0.06 0.03 0.06 100 0 0 Ertapenem <0.03–1 0.03 1 100 0 0 Ciprofloxacin <0.03–8 0.25 4 75 0 25 Levofloxacin <0.03–2 0.25 2 100 0 0 Moxifloxacin 0.12–8 0.5 4 – – – Gentamicin 0.12– >128 0.5 128 67 0 33 Amikacin 0.5–8 1 4 100 0 0 Netilmicin 0.5–8 1 4 100 0 0 Isepamicin 0.5–1 1 1 – – – Tigecycline 0.5–1 0.5 1 – – – Morganella morganii (33) Cefazolin >128 >128 >128 0 0 100 Cefmetazole 4–64 8 16 97 0 3 Ceftriaxone <0.03–128 0.03 4 94 0 6 Ceftazidime 0.12– >128 0.25 4 91 0 9 Cefepime <0.03–2 0.03 0.25 100 0 0 Piperacillin–tazobactam 0.12– >128 0.5 2 97 0 3 Cefoperazone–sulbactam 1–64 2 8 – – – Imipenem 0.06–0.25 0.25 0.25 100 0 0 Meropenem 0.06–0.12 0.12 0.12 100 0 0 Ertapenem <0.03–0.25 0.03 0.06 100 0 0 Ciprofloxacin <0.03–32 1 8 55 24 21
(13%) were the four leading pathogens with the highest
rates of ESBL production. None of our C. freundii isolates
exhibited ESBL-producing phenotype.
This 2005 multicenter study regarding the antimicrobial
susceptibilities of Enterobacteriaceae disclosed three
im-portant points. First, persistently high rates of ESBL
phenotype were found among our K. pneumoniae and E.
coli isolates. In comparison with the data in 2000 [
1
], a
2.4-fold increase in the prevalence rate of ESBL phenotype was
found among K. pneumoniae isolates (p=0.002, by
chi-square test). Second, high percentages (>10%) of ESBL
phenotype were also found in our S. marcescens and P.
mirabilis isolates. Third, carbapenem-resistant
Enterobac-teriaceae isolates have emerged in ICUs in Taiwan.
In this study, the prevalence rates of ESBL-producing K.
pneumoniae and E. coli isolates resembled those of ICU
pathogens in North America [
6
]. Fortunately, these rates
remained lower than those from Latin America and several
Asian countries [
5
,
7
]. Higher prevalence of ESBL
production among our S. marcescens isolates than two
common AmpC producers (E. cloacae and C. freundii)
might be partially responsible for the higher non-susceptible
rate of S. marcescens to cefepime.
Carbapenems are often considered as the last resort for
the management of serious infections in ICUs. However,
ertapenem was considered as the most vulnerably affected
carbapenem agent against K. pneumoniae (with plasmid
encoding AmpC or ESBLs or in porin-deficient isolates)
[
8
], E. coli (AmpC
β- lactamase production, associated
with loss of both OmpC and OmpF porins) [
9
], and E.
cloacae (with enhanced efflux of ertapenem) isolates [
10
],
which was consistent with our data in terms of higher
non-susceptibilities of ertapenem than others. Concerning the
susceptibilities of fluoroquinolones in our study, with the
exception of E. cloacae, the other Enterobacteriaceae
showed heterogeneous susceptible rates to these agents.
However, levofloxacin was significantly more active
against important enteric GNBs than ciprofloxacin in our
ICU survey results. Finally, except for Proteus isolates,
tigecycline possessed excellent in vitro activity against
Table 1 (continued)Antimicrobial agent MIC (μg/ml) % for indicated agent
Range MIC50 MIC90 S I R
Levofloxacin <0.03–8 0.5 8 82 3 15 Moxifloxacin 0.06–32 2 16 – – – Gentamicin 0.05– >128 2 128 61 0 39 Amikacin 0.5–4 1 2 100 0 0 Netilmicin 0.25– 8 1 4 100 0 0 Isepamicin 0.5–8 1 4 – – – Tigecycline 1–8 2 2 – – – Proteus mirabilis (64) Cefazolin 4– >128 8 >128 59 13 28 Cefmetazole 1–16 2 4 100 0 0 Ceftriaxone <0.03–128 <0.03 8 95 2 3 Ceftazidime <0.03–32 0.12 0.5 97 0 3 Cefepime 0.06–16 0.12 4 98 2 0 Piperacillin–tazobactam 0.25–16 0.5 1 100 0 0 Cefoperazone–sulbactam 0.5–32 2 16 – – – Imipenem <0.03–0.12 0.06 0.12 100 0 0 Meropenem <0.03–0.12 0.06 0.06 100 0 0 Ertapenem <0.03–0.12 <0.03 0.03 100 0 0 Ciprofloxacin <0.03–64 0.5 32 60 6 34 Levofloxacin 0.06– >32 0.5 16 64 11 25 Moxifloxacin 0.25– >32 4 32 – – – Gentamicin 0.5– >128 16 >128 42 3 55 Amikacin 1– >128 4 8 91 0 9 Netilmicin 0. 5– >128 4 16 90 6 4 Isepamicin 2– >128 8 16 – – – Tigecycline 2–>32 16 32 – – –
S susceptible, I intermediate, R resistant
Enterobacteriaceae isolates, including phenotypic
ESBL-and AmpC-producing organisms. However, because of its
bacteriostatic mechanism, close monitoring of future
changes in the values of tigecycline MIC for
Enterobacter-iaceae isolates is warranted.
In conclusion, the emergence of ESBL-producing
Enter-obacteriaceae other than E. coli and K. pneumoniae was
found. Resistance to carbapenems is emerging, and
resis-tance to fluoroquinolones continues to be a worrisome
problem. Periodic surveillance of antimicrobial resistances
among isolates from ICUs is crucial for initiation of
appropriate empirical antimicrobial therapy.
References
1. Hsueh PR, Liu YC, Yang D, Yan JJ, Wu TL, Huang WK et al (2001) Multicenter surveillance of antimicrobial resistance of major bacterial pathogens in intensive care units in 2000 in
Taiwan. Microb Drug Resist 7:373–382. doi:10.1089/
10766290152773383
2. Ho PL, Chan WM, Tsang KW, Wong SS, Young K (2002) Bacteraemia caused by Escherichia coli producing
extended-spectrum β-lactamase: a case-control study of risk factors and
outcomes. Scand J Infect Dis 34:567–573. doi:10.1080/
00365540210147516
3. Clinical and Laboratory Standards Institute (2005) Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, 6th edn. Approved standard M7-A6. CLSI, Wayne, PA, USA
4. Clinical and Laboratory Standards Institute (2005) Performance
standards for antimicrobial susceptibility testing—fifteenth
infor-mational supplement. M100-S15. CLSI, Wayne, PA, USA 5. Paterson DL, Rossi F, Baquero F, Hsueh PR, Woods GL,
Satishchandran V et al (2005) In vitro susceptibilities of aerobic and facultative Gram-negative bacilli isolated from patients with intra-abdominal infections worldwide: the 2003 Study for Mon-itoring Antimicrobial Resistance Trends (SMART). J Antimicrob
Chemother 55:965–973. doi:10.1093/jac/dki117
6. Streit JM, Jones RN, Sader HS, Fritsche TR (2004) Assessment of pathogen occurrences and resistance profiles among infected patients in the intensive care unit: report from the SENTRY Antimicrobial Surveillance Programme (North America, 2001).
Int J Antimicrob Agents 24:111–118. doi:10.1016/j.ijantimicag.
2003.12.019
7. Gales AC, Sader HHS, Jones RN (2002) Respiratory tract pathogens isolated from patients hospitalized with suspected pneumonia in Latin America: frequency of occurrence and antimicrobial susceptibility profile: results from the SENTRY
Antimicrobial Surveillance Program (1997–2000). Diagn
Micro-biol Infect Dis 44:301–311. doi:10.1016/S0732–8893(02)
00499–6
8. Jacoby GA, Mills DM, Chow N (2004) Role ofβ-lactamases and
porins in resistance to ertapenem and other β-lactams in
Klebsiella pneumoniae. Antimicrob Agents Chemother 48:3203–
3206. doi:10.1128/AAC.48.8.3203–3206.2004
9. Mammeri H, Nordmann P, Berkani A, Eb F (2008) Contribution of extended-spectrum AmpC (ESAC) beta-lactamases to carbape-nem resistance in Escherichia coli. FEMS Microbiol Lett
282:238–240. doi:10.1111/j.1574–6968.2008.01126.x
10. Szabó D, Silveira F, Hujer AM, Bonomo RA, Hujer KM, Marsh JW et al (2006) Outer membrane protein changes and efflux pump expression together may confer resistance to ertapenem in
Enter-obacter cloacae. Antimicrob Agents Chemother 50:2833–2835.