On: 28 April 2014, At: 16:47 Publisher: Routledge
Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Social Work in End-Of-Life &
Palliative Care
Publication details, including instructions for authors and subscription information:
http://www.tandfonline.com/loi/wswe20
Relationship Between Pain and Chronic
Illness Among Seriously Ill Older Adults:
Expanding Role for Palliative Social Work
Mary Beth Morrissey a , Deborah Viola b & Qiuhu Shi ca
Global Healthcare Innovation Management Center , Fordham University Graduate School of Business Administration , West Harrison , New York , USA
b
Center for Long Term Care Research & Policy , New York Medical College, School of Health Sciences and Practice , Valhalla , New York , USA
c
Epidemiology and Community Health , New York Medical College, School of Health Sciences and Practice , Valhalla , New York , USA Published online: 14 Mar 2014.
To cite this article: Mary Beth Morrissey , Deborah Viola & Qiuhu Shi (2014) Relationship Between Pain and Chronic Illness Among Seriously Ill Older Adults: Expanding Role for Palliative Social Work, Journal of Social Work in End-Of-Life & Palliative Care, 10:1, 8-33, DOI: 10.1080/15524256.2013.877861 To link to this article: http://dx.doi.org/10.1080/15524256.2013.877861
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
and-conditions
8 Copyright © Taylor & Francis Group, LLC ISSN: 1552-4256 print/1552-4264 online DOI: 10.1080/15524256.2013.877861
Received 3 October 2012; accepted 3 July 2013.
Address correspondence to Mary Beth Morrissey, PhD, MPH, JD, Fordham University Graduate School of Business Administration, Global Healthcare Innovation Management Center, 400 Westchester Avenue, West Harrison, NY 10604, USA. E-mail: mamorrissey@ fordham.edu
PEER-REVIEWED ARTICLES
Relationship Between Pain and Chronic Illness
Among Seriously Ill Older Adults: Expanding
Role for Palliative Social Work
MARY BETH MORRISSEY
Global Healthcare Innovation Management Center, Fordham University Graduate School of Business Administration, West Harrison, New York, USA
DEBORAH VIOLA
Center for Long Term Care Research & Policy, New York Medical College, School of Health Sciences and Practice, Valhalla, New York, USA
QIUHU SHI
Epidemiology and Community Health, New York Medical College, School of Health Sciences and Practice, Valhalla, New York, USA
Confronting the issue of pain among chronically ill older adults merits serious attention in light of mounting evidence that pain in this population is often undertreated or not treated at all (Institute of Medicine, 2011). The relationship between pain and chronic illness among adults age 50 and over was exam-ined in this study through the use of longitudinal data from the University of Michigan Health and Retirement Study, spon-sored by the National Institute on Aging and the Social Security Administration. Findings suggested positive associations between pain and chronic disease, pain and multimorbidity, as well as an inverse association between pain and education. Policy impli-cations for workforce development and public health are many, and amplification of palliative social work roles to relieve pain
and suffering among seriously ill older adults at all stages of the chronic illness trajectory is needed.
KEYWORDS chronic illness, pain, palliative social work, public health
INTRODUCTION
Chronic illness is widely recognized as a major public health problem in the United States and creates challenges related to both prevention and pain and disease management. There is broad consensus that the incidence and prevalence of chronic illness and chronic pain impose an unacceptably high burden of illness and suffering in society as a whole. This burden has unintended consequences as well as social and economic costs. Many mem-bers of the society, who continue to face disparities in pain care (Meghani et al., 2012; Sacco, Deravin Carr, & Viola, 2013), also experience widening gaps in income prosperity and longevity (Olshansky et al., 2012). These consequences and costs also correlate with low educational attainment and other deeply embedded economic and social structural and system level factors such as occupation, poverty, racial/ethnic minority status, lack of insurance and underinsurance, geography, and language barriers (Atlas & Skinner, 2010; Meghani et al., 2012; Olshansky et al., 2012). The challenges posed by this structural/system complexity have been the subject of exten-sive policy debate as they pertain to implementation of health reform and health care cost containment initiatives, and their impact on long-term care services (Baicker, Shepard, & Skinner, 2013; Wiener, 2013). As such chal-lenges affect aging adults and Medicare beneficiaries, who often suffer from advanced life-limiting illnesses, frailty, and functional impairments, questions about the role of government and appropriate policy interventions become even more critical.
While research increasingly focuses on the growing problem of mul-tiple chronic conditions among older adults (Freid, Bernstein, & Bush, 2012), the relationship of pain to chronic illness has not received adequate atten-tion. The experience and treatment of pain are an integral part of devising policy solutions and advocacy responses to address older adults’ complex health needs and inequities.
Social work (Altilio, 2004; Altilio, Otis-Green, Hedlund, & Cohen Fineberg, 2006; Cagle & Altilio, 2011) and other disciplines have contrib-uted significant knowledge about pain as a multidimensional experience, but more work needs to be done across provisions of care in advancing understanding about the interaction between pain and chronic illness in complex social environments. Consistent with the well-established World Health Organization (1946) definition of health, a public health approach to understanding chronic illness involves a turn to the underlying social
determinants of health that ground an examination of health issues and assessment of impact on population health and well-being. The entangle-ments of pain and chronic illness merit investigation in the context of older adults’ unique social ecologies including such factors as health status, neigh-borhood, housing, education, resources, benefits, income, occupation, access or barriers to health services, health literacy, communication with physicians and other health professionals, marital status, and social support.
Persistent pain has been described and formally recognized only in the last decade as a chronic illness in its own right that threatens multiple domains of well-being (Institute of Medicine [IOM], 2011). In cases where persistent pain goes unattended or becomes intolerable or intractable, it may often lead to detrimental and unrelieved suffering for older adults.
Recent studies have yielded fruitful insights into the significant role of emotional, social, and spiritual processes and states including attachment and empathy (Lumley et al., 2011; Sulmasy, 2002; Wachholtz, Pearce, & Koenig, 2007). This research provides evidence of the promise nonpharmacologic approaches to pain relief and palliative care may hold.
The present study was undertaken to examine the relationship between pain and chronic illness among a population of primarily community-dwelling adults and a small population of nursing home residents using longitudinal data from the University of Michigan Health and Retirement Study (Health and Retirement Study, 2002–2010). While a wealth of research has been conducted examining the data of the Health and Retirement Study, this study analyzes the data through the framework of pain experienced by chronic illness sufferers.
The purpose of the study was to build empirical knowledge and provide insight into the nature and scope of the pain-chronic illness relationship to inform social work policy, advocacy, and practice. The researchers hypothe-sized that pain and chronic disease are positively associated, thereby increas-ing older adults’ disease burden and medically complex needs, and that pain and chronic disease are negatively associated with functioning.
CHRONIC ILLNESS AND FRAILTY
Patterns of chronic illness, frailty, and pain and suffering pose increasingly dif-ficult challenges for health care providers and professionals who serve older adults with advanced life-limiting illness across care settings, as well as their family caregivers. Generally, frailty has been defined in the literature as an impairment of physiological systems, both quantitatively and qualitatively (Weiss, Hoenig, Varadhan, Simonsick, & Fried, 2010; Rodriguez-Mañas et al., 2013). Factors associated with frailty include weakness, weight loss, reduced activity and lower extremity exercise capacity, a decline in reserve and resis-tance, and increased risk of functional limitations that may necessitate long-term
care services and more frequent hospitalizations and care transitions (Naylor et al., 2012; Reinhard, Levine, & Samis, 2012; Rodriguez-Mañas et al., 2013; Weiss et al., 2010). However, there is no clear consensus regarding an opera-tional definition of frailty for clinical purposes (Rodriquez-Mañas et al., 2013).
Recent research on multimorbidity, defined as two or more chronic diseases coexisting in the same individual, shows that it is a common prob-lem in older people that increases risks of mortality, physical and mental functional limitations and losses, detrimental impacts on quality of life, and severity of disease or multimorbidity burden (Diederichs, Berger, & Bartels, 2011; Lappenschaar, Hommersom, & Lucas, 2012). Lunney, Lynn, and Hogan (2003) reported that the trajectory of dying for frail decedents is associated with more functional decline and disability at the end of life than for can-cer, organ failure, or sudden death decedents. For example, Chiu and Wray (2011) have presented evidence that there is a high rate of disability over time in frail adults with a diagnosis of diabetes, particularly for women, non-Whites, and less educated adults. In a study by Murphy et al. (2011), findings suggested a dependent relationship between functional disability and death. Researchers reported that decedents, as compared with survivors, had a rapid decline in functional ability in the months prior to death.
In a recent study of family caregiving (Reinhard et al., 2012), researchers found that the presence of chronic conditions in multiple and overlapping physical, cognitive, sensory, and behavioral domains increased the com-plexity of the medical/nursing tasks required of caregivers and the burden on family caregivers. The researchers reported that in addition to complex medical/nursing care, family caregivers were also performing care coordina-tion roles. Study results of the relacoordina-tionship between chronic condicoordina-tions and effects on care recipients’ quality of life also showed decreasing indepen-dence and increased activity limitations among care recipients with five or more chronic conditions. In situations in which care recipients were living with five or more chronic conditions, family caregivers felt they were helping to keep their loved ones from being institutionalized (Reinhard et al., 2012).
Mezey, Dubler, Mitty, and Brody (2002) and others (Naylor et al., 2012; Reinhard et al., 2012) have addressed the impact of setting and care transi-tions on quality of life and the quality of the dying process for vulnerable older people who may be approaching the end of life, including those in skilled nursing facilities. Over 20% of deaths occur in skilled nursing facili-ties, calling attention to the need to improve quality of life for frail nursing home residents even as they may be nearing the end of life (Bern-Klug, 2010; Bern-Klug & Simons, 2011). The profile of actively dying older adults in skilled nursing facilities is one generally characterized by frailty, dementia, feeding and hydration issues, and pain and suffering. Nursing home residents who are frail and burdened with chronic illness live through a longer and somewhat unpredictable dying period that is characterized by decreasing independence and sometimes loss of appetite (Allegre, 2010; Lynn, 2005).
Pain in older adults, and in older women in particular, is well-documented in the literature (Gold & Roberto, 2000; Peat, Thomas, Handy, & Croft, 2004; Roberto, Perkins, & Holland, 2007; Roberto & Reynolds, 2002; Smith et al., 2010; Teno, Kabumoto, Wetle, Roy, & Mor, 2004; Tse, Leung, & Ho, 2012). The prevalence of pain among institutionalized older adults is reported in the literature in a mid- to high range from 45 to 85% (Smith et al., 2010; Tse et al., 2012). The American Geriatrics Society (AGS) Panel on Persistent Pain in Older Persons (2002) reported that approximately 45 to 80% of older adult nursing home residents are undertreated for substantial pain. The experience of pain in older adults has been found to be associated with fatigue, sleep-ing problems, depressed mood, cognitive impairment, diminished physical activity and function, and quality of life as well as increased health care costs (AGS, 2002; Griffin, Harmon, & Kennedy, 2012; IOM, 2011; Jakobbson, Klevsgard, Westergren, & Hallberg, 2003; Shega et al., 2012). The presence of pain may also affect older adults’ relationships and intimacy with family members (Roberto, 2001).
In its groundbreaking 2011 report, Relieving Pain in America:
A Blueprint for Transforming Prevention, Care, Education and Research, the
IOM described the magnitude of pain as a public health problem in the United States, citing the growing prevalence and incidence of pain, health disparities in the assessment and treatment of pain conditions, and the enor-mous social and economic consequences of pain. The IOM report recog-nized that pain, in addition to constituting a chronic condition in its own right in many cases, is a significant yet frequently overlooked aspect of chronic disease and multimorbidity. While acknowledging the difficulty of arriving at an accurate estimate of prevalence due to variations in definitions of pain and methods used, the IOM reported that approximately 100 million people in the United States are living with pain.
The authors of the IOM report (2011) specifically linked rising pain prevalence to the aging of the U.S. population and the associated chronic diseases such as diabetes, cardiovascular disorders, arthritis, and cancer. Suffering from multiple diseases was also cited as a factor contributing to severity of pain among elderly persons. Elderly persons, persons with cog-nitive impairments including dementia, and persons at the end of life were among the populations identified by the IOM as at risk for under treatment of pain. The IOM estimated that the cost impact of pain to U.S. society is somewhere between $560 and $635 billion per annum, accounting for health care costs and losses in productivity.
In a more recent study by researchers at Johns Hopkins University (Gaskin & Richard, 2012), the economic burden and costs of pain in the United States were measured using data from the U.S. Department of Health and Human Services Medical Expenditure Panel Survey. The study sample of 15,954 noninstitutionalized persons with pain, ranging from ages 24 to 64, was defined using the following measures: persons who self-reported that
they experienced pain that limited their ability to work; persons diagnosed with joint pain or arthritis; and persons who had a disability that limited their ability to work. The researchers hypothesized that as pain increased, utilization and intensity of health services increased. Drawing first on other studies, researchers reported variation in chronic pain prevalence by type of pain such as migraine, neck, and lower back, ranging from 2 to 40% (Manchikanti, Singh, Datta, Cohen, & Hirsch, 2009; Turk, 2002). Variation was also reported in the economic costs associated with different types of pain. Estimates for indirect costs of pain were reported ranging from $6.9 billion (Turk & Theodore, 2011) to over $60 billion (Stewart, Ricci, Chee, Morganstein, & Lipton, 2003) in productivity losses. Gaskin and Richard (2012) acknowledged the limitations of these previous studies which drew on different sources and samples, and therefore did not provide a complete picture of relevant markets.
Gaskin and Richard’s (2012) own study showed that adults with pain had higher health care expenditures than adults without pain. Researchers reported that women were more likely to incur health care expenditures and higher expenditures as compared to men. The level of incurring health care expenditures also increased by age, education, income, and health insurance status. The researchers estimated that 100 million people in the United States had at least one pain condition, with joint pain being the most prevalent pain condition. Incremental costs of health care for these pain conditions ranged from $251 to $300 billion per annum, and indirect costs from lower productivity from $299 to $335 billion (Gaskin & Richard, 2012). Gaskin and Richard (2012) also cited the limitations of their own research study. Because the study did not include experiences of pain among institutionalized, noncivilian populations such as nursing home residents, military personnel, and prison inmates, nor of adults under 24 or over 65, or their caregivers, they described their estimates of the cost of chronic pain as conservative. Their study also did not evaluate costs associated with the emotional or psychological impacts of chronic pain experiences.
Policy Issues
Three of the most central issues in current public policy discussions concern-ing the public health crisis of increasconcern-ing chronic illness are management of the dual-eligible Medicare beneficiary population with multiple chronic con-ditions, utilization of health care services at the end of life, and health care costs and their ethical implications.
A recently issued National Center for Health Statistics Brief (Freid et al., 2012) reported trend data over the last 10 years documenting an increase in the prevalence of multiple chronic conditions among older adults. According to this report, between the decades 1999–2000 and 2009–2010, the prevalence
of both hypertension and diabetes in adults 65 and over increased from 9 to 15%. The prevalence rates of hypertension and other chronic conditions increased by three percentage points.
The U.S. Department of Health and Human Services has devel-oped a strategic framework for addressing multiple chronic conditions, which includes strengthening the public health systems through invest-ments supporting both research and targeted initiatives under the Patient Protection and Affordable Care Act (ACA, 2010). Under the ACA (2010), the U.S. Department of Health and Human Services (HHS) has established a new Federal Coordinated Health Care Office (the Medicare-Medicaid Coordination Office) to work with states to improve the coordination of care for 9 million Americans enrolled in both the Medicare and Medicaid programs (Cassidy, 2012). Important goals of this new office are also to help states save money and improve care through providing better access to Medicare data and funding demonstration projects. The Centers for Medicare and Medicaid Services (CMS) reports annual expenditures of $300 billion to care for this sickest and most vulnerable population of older adults enrolled in both Medicare and Medicaid. Approximately 60% of these older adults have multiple chronic illnesses resulting in complex medical needs. In 2008, these highest cost beneficiaries, who constituted 15% of Medicaid enrollees and 20% of Medicare beneficiaries, accounted for 39% of Medicaid spending and 31% of Medicare spending (Cassidy, 2012; Gold, Jacobson, & Garfield, 2012).
The Hospital Readmissions Reduction Program, the National Pilot Program on Payment Bundling, and the Community-Based Care Transitions Program, provisions of the ACA that target the Medicare population, aim to improve transitional care (Naylor et al., 2012). According to Naylor et al. (2012), these recent initiatives under the ACA to reduce hospital readmis-sions and improve care transitions may not fully account for the multiple chronic conditions, functional impairments, and more complex medical and long-term care service needs of the frail elderly population. At present, these initiatives may have the unintended consequences of further frag-menting care for older adults in particular, especially in continuity of care from hospital and postacute to long-term care. Naylor et al. (2012) also suggest that misaligned payment incentives in the new bundled payment proposals may impede the transition to long-term care services for many frail older adults.
For many frail elderly persons who need long-term services, illness and dying trajectories are made that much more difficult by transitions in and out of emergency departments and hospitals. Several recent studies have identified social structural factors that correlate with older adults’ overall health and health care utilization including Emergency Department (ED) use. A 2008 United Hospital Fund study in New York City showed that over 25% of ED visits by adults in the over 65 category resulted in admissions,
exceeding any other age category (Raven & Gould, 2008). The research also showed a strong neighborhood effect, with higher ED visit rates in neigh-borhoods with higher rates of poverty and mortality. A more recent United Hospital Fund report (2012) that focused on “treat and release” ED visits also showed a neighborhood effect defined by the researchers as an association between ED use and neighborhood poverty, insurance status, race/ethnicity, poor health status, and barriers to accessing care such as no regular doc-tor. Researchers also reported that more frequent ED use resulted in more frequent hospitalizations. Additionally, ED usage was higher in communities of color, particularly among Black and Latino persons. Residential instabil-ity and risk of homelessness as well as complex illness needs were also cited as drivers of more intense use of medical services including both ED services and inpatient care. In a recent study of pain care for older adults administered in the ED, researchers (Hwang, Richardson, Harris, & Morrison, 2010) also identified pain care disparities in the ED setting that showed older adults were less likely than younger adult patients to receive opioid analge-sics for moderate to severe pain.
The high incidence and prevalence of pain in elderly adults, along with the increased likelihood of undertreatment, demand investigation of these gaps in care. Not surprisingly, given the high incidence and prevalence of chronic illness among elderly persons and resulting complex medical needs, historically there has been a high utilization of services in the last 6 months of life nationwide, although with wide regional variations. While Dartmouth Institute researchers (Goodman et al., 2013; Goodman, Esty, Fisher, & Chang, 2011) have reported that end-of-life trends in the United States among Medicare beneficiaries have improved in certain areas, such as days spent in the hospital and utilization of hospice, for the years 2007 through 2010 the number of physician visits and number of days spent in the ICU remained relatively stable. For the same period, there was a 15.2% increase in Medicare spending per patient during the last 2 years of life (Goodman et al., 2013). Smith et al. (2012) reported in a recent analysis of longitudinal data from the Health and Retirement Study that ED use for patients 65 and older in both the last 6 months and the last month of life contributed to high end-of-life costs and increased risk of heightened illness burden. In a study of deceased Medicare beneficiaries with poor-prognosis cancer, in which patients were likely to die within a year, Morden et al. (2012) found individuals received high intensity care in the last weeks of life on 11 end-of-life care measures that varied widely across all types of hospitals. Out-of-pocket health care expenditures in the last 5 years prior to death have also been reported to be high for Medicare beneficiaries, exceeding more than half of their baseline assets on average and posing a financial risk to older adults near the end of life (Kelley et al., 2012).
In a recent article on health care costs as an ethical issue in the context of chronic illness in the aging population and medical services at the end of
life, Jennings and Morrissey (2011) recognized limits on resources and the absence of an absolute right to medical treatment. However, the authors did advocate for the right to palliative care for persons who are chronically ill or at the end of life, suggesting that this may be the most cost effective reform, in addition to the most humane. There is strong evidence that palliative care is cost effective (Morrison et al., 2011; Morrison et al., 2008; Viola, Leven, & LePere, 2009).
METHODOLOGY
Sample and Demographics
The researchers conducted a study analyzing longitudinal survey data from the University of Michigan Health and Retirement Study, sponsored by the National Institute for Aging and the Social Security Administration, for the years 2002, 2004, 2006, 2008, and 2010—constituting five “waves” of data— to examine the relationship between pain and chronic illness. The research questions were: Are there associations between pain and chronic illness, pain and number of chronic diseases (i.e., multimorbidity), and pain and chronic disease and functioning. The hypotheses included: pain and chronic illness, and pain and multimorbidity would be positively associated, but that pain and chronic disease would be negatively associated with functioning. A sample comprised mainly community-dwelling adults, the majority of whom were over 65, were represented in this national survey. The sample also included nursing home residents.
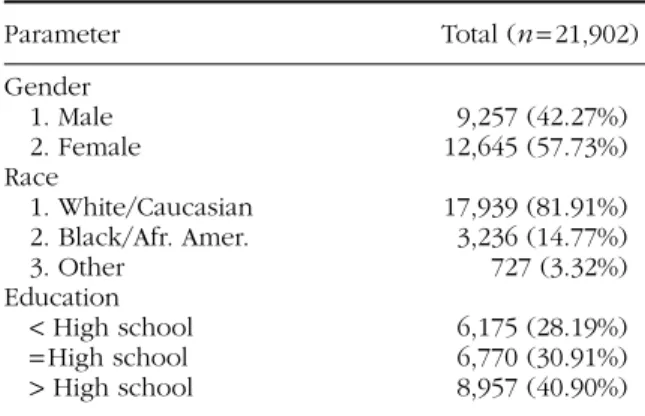
This study’s measures included demographic characteristics—such as gender, race, and education—for a sample of 21,902 individuals in total who participated in one or more of the five waves. Many people in the longitu-dinal study participated in several of the waves; however, each individual is counted only once for the total number of participants.
The majority of participants were female, White/Caucasian, or in the 65 to 84 age category. Over 96% were community-dwelling adults, and nearly 72% had achieved at least a high school education (see Tables 1 and 2). In 2010, more than 70% of participants were 65 or older, with more than 10% in the oldest old category of 85 and above. Fewer than 30% of participants were in the 50 to 64 age bracket. These numbers showed a decline in the 50 to 64 age bracket over the five waves from 2002, and a trending upward for that same period for the 65 to 84 and 85-plus age brackets. In 2010, more than half of participants were married and almost all community-dwelling. Under 4% of participants, or 530 persons, reported living in a nursing home (see Table 2). While nearly 41% of study partici-pants had over a high school education, nearly 60% had completed their education at the high school level.
Measurement of Variables
The variables of age, marital status, living in a nursing home, type of illness, and pain were measured at 2-year intervals over a 10-year period in the Health and Retirement Study. This study examined data from five waves of the study, between 2002 and 2010, with discrete 2-year intervals of data col-lection. Certain demographic characteristics of subjects who participated in at least one wave data did not change. However, certain data trends, such as increasing prevalence of chronic disease, may have been due to some mem-bers of the sample getting older.
DEPENDENTVARIABLE
Consistent with understanding of pain, pain was conceptualized as experi-enced by the study participant and measured based upon the participant’s self-report. The pain variable was operationalized into whether a person was troubled with pain (yes/no), the level of pain intensity they experienced most of the time (from mild to severe), and whether pain interfered with usual activities such as household chores or work (yes/no).
INDEPENDENTVARIABLES
Age, marital status, living in a nursing home, and number and type of chronic diseases were selected as the independent variables of interest in this study (see Table 2). The marital status variable is defined as currently married or living with a partner. Consistent with the literature on multimor-bidity, disease burden is used in this study to reference number and type of chronic diseases as well as their associated risks and outcomes. Marital status, social and family support have been positively associated with the
TABLE 1 Demographic Characteristics of Subjects Who Had at Least One Wave Data (2002–2010)
Parameter Total (n = 21,902) Gender 1. Male 9,257 (42.27%) 2. Female 12,645 (57.73%) Race 1. White/Caucasian 17,939 (81.91%) 2. Black/Afr. Amer. 3,236 (14.77%) 3. Other 727 (3.32%) Education < High school 6,175 (28.19%) = High school 6,770 (30.91%) > High school 8,957 (40.90%) Note. Pain study using Health and Retirement Study data
(2002–2010).
T
ABLE 2
P
ain and Disease Status W
ith Subjects Who Had at Least One W
av e Data (2002–2010) P a rameter 2002 (n = 17,336) 2004 (n = 18,729) 2006 (n = 17,430) 2008 (n = 16,372) (n Gender 1. Male 7,213 (41.61%) 7,932 (42.35%) 7,255 (41.62%) 6,751 (41.24%) 5,986 (40.75%) 2. Female 10,123 (58.39%) 10,797 (57.65%) 10,175 (58.38%) 9,621 (58.76%) 8,705 (59.25%) Race 1. White/Caucasian 14,513 (83.72%) 15,421 (82.34%) 14,417 (82.71%) 13,493 (82.42%) 12,057(82.07%) 2. Black/Afr . Amer . 2,422 (13.97%) 2,741 (14.64%) 2,499 (14.34%) 2,371 (14.48%) 2,147 (14.61%) 3. Other 401 (2.31%) 567 (3.03%) 514 (2.95%) 508 (3.10%)
Education < High school
5,209 (30.05%) 5,130 (27.39%) 4,633 (26.58%) 4,211 (25.72%) 3,599 (24.50%) = High school 5,555 (32.04%) 5,841 (31.19%) 5,450 (31.27%) 5,098 (31.14%) 4,563 (31.06%) > High school 6,572 (37.91%) 7,758 (41.42%) 7,347 (42.15%) 7,063 (43.14%) 6,529 (44.44%) Age 50–64 6,617 (38.17%) 7,864 (41.99%) 6,295 (36.12%) 5,295 (32.34%) 4,338 (29.53%) 65–84 9,371 (54.06%) 9,460 (50.51%) 9,630 (55.25%) 9,496 (58.00%) 8,825 (60.07%) ≥ 85 1,348 (7.78%) 1,405 (7.50%) 1,505 (8.63%) 1,581 (9.66%) 1,528 (10.40%) Marital status No 6,241 (36.03%) 6,698 (35.79%) 6,348 (36.42%) 6,127 (37.43%) 5,718 (38.93%) Y e s 11,081 (63.97%) 12,017 (64.21%) 11,080 (63.58%) 10,243 (62.57%) 8,971 (61.07%)
Living in nursing home No
16,820 (97.02%) 18,218 (97.27%) 16,944 (97.21%) 15,880 (96.99%) 14,161 (96.39%) Y e s 516 (2.98%) 511 (2.73%) 486 (2.79%) 492 (3.01%)
Number of chronic diseases* 0
3,871 (22.33%) 4,564 (24.37%) 3,775 (21.66%) 3,197 (19.53%) 1 6,522 (37.62%) 6,750 (36.04%) 6,219 (35.69%) 5,845 (35.71%) 5,034 (34.27%) 2 4,247 (24.50%) 4,542 (24.25%) 4,442 (25.49%) 4,287 (26.19%) 4,082 (27.79%) 3 1,942 (11.20%) 2,011 (10.74%) 2,093 (12.01%) 2,107 (12.87%) 2,023 (13.77%) 4 636 (3.67%) 708 (3.78%) 718 (4.12%) 744 (4.54%) 5 108 (0.62%) 132 (0.70%) 164 (0.94%) 173 (1.06%) 6 10 (0.06%) 20 (0.11%) 15 (0.09%) 17 (0.10%) 18
19
T
roubled with pain No
12,089 (69.86%) 12,518 (67.00%) 11,443 (65.76%) 10,726 (65.60%) 9,186 (62.64%) Y e s 5,216 (30.14%) 6,166 (33.00%) 5,959 (34.24%) 5,625 (34.40%) 5,479 (37.36%) How pain No P ain 12,089 (69.94%) 12,518 (67.11%) 11,443 (65.86%) 10,726 (65.67%) 9,186 (62.75%) Mild 1,320 (7.64%) 1,681 (9.01%) 1,639 (9.43%) 1,561 (9.56%) 1,553 (10.61%) Moder ate 2,915 (16.86%) 3,358 (18.00%) 3,156 (18.17%) 3,101 (18.99%) 2,974 (20.32%) Se v ere 962 (5.57%) 1,096 (5.88%) 1,136 (6.54%) 944 (5.78%) 925 (6.32%) P ain eff e ct activities No 14,051 (81.28%) 14,817 (79.43%) 13514 (77.74%) 12,711 (77.81%) 11,176 (76.39%) Y e s 3,236 (18.72%) 3,838 (20.57%) 3,869 (22.26%) 3,625 (22.19%) 3,455 (23.61%) Diabetes No 14,200 (81.94%) 15,194 (81.21%) 13,768 (79.08%) 12,670 (77.47%) 11,064 (75.43%) Y e s 3,129 (18.06%) 3,515 (18.79%) 3,642 (20.92%) 3,685 (22.53%) 3,603 (24.57%) Cancer ex cluding skin No 14,907 (86.02%) 16,124 (86.16%) 14,794 (84.96%) 13,714 (83.82%) 12,125 (82.63%) Y e s 2,423 (13.98%) 2,591 (13.84%) 2,619 (15.04%) 2,647 (16.18%) 2,548 (17.37%) Lung disease No 15,539 (89.68%) 16,761 (89.55%) 15,495 (89.01%) 14,464 (88.39%) 12,913 (88.00%) Y e s 1,789 (10.32%) 1,955 (10.45%) 914 (10.99%) 1,899 (11.61%) 1,761 (12.00%) Hear t condition No 12,782 (73.78%) 13,958 (74.61%) 12,685 (72.86%) 11,799 (72.14%) 10,424 (71.07%) Y e s 4,543 (26.22%) 4,751 (25.39%) 4,726 (27.14%) 4,556 (27.86%) 4,244 (28.93%) Strok e No 15,930 (91.94%) 17,282 (92.31%) 16,003 (91.89%) 14,969 (91.50%) 13,339 (90.87%) Y e s 1,397 (8.06%) 1,440 (7.69%) 1,413 (8.11%) 1,391 (8.50%) 1,341 (9.13%) Ar thritis No 6,606 (38.16%) 7,477 (39.98%) 6,561 (37.68%) 5,841 (35.73%) 4,986 (34.02%) Y e s 10,705 (61.84%) 11,227 (60.02%) 10,850 (62.32%) 10,505 (64.27%) 9,670 (65.98%) Back P ain No 113 (59.79%) 11,853 (63.39%) 101 (60.84%) 10,424 (63.75%) 51 (49.51%) Y e s 76 (40.21%) 6,847 (36.61%) 65 (39.16%) 5,927 (36.25%) 52 (50.49%) Note. P
ain study using Health and R
etirement Study data (2002–2010).
*Chronic diseases included: diabetes,
cancer (ex cluding skin), lung disease, hear t condition, strok e, and ar thritis. Missing, D K (don’t know), (refused to answ er) ex cluded.
care of seriously ill older adults (Auslander & Freedenthal, 2006; Gardener, 2011). Residence, such as a in nursing home, and social environment can also affect older adults’ care and health such as living in a nursing home (Bern-Klug & Simons, 2011). The type of chronic disease and chronic dis-ease burden, as well as their associations with pain, were also independent variables of interest in this study.
RESULTS
Prevalence of Chronic Disease
There was considerable variation in the prevalence of chronic diseases by number. The number of participants with no chronic disease or with only one chronic disease declined over the 10-year period of the study, while in every other category rates of prevalence rose. Among rising rates of preva-lence in the categories of two or more diseases, the highest prevapreva-lence was almost 28% in the category of two or more chronic diseases in 2010, up from 24.50% in 2002. This rate was still lower than the 34.27% prevalence rate for one chronic disease (see Table 2).
Data were reported by disease category for the following diseases, each of which increased in prevalence over time: diabetes, cancer (excluding skin), lung disease, heart condition, stroke, arthritis, as well as back pain. Prevalence rates were the highest in the categories of arthritis—ranging from 60.02 to 65.98%—and back pain—ranging between 36.25 and 50.49% (see Table 2).
Prevalence of Pain
Approximately one-third of participants reported having trouble with pain, with some variation over the five waves, trending upward about 7 points, to 37.36% in 2010 from 30.14% in 2002. The number of participants with no pain declined over the five waves (range: 69.86 to 62.64%). Prevalence of pain by intensity was highest at the moderate level (20.32%) over the five waves. In all three levels—mild, moderate, severe—prevalence rates rose over the 10-year period (see Table 2).
In 2010, 23.61% of participants reported that pain made it difficult for them to perform their usual activities such as household chores or work, referred to in this study as “pain effect.” This prevalence rate also increased over the five waves from 18.72% in 2002 (see Table 2).
Results for pain effect activities over the years show some variation for pain intensity. At the moderate level of pain effect, the highest prevalence of pain effect over the years was 59.06% as compared to 25.80% in the severe category. For all of the chronic diseases, pain effect prevalence is highest over the five waves in the moderate category.
PAINAND AGE
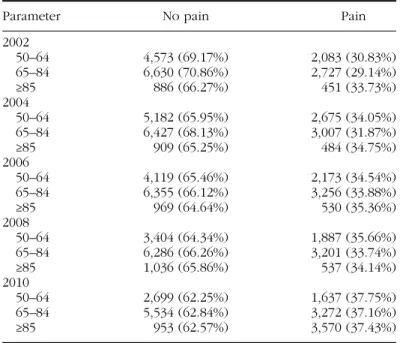
Pain prevalence (“troubled with pain” variable) rose in each age bracket over the five waves with a slight dip moving from the 50 to 64 age bracket to the 65 to 84 age bracket (50 to 64 range: 30.83–37.75%; 65 to 84 range: 29.14–37.16%). In 2010, the prevalence of pain for the 85 and over age bracket lagged slightly behind the prevalence of pain for the 50 to 64 age bracket (37.43 as compared to 37.75%). The largest growth in prevalence of pain was in the 65 to 84 age bracket, going from 29.14% in 2002 to 37.16% in 2010. These data show gener-ally that variation in self-reported pain was fairly stable over the five waves in the three age brackets, with a steady progression upward (see Table 3).
Reported levels of pain also trended upward in each category of pain intensity over the years by age. At the moderate pain level, in the 65 to 84 age bracket, the range was from 16.74 to 20.42%; in the 85 and over age bracket, pain held at about 20%; in the 50 to 64 bracket, the range was from 16.40 to 19.73%. Overall participants in the 85 and over bracket experienced the highest pain levels. In all age brackets, pain reported at the level of severe pain intensity was fairly stable over the years, with little variation. PAIN, MARITALSTATUS, ANDRESIDENCE
Pain prevalence by marital status was significantly lower overall among the married than those who were not married, with that gap widening further over time. Pain prevalence rates rose among married individuals at a slower progression over the waves of the study than among those who were not
TABLE 3 Pain Over Years (2002–2010) for Age
Parameter No pain Pain
2002 50–64 4,573 (69.17%) 2,083 (30.83%) 65–84 6,630 (70.86%) 2,727 (29.14%) ≥85 886 (66.27%) 451 (33.73%) 2004 50–64 5,182 (65.95%) 2,675 (34.05%) 65–84 6,427 (68.13%) 3,007 (31.87%) ≥85 909 (65.25%) 484 (34.75%) 2006 50–64 4,119 (65.46%) 2,173 (34.54%) 65–84 6,355 (66.12%) 3,256 (33.88%) ≥85 969 (64.64%) 530 (35.36%) 2008 50–64 3,404 (64.34%) 1,887 (35.66%) 65–84 6,286 (66.26%) 3,201 (33.74%) ≥85 1,036 (65.86%) 537 (34.14%) 2010 50–64 2,699 (62.25%) 1,637 (37.75%) 65–84 5,534 (62.84%) 3,272 (37.16%) ≥85 953 (62.57%) 3,570 (37.43%)
married (married range: 28.95–35.46%; nonmarried range: 32.22–40.35%). Similarly, pain prevalence was higher for those who were living in nursing homes, where nearly all residents regardless of marital status live apart from their spouses and the attendant social support they provide, as compared to those who were community-dwelling (42.48 vs. 37.17%).
PAIN, GENDER, ANDRACE
The prevalence of pain by gender was higher among females (range: 32.62 to 40.37%) over the 10-year period than males. Pain prevalence was also higher among White/Caucasians (range: 30.36 to 37.34%) than Black/African Americans, with the gap between White/Caucasians and Black/African Americans narrowing over the 10-year period (in 2010, 37.34 vs. 37.10%). PAINAND DISEASECATEGORY
For all of the chronic diseases (back pain excluded), pain prevalence rose over the years, with heart condition and arthritis having the biggest jumps in pain prevalence over the five waves. In 2010, lung disease had the highest pain prevalence rate (53.24%) followed by arthritis (48.13%).
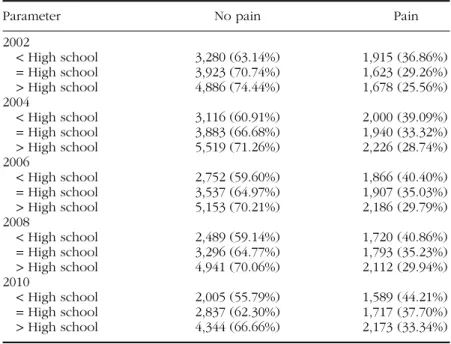
Pain and Education
The data on pain and education show an inverse relationship between pain and education (see Table 4). As education grade level increased, pain decreased. Conversely, as education grade level decreased, pain increased.
TABLE 4 Pain Over Years (2002–2010) for Education
Parameter No pain Pain
2002 < High school 3,280 (63.14%) 1,915 (36.86%) = High school 3,923 (70.74%) 1,623 (29.26%) > High school 4,886 (74.44%) 1,678 (25.56%) 2004 < High school 3,116 (60.91%) 2,000 (39.09%) = High school 3,883 (66.68%) 1,940 (33.32%) > High school 5,519 (71.26%) 2,226 (28.74%) 2006 < High school 2,752 (59.60%) 1,866 (40.40%) = High school 3,537 (64.97%) 1,907 (35.03%) > High school 5,153 (70.21%) 2,186 (29.79%) 2008 < High school 2,489 (59.14%) 1,720 (40.86%) = High school 3,296 (64.77%) 1,793 (35.23%) > High school 4,941 (70.06%) 2,112 (29.94%) 2010 < High school 2,005 (55.79%) 1,589 (44.21%) = High school 2,837 (62.30%) 1,717 (37.70%) > High school 4,344 (66.66%) 2,173 (33.34%)
While data have suggested an inverse relationship between education level and prevalence of chronic disease, education may also mediate the relation-ship between pain and chronic disease. Pain prevalence rates (troubled with pain) by pain intensity followed a similar pattern, with the highest preva-lence rates in the moderate category of pain intensity. Pain prevapreva-lence rates rose among people of all education levels over the five waves of the study.
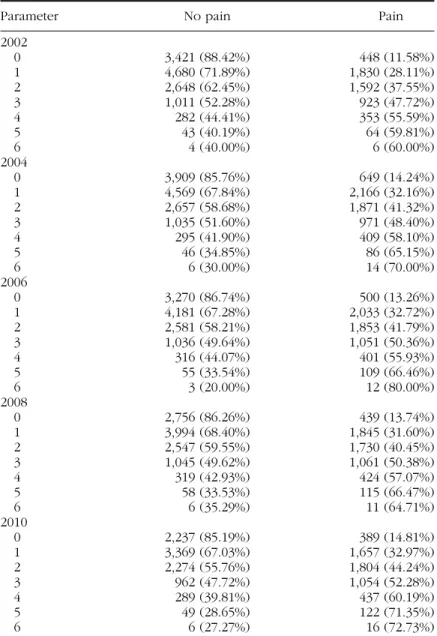
TABLE 5 Pain Over Years (2002–2010) for Number of Chronic Diseases*
Parameter No pain Pain
2002 0 3,421 (88.42%) 448 (11.58%) 1 4,680 (71.89%) 1,830 (28.11%) 2 2,648 (62.45%) 1,592 (37.55%) 3 1,011 (52.28%) 923 (47.72%) 4 282 (44.41%) 353 (55.59%) 5 43 (40.19%) 64 (59.81%) 6 4 (40.00%) 6 (60.00%) 2004 0 3,909 (85.76%) 649 (14.24%) 1 4,569 (67.84%) 2,166 (32.16%) 2 2,657 (58.68%) 1,871 (41.32%) 3 1,035 (51.60%) 971 (48.40%) 4 295 (41.90%) 409 (58.10%) 5 46 (34.85%) 86 (65.15%) 6 6 (30.00%) 14 (70.00%) 2006 0 3,270 (86.74%) 500 (13.26%) 1 4,181 (67.28%) 2,033 (32.72%) 2 2,581 (58.21%) 1,853 (41.79%) 3 1,036 (49.64%) 1,051 (50.36%) 4 316 (44.07%) 401 (55.93%) 5 55 (33.54%) 109 (66.46%) 6 3 (20.00%) 12 (80.00%) 2008 0 2,756 (86.26%) 439 (13.74%) 1 3,994 (68.40%) 1,845 (31.60%) 2 2,547 (59.55%) 1,730 (40.45%) 3 1,045 (49.62%) 1,061 (50.38%) 4 319 (42.93%) 424 (57.07%) 5 58 (33.53%) 115 (66.47%) 6 6 (35.29%) 11 (64.71%) 2010 0 2,237 (85.19%) 389 (14.81%) 1 3,369 (67.03%) 1,657 (32.97%) 2 2,274 (55.76%) 1,804 (44.24%) 3 962 (47.72%) 1,054 (52.28%) 4 289 (39.81%) 437 (60.19%) 5 49 (28.65%) 122 (71.35%) 6 6 (27.27%) 16 (72.73%)
Note. Pain study using Health and Retirement Study data (2002–2010).
*Chronic diseases included: diabetes, cancer (excluding skin), lung disease, heart condition, stroke, and arthritis.
Pain and Chronic Disease Burden
As hypothesized, the data show a positive association between pain and chronic disease burden over the years (see Table 5). In every case over the five waves of the study, pain prevalence rates rose as the number of chronic diseases rose and disease burden increased. For example, in 2010, pain prevalence was nearly 73% for six chronic diseases as compared to only roughly 44% for two chronic diseases. Pain prevalence over the years for number of chronic disease by pain intensity followed a similar pattern. In the mild and moderate categories there was some variation in the category of six chronic diseases. A pattern was more pronounced in the severe category. For example, for six chronic diseases, pain intensity in the severe category rose from 20% in 2002 to 45% in 2004, and rose to a 50% prevalence rate in 2010.
DISCUSSION
The “triple aims” of health reform in the United States under the ACA (2010)—sometimes referred to as better health, better health care, and lower costs—are to expand insurance coverage, reduce health care costs, and improve the public health. While sometimes overlooked in policy discus-sions, this last public policy goal is central to successful implementation of the ACA. Further, understanding the experiences and ecology of pain, espe-cially within particularly vulnerable populations, is paramount to the nation’s public health.
While prevalence of chronic illness is a public health challenge that spans all ages, older adults experience high suffering and illness burden as they age, sometimes enduring multiple chronic conditions. Exploring and understand-ing more about the etiology of chronic illness, as well as its prevalence among older adults, and the consequences and costs are critical to developing public health prevention strategies. To change illness trajectories and social condi-tions that contribute to persistent disparities and inequities for the older adult population, the contributing factors and the complex impact of the pain expe-rience on particularly vulnerable individuals, such as nursing home residents, must be at the fore of public health consciousness, especially with the grave personal and economic costs associated with the end of life.
The data examined in this particular study over the five waves of the Health and Retirement Study supported the hypotheses that there would be a positive association between pain and chronic disease, and more specifi-cally, between pain and multiple chronic disease burden. Certain data trends may have been due to the sample getting older in the later waves, which may represent a limitation in the study. However, a strong case can be made from the prevalence data that pain increases with age, and pain intensity also increases as one ages.
Interestingly, the data showed consistently higher rates of prevalence at moderate levels of pain than in the severe category. The consistently higher prevalence in the category of severe pain for individuals with the heavi-est disease burden would seem to suggheavi-est underreporting of pain inten-sity among seriously ill older adults, who may be either reluctant to report pain, or unable to communicate their experiences of pain due to cognitive impairments.
The prevalence findings are also remarkable regarding the association between pain and number of chronic diseases. The prevalence of pain rose fairly consistently over the 10-year period in proportion to two or more chronic diseases. The findings on the increase in pain intensity associated with multiple chronic diseases are quite staggering, reflecting that with a heavy disease burden of six chronic diseases approximately half of older adults in the sample are experiencing severe pain. The contribution of these findings add to current knowledge of aging experience, which has not yet been well informed by the robust longitudinal data on pain and chronic ill-ness experience.
These findings, and the thematizing of pain as a more visible problem in old age, may have an impact on the mapping of illness and dying trajec-tories of older adults at the population level, especially among frail elders. In very practical terms, the positive association between chronic illness and pain effect interferes with chronically ill older adults’ functioning and ability to perform their usual activities such as household chores. Such functional deficits and impairments among older adults, especially in the frail elderly, need to be accounted for in policy planning.
The data analysis also suggests that pain has strong social correlates in the domain of education. This is consistent with a recent study done by Atlas and Skinner (2010) who reported that low educational attainment is strongly associated with higher rates of reported pain, more disability, and poor health outcomes among older adults. Atlas and Skinner (2010) have suggested that education may actually change the experience of pain over time at the neurobiological level, and further that socioeco-nomic status, social norms, and emotions may play a significant role in both processing and perception. Their findings indicate that education makes a difference in pain over time. Our findings support their conclu-sions using the Health and Retirement Study as well, but looking at data across the five waves.
The pain profile differed among age groups and over time, as well as in relation to number of chronic diseases. Based on inferences about pain and the three-way relationship among chronic disease, education, and age drawn from the longitudinal study data, we conclude from the findings that older adults with higher chronic disease burden and lower educational attainment are at higher risk of increased pain and heightened suffering. The research findings of Olshansky et al. (2012) on longevity would also suggest that this
population would likely have shorter life spans. Interventions that take into account these underlying dynamic relationships may help to reduce the bur-den and suffering of older adults, especially at the end of life.
The demographic data for this study reflect a population that is primar-ily female, White/Caucasian, married and community-dwelling. Generally, females and White/Caucasians reported higher pain rates than males and Black/African Americans, respectively. However, their rates of pain intensity varied between White/Caucasians and Black/African Americans, with Black/ African Americans having lower rates of pain overall but higher rates of pain in the severe category. Married and community-dwelling participants in the study reported lower pain rates than nonmarried and nursing home residents.
These data indicating that frail elderly women—especially women of color—who live in nursing homes and are among the vulnerable subgroups who may be at very high risk of poor health, warrant identifying them as one of several target populations that could benefit from early access to pallia-tive care services. These results also suggest that social support either in the marital relationship, or through living at home or through social networks, may mediate the relationship between pain and chronic illness. Because pal-liative care interventions in principle and in practice share these features of empathic care, social support, and effective communication, this approach may continue to hold the greatest promise for preventing and relieving pain among frail, chronically ill elderly persons at all stages of illness and at the end of life. The unit of care in palliative care has always been the patient and the patient’s family and caregivers. Providing specialized medical care and support to the older adult patient in the context of her/his social ecology includes extending support to the patient’s family and caregiver and remains a key pillar of palliative care and palliative social work.
POLICY IMPLICATIONS
These results have important implications for public health policy. Expanding palliative social work in all health care settings as well as strengthening the generalist-level palliative care workforce, plays an important part in the pre-vention and relief of pain and suffering among chronically ill older adults. The shortage of enough adequately trained geriatric professionals to meet the needs of the chronically ill aging population has been widely acknowl-edged for well over a decade (Kovner, Mezey, & Harrington, 2002). This crisis in the geriatric workforce has only been heightened by the slow develop-ment of the generalist-level palliative care workforce and inadequate training for professionals in core areas of palliative care such as pain management.
Members of the social work profession are well suited to help fill this void in care.
It is in this context that the social work profession must assume prominent leadership roles among the care-related professions. Social work professionals must shape changes in pain and workforce policy to strengthen the caregiving workforce. Policies must focus on providing the sickest and most vulnerable older adults with access to services that will help them attain the highest standards of health and well-being in accordance with human rights principles (Blacker & Christ, 2011; Raymer & Gardia, 2011). Consistent with public health strategies, social work leadership and policy advocacy at the macro level need to coalesce around collaboration with other profession-als and organizations. The public health field must share a common goal of enhancing capacity to deliver palliative care throughout the health systems, from the generalist level to specialized medical care, and in both primary and community-based care settings. The movement toward generalist-level pallia-tive care, as part of the broader public policy goal to develop the health care workforce, will require investment to rebalance medical and social services and to expand social support and planning systems for older adults, espe-cially at the local level (Lynn, 2005). Social workers have a critical role to play in the expansion of palliative social services for older adults, a need that will only increase with the aging of one of the largest generations of Americans. Only with a better understanding of the contributions social workers add to society will policy makers and regulators create programs that expand the profession and encourage more people to pursue training as social workers.
PRACTICE AND EDUCATION
Social work processes that are central to palliative care such as communication, planning, care coordination, and conflict negotiation are crucial to public health as are social work competencies in human development, assessment, treatment, family systems and culturally sensitive care, and pain and symp-tom management (Blacker & Christ, 2011; Gwyther et al., 2005). Social work-ers who receive basic training and demonstrate clinical competency in the fundamental elements of palliative care—such as basic pain and symptom management, advance care planning, and goals of care discussions (Quill & Abernethy, 2013)—should be well-positioned to serve as generalist-level palliative care practitioners. Even without specialist training in palliative care, social workers are well-equipped by virtue of their core training in process and family systems to conduct a comprehensive social assessment. They can engage seriously ill older adults, as well as their family members and care-givers, through process conversations that address their values, preferences, and goals of care including goals for good pain care.
The generalist or primary palliative social work practitioner will also be able to conduct a pain assessment, provide pain education, and inform older adults of their rights to pain and palliative care, engage in treatment
planning, advocate for appropriate levels of care and early palliative care interventions for older adults with pain and chronic illness, seek consulta-tions with pain specialists in more advanced or refractory symptom man-agement (Quill & Abernethy, 2013), provide pharmacologic and medical management as needed, and coordinate care across varied health care set-tings. In addition, social workers provide emotional and social support to seriously ill older adults and their loved ones who may be experiencing trauma. Social work interventions encompass ongoing conversations and communication with older adults about changes in their clinical conditions, social and spiritual life, and experiences of loss associated with illness and dying. Social workers, more than practically any other profession, can help older adults identify what is most meaningful to them in preserving hope and dignity in the face of chronic illness and at the end of life.
Steps to integrate the fundamentals of palliative social work into sys-tems of care to combat persistent pain and chronic illness among older adults, especially frail elders, must become a public health priority. Social workers provide personal, social, and cultural attunement that fosters more humanistic and relational care praxes in serious illness and at the end of life. As key members of interdisciplinary teams, social workers contribute the kind of empathic care necessary to effect radical change in seriously ill older adults’ pain experiences and to influence associated chronic illness trajecto-ries and outcomes. Social workers on interdisciplinary teams play a central role in advocating for strengthened palliative care at all stages of illness, and working across disciplines to assure that the palliative social service needs of older adults receive balanced treatment in interdisciplinary collaborative practice.
FUTURE RESEARCH AGENDA
In shaping a future research agenda, the data on the positive role of community support systems lead us to the possibilities that biopsychosocial and spiritual research may continue to offer. Great strides have been made in neurobiological and psychological research exploring social and spiritual aspects of pain over the last decade as outlined by Lumley et al. (2011), Sulmasy (2002), and others. In particular, the role of emotional, spiritual, and social processes of human development and decision making in chronic ill-ness and pain development and trajectories are ripe for research and inves-tigation. A revised research agenda should include a sharpened focus on the impact of these processes on older adults’ pain care outcomes associated with neighborhood, housing, residential stability, health and pain dispari-ties, and economic and social structures, especially in light of the insights gleaned from the present and other studies of Health and Retirement Study participants’ data on pain. A deeper investigation into the social capital,
networks, support, relationships, and communication abilities, including empathy (Lumley et al., 2011) of chronically ill older adults could hold major implications for providing care more effectively and humanely.
Researchers also need to continue to build on the successes of diverse qualitative research methods, which allow access to the psychological and emotional processes and intentionalities of persons themselves who are liv-ing through pain, sufferliv-ing, and chronic illness (Wertz et al., 2011). As more data for the Medicare and dual eligible population become available, it will become increasingly important to use this data to design qualitative stud-ies of the experience of chronic illness among the most vulnerable older adults from their first person perspective. This type of research will yield insight into the meanings of pain for chronically ill elderly persons and pro-vide stronger foundations for developing palliative care programs for diverse subgroups such as the disabled, the cognitively impaired, veterans, prison inmates, immigrants, and persons with serious mental illness. The experi-ence of seriously ill older adults at the end of life is a particularly fruitful area for investigation in seeking to understand the relationship between pain and chronic illness and how best to relieve pain and suffering at the end of life. This kind of research will help to strengthen the evidence base for the integration of palliative social work and the provision of critical services to older adults much earlier in their interactions with the health systems.
REFERENCES
Allegre, A. (2010). Anticipating and managing common medical challenges encountered at the end of life. In M. Bern-Klug (Ed.), Transforming palliative
care in nursing homes (pp. 107–139). New York, NY: Columbia University Press.
Altilio, T. (2004). Pain and symptom management: An essential role for social work. In J. Berzoff & P. R. Silverman (Eds.), Living with dying: Handbook for
end-of-life practioners (pp. 380–408). New York, NY: Columbia University Press.
Altilio, T., Otis-Green, S., Hedlund, S., & Cohen Finberg, I. (2006). Pain management and palliative care. In S. Gehlert & T. A. Browne (Eds.), Handbook of health
social work (pp. 645–673). New York, NY: John Wiley and Sons.
American Geriatrics Society Panel on Persistent Pain in Older Persons. (2002). The management of persistent pain in older persons. Journal of the American
Geriatrics Society, 50(6), S205–S224.
Atlas, S. J., & Skinner, J. (2010). Education and the prevalence of pain. In D. A. Wise (Ed.), Research findings in the economics of aging (pp. 145–166). Chicago, IL: University of Chicago Press.
Auslander, W., & Freedenthal, S. (2006). Social work and chronic disease. Diabetes, heart disease, and HIV/AIDS. In S. Gehlert, & T. A. Browne (Eds.), Handbook of
health social work (pp. 532–567). New York, NY: John Wiley and Sons.
Baicker, K., Shepard, M., & Skinner, J. (2013). Public financing of the Medicare pro-gram will make its uniform structure increasingly costly to maintain. Health
Affairs, 32(5), 882 –890.
Bern-Klug, M. (2010). Trends in the characteristics of nursing homes and residents. In M. Bern-Klug (Ed.), Transforming palliative care in nursing homes (pp. 84–106). New York, NY: Columbia University Press.
Bern-Klug, M., & Simons, S. (2011). Palliative care in long term care facilities. In T. Altilio & S. Otis-Green (Eds.), Oxford textbook of palliative social work (pp. 103–114). New York, NY: Oxford University Press.
Blacker, S., & Christ, G. H. (2011). Defining social work’s role and leadership con-tributions in palliative care. In T. Altilio & S. Otis-Green (Eds.), Oxford textbook
of palliative social work (pp. 21–30). New York, NY: Oxford University Press.
Cagle, J. G., & Altilio, T. (2011). The social work role in pain and symptom manage-ment. In T. Atilio & S. Otis-Green (Eds.), Oxford textbook of palliative social
work (pp. 271–286). New York, NY: Oxford University Press.
Cassidy, A. (2012, June 13). Care for dual eligibles. Retrieved from http://www. healthaffairs.org/healthpolicybriefs/brief.php?brief_id=70
Chiu, C. J., & Wray, L. A. (2011). Physical disability trajectories in older Americans with and without diabetes: The role of age, gender, race or ethnicity, and edu-cation. Gerontologist, 51(1), 51–63.
Diederichs, C., Berger, K., & Bartels, D. B. (2011). The measurement of multiple chronic diseases: A systematic review on existing multimorbidity indices. The
Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 66(3), 301–311. doi:10.1093/gerona/glq208
Freid, V. M., Bernstein, A. B., & Bush, M. A. (2012). Multiple chronic conditions
among adults age 45 and over: Trends over the past 10 years (NCHS Data Brief
No. 100). Hyattsville, MD: National Center for Health Statistics.
Gardener, D. (2011). Palliative social work with older adults and their families. In T. Atilio & S. Otis-Green (Eds.), Oxford textbook of palliative social work (pp. 397–414). New York, NY: Oxford University Press.
Gaskin, D. J., & Richard, P. (2012). The economic costs of pain in the United States.
Journal of Pain, 13(6), 715–724.
Gold, D. T., & Roberto, K. A. (2000). Correlates and consequences of chronic pain in older adults. Geriatric Nursing, 21(5), 270–273.
Gold, M. R., Jacobson, G. A., & Garfield, R. L. (2012). There is little experience and limited data to support policy making on integrated care for dual eligibles.
Health Affairs, 31(6), 1176–1185.
Goodman, D., Esty, A. R., Fisher, E. S., & Chang, C. H. (2011). Trends and
varia-tion in end-of-life care for Medicare beneficiaries with severe chronic ill-ness. Hanover, NH: The Dartmouth Institute for Health Policy and Clinical
Practice.
Goodman, D, Fisher, E., Wennberg, J. E., Skinner, J. S., Chasan-Taber, S., & Bronner, K. K. (2013). Tracking improvement in the care of chronically ill patients: A
Dartmouth atlas brief on Medicare beneficiaries near the end of life. Hanover,
NH: The Dartmouth Institute for Health Policy and Clinical Practice.
Griffin, D. W., Harmon, D. C., & Kennedy, N. M. (2012). Do patients with chronic low back pain have an altered level and/or pattern of physical activity compared to healthy individuals? A systematic review of the literature. Physiotherapy, 93(1), 13–23. Gwyther, L. P., Altilio, T., Blacker, S., Christ, G., Csikai, E. L., Hooyman, N., & Howe, J.
(2005). Social work competencies in palliative and end-of-life care. Journal of
Social Work in End-of-Life and Palliative Care, 1(1), 87–120.
Health and Retirement Study. (2002–2010). Retrieved from http://hrsonline.isr.umich. edu/index.php?p=avail
Hwang, U., Richardson, L. D., Harris, B., & Morrison, R. S. (2010). The quality of emergency department pain care for older adult patients. Journal of the
American Geriatrics Society, 58, 2122–2128.
Institute of Medicine. (2011). Relieving pain in America: A blueprint for transforming
prevention, care, education and research. Washington, DC: National Academies
Press.
Jakobbson, U., Klevsgard, R., Westergren, A., & Hallberg, I. R. (2003). Old people in pain: A comparative study. Journal of Pain and Symptom Management, 26(1), 625–635.
Jennings, B. J., & Morrissey, M. B. (2011). Healthcare costs in end-of-life and pallia-tive care: A quest for ethical reform. Journal of Social Work in End-of-Life and
Palliative Care, 7(4), 30–37.
Kelley, A. S., McGarry, K., Fahle, S., Marshall, S. M., Du, Q., & Skinner, J. S. (2012). Out-of-pocket spending in the last five years of life. Journal of General Internal
Medicine, 28(2), 304–309.
Kovner, C. T., Mezey, M., & Harrington, C. (2002). Who cares for older adults? Workforce implications of an aging society. Health Affairs, 21(5), 78–89. Lappenschaar, M., Hommersom, A., & Lucas, P. J. F. (2012). Probabilistic causal
mod-els of multimorbidity concepts. AMIA Annual Symposium Proceedings, 2012, 475–484.
Lumley, M. A., Cohen, J. L., Borszcz, G. S., Cano, A., Radcliffe, A. M., Porter, L. S., & Keefe, F. J. (2011). Pain and emotion: A biopsychosocial review of recent research.
Journal of Clinical Psychology, 67(9), 942–968.
Lunney, J. R., Lynn, J., & Hogan, C. (2003). Profiles of older Medicare decedents.
Journal of the American Geriatrics Society, 50, 1108–1112.
Lynn, J. (2005). Living long in fragile health: The new demographics shape end of life care. Hastings Center Special Report, 35(6), S14–S18.
Manchikanti, L., Singh, V., Datta, S., Cohen, S. P., & Hirsch, J. A. (2009). Comprehensive review of epidemiology, scope and impact of spinal pain. Pain Physician, 12, E35–E70.
Meghani, S. H., Polomano, R. C., Tait, R. C., Vallerand, A. H., Anderson, K. O., & Gallagher, R. M. (2012). Advancing a national agenda to eliminate disparities in pain care: Directions for health policy, education, practice, and research. Pain
Medicine, 13, 5–28.
Mezey, M., Dubler, N., Mitty, E., & Brody, A. (2002). What impact do setting and transi-tions have on the quality of the dying process? The Gerontologist, 42(3), 54–67. Morden, N. E., Chang, C. H., Jacobson, J. O., Berke, E. M., Bynum, J. P. W., Murray,
K. M., & Goodman, D. C. (2012). End-of-life care for Medicare beneficiaries with cancer is highly intensive overall and varies widely. Health Affairs, 31(4), 786–796. Morrison, R. S., Dietrich, J., Ladwig, S., Quill, T., Sacco, J., Tangeman, J., & Meier,
D. E. (2011). Palliative care consultation teams cut hospital costs for Medicaid beneficiaries. Health Affairs, 30(3), 454–463.
Morrison, R. S., Penrod, J. D., Cassell, J. B., Caust-Ellenbogen, M., Litke, A., Spragens, I., & Meier, D. E. (2008). Cost savings associated with United States hospital palliative care consultation programs. Archives of Internal Medicine, 168(16), 1784–1790.
Murphy, T. E., Han, L., Allore, H. G., Peduzzi, P. N., Gill, T. M., & Lin, H. (2011). Treatment of death in the analysis of longitudinal studies of gerontological out-comes. The Journals of Gerontology Series A: Biological Sciences and Medical
Sciences, 66(1), 109–114.
Naylor, M. D., Kurtzman, E. T., Grabowski, D. C., Harrington, C., McClellan, M., & Reinhard, S. C. (2012). Unintended consequences of steps to cut readmis-sions and reform payment may threaten care of vulnerable older adults. Health
Affairs, 31(7), 1623–1632.
Olshansky, S. J., Antonucci, T., Berkman, L., Binstock, R. H., Boersch-Supan, A., Cacioppo, J. T., & Rowe, J. (2012). Differences in life expectancy due to race and educational differences are widening, and may not catch up. Health Affairs,
31(8), 1803–1813.
Patient Protection and Affordable Care Act, Pub. L. No. 111–148, 124 Stat. 119 (2010). Retrieved from http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf
Peat, G., Thomas, E., Handy, J., & Croft, P. (2004). Social networks and pain interfer-ence with daily activities in middle and old age. Pain, 112, 397–405.
Quill, T. E., & Abernethy, A. P. (2013). Generalist plus specialist palliative care– Creating a more sustainable model. New England Journal of Medicine, 368(13), 1173–1175.
Raven, M., & Gould, D. A. (2012). Time and again: Frequent users of emergency
department services in New York City. Retrieved from http://www.uhfnyc.org/
publications/880847
Raymer, M., & Gardia, G. (2011). Enhancing professionalism, leadership, and advocacy: A call to arms. In T. Altilio & S. Otis-Green (Eds.), Oxford textbook
of palliative social work (pp. 683–687). New York, NY: Oxford University
Press.
Reinhard, S., Levine, C., & Samis, S. (2012). Home alone: Family caregivers providing
complex chronic care. Washington, DC: AARP Public Policy Institute.
Roberto, K. A. (2001). Chronic pain and intimacy in the relationships of older adults.
Generations, 25(2), 65–69.
Roberto, K. A., & Reynolds, S. G. (2002). Older women’s experiences with chronic pain: Daily challenges and self care practices. Journal of Women and Aging,
14(3–4), 5–23.
Roberto, K. A., Perkins, S. N., & Holland, A. K. (2007). Research on persistent pain in late life: Current topics and challenges. Journal of Women and Aging, 19(3–4), 5–19.
Rodriguez-Mañas, L., Féart, C., Mann, G., Viña, J., Chatterji, S., Chodzko-Zajko, W., & FOD-CC Group. (2013). Searching for an operational definition of frailty: A Delphi method based consensus statement: The Frailty Operative Definition-Consensus Conference Project. The Journals of Gerontology Series A: Biological
Sciences and Medical Sciences, 68(1), 62–67.
Sacco, J., Deravin Carr, D. R., & Viola, D. (2013). The effects of the palliative medicine consultation on the DNR status of African Americans in a safety-net hospital.
American Journal of Hospice & Palliative Medicine, 30(4), 363–369. Retrieved
from http://ajh.sagepub.com/content/30/4/363
Shega, J. W., Andrew, M., Hemmerrich, J., Cagney, K. A., Ersek, M., Weiner, D. K., & Dale, W. (2012). The relationship of pain and cognitive impairment with social