R E S E A R C H M E T H O D O L O G Y
Chinese Version of the Positive and Negative Suicide Ideation:
Instrument Development
Hsiu-Ju Chang, Chia-Chin Lin, Kuei-Ru Chou, Wei-Fen Ma & Chyn-Yng Yang
Accepted for publication 12 February 2009
Correspondence to C.-Y. Yang: e-mail: caring@mail.tmch.org.tw Hsiu-Ju Chang PhD RN Associate Professor
College of Nursing, Taipei Medical University,
and Member,
Psychiatric Research Center, Taipei Medical University Hospital, Taipei, Taiwan Chia-Chin Lin PhD RN
Professor
College of Nursing, Taipei Medical University, Taipei, Taiwan Kuei-Ru Chou PhD RN Professor
College of Nursing, Taipei Medical University,
and Member,
Psychiatric Research Center, Taipei Medical University Hospital, Taipei, Taiwan Wei-Fen Ma PhD RN
Assistant Professor
School of Nursing, China Medical University, Taichung, Taiwan
Chyn-Yng Yang MS RN
Vice Director, Department of Nursing, Taipei Medical University Hospital,
and Doctoral Student,
College of Nursing, Taipei Medical University, Taipei, Taiwan
C H A N G H . - J . , L I N C . - C . , C H O U K . - R . , M A W . - F . & Y A N G C . - Y . ( 2 0 0 9 )
C H A N G H . - J . , L I N C . - C . , C H O U K . - R . , M A W . - F . & Y A N G C . - Y . ( 2 0 0 9 ) Chinese Version of the Positive and Negative Suicide Ideation: Instrument Development. Journal of Advanced Nursing 65(7), 1485–1496
doi: 10.1111/j.1365-2648.2009.05005.x
Abstract
Title. Chinese Version of the Positive and Negative Suicide Ideation: Instrument Development.
Aim. This paper is a report of a study conducted to develop a Chinese version of the Positive and Negative Suicide Ideation Inventory and evaluate its psychometric properties.
Background. Comprehensive assessment of suicidal behaviour in youths should incorporate both protective factors and risk factors.
Methods. We recruited 2341 middle- and high-school students for a longitudinal and prospective study, conducted between 2005 and 2007. To assess predictive validity, a convenience sample of 251 of the 2341 students was recruited 1 year later to follow-up on suicide attempts during the preceding 2 weeks. To evaluate construct validity, a small convenience sample of 94 adolescent inpatients and outpatients was used as a comparison group. Instruments used included the Children’s Depression Inventory, the Self-Control Schedule, and the Cognitive Triad for Children. Results. Cronbach’s a coefficients for the Chinese version of the positive and negative suicide ideation–negative suicide ideation and the Chinese version of the positive and negative suicide ideation–positive ideation were 0Æ94 and 0Æ86 respectively. Satisfactory test–retest reliability was evident. Convergent and divergent validities were demon-strated by statistically significant correlations among subscales and the other instruments used. Construct validity was evidenced by statistically significantly different scores on the subscales among the contrasted groups. Subscale scores in the first-wave study statistically significantly predicted attempted suicide behaviour 1 year later, demon-strating evidence of predictive validity. Factor analysis showed a two-factor structure. Conclusion. The Chinese Version of the Positive and Negative Suicide Ideation Inventory may be a reliable and valid instrument to measure the severity of suicidal ideation in adolescents, subject to further research to test the generalizability of the present findings.
Keywords: Chinese version, instrument development, nursing, positive and negative suicide ideation, reliability, validity
Introduction
Suicide is a major worldwide public mental-health problem. It is the leading cause of death among youths aged 10– 24 years in western countries, and the second leading cause of death among those aged 15–24 years in Taiwan (Depart-ment of Health, Executive Yuan, Taiwan 2005). In Taiwan, suicide has been one of the top 10 causes of death among young people aged 15–24 years since 1991. Despite an overall decline in the suicide rate over the past 20 years in the United States, the rates for youths aged 10–14 and 15– 19 years increased by more than 100% and 6% from 1979 to 1998 respectively (National Youth Violence Prevention Resource Center 2007). Also, the Centers for Disease Control and Prevention noted that from 2003 to 2004, the suicide rate for those aged 10–24 years increased by 8% (National Youth Violence Prevention Resource Center 2007). Thoughts of suicide are not rare among youths, with over 19% reporting serious suicidal ideation in the United States of America (USA) (Gould et al. 2003). Previous studies in the USA and Australia have shown that suicidal ideation was a predictor of or was related to psychopathology, such as mood, anxiety, and substance-use disorders, among adolescents (Cooper et al. 1994, Kessler et al. 1999, Goldney et al. 2003). Prolonged and severe suicidal ideation was found in the UK and France to be related to a high risk of attempted suicide, and adolescents who have attempted suicide are at high risk of subsequently completing suicide (Kerfoot & McHugh 1992, Granboulan et al. 1995).
Background
Although it is widely acknowledged that suicide-related behaviours are closely linked to several risk factors, such as the pathological environment, psychological distress and psychiatric disorders (Hawton & Heeringen 2000), research-ers have noted that suicide ideation may be multidimensional (Perkins & Hartless 2002). For example, individuals at high risk for suicidal ideation may still express a desire to live (Turner et al. 1998). Therefore, an increasing number of researchers have recommended that a comprehensive assess-ment of suicidal behaviour in adolescents and young adults incorporate both protective factors and negative risk factors (Perkins & Hartless 2002, Osman et al. 2003).
Numerous instruments have been developed to assess suicidal ideation among adolescents. For example, the original Suicidal Behaviors Questionnaire (M.M. Linehan & M.E. Addis, University of Washington, Seattle, unpub-lished manuscript) was developed to assess past history of suicide attempts and suicidal thoughts. The Suicide
Probability Scale (Cull & Gill 1982) was designed to assess suicide risk factors for youths under clinical care. Three other instruments, the modified scale for suicidal ideation (Miller et al. 1986), the Beck Scale for Suicide Ideation (Beck & Steer 1991) and the Suicidal Ideation Questionnaire (Reynolds 1987), were likewise designed to assess suicide-related risk factors. Among these instruments used for assessing suicidal ideation, researchers have focused mainly on negative risk factors (Osman et al. 2003). While the Reasons for Living Inventory for Adolescents (Osman et al. 1998) measures adaptive factors, few instruments are designed to measure both protective and risk factors.
Osman et al. (1998) recently designed a 14-item self-report instrument to measure suicidal ideation that incorporates both positive and negative dimensions of risk. This new instrument, the Positive and Negative Suicide Ideation (PANSI) Inventory, was developed to assess the frequency of suicidal ideation among adolescents and adults aged ‡14 years. The PANSI is composed of two subscales: positive ideation (PANSI-PI; six items) and negative suicide ideation (PANSI-NSI; eight items). Respondents are asked to report the frequency of their suicidal ideation over a 2-week timeframe. Each item consists of five self-evaluative state-ments scored on a scale of 1 (indicating none of the time) to 5 (indicating most of the time). Total scores on the subscales can be computed by summing all items. Total scores range from 0 to 30 and from 0 to 40 for the PI and PANSI-NSI respectively. Higher scores represent more positive ideation and negative suicidal ideation respectively.
Studies demonstrating the PANSI’s psychometric proper-ties have been conducted with undergraduate students and adults (Osman et al. 1998), adolescent psychiatric inpatients (Osman et al. 2002) and young adults (Muehlenkamp et al. 2005). Thus far, only one study has shown psychometric properties of the PANSI in a sample of normal adolescents (Osman et al. 2003). This revealed that the internal consis-tency coefficients for the PANSI-PI and PANSI-NSI were 0Æ81 and 0Æ94 respectively. Confirmatory factor analyses (CFAs) supported the two-factor structure, which indicated good evidence of construct validity. Scores on the PANSI-NSI and PANSI-PI differ statistically significantly among psychiatric suicide-risk and high-school suicide-risk subgroups, indicat-ing evidence of criterion validity. Osman et al. (2003) concluded that the PANSI is a valid and reliable instrument for screening for suicidal ideation in research situations and should be used to screen for risk of suicidal ideation, to measure clinical improvement, and to assess the wide range of factors affecting suicide risk in adolescents.
The PANSI has not previously been translated into tradi-tional Chinese, and its psychometric properties have not been
tested with normal Asian adolescents and there is no existing instrument for measuring both positive ideation and negative suicide ideation in Taiwanese adolescent populations.
The study
Aim
The aim of the study was to translate the English version of the PANSI into Chinese (PANSI-C) and evaluated its psychometric properties in a community-based sample of Taiwanese youths.
Design
A longitudinal and prospective design was used to evaluate the reliability and validity of the PANSI-C with a community-based sample of adolescents. We used a procedure proposed by Brislin (1970) to guide the translation of instruments. The purpose of the procedure is to ensure appropriate and equivalent meanings for words and expressions (Hall et al. 2003). The steps are as follows: 1) selection of concise language; 2) use of competent translators familiar with issues related to the study; 3) use of two bilingual translators (one translates from English into Chinese, and the other translates back into English without having seen the first version); and 4) use of a refinement group for both the translation and the back-translation.
Permission for the translation was obtained from Professor Osman, the instrument’s designer.
Participants
Fifteen schools – seven middle schools and eight high schools – were randomly selected from a list of middle and high schools in Taipei city. A convenience sampling method was then used to select two classes in each grade from those schools.
The inclusion criteria were as follows: 1) age of 12–19 years and 2) ability to read, write, and speak Chinese. A sample of 2341 normal community-based adolescents completed the questionnaires. The response rate was 93Æ71%. The instru-ments were administered to a convenience sample of 33 adolescents and were then re-administered to them 1 month later to evaluate test–retest reliability. To assess predictive validity, a convenience sample of 251 students was recruited from the original 2341 to complete the PANSI-C again 1 year later, with one added question asking whether they had attempted suicide during the preceding 2 weeks. A small convenience sample of 94 inpatient and outpatient adolescents
with psychiatric disorders (comprising the clinical group) was recruited to evaluate construct validity. Psychiatric disorders are a major risk factor for youth suicide. Studies have shown that 70–91% of community-based youths who have experi-enced suicidal ideation or attempted suicide have a psychiatric disorder (Fergusson & Lynskey 1995, Gould et al. 1998), such as mood disorders, anxiety, disruptive behaviour or substance use, which have been identified as risk factors (Andrews & Lewinsohn 1992, Lewinsohn et al. 1994, 1995, Reinherz et al. 1995, Gould et al. 1998, Pilowsky et al. 1999).
The Children’s Depression Inventory (CDI) was used to identify a high-depression-risk community group. Kovacs (1981, 1982) suggested that a score of ‡19 can be used to identify a clinical level of depression. Reynolds and Johnston (1994) likewise indicated that a cutoff of 19 is probably adequate, as this score distribution was found among diverse school-based samples of adolescents. In the present study, using the cutoff score of 19, 23Æ4% of adolescents were found to have a clinical level of depressive symptoms, and these students were categorized as at high risk for depression.
Translation, back-translation, and equivalence assessment of the PANSI-C
The English version of the PANSI was initially translated into Chinese by one of the authors, who is bilingual in Chinese and English and experienced in the study topic. A second qualified and blinded bilingual expert back-translated the Chinese version of the PANSI, creating a new English version. A monolingual reviewer on the research team then compared the original and back-translated versions of the PANSI.
To guarantee cultural equivalence, a refinement group of bilingual experts in child and adolescent mental health was formed, including two child and adolescent psychiatrists, two child and adolescent psychiatric nurses, one school psychol-ogist, and one mental-health faculty member. These experts were asked to rate the relevance of the content independently using a content validity index (CVI). They were asked to rate each item on the PANSI-C based on relevance and semantic equivalence using the following 4-point Likert scale: 1 = not relevant (not appropriate), 2 = somewhat relevant (some-what appropriate), 3 = relevant (quite appropriate), 4 = very relevant (very appropriate). The CVI was then computed based on the percentage of total items rated by the experts as either 3 or 4. According to Norwood (2000), a CVI rating exceeding 0Æ80 can be considered to show good content validity. All items in the PANSI-C were rated by the panel experts as having a CVI >0Æ90. Semantic equivalence was also found to have appropriateness above 0Æ90. In response to the experts’ suggestions, ten minor semantic errors were
corrected and one sentence item was reworded. For the final version, the CVIs for relevance and semantic equivalence both exceeded 0Æ95.
The PANSI-C was then pilot-tested with a small sample of ten school-aged adolescents recruited from middle and high schools, with five additional adolescents recruited from a psychiatric outpatient center. Most of the adolescents con-firmed that all items on the PANSI-C were easy to read and understand, and the form took approximately 5 minutes to complete.
Data collection
Data were collected between January 2005 and July 2007. Instruments were distributed to all eligible students whose parents granted written informed consent. Students were asked to record their student ID numbers on the tests in order to link the PANSI-C scores to suicide attempts 1 year later. On completion of the questionnaires, students were given a small gift.
Children’s Depression Inventory
The CDI (Kovacs 1981) is a commonly-used self-report questionnaire designed for children aged 7–17 to measure the presence and severity of depressive symptoms, including cognitive, affective, and behavioural symptoms, during the preceding 2 weeks. One study showed that Cronbach’s a coefficient for the Chinese version was 0Æ89 (Chang et al. 2007). In our study, Cronbach’s a coefficient was 0Æ89. Sta-tistically significant correlations with suicidal ideation and the cognitive triad demonstrated evidence of construct validity (Chang et al. 2007).
Self-control schedule
The self-report self-control schedule (SCS), which assesses individual tendencies to use self-control skills to solve behavioural problems, was used to evaluate adolescents’ learned resourcefulness (Rosenbaum 1980). High scores on the SCS indicate greater resourcefulness. Studies have demonstrated satisfactory reliability and validity for this scale (Rosenbaum 1980, 1990). A recent study showed that Cronbach’s a coefficient for the scale was 0Æ83 (Zauszniewski et al. 2002); it was 0Æ77 in our study using the Chinese ver-sion. Statistically significant correlations between depressive symptoms and psychosocial attitudes indicated the construct validity of the measure (Zauszniewski 1997).
Cognitive triad for children
The 36-item Cognitive Triad for Children (CTI-C; Kaslow et al. 1992) is used to measure an adolescent’s view of self,
the world and the future. Higher scores indicate more posi-tive thought patterns. One study showed that the internal consistency coefficient for the Chinese version was 0Æ89 (Chang et al. 2007). Statistically significant correlations with depressive symptoms (r = 0Æ69) and learned resourcefulness (r = 0Æ42) provided evidence of construct validity (Chang et al. 2007). In our study, the Cronbach’s a coefficient for the PANSI-C was 0Æ89. Statistically significant correlations with depressive symptoms (r = 0Æ69) and learned resourcefulness (r = 0Æ42) demonstrated evidence of construct validity. All correlations were statistically significant at the P < 0Æ01 level.
Ethical considerations
The appropriate institutional review board approved the study. Students and their parents were informed that partic-ipation was voluntary, results would be reported only in aggregate, and that there would be no consequences for refusing to participate. Students and their parents were also assured that the study responses and data management would be kept confidential.
Data analysis SPSS/PC
SPSS/PC for Windows version 15.0 and AMOSAMOS version 7.0
software were used for the statistical analyses. Several methods were used to evaluate the PANSI’s reliability and validity. Reliability was evaluated with Cronbach a’s coeffi-cients and test–retest reliability. Test–retest reliability was measured with the intraclass correlation coefficient (ICC). An ICC of ‡0Æ70 was considered acceptable (Scientific Advisory Committee of the Medical Outcomes Trust 2002).
Exploratory factor analysis (EFA) was used to examine the factor structures for the instrument. The suitability of the data for the factor analysis was evaluated using a correlation matrix and the Kaiser–Meyer Oklin (KMO) value. CFA was then used to confirm the factor structures obtained from the EFA to support the evidence of construct validity.
The overall fit of measurement models to research data can be tested using several alternative statistics. One is the chi-square goodness-of-fit statistic, which has a low, non-statistically significant value when the model fit is good. A value of SB-v2/d.f. (chi-square divided by its degrees of freedom) of <2 indicates an acceptable model. A variety of non-chi-square goodness-of-fit indices were also used: the Comparative Fit Index (CFI), Normed Fit Index (NFI), Goodness-of-Fit Index (GFI), root-mean-squared residual (RMR) and root-mean-square error of approximation (RMSEA). The CFI, GFI, and NFI should be >0Æ90 for an
acceptable fit. The fit is acceptable if the RMSEA is <0Æ08. The smaller the RMR, the better the model fit. The RMR is 0 when the model fit is perfect, and the acceptability cutoff is £0Æ05.
Convergent validity was evaluated by the statistically significant positive relationships among the total scores on the subscales, CDI, CTI-C and SCS. Divergent validity was also assessed by the statistically significant negative relation-ships among the total scores on the subscales, CDI, CTI-C and SCS. An independent-sample t-test was used to compare scores on the subscales between community and clinical samples and between the high-depression-risk and low-depression-risk groups. Logistic regression analysis was used to determine whether an adolescent’s positive ideation and negative suicide ideation in the first year predict attempted-suicide behaviour 1 year later, to establish predictive validity. A non-statistically significant P value on the Hosmer and Lemeshow test was used to indicate that a model prediction is not statistically significantly different from observed values, which is a well-fitting model. A statistically significant P value on the Omnibus tests was used to indicate that the model with the predictor is statistically significantly different from the model with the intercept only. In addition, receiver operating characteristic analyses were performed to identify cutoff values for evaluating the protective and risk ideation. Mean cutoff values were determined for the purpose of comparison with the findings of Osman et al. (2003), although in the study we specifically proposed total cutoff scores for the purpose of wider use in research and practice.
Results
Demographics
The sample of 2341 adolescents included 1240 middle-school students (53Æ0%) and 1101 high-school students (47Æ0%) with a mean age of 15Æ16 (SDSD= 1Æ58) years. Gender was
represented equally, with 48% boys and 52% girls. The majority of the adolescents were from intact families (n = 1746, 74Æ6%). Only the scores on the negative ideation subscale differed between boys and girls, with girls reporting higher scores (Table 1).
Descriptive statistics and intercorrelations among the study variables
Correlations were used to examine relationships among the variables. The descriptive statistics of the study variables, bivariate correlation matrix, and internal consistency esti-mates (Cronbach a) of the instruments are given in Table 2.
Statistically significant correlations were present among the major study variables. Positive ideation was negatively related to negative suicide ideation (r = 0Æ32) and depres-sive symptoms (r = 0Æ52) and positively related to the cognitive triad (r = 0Æ65) and learned resourcefulness (r = 0Æ46). Negative suicidal ideation was negatively related to the cognitive triad (r = 0Æ52) and learned resourcefulness (r = 0Æ30) and positively related to depressive symptoms (r = 0Æ61). The cognitive triad was positively related to learned resourcefulness (r = 0Æ55) and negatively related to depressive symptoms (r = 0Æ77). Depressive symptoms were negatively related to learned resourcefulness (r = 0Æ47). All correlations were statistically significant at the P < 0Æ01 level.
The results indicated that adolescents with high levels of positive ideation had more positive cognitive triads and resourcefulness, as well as less negative suicidal ideation and fewer depressive symptoms. In contrast, those with more negative suicidal ideation had less positive cognitive triads and resourcefulness, as well as higher levels of depressive symptoms. Those with more positive cognitive triads had more resourcefulness and lower levels of depressive symp-toms. Those with higher levels of depressive symptoms showed less resourcefulness.
Reliability estimate
Internal consistency
In this study, the Cronbach’s a coefficients were 0Æ86 and 0Æ94 for the total scores on the PANSI-PI and PANSI-NSI, respectively, indicating adequate internal consistency based on the suggested criterion level for a coefficient’s a of 0Æ70 or above (Nunnally & Bernstein 1994). The Cronbach’s a-if-item-deleted ranged from 0Æ82 to 0Æ86 and from 0Æ93 to 0Æ94
Table 1 Mean difference in the PANSI-C subscales between boys (n = 1119) and girls (n = 1222) Mean SDSD t Value PANSI-PI Boy 19Æ39 5Æ57 1Æ18 Girl 19Æ65 4Æ94 PANSI-NSI Boy 11Æ59 6Æ02 2Æ72** Girl 12Æ28 6Æ33
PANSI-C, the Chinese Version of the Positive and Negative Suicide Ideation Inventory; PANSI-PI, the positive and negative suicide ide-ation positive ideide-ation; PANSI-NSI, the positive and negative suicide ideation-negative suicide ideation.
for the PANSI-PI and PANSI-NSI, respectively, indicating that no items were unreliable.
Item-total and inter-item correlations
Corrected item-total correlations ranged from 0Æ72 to 0Æ83 and from 0Æ53 to 0Æ73 for the PANSI-NSI and PANSI-PI, respectively, indicating adequate homogeneity of items. Inter-item correlations ranged from 0Æ57 to 0Æ75 and from 0Æ35 to 0Æ66 for the PANSI-NSI and PANSI-PI respectively; these were below 0Æ80, indicating lack of multicollinearity (Tabachnick & Fidell 2007).
Test–retest reliability
Intraclass correlation coefficient coefficients were 0Æ82 and 0Æ70 for the total scores on the PANSI-PI and PANSI-NSI, respectively, indicating acceptable stability over a 4-week period. All correlations were statistically significant at the P < 0Æ05 level.
Validity estimate
Construct validities
Convergent and divergent validities were demonstrated by relationships between the subscales and the conceptually-related constructs. It is widely accepted that depression con-tributes to the development of suicidal behaviour (Dieserud et al. 2001). In addition, the cognitive theory of suicide (Alford & Beck 1997) assumes that cognition is the central element of suicidal behaviour. Suicidal individuals tend to have a negative cognitive triad. In an empirical study (Chang et al. 2007) the cognitive triad was negatively related to and predicted suicidal ideation. Learned resourcefulness theory asserts that resourcefulness is a learned set of cognitive– behavioural self-control skills that can increase one’s capa-bility for coping with life events (Rosenbaum 1990). Rosen-baum (1998) noted that individuals who have a high level of resourcefulness can maintain healthy behaviours. Lack of
resourcefulness has been shown to play a major role in the etiology of depressive symptoms (Warheit 1979). No empir-ical study has revealed a relationship between resourcefulness and suicidal ideation. Because depression is conceptually related to suicide, we assumed that resourcefulness was also conceptually related to suicidal ideation.
Evidence of convergent validity was demonstrated by statistically significant and positive correlations between total scores on the PANSI-NSI and CDI (r = 0Æ61), the PANSI-PI and CTI-C (r = 0Æ65), and the PANSI-PI and SCS (r = 0Æ46). Evidence of divergent validity was demonstrated by statisti-cally significant and negative correlations between the total scores on the PANSI-PI and CDI (r = 0Æ52), the PANSI-NSI and CTI-C (r = 0Æ52), and the PANSI-NSI and SCS (r = 0Æ30). All correlations were statistically significant at the P < 0Æ01 level (Table 2).
Contrasting group comparisons were also used to support the construct validity of the subscales. The independent-sample t-test revealed that the total scores on the PANSI-NSI in the clinical sample were statistically significantly higher than those in the community sample (P < 0Æ01) (Table 3). The mean total score for the PANSI-PI in the community sample was statistically significantly higher than that in the clinical sample (P < 0Æ01). Furthermore, the mean total scores for the PANSI-NSI and PANSI-PI subscales differed statistically significantly between the community high-depres-sion-risk and community low-depression-risk groups (P < 0Æ001). The results consistently revealed that the PANSI-C’s subscales discriminated adequately between psy-chiatric and community groups, as well as between depressed and normal community groups.
Construct validity was examined further using both EFA and CFA, and all item-total coefficients ranged from 0Æ42 to 0Æ71. None of the 14 items was considered redundant. The KMO value was 0Æ93, which is higher than the recommended value of 0Æ60, and Barlett’s Test of Sphericity reached statistical significance, supporting the
Table 2 Descriptive statistics and intercorrelations for the study variables
Variable 1 2 3 4 5 Mean (SDSD) Actual range Possible range Alpha 1. PANSI-PI 1Æ00 19Æ52 (5Æ33) 6–30 0–30 0Æ86 2. PANSI-NSI 0Æ32** 1Æ00 11Æ92 (6Æ10) 8–40 0–40 0Æ94 3. CTI-C 0Æ65** 0Æ52** 1Æ00 46Æ02 (10Æ83) 7–70 0–72 0Æ89 4. CDI 0Æ52** 0Æ61** 0Æ77** 1Æ00 13Æ91 (7Æ77) 0–53 0–54 0Æ89 5. SCS 0Æ46** 0Æ30** 0Æ55** 0Æ47** 1Æ00 101Æ36 (19Æ10) 9–159 0–216 0Æ77
PANSI-PI, the positive and negative suicide ideation positive ideation; PANSI-NSI, the positive and negative suicide ideation-negative suicide ideation; CTI-C, the Cognitive Triad for Children Inventory; CDI, the Children’s Depression Inventory; SCS, the self-control schedule. **P < 0Æ01.
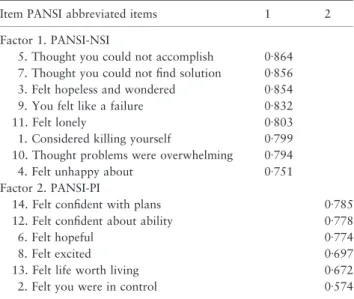
factorability of the correlation matrix. Consistent with the findings of Osman et al. (2003), a two-factor structure was found based on the EFA. The principal axis factoring analysis showed the presence of two components with eigenvalues exceeding 1, explaining 66Æ37% of the variance in the scale. Premix with Kaiser Normalization rotation was performed, and the rotated solution showed the presence of a simple structure (Table 4). All eight negative items were loaded on the PANSI-NSI. All six positive items were loaded on the PANSI-PI. Factor 1 (PANSI-NSI) was statistically significantly related to factor 2 (PANSI-PI) (r = 0Æ32, P < 0Æ001).
Confirmatory factor analyse was then conducted usingSPSSSPSS
version 15.0 withAMOSAMOSversion 7.0 to confirm the two-factor
structure obtained by the EFA. The goodness-of-fit indices for the two competing models were computed. Model one (M1) was a one-factor model that hypothesized that all 14 items were loaded on a single factor of suicidal ideation. Model two (M2) was a two-factor model that was obtained from the EFA solution in this study. The results indicated that the factor oblique model had the best fit. The CFA using the two-factor model yielded the following results: SB-v2= 1191Æ71, d.f. = 76, P < 0Æ001, SB-v2/d.f. = 15Æ68, CFI = 0Æ950, NFI = 0Æ947, GFI = 0Æ933, RMSEA = 0Æ078 and RMR = 0Æ052 (Table 5). The analysis showed that the SB-v2value was large and statistically significant, and the ratio of SB-v2/
d.f. was >0Æ2. According to Schumacker and Lomax (1996), a statistically significant v2-value indicates the probability
that the difference between the observed and estimated matrices is because of sampling variation, while a non-statistically significant v2-value indicates that the observed
and estimated matrices do not differ statistically significantly. In the CFA, a non-statistically significant v2-value
demon-strates that the data fit the model. Uncertainty will always exist, however, because other models may also fit the data (Schumacker & Lomax 1996). The v2-test is very sensitive to
sample size. As the sample size increases (generally >200), the v2-test is likely to indicate a statistically significant
probability level, while as the sample size decreases (generally <100), the v2-test is likely to indicate a non-statistically
significant probability level (Schumacker & Lomax 1996). Also, one of the shortcomings of the v2-test is that it is very
sensitive to departures from multivariate normality of the observed variables (Schumacker & Lomax 1996). We found a statistically significant v2-value and a high ratio of SB-v2/
d.f., which might have been as a result of the large sample size used. The goodness-of-fit indices for the CFI, NFI, GFI, RMSEA and RMR were all close to the cutoff values for an acceptable fit, indicating that the two-factor model was acceptable.
Table 3 Mean differences in the PANSI-C subscales between the community and clinical samples and between the community depression high-risk and low-high-risk group
Community sample Clinical sample
t Value Community depression-high-risk group (CDI 3 19) Community depression-low-risk group (CDI < 19) t Value
Mean SDSD Mean SDSD Mean SDSD Mean SDSD
PANSI-NSI 11Æ92 6Æ10 15Æ12 9Æ20 3Æ40** 17Æ81 8Æ13 10Æ15 3Æ87 20Æ76***
PANSI-PI 19Æ52 5Æ33 17Æ58 5Æ47 3Æ85*** 15Æ45 4Æ63 20Æ75 4Æ90 22Æ00***
PANSI-C, the Chinese Version of the Positive and Negative Suicide Ideation Inventory; PANSI-NSI, the positive and negative suicide ideation-negative suicide ideation; PANSI-PI, the positive and ideation-negative suicide ideation positive ideation; CDI, the Children’s Depression Inventory. ***P < 0Æ001.
Table 4 Exploratory factor analysis of the two-factor model
Item PANSI abbreviated items 1 2
Factor 1. PANSI-NSI
5. Thought you could not accomplish 0Æ864
7. Thought you could not find solution 0Æ856
3. Felt hopeless and wondered 0Æ854
9. You felt like a failure 0Æ832
11. Felt lonely 0Æ803
1. Considered killing yourself 0Æ799
10. Thought problems were overwhelming 0Æ794
4. Felt unhappy about 0Æ751
Factor 2. PANSI-PI
14. Felt confident with plans 0Æ785
12. Felt confident about ability 0Æ778
6. Felt hopeful 0Æ774
8. Felt excited 0Æ697
13. Felt life worth living 0Æ672
2. Felt you were in control 0Æ574
PANSI, the Positive and Negative Suicide Ideation Inventory; PANSI-NSI, the positive and negative suicide ideation negative suicide ide-ation; PANSI-PI, the positive and negative suicide ideation positive ideation.
Predictive validity
One year after the first-wave study, a convenience sample of 251 middle- and high-school students from the first-wave study was selected to complete the PANSI-C instrument, with one categorical question added asking if they had attempted suicide during the preceding 2 weeks. Twenty-six of the 251 students (10Æ4%) had attempted suicide. Logistic regression analysis showed that the total score on the PANSI-NSI in the first-wave study statistically significantly predicted the at-tempted-suicide behaviour after 1 year (coefficient = 0Æ095,
SE
SE= 0Æ022, Wald = 18Æ93, P < 0Æ001; OR = 1Æ10, 95%
CI = 1Æ05–1Æ15). The overall classification rate was good, at 89Æ4%. The total score of the PANSI-PI in the first-wave study also statistically significantly predicted the attempted-suicide behaviour after 1 year (coefficient = 0Æ084,
SE
SE= 0Æ035, Wald = 5Æ74, P < 0Æ05; OR = 0Æ92, 95%
CI = 0Æ86–0Æ99). At 89Æ9%, the overall classification rate was good. Omnibus tests showed that the chi-square values for the models with PANSI-PI and PANSI-NSI as predictors were 5Æ94 (P < 0Æ05) and 18Æ24 (P < 0Æ001). Hosmer and Lemeshow test revealed that the chi-square for the models with PANSI-PI and PANSI-NSI as predictors were 5Æ75 (P > 0Æ05) and 7Æ47 (P > 0Æ05). Both models were appro-priate.
Receiver operating characteristic curve analysis
Receiver operating characteristic analyses were used to determine cutoff points of the PANSI-NSI and PANSI-PI subscales for identifying the necessity for further assessing suicidal ideation. The sample of 251community-based ado-lescents was used to identify specific cutoff scores for the subscales of the PANSI-C. As shown in Table 6, the mean cutoff scores for the PANSI-NSI and PANSI-PI were 2Æ38 and 2Æ75 respectively. The total cutoff scores for the PANSI-NSI and PANSI-PI were 19 and 16Æ5 respectively.
Discussion
The primary aim of this study was to explore the reliability and validity of the PANSI-C. In line with a previous study using a normal community-based adolescent sample (Osman et al. 2003), we found that the PANSI-C may be a reliable and valid instrument to measure the severity of suicidal ideation in adolescents. The generalizability of this study may be limited by the recruitment of adolescents from northern and urban areas only.
We found that the total score on the PANSI-PI did not differ statistically significantly between boys and girls. Although scores on the PANSI-NSI did differ statistically
Table 5 Goodness-of-fit indices
Model SB-x2 d.f. P value SB-x2/d.f. CFI NFI GFI RMSEA RMR
Null Model 22439Æ82 91 <0Æ001 246Æ59 – – 0Æ268 0Æ317 0Æ423
One-factor 6015Æ33 77 <0Æ001 78Æ1 0Æ734 0Æ732 0Æ649 0Æ178 0Æ212
Two factor oblique
1191Æ71 76 <0Æ001 15Æ68 0Æ950 0Æ947 0Æ933 0Æ078 0Æ052
SB-v2, Satorra–Bentler-v2; d.f., degrees of freedom; CFI, Comparative Fit Index; NFI, Normed Fit Index; GFI, Goodness-of-Fit Index; RMSEA,
root-mean-square error of approximation; RMR, root-mean-squared residual.
Table 6 A comparison of the Cutoff Score between this Study and Osman et al.’s study
Chang et al. (2007) Osman et al. (2003)
Cutoff Score AUC Sensitivity (%) Specificity (%) Cutoff Score AUC Sensitivity (%) Specificity (%)
Mean score PANSI-NSI 2Æ38 85Æ1*** 76Æ9 86Æ9 1Æ13 88Æ7 89Æ7 79Æ8 PANSI-PI 2Æ75 62Æ3* 53Æ8 69Æ8 3Æ33 84Æ6 75Æ9 81Æ4 Total score PANSI-NSI 19 85Æ1*** 76Æ0 87Æ5 PANSI-PI 16Æ5 62Æ7* 53Æ8 70
AUC, the area under the curve; PANSI-NSI, the positive and negative suicide ideation negative suicide ideation; PANSI-PI, the positive and negative suicide ideation-positive ideation.
significantly between boys and girls, this difference was approximately 0Æ7, which is small relative to the large sample size. Because with large samples any trivial difference can reach statistical significance, we cannot conclude that suicidal ideation differs by gender. This result is consistent with previous similar studies (Osman et al. 1998, 2003).
Consistent with Osman et al. (2003), the Cronbach’s a coefficients for the PANSI-NSI and PANSI-PI in this study were satisfactory. Other studies testing the PANSI instru-ments in young adults and adolescent psychiatric inpatients also revealed similarly internally consistent coefficients (Os-man et al. 2002, Muehlenkamp et al. 2005). We used a small convenience sample of adolescents to evaluate the test–retest reliability. The results revealed acceptable ICC coefficients for the PANSI-PI and PANSI-NSI, offering additional evi-dence of the reliability of the PANSI-C tested in normal adolescent samples.
Various forms of evidence of construct validity, including convergent and divergent validities, contrasted group com-parisons and factor analysis, were evaluated and approved.
Results for convergent validity revealed that community adolescents with higher levels of negative suicidal ideation had higher levels of depressive symptoms. Adolescents who had higher levels of positive ideation had more strongly positive cognitive triad and learned resourcefulness. Results for divergent validity demonstrated that adolescents with higher levels of positive ideation had lower levels of depressive symptoms, while those with higher levels of negative suicidal ideation had less positive cognitive triad and learned resourcefulness. Results for construct validity showed that adolescents under clinical care and those in a community high-depression-risk group reported statistically significantly higher levels of negative suicidal ideation, whereas the community adolescents and those in a community low-depression-risk group reported statistically significantly higher scores for positive ideation. The results suggested that multi-component school-based suicide-prevention programmes should incorporate strategies for enhancing students’ positive desire to live, in addition to decreasing their negative ideation about suicide. For example, curricula could be developed that address the cognitive factors in developing positive belief systems about life and the potential protective factors such as religion, responsibility to family and friendship.
Results from the EFA suggested that all factor loadings strongly and cleanly loaded on to the two recommended factors. In line with Osman et al. (2003), the CFAs further confirmed the two-factor model, offering accumulated empirical evidence of construct validity. This unique study used longitudinal data to explore the predictive validity of the PANSI-C. Logistic regression analyses showed that the
PANSI-NSI and PANSI-PI administered in the first-wave study statistically significantly predicted attempted-suicide behaviour 1 year later. The results revealed that decreased positive ideation and increased negative suicidal ideation contributed statistically significantly to subsequent at-tempted suicide, demonstrating adequate evidence of pre-dictive validity. We found that 10Æ4% of adolescents who reported suicidal ideation had subsequently attempted suicide after 1 year. To the best of our knowledge, there has been no prior longitudinal follow-up study in Taiwan evaluating the prevalence of subsequent attempted suicide for adolescents with suicidal ideation. However, De Wilde and Kienhorst (1998) reported that suicidal ideation during the preceding month increased the risk of a suicide attempt by 3Æ3-fold. In Taiwan, a cross-sectional study has shown that 5Æ2% of the middle and high school students reported having suicide attempts (Y.C. Cheng, China Medical University, Taichung, unpublished Master’s thesis). One national survey study found that 7Æ24% of students in a middle school reported having attempted suicide during the preceding year (Bureau of Health Promotion, Department of Health, 2008). Compared with the relatively low prevalence of attempted suicide found in cross-sectional studies, ado-lescent students in our study with suicidal ideation indeed had higher probability of reporting subsequent suicide attempts.
Receiver operating characteristic curve analyses showed that the cutoff mean values for the PANSI-NSI and PANSI-PI were 2Æ38 and 2Æ75, while Osman et al. (2003) found that the cutoff mean values for these were 1Æ13 and 3Æ33 respectively. Thus, our study had a higher mean cutoff value for the PANSI-NSI and a lower mean cutoff value for the PANSI-PI compared with the findings of Osman et al. Although our results suggested that a higher mean score for the PANSI-NSI and a lower mean score for the PANSI-PI may be needed for assessing suicidal ideation among Taiwanese adolescents, the results should be interpreted cautiously to account for cultural differences in attitudes toward the expression of negative emotions. Chinese culture tends to lead people to hide negative emotions, partly to avoid the social stigma of psychiatric disease. Especially in adolescent cohorts, aware-ness of suicidal ideation may be complicated, with dramatic psycho-physiological and social changes. Consequently, ado-lescents may report less suicidal ideation than they actually experience, which could lead to a higher mean cutoff score on the PANSI-NSI. Another reason for caution in interpreting the results is the small sample size (n = 251) used for determining cutoff values. Future studies should be con-ducted using larger samples in order to validate the results of the present study.
Conclusion
Future researchers should use more heterogeneous samples, including nationwide and psychiatric samples, for compari-son with the results obtained in the present study.
One of the major responsibilities of school nurses is to provide assessment of health conditions and direct health care to students. School nurses in Taiwan can use this reliable and valid instrument along with other instruments for compre-hensive assessment of possible risk and protective factors for suicide behaviours. Further intervention can then be designed to integrate with courses aimed to facilitate students’ positive belief systems and other protective factors against suicide behaviours. The idea of assessing both protective factors and
negative suicidal ideation as well as providing comprehensive strategies for preventing and intervening in suicide behav-iours should be incorporated into the nursing curriculum in order to increase nursing students’ ability to recognize and prevent suicidal behaviour.
Acknowledgements
We would like to thank the National Science Council and Taipei Medical University for providing financial support, along with all of the students who participated in this study.
Funding
Funding for the study was provided by the National Science Council (NSC 93-2314-B-038-052) (NSC 94-2314-B-038-054), and the Taipei Medical University (94TMU-TMUH-15).
Conflict of interest
None declared.
Author contributions
CHJ, LCC, CKR and YCY were responsible for the study conception and design CHJ, CKR and MWF performed the data collection CHJ performed the data analysis. CHJ, MWF and YCY were responsible for the drafting of the manuscript. CHJ and YCY made critical revisions to the paper for important intellectual content. CHJ provided statistical expertise. CHJ, LCC, MWF and YCY obtained funding CHJ, LCC, CKR, MWF and YCY provided administrative, technical or material support. CHJ, LCC, CKR and YCY supervised the study.
References
Alford B.A. & Beck A.T. (1997) The Integrative Power of Cognitive Therapy. Guilford Press, New York.
Andrews J.A. & Lewinsohn P.M. (1992) Suicidal attempts among older adolescents: prevalence and co-occurrence with psychiatric disorders. Journal of the American Academy of Child and Adolescent Psychiatry 31, 655–662.
Beck A.T. & Steer R.A. (1991) Manual for Beck Scale for Suicide Ideation. Psychological Corporation, San Antonio, TX.
Brislin R.W. (1970) Back-translation for cross-cultural research. Journal of Cross-Cultural Psychology 1, 185–216.
Bureau of Health Promotion, Department of Health (2008) National Investigation. Retrieved from http://olap.bhp.doh.gov.tw/search/ List Health1.aspx?menu=1&mode=3&year=95&sel=0 on 14 December 2008.
What is already known about this topic
• The Positive and Negative Suicide Ideation (PANSI) Inventory has been shown to possess satisfactory reli-ability and validity in western countries.
• Cronbach’s a coefficients for normal adolescents have been reported to be 0Æ94 and 0Æ81 for the PANSI-NSI and PANSI-PI respectively.
• Construct criterion validity have also been demonstrated in previous studies.
What this paper adds
• The Chinese version of the Positive and Negative Suicide Ideation Inventory (PANSI-C) was found to have satis-factory reliability and validity in an Asian country. • Cronbach’s alphas showed that the Chinese version had
satisfactory levels of reliability.
• Logistic regression analyses showed that decreased positive ideation and increased negative suicidal ideation contributed statistically significantly to subsequent attempted suicide, demonstrating adequate evidence of predictive validity.
Implications for practice and/or policy
• The PANSI-C may be a reliable and valid instrument to measure the severity of suicidal ideation in adolescents. • The idea of assessing both protective factors and nega-tive suicidal ideation, as well as providing comprehen-sive strategies for preventing and intervening in suicide behaviours, should be incorporated into the nursing curriculum in order to increase nursing students’ ability to recognize and prevent suicidal behaviour.
Chang H.J., Lin M.F. & Lin K.C. (2007) The mediating and mod-erating roles of the cognitive triad on adolescent suicidal ideation. Nursing Research 56(4), 252–259.
Cooper P.L., Crum R.M. & Ford D.E. (1994) Identifying suicidal ideation in general medical patients. JAMA: The Journal of the American Medical Association 272, 1757–1762.
Cull J.G. & Gill W.S. (1982) Suicide Probability Scale. Western Psychological Services, Los Angeles, CA.
De Wilde E.J. & Kienhorst C.W.M. (1998) Self-Reported Suicidal Thoughts as Predictor of Suicide Attempts in Adolescents with Depressed Mood. Paper presented at the third conference of Psychology and Health, Kerkrade.
Department of Health, Executive Yuan, Taiwan (2005) Taiwan Area Main Causes of Death. Retrieved from http://www.doh.gov.tw/ Statistic/index.htm on 27 August 2006.
Dieserud G., Røysamb E., Ekeberg O. & Kraft P. (2001) Toward an integrative model of suicide attempt: a cognitive psychologi-cal approach. Suicide and Life-threatening Behavior 31(2), 153– 165.
Fergusson D.M. & Lynskey M.T. (1995) Suicide attempts and suicidal ideation in a birth cohort of 16-year-old New Zealanders. Journal of the American Academy of Child and Adolescent Psychiatry 34, 1308–1317.
Goldney R.D., Grande E.D., Fisher L.J. & Wilson D. (2003) Popu-lation attributable risk of major or suicidal ideation in a random and representative community sample. Journal of Affective Disorders 74, 267–272.
Gould M.S., King R., Greenwald S., Fisher P., Schwab-Stone M., Kramer R., Flisher A. J., Goodman S., Canino G. & Shaffer D. (1998) Psychopathology associated with suicidal ideation and at-tempts among children and adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 37, 915–923. Gould M.S., Greenberg T., Velting D. & Shaffer D. (2003) Youth
suicide risk and preventive interventions: a review of the past 10 years. Journal of the American Academy of Child and Adoles-cent Psychiatry 42(4), 386–405.
Granboulan V., Rabain D. & Basquin M. (1995) The outcome of adolescent suicide attempts. Acta Psychiatrica Scandinavica 91, 265–270.
Hall E.O.C., Wilson M.E. & Frankenfield J.A. (2003) Translation and restandardization of an instrument: The Early Infant Tem-perament Questionnaire. Journal of Advanced Nursing 42(2), 159–168.
Hawton K. & Heeringen K.V. (2000) The International Handbook of Suicide and Attempted Suicide. Wiley, New York.
Kaslow N., Stark K., Printz B., Livingston R. & Tsai Y. (1992) Cognitive Triad Inventory for children: development and rela-tionship to depression and anxiety. Journal of Clinical Child and Adolescent Psychology 21, 339–347.
Kerfoot M. & McHugh B. (1992) The outcome of childhood suicidal behaviour. Acta Paedopsychiatrica 55, 141–145.
Kessler R.C., Borges G. & Walters E.E. (1999) Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Archives of General Psychiatry 56(7), 617–626.
Kovacs M. (1981) Rating scales to assess depression in school-aged children. Acta Paedopsychiatrica 46, 305–315.
Kovacs M. (1982) Prediction of suicidal behaviors. Bibliotheca Psy-chiatrica 162, 61–76.
Lewinsohn P.M., Rohde P. & Seeley J.R. (1994) Psychosocial risk factors for future adolescent suicide attempts. Journal of Con-sulting and Clinical Psychology 62, 297–305.
Lewinsohn P.M., Rohde P. & Seeley J.R. (1995) Adolescent psychopathology, III: the clinical consequences of comorbidity. Journal of the American Academy of Child and Adolescent Psychiatry 34, 510–519.
Miller I., Norman W., Bishop S. & Dow M. (1986) The modified scale for suicidal ideation: reliability and validity. Journal of Consulting and Clinical Psychology 54, 724–725.
Muehlenkamp J.J., Gutierrez P.M., Osman A. & Barrios F.X. (2005) Validation of the Positive and Negative Suicide Ideation (PANSI) Inventory within a diverse sample of young adults. Journal of Clinical Psychology 61(4), 431–445.
National Youth Violence Prevention Resource Center (2007) CDC Report Shows Largest One-Year Increase in Youth Suicide Rate in 15 Years. Retrieved from http://www.safeyouth.org/scripts/facts/ suicide.asp#overview on 2 October 2007.
Norwood S.L. (2000) Research Strategies for Advanced Practices Nurses. Prentice-Hall Health, Upper Saddle River, NJ.
Nunnally J.C. & Bernstein I.H. (1994) Psychometric Theory. McGraw-Hill, New York.
Osman A., Gutierrez P.M., Kopper B.A., Barrios F.X. & Chiros C.E. (1998) The Positive and Negative Suicide Ideation (PANSI) Inventory: development and validation. Psychological Reports 82, 783–793.
Osman A., Barrios F.X., Gutierrez P.M., Wrangham J.J., Kopper B.A., Truelove R.S. et al. (2002) The Positive and Negative Suicide Ideation (PANSI) Inventory: psychometric evaluation with ado-lescent psychiatric inpatient samples. Journal of Personality Assessment 79(3), 512–530.
Osman A., Gutierrez P.M., Jiandani J., Kopper B.A., Barrios F.X., Linden S.C. et al. (2003) A preliminary validation of the Positive and Negative Suicide Ideation (PANSI) Inventory with normal adolescent samples. Journal of Clinical Psychology 59(4), 493– 512.
Perkins D.F. & Hartless G. (2002) An ecological risk-factor exami-nation of suicide ideation and behavior of adolescent. Journal of Adolescent Research 17, 3–26.
Pilowsky D.J., Wu L.T. & Anthony J.C. (1999) Panic attacks and suicide attempts in mid-adolescence. The American Journal of Psychiatry 156, 1545–1549.
Reinherz H.Z., Giaconia R.M., Silverman A.B., Friedman A., Pakiz B., Frost A.K. et al. (1995) Early psychosocial risks for adolescent suicidal ideation and attempts. Journal of the American Academy of Child and Adolescent Psychiatry 34, 599–611.
Reynolds W.M. (1987) Suicidal Ideation Questionnaire. Psycholog-ical Assessment Resources, Odessa, FL.
Reynolds W.M. & Johnston H.F. (1994) Handbook of Depression in Children and Adolescents. Plenum Press, New York; London. Rosenbaum M. (1980) A schedule for assessing self-control
behav-iors: preliminary findings. Behavior Therapy 11, 109–121. Rosenbaum M. (1990) Learned Resourcefulness: On Coping Skills,
Self-Control, and Adaptive Behavior. Springer, New York. Rosenbaum M. (1998) Opening versus closing strategies in
control-ling one’s responses to experience. In Personal Control in Action: Cognitive and Motivational Mechanisms (Kofta M., Weary G. & Sedek G., eds), Plenum, New York, pp. 61–84.
Schumacker R.E. & Lomax R.G. (1996) A Beginner’s Guide to Structural Equation Modeling. Lawrende Erlvaum Associates, New York.
Scientific Advisory Committee of the Medical Outcomes Trust (2002) Assessing health status and quality-of-life instruments: attributes and review criteria. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation 11(3), 193–205.
Tabachnick B.G. & Fidell L.S. (2007) Using Multivariate Statiatics, 5th edn. Ally & Bacon, Boston, MA.
Turner R.M., Korslund K.E., Bartnett B.E. & Josiassen R.C. (1998) Assessment of suicide in schizophrenia. Cognitive and Behavioral Practice 5, 139–169.
Warheit G.J. (1979) Life events, coping, stress, and depressive symptomology. American Journal of Psychiatry 136(4), 502–507. Zauszniewski J.A. (1997) The depressive cognition scale: further psychometric evaluation. Journal of Nursing Measurement 5(2), 191–200.
Zauszniewski J.A., Chung C., Chang H.J. & Krafcik K. (2002) Pre-dictors of resourcefulness in school-aged children. Issues in Mental Health Nursing 23(4), 385–401.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original research reports and methodological and theoretical papers. For further information, please visit the journal web-site: http://www.journalofadvancednursing.com