TAIPEI MEDICAL UNIVERSITY
SCHOOL OF HEALTH CARE ADMINISTRATION
MASTER’S THESIS
PATIENT SATISFACTION WITH HEALTHCARE QUALITY AT
SOLOMON ISLANDS, NATIONAL REFERRAL HOSPITAL
GRADUATE STUDENT: NELSON A. BILAU
ADVISOR: PROFESSOR, CHE-MING YANG
III
V
Acknowledgement
Firstly as a Christian want to place my sincere gratitude for God, with his invisible guidance, therefore, all Glory and honor given back to him.
Second, want to say thank you to my thesis advisor, Professor, (Che-Ming Yang) for his
academic advices result in completing my Master Thesis. Also want to extend my sincere thanks for the thesis committee members for supporting.
Want to thank my family back in the Solomon Islands for the moral support in one and the other during my two years in the University.
Also want to thank the staff of Taipei Medical University International Office for the great support.
Thank you also for the Teaching Faculty in the school of Health Care Administration, and other Department Faculties within the University.
Want to extend my thanks for the Research Committee at the Ministry Of Health in the Solomon Islands for kindly accepting my research proposal to do my research data collection in the National Referral Hospital.
Thank you for the administrators and the health care staff in the National Referral Hospital for supporting me during my research though they have very busy schedule with patients, but provided me time to collect necessary information.
Thank you also for the Research Assistance in the School of Health Care Administration for the support and providing appropriate information and directives when needed.
Want to extend my sincere thanks for the staff at the Taipei Medical University Hospital during my admission in the Hospital, really appreciate their care and healthful advices.
VI
Thank you for the students in the school of Health Care Administration for smiles and laughter we share some times.
Want to extend my biggest thank you for Christopher Douglas my best ever friend from Australia, he really supported whenever I expressed my financial constraints.
Also want to say thank you that words can‟t express for my for class mates, the good times we had, the laughter we shared, above all the interactions we had it means a lot to me.
Lastly, but not the least, like extend my big thank you for all the staff and students at Taipei Medical University for great support in one way and the other.
VII
Abstract
Title of the Thesis: Patient Satisfaction with Healthcare Quality at Solomon
Islands, National Referral Hospital.
Author: Bilau A. Nelson
Thesis advised by: Che-Ming Yang, Ph. D
Research background:
Research investigating patients‟ satisfaction has identified many dimensions or attributes that contribute to the construct of patient satisfaction with quality health care services. Patient satisfaction has been measured in the healthcare organizations in around the world over the past decade with various models are examined that have attempt to define and interpret the idea of determining individual perception of the quality of health care delivered. In this context, patient satisfaction can be defined as practitioner provides the treatment necessary to produce the health improvement possible. Our research study set on the Solomon Islands, National Referral
Hospital, and the largest of the hospitals. Primary aim is to evaluate the quality health care with patient satisfaction with the model to examine the service provided, coincide with identifying areas for improvement. The research hypothesis is based on the six quality dimensions in the conceptual frame work (Fig.1).
Labeled, medical care, treatment by doctor, treatment by nurse, information, participation and hospital physical environment. The expectation of patient satisfaction would be influence by the patient satisfaction health care quality dimensions or factors respectively.
VIII
Research objectives:
This paper evaluates the level of Patient Satisfaction with the regards to Quality Healthcare service provided at the Solomon Islands, National Referral Hospital.
To give the outcome (Result) to the Hospital Health Administrators and the Managers for further prospective considerations, basically patient health care strategic development for improvement.
Methodology:
The cross-sectional study was conducted with use of structured questionnaires. Total of 252 subjects are responds by using connivance sample technique. Inpatients for hospital stay, more than 48hours are eligible to participate with no age restriction. Each questionnaire last for less than 10 minutes. SPSS version 16.Sotfwear was used to analyzed utilizing the students‟-test paired differences, and One-Way ANOVA, the Pearson correlation, and linear regression
analyses by synthesized the quality factors to in respect to identify which factor has an influence on patient satisfaction as far as quality health care service is concern in the hospital. Statistical Significance was set at 0.05 (tow-tailed) for all analysis.
Results:
We measure total patient satisfaction by using single overall satisfaction question. The overall patient satisfaction is (89.7%) with the mean average (=8), and (SD =1.5). For each measuring quality factors, we found that Medical Care patient satisfied 59%, Treatment by Doctor 57%,
IX
Treatment by Nurse 64%, Information 63%, Participation 65%, and Hospital Physical Environment 64%.
Conclusion:
To our knowledge this is the first time the quality care patient satisfaction is conducted in the Solomon Islands hospital. The result display outcome of this research seems indicate half of our quality factors are controversial to the initial study hypothesis, but term as important and
essential. Those quality factors that least satisfied are expose to the health care mangers for improvement. In this regard quality factors such as Information and participation should be untaken by putting greater emphasis. As we summarize, though we had higher percentage of total patient satisfaction, it was a challenge for hospital with limited diagnostic devices, therefore, concerted effort and further prospective study is recommended in this regard.
X
Table of Contents
Acknowledgments………...V Abstract………....VII Table of Contents………...X List of Tables………...XII Figures………...XII
Chapter 1: Introduction 1.1 Background ………...1 1.2 Research Motivation………....21.3 Statement of the Problem………...3
1.4 Significant of the Research………...3
1.5 Research Objective………...3
Chapter 2: Literature Review 2.1 Healthcare Professional with quality care………..4
2.2 Patient Participation and Information………...10
2.3 Hospital Wards Environment………....15
2.4 Summary of Literature Review………...16
Chapter 3: Methodologies 3.1 Conceptual Frame Work………...18
3.2 QSP Model Description………...19
3.3 Hypothesis………...19
3.4 Operational Definition………...20
3.5 Instrument………...22
XI
3.7 Research Design………...23
3.8 Unit of Analysis………...24
3.9 Data Source & Collection………...24
3.10 Data Analysis………...25
Chapter 4: Results 4.1: Respondents‟ Characteristics………26
4.2: Patent Responds to Satisfaction items………...32
4.3: T/test & One- way ANOVA Analysis for Patient Satisfaction………..35
4.4 Pearson correlations with Patient Satisfaction….………...37
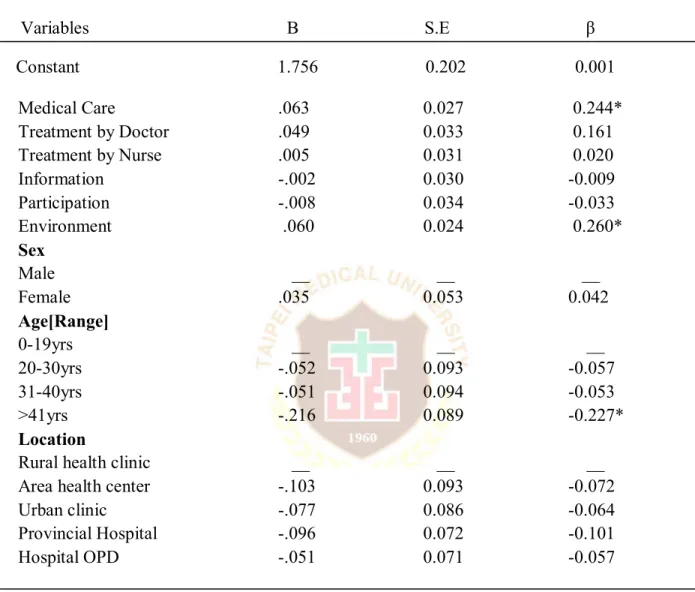
4.5 Regression Analysis for Six Quality Factors with Patient Satisfaction…...37
4.6. Liner Regression Analysis for Both Quality factors………...42
4.7. Result summary………..43 Chapter 5: Discussion 5.1: Discussions…...44 Chapter 6: Conclusion/Recommendations 6.1: Conclusion………...50 6.2: Recommendation………...51
XII
References………...52
Appendix 1: Patient Consent Form………...58
Appendix 2: Questionnaire………...60
Appendix 3: Request Letter……….68
Appendix 4: Permission Response………..70
List of Tables
Table1: Operational Definitions………..20
Table 2: Respondents Characteristics……….29
Table 3: Mean and Standard Deviation………...30
Table 4: Quality Patient Satisfaction Items……….33
Table 5:T.test and One-way ANOVA………...36
Table 6: Pearson correlation coefficient……….39
Table 7: Liner Regression for Six Quality Factors……….39
Table 8: Liner Regression Analysis for Patient Satisfaction………..40
Figures:
Figure 1: quality patient satisfaction (QPS) model………..18
1
Chapter 1: Introduction
1.1 Background
Research investigating patients‟ satisfaction has identified many dimensions or attributes that contribute to the construct of patient satisfaction with quality health care services. However, as many satisfaction studies are conducted in very specific context, it is understandable that any standard classification never seems entirely appropriate. Otherwise, Stimson and Webb (1993) defined satisfaction as “having enough” or “customer satisfaction”. But, in healthcare sectors, Donabedian, (1987), even provide more formal definition of patient satisfaction quality care which practitioners provide the treatment necessary to produce the health improvement possible. There is some disagreement in the literature regarding patient‟s ability to evaluate the quality of health care leading to patient satisfaction.
It is generally agree that patients are able to judge the delivery of care, or the interpersonal aspects, but some discord exists as to whether they can accurately judge the quality health care patients satisfaction of their technical care. Suggesting that patients‟ judgment of interpersonal care influence their judgments of technical care. Various models are examined in attempt to define & interpret the idea of determining satisfaction of quality health care delivered. Although research has identify that patients do have opinion about the various aspect of their care, it has not been examine with sophisticated methodology to determine if their judgments about health care services provide can predict their judgment about technical quality of care. The measurement of the patients‟ opinion about health care services a basis of quality patient satisfaction assurance, and different forms of benchmarking.
In this project, we adapt a model from previous study that focuses on the basis of patient quality healthcare satisfaction (Jorgen, Ingrid, Munk, Ingemar, & Sandber, 2001). Consequently, their objective is base on the tow prominent model, the „Quality patients‟ perspective (QPP), and Quality satisfaction performance (QSP) models, with respect to application, strengths, and weakness. Connivance sampling was used. This paper, we adapt the QSP model, which originates from a method use to assess health care customers‟ satisfaction. This model has been
2
used to assess patient satisfaction, mostly in the Obstetrics, and Gynecology departments. Reason we adapt this QSP model, because it measure a wide range of quality areas of patient perceived quality health care service delivery. This quality patient satisfaction model is rate on a standardize scale, and assess by means of questions.
Therefore, experience quality of different dimensions or factors of quality are priori regard as important in explaining patient satisfaction. However, in such a country that still in transition with its health care system, the study will anticipate to contribute for benchmarking with improvement of health care services when considering the outcomes, and recommendations. The demand for measurement of patient health care satisfaction outcome is the result of many factors, including lack of research, and the need for quantifiable data concerning health care, and variations within the clinical intervention in the hospital wards. In this regard, the instruments use is an adaption, because of reliability and validity for its extensive used. The main prime objective of the research is to evaluate „patient satisfaction, subsequently recommending for improvement.
1.2 Research motivation
Consumers of health care industry demand quality care services, and among is patient satisfaction. Patient satisfaction with quality of health care in particular, seen as the most important predictors of patients‟ overall satisfaction with their hospital care. Furthermore, it is somehow; appropriate to use patient satisfaction as a benchmark instead of medical‟ and clinical outcome indicators. Reason because patients are the recipient of care, and remain focus on basic physical needs that were central to their wellbeing, rather than technical aspects of care. Also for archiving the higher patient satisfaction, therefore, seems a necessary pursuit for any health care agency, and patient deserves quality of health care services.
3
1.3 Statement of the problem
Patient satisfaction of quality health care is absolutely the right of every health care consumer, and it is an essential service require in all health care centers. The National Referral Hospital healthcare professionals should offer the level of care that is acceptable to clients, authorities, and public at large. However, the trend of care provided more or less falls short of the required standard optimum or even to the maximum care. On this regard, quality health care is the essential service needing in the hospital. Also in quality health care assessment, measurement from the technical point of view is not enough, so as the measurements of inter-personal aspects. We feel that users‟ opinions are important for consideration.
1.4 Significance of the Research
Retrospectively no such nature of study, specifically in the discipline of quality health care patient satisfaction at the hospital. We think, it‟s a significant, and coincidently imperative as we anticipating taking this opportunity. Additionally, for further contribution in terms of identifying health care benchmarking in the area of quality patient satisfaction. Therefore, term as a determinative concept for prospective reference, and beneficial in one way and the other to the health care authority in the hospital, so as the policy makers at the ministry of health & medical services (MHMS). Also the consideration of relative importance of the different quality factors that use to perceive the outcome of the patient satisfaction, thus, it is often imply to the aspects of satisfaction with which patient least satisfy should be consider as priorities for improvement.
1.5 Research Objective
To assess and evaluate the level of patient satisfaction of quality at Solomon Islands National Referral Hospital and able give result to the hospital health care managers in the hospital for further prospective patient health care strategic development for improvement.
4
Chapter 2: Literature Review
This chapter reviews some of the issues that contribute to patient quality health care satisfaction, and therefore, divided in to three sections. Firstly, the Healthcare Professional with quality of care, („Medical care‟ and „Treatment by the health care providers‟), in the hospital wards that contribute in meeting patient quality care satisfaction when delivering health care to the patient. The second part, focus on the „information‟ that provide by the health care providers and with the „participation‟thus,decision making, coupling with the problem solving when it comes to patient health care satisfaction. And finally the „Environment‟ in which the patient stay during admission days in the hospital.
2.1: Healthcare Professional Quality Care
Professional healthcare providers was regarded as the basis of quality care as Zeki, & Erdogmus (2004) states they can contribute to dissatisfaction of care, rather than satisfaction, especially when they interact with patient with little intention of providing adequate health care service. In their investigation of patients‟ satisfaction rating, and medical health care services. Rakich & Darr (2000) found there was a significant association between satisfaction, and medical care, which was their objective measure. They could not conclude however, there was a relationship between satisfaction, and quality patient care. In a study of vulnerable elders‟ Chang, Hays, & Shakele (2006) has found that patient global ratings of satisfaction did not correlated with objective measure of quality health care patient satisfaction.
Their research compared objective measures of technical quality of care, that was, events in patients‟ charts were evaluated by a research team with specific quality indications with patient satisfaction do not necessarily mean that they actually received good quality care. Lee, & Kasper (2008) found through focus groups that health care consumers perceived three distinct components of patient care in hospital settings, the structure (hospital), the process (physician, nurses, and support staff), and outcome (resolution of health problem). They further found that consumers want their physician to display expertise that was comprised of competency, and
5
interpersonal skills. On this juncture, Zebiene, Razgauskas, Basys, Baubinien, Gurevicius, Padaika, & Svab (2004) posited that physician can control perceptions of patients care quality by giving patients compelling, and validating interpersonal care. Janko Kersnik (2000) imply that it was possible for patients to make appropriate technical judgment. Many researchers also believed patients are capable of making direct judgment of quality health care (Fan, Reber, Diehr, 2005; Chang et al., 2006; Otani, Kurs, Harris, 2005; Peter, David, Kavitha, Krishna, Ashraf, & Gilbert, 2008).
In an attempt to evaluate patient perception of satisfaction Lee & Kasper (2008) had manipulated levels of competency, and courtesy in simulated physician- patient interaction. It was concluded that patients were able to distinguished extreme difference between good, and poor physician behavior. Also Maria, Sean, Linda, Banica, Douglas, & Sabina (2008) has found that patient satisfied with medical care mostly, otherwise they consistently predicts satisfaction with technical skills, and nursing care appeared to be the most important variables that had an influence on patient satisfaction. In 2004, Zeki & Erdogrmus discovered patients perception of nursing staff, technical competence had little to do with overall patient satisfaction on quality health care service. Other researchers also found output of patient care satisfaction determines if the health care providers demonstrating services that meet patient needs (Rakich & Darr, 2000). However, Yu-Chi Tungi & Guann-Ming Chang (2009) discovered patient satisfaction of quality health care determined doctor‟s technical skills were outstanding, coupling with interpersonal skills, subsequently through doctors‟ physical examinations during ward round, medical treatment they have prescribed for the patient, including the overall staff care in the hospital wards. Otherwise supported with patient education for both overall satisfaction, and recommendation.
That is relatively similar to Otani and colleagues (2005) has described physician care was most influential, especially when doctor was more experienced, and serve more years in the field. On this matter, physician care that most directly affects the patient‟s medical concern or health recovery was associated with patient satisfaction. Generally, such findings can only guarantee that doctors‟ technical skill was more related to overall satisfaction of quality medical care. There finding is in line with Zeki & Erdogmus (2004) researched regarding inpatient care, said that, doctor‟s interpersonal skill was more correlated with overall satisfaction; coupling with the
6
doctor‟s technical skill was more significant factor in quality medical care. Another study discovered that 40% of the total patient study sample was satisfied with medical healthcare that was nearly equal proportions of patients satisfied. The second most frequently mentioned were contextual factors (21%) which related to conditions of doctor medical care skills, with two-thirds of the evaluations being rated dissatisfied (Ludmila, Konstanttynowicz, & Chlabicz, 2009). In 2000, Janko found patient satisfaction similarities are common in most hospitals or health centers, in particular those warded in surgery departments, tended to a higher value on technical skills, although pediatric patients also placed a high value on interpersonal skills. Cheng, Yang, & Chiang (2003) found the role of the doctor were found to be more associated with overall satisfaction, however, even among surgical patients, older patients [>50 yrs] placed higher values on medical care skills than younger patients[18-35yrs], but overall satisfaction was found to be more associated with all health care professionals (besides doctors), and that conclude that differences in patient satisfaction levels could be influenced by different health care staff with prioritized skills. In contrast, Fan et al. (2005) states having quality of healthcare satisfaction does not depend on doctors‟ skills, and staff care alone, but other contributing factors.
Also found patients were less satisfied with commitment, and care from their doctors‟ by not showing interest on their personal care situations, and most staff was showing very little interest when patients want their attention for support, otherwise only their guardians or proxy can support them in any way in the absence of the nurses, and the doctors in the ward. Therefore, patients were not satisfied with the behavior of medical officers, and the health staff (nurses).On the other hand Peter et al.(2008) found that patient perceived quality care was capitalized on when health workers are more comprehensive in taking patients‟ histories, good conduction of physical examinations, along with effective communication and courteous. However, patient satisfaction was compromised, when it comes to gender difference, male, and female doctor respectively. Fan et al. (2005) discovered the issue of culture, and patient dignity, due to some patients really want female doctors to take care of them, and vice versa, especially when it comes to physical examination.
7
Therefore, the presence, and involvement of the doctors‟ as qualified personal at the facility was associated with client perceptions of quality care satisfaction, and it was concluded with quality of healthcare satisfaction to be archive, exceptionally much depends on the specific independent variables such as health care medical professionals, the physicians, and the nurses .literally speaking, in general patient perspective of quality care was concluded when concerted efforts of all medical specialties to provide the health care consumers with the basic, and quality of care ever needed for comprehensive patient quality care satisfaction. A study found the relationship of high levels of satisfaction in each dimensions, such medical technical skills, interpersonal manner, and information, Compared to elderly patient to middle age patient was contradicted, while satisfaction was high, with over 90 percent surveyed expressing satisfaction, there was substantial variation with less likelihood of high satisfaction among those above 60years or older, with less education and in poorer health condition (Lee & Kasper, 2008).
On this juncture in regards to treatment done by the health staff with respect to patient, commitment of care and listening to the patient, however, was proved satisfied, in due respect with the care that were given to them (patient), particularly show them respect, and commitment of care, to fully satisfy their health needs. Most patient satisfy because health care providers are getting close to them for comfort, and assurance, therefore, patient most satisfied with the health care provider able to listen to them carefully, although they have the significant reasons for excuses (Maria et al., 2008).
Focus study on patients comparison of doctors‟ to nurses care, related to certain satisfactory elements, such as respect, commitment of care, listening, and treat the patient in a positive manner Ludmila, & colleagues (2009) apparently found patient in other countries most satisfied with nursing care than their physicians care. That also contributes to the point where patients in the observation units are more satisfied when doctors are more concentrated on their care, particularly taking care of their needs, respect their opinions and show them great commitment of caring attitudes. On the other hand, patient satisfied with care when their care providers, the doctors‟, and the nurses‟ are providing them with courtesy and emotional support prior to their admission in the hospital wards (Nerea et al, 2005). It was proven by doing holistic care which includes physically, socially, mentality, and even spiritually, patients can discouraged the path of anxiety and then reduce the rate of stress that mostly couple with his or her current unhealthy
8
situation while in the hospital caring wards, for this reason the health workers are very close to them (patients) and provided more support, and encouragement (Nerea et al., 2005). Most patient were satisfy with care that has been provide by the nurse, and the doctors with openness, whenever they ask them questions regarding their care, and conditions in the hospital. Coincidently it was not the same for all age groups Kerem et al. (2009) has found from age 18 -30 years are not satisfied with care from the health care providers, particularly with the element of respect shown to the patient, answering their questions, and demonstrating the commitment for meeting their caring needs, so as physical examination while in the wards. Otherwise they found patients above 30 years are more satisfied, and comfortable with care.
In 2009, Kerem et.al.concluded with the finding that patient were 96% satisfied with the care that doctors‟, and the nurse are equipped with or having a good broad knowledge of the disease, and the technical skills relating to the particular diseases they have, therefore, in this scenario most patients were said to satisfied with their medical care from the doctors, and the nurses in the hospital.
And also similar occasion, 98% patient satisfied was found from the research done in Korean hospital Jae et al. (2009) found patient satisfied with care because they have cordial relationship with their doctors, and nurses for not exceeding the period of five years, so that interpersonal can be maintained, in terms of respect, and able to deliver commitment along with the skills, above all patient mostly appreciate the care given by the nurses in the Korean hospital. Otherwise in contrast, some patients are not satisfied with their doctors, if they have relationship exceeding five years, based on the reason, the doctors will lose interest, and not showed them courtesy, and commitment for care, but other research found that the longer patient have relationship with health care providers (Doctors) more confidents the client should with their doctors in the hospitals, and health centers (Shea et al., 2007).
Therefore, number of factors known to influence patient satisfaction that patient expectation of service and actual service received is not adequate , like the age of the patient, younger patients in twenties, said to be more discerning, by voicing greater dissatisfaction with care that has been provided by the health providers (doctors & nurses) in the hospital, also found that patients tended to be more critical of attitudinal aspects of care, rather than technical aspect, and for gender, women (97%) voiced greater satisfaction with their care than men (73%). But on the
9
other perspective for total satisfaction, underscores that client satisfaction was determined by the cultural background of the people as well. It shows the dilemma that though optimally care should be capable of meeting both medical and psychosocial needs (O‟Connell B., & Young J., 1999).
In 2008, Georgios, Birbils, Olga, & Chrysou found that patient satisfaction was higher for the medical (89.7%), and nursing(86.4%) service respectively, but has nothing to do with culture or personal background in some ways either organizational culture, and to somewhat extend depending on age, gender, location, education, number of previous admissions, and self-assessment of health status at the first, and last dayof patients' stay in the hospital wards. Gender and race differences are also emerged in respondents‟ perception of identity threat. In this scenario satisfaction of patient health care quality does not stable on the certain quality dimensions or factors, but rather it is a diverse and complex patient outcome to measure when it comes to the patient health care quality satisfaction in the health care industries/institutions (Coyle, 2010).
To allude the concept of patient health care satisfaction in the health care industries, we can appreciate the fact, that in order for patient satisfaction in health care arenas to take its full potential courses or directions, it is the role of the health care providers to demonstrate, and deliver the best caring attitude, and behavioral manner, coupling with the technical skills, interpersonal skills, information transferring, and problem solving techniques. Georgios et al. (2008) also found that patient satisfaction with medical care was influenced of decisions regarding choice of health care plans, that compliance with prescribed regimens, and clinical outcomes.
In addition, patient characteristics also influence by manner in which the health care is delivering, the type of care, setting, and characteristics of the health care consumers, such as education, age, gender, and location, all contributing to patient satisfaction of health care quality (Alazi & Neal, 2003). It has been thought for some time that patient satisfaction with medical care reflects satisfaction both with how care is delivering (process), and with the results of that care (outcome). However, Kravitz (1998) suggests that health status (rather than degree of improvement in health status) also influences satisfaction.
10
2.2: Patient Participation and Information
It has been a major shift in the approaches to clinical decision making in the last generation of practicing physicians. For much of the 20th century, physicians, and their designates are consider as the keepers of medical information, and the sole decision makers. Rajiv & Carol (2008) found information exchange is an important component of patient care, but since then the measurement of patient satisfaction has been encourage by a growing consumer orientation in health care, and especially since it yields participation in decision making, and information about consumers views in the form which can be use for comparison, and monitoring. But drawing on literature from a particular source, apparently Avis, Ma, & Arthur (1994) pointed out, there remains several unresolved issues relating to the measurement of satisfaction, inclusively in the capacity of participation, and information sharing with patients while in the observation units or in the hospital wards.
Was also argued by Hall, & Dorman, (2002) that current approaches to measuring satisfaction may not be grounded in the values, and experiences of patients despite perfect medical, nursing, and interpersonal skills, that the health care professionals has demonstrated, therefore, the indication of satisfaction surveys could be denying patients opportunity to have their opinions included in the planning, and evaluation of their health care services.
On that knowledge, when it comes to participation, and information sharing in socio-demographic status, there were some difference in the hospital wards, it was not correlated to satisfaction as all measures were contradicted to each other when examines the relation of patients with their satisfaction of health care, by saying that, in 2002 Hall, & Dorman found some patients in the wards rated participation, and information received from the health care providers very low.
In contrast, one survey of 236, “vulnerable” older patients found that receiving information or having communication skills were linked to higher patient satisfaction (Chang et al., 2006). With this regard, patient satisfaction is significantly positive associate with greater age (elderly)
11
patients‟ satisfaction with quality of health care is sparse, less education, and also marginally significant satisfaction associated with being married, and having higher social status.
These factors otherwise contribute a lot in receiving information from the health workers with their involvement in their healthcare while in the hospital. However, that does not guarantee some of the study variables to have the same outcomes as the average magnitudes of relations. In a recent study by Moret, Nguyen, Volteau, Falissard, , Lombrail, & Gasquet (2007) discovered age being the strongest correlate of satisfaction, and no overall relationship was found for ethnicity, sex, income, or family size. For all socio-demographic variables, the distribution of correlations was significantly heterogeneous, and statistical contrasts revealed the operation of several moderating variables. Therefore, the ability of the doctor to inform, and instill confidence in patients, and convince them of the need for their compliance, for example, can make the difference between satisfaction, and dissatisfaction, in this context, the information was far more important.
It has been identified that all the caring health professionals, face the similar problems with patients who are non-compliant, and with those who have difficulty in understanding the instructions being given, that leads to the reason why patient satisfaction was not archived in information sharing, because lack of adequate information and participation from the health care providers with their patients, and sometimes the patient attitude causes themselves to reject being involve in their care, also they discovered most doctors and nurses are concentrate only on medical care management rather than information so as participative approaches with the patients (Schmid, Hall, & Roter, 2008).
Angie, Karlsen, & Addington (2000) found that dissatisfaction was arise from the sense of being „devalued‟, „dehumanzied‟or „disempowered‟ and from the situations in which the „rules governing the expected health professionals – patient relationship were broken, and that was some of the causes of not satisfied with the participation in their care, and very much similar to those who received information regarding their inpatient care management.
In 2008, Schmid et al also found why information is not meet the client satisfaction in several health care centers, because they [patient] expect those who deliver the information regarding patient health care must have the correct identification of who they are, more particularly in their field of medical specialization, and also those (nurses) who receive information about their (patient) health status is not adequately deliver, and explain in detail the conditions or the
12
prognosis, and the medical diagnosis. Schedule for medical information, and other related activities must explain to patients in advance before the health workers can carried their medical procedures. Recently Rajiv et al. (2008) found that participation in decision making was rated higher satisfaction of 91% ,and obviously patient satisfied with their care because, it help the patient to improve their knowledge, reduce medical decisional conflicts, and stimulate patient to be more active in decision making without increasing their anxiety.
Consequently participative relationship between patient, and health care workers, the physicians, and the staff, resulted in the facilitated communication, and medical care quality decision making, a decrease of patient fear, and better treatment adherence (Mari, Hanneke, Haes, & Smets, 2010). In addition more on patient satisfaction with participative in their decision making, there is a degree of uncertainty with respect of treatment of effectiveness, quality of life, and functions outcomes in the medical health care arenas under these concepts, are participation and communication between the patient, and the physician is essential to guide treatment decision making to select the treatment that most consistent with the patient value, and life style.
Shared of decision making, Gulmans el at. (2008) debated the process of actively involve the patient in their care, and was characterized in two fold, by which information between the physician, and the patient. It was found patients satisfied when physician sheared the technical information such as diagnosis, treatment alternative, risks, and benefits, and the anticipated outcomes of the total care, while in the hospital observation units. And on the other hand, patient too, can share their personal information such as lifestyle, work and family responsibilities, beliefs and fear. After this kind of participative information exchange or dialogue, both the patient ,and the physician can work together to arrive at the mutually acceptable treatment decision, by doing so, patient can fully satisfied with the care and the treatment he or she received afterward (Rahmqvist, & Bara, 2010).
In contrast, Geppert (2002) discovered that involving patient in the planning of delivery of the services was comprehensive, and nobody knew how to do it better, and even there was no evidence of such improving the quality of care for the patient in the past, however, was proven as misleading. Marij et al. (2010) convinced that there was a living evidence as demand for quality
13
health care was concern, patients were encouraged to involve in the planning of health care service by giving them information about quality of services that leads to patient satisfaction. Though found it was paramount important for patient to involve in decision making regarding their care, there were some barriers as most health care professionals concerns about not having enough time, from the perception that patient characteristic or clinical situations were not conducive to share decision making, however, was found 93% clinician agreed that sharing decision making with the patient was useful, and most patient want to participate in making decision together with their health care professionals, and also another important concept is the information sharing to the patient, as most patient are very pleased if they have adequate information regarding their present diseases, can relatively contribute to the sense of self preventive measures from having such in the future (Rajiv et al, 2008).
It is worthy when provide information, and opportunity in involving patients in decision makings, as Edward & Elwyn (2001) found health care consumers become more weary of the treatment offer, and making more conservative choices, and it convincing for health care providers to inform the health care consumers by means of certain programs within the hospital wards, such as health education through video, music, pamphlets, posters, and other forms that can convinced the mindset of the patient or heath care consumers. Was found 89% patient satisfied with care when received the information through open discussion by providing their medical documents, and explained thoroughly the nature of their medical problems, therefore, effective communication was the way important in reducing patient anxiety, and, the health care consumers.
Shea et al. (2007) imply that understanding of information sharing is a vital element in patient archiving health care satisfaction, and therefore, separation of information items from explanation, and understanding may show a hidden desire of patient to received information in a way that acceptable to them, but it was discovered 41% the total population were satisfied with the information received in the health care units in the Lithuania hospital in Europe.
Apparently, information transferring to patient from health care providers is very poor as it was negatively assessed, but on the other perspective was scrutinized from another study, and foreseen that health literacy was a huge contributing factor that hindering the flow of medical
14
information from health care providers to the health care consumers, in this scenario it is difficult for the patient to understand the information deliver in the health care setting. More low literacy rate patients can also contribute to the dissatisfaction of the information given about their healthcare. Edward and Elwyn (2001) found that health care providers need to explain, and provide appropriate information that needed, before patient can satisfy. Compared to the age group Geppert (2004) found younger patients were not satisfied at all regarding the information received while in the hospital. And also it has long been recognized that difficulties in the effective delivery of health care can arise from problems in communication/information given between patient and provider rather than from any failing in the technical aspects of medical care.
Improvements in provider-patient communication can have beneficial effects on health outcomes. A systematic review of randomized clinical trials and analytic studies of physician-patient communication Geppert (2004) confirmed a positive influence of quality communication on health outcomes. Also to add on, doctor-patient communication (Information) can also affect the rates of satisfaction. When patients who presented to their family physician for work-related, low-back pain felt that communication with physician was positive (i.e., the physician took the problem seriously, explained the condition clearly, tried to understand the patient‟s job, and gave advice to prevent reinjures), their rates of satisfaction were higher than could be explained by symptoms relief (Coyle, 2010).
In this regard, adequate information, and patient participation in decision making are factors alluded to health care satisfaction. For participation Kasper and Fowler (1993) surveyed 150 women recently, diagnosed with breast cancer, 20% wanted an active role in deciding their treatment, 28% preferred a joint decision, and just over half (52%) wanted their surgeon to decide for them. In this scenario, adequate information and let the patients participation are most important factors in patient perceived health care satisfaction.
15
2.3: Hospital physical Environment
The surrounding physical environment had an influence on patient satisfaction, They were asserted physical environment includes cleanliness was very crucial aspect in the health care units in the hospital, patient can felt the first expression of healing psychologically when they confront with the clean environment. It was found that 89% patient satisfied with clean hospital environment (Gulmans el at., 2008). Food on the other hand is another very important entity as it constitutes more of balance diet can also help patient for contribution of healing, but they discovered patients were not satisfied (30%) with the preparation of the food, and more patient are satisfied when their health care providers provide them information regarding balance diet, and most of all the patients preference regarding what type of food.
For good environment for the sick patients Geppert (2004) found that most patient prefer environment that less of sound or noises, as they contemplating that most patient are not satisfied with the hospitals that located very close to the busy street, particularly in the metropolitan context. Lastly they found most patients were satisfied (96%), because the environment was conducive in terms of aesthetics of the premises, and more than that, the rest rooms, and ablution blocks are accessible, and be in good health condition. Also most patients registered their satisfaction with the environment because, hospitals are having admissions rooms for only maximum of two patients, they discussed less satisfaction (45%) if more than maximum numbers confine in one admission room. Generally patients also satisfied with the hospital linens are clean and in good condition, so as available when it needed (Johansson, Oleni, & Bengt, 2002). They also asserted that patient satisfied because the hospital environment they lived was of good relationship, between the health care providers, and also had sound, and close relationship with their patients. Otherwise 2006, Shea et al. also found patients satisfied with hospital physical environments was clean, more privacy, and promoting independence whenever necessary. Patients also satisfied because sufficient supplies of bedding, clothing, and personal linen are provided. Most of all they (patient) satisfied because their dignity is always maintained, and culture is respected.
16
2.4: Summary Literature Review
To evaluate, and improve the quality of healthcare, it is everybody‟s‟ responsibility, the health workers who deliver the services, and the health consumers as the recipient of the services. Patient satisfaction found as a significant indicator of the quality of care. Consequently, quality work includes investigations that map out patient satisfaction, inclusive of the interactions, information sharing, and the environment in which the patient stay. As it has been discussed in the literature review that patient satisfaction somehow is the basis of quality indicator for satisfactory health care services.
It has been thought for some time that patient satisfaction with medical care reflects satisfaction both with how care is delivering (process), and with the results of the care (outcome). In the literature review we discovered that patient satisfaction has been challenged in today‟s health care institution in many developed, and developing countries. Having said, that patient satisfaction is the fundamental component for quality healthcare services. Professional health care providers are the basis of quality care; they can arbitrarily influence the progress in one way and the other.
In this regard, patient satisfaction depends on many quality factors, but based on literature, technical and interpersonal skills, good behavior, commitment of care and effective communication (information) so as involving patient (participation) in decision making are the elements that contributed most to patient satisfaction. Therefore, patient satisfaction has been researched for years, and many countries has been drastically improved their health care facilities, but compared to Solomon Islands hospital even very little has done with this regard. Otherwise we optimistic the study will able to make any changes or improvement along with our findings on the areas that contribute to the quality health care patient satisfaction.
17
Chapter 3: Methodologies
This chapter has introduced the method that used in the survey research, which includes the conceptual frame work, hypothesis, operational definitions, instruments, sampling, data source, units of analysis, and analytical measures. Since the objective of this study to evaluate patient quality healthcare satisfaction, the key dependent variable is, „Patient satisfaction‟. The independent variables of this study are Medical care, Treatment by doctor, Treatment by nurse, Information, Participation, and Environment. While on the other hand the confounding variables which support measuring the patient quality health care satisfaction, such as Gender, year of birth (Age), Wards, Education level, and Location respectively.
18
3.1 Quality Patient Satisfaction (QPS) Model
Quality Factors
Fig1: Conceptual Frame work of the study.
Patient satisfaction
Age Wards Gender Location Education Medical care Treatment by doctor Treatment by nurse Information Participation Environment19
3.2: QPS Model Description:
The QSP model originated from a method used to assess customer satisfaction. The model has been developed, and adapted for assessing patient satisfaction. Study has been done in the gynecology and obstetrics wards (Jorgen N. B., & colleagues, 2001). Patient Satisfaction model was rated on a standardized scale, and assessed by means of questions. This forms the „Patient Satisfaction Index‟ (PSI) which was estimated from the weighted average of the questions. Experienced quality of different dimensions or factors of quality are a priori regarded as important in explaining patient satisfaction.
Three or four questions were formulated to cover each factor. This conceptual model used to capture the outcome of care in regards to patient satisfaction. Instruments are structured, relatively genesis, and extracted from the literature review as an adaptation. Coincidently the confounding variables definitely include, such as gender, age, ward, educational level, and location. In regards to perceive patient hospitalize quality care patient satisfaction, the above model (Fig 1) was used to measure the quality of healthcare service of the hospitalized patients.
3.3 Hypothesis:
Hypothesis 1: We said that patients are satisfied with Medical Care service provided at the National Referral Hospital.
Hypothesis 2: Patients are satisfied with treatment given by the doctor in the wards at the hospital.
Hypothesis 3: Also we said, patients are satisfied with treatment by the nurse in the hospital. Hypothesis 4: Patients are satisfied with Information they received from the health care Providers in the hospital observation units/wards.
20 to their care while in the hospital.
Hypothesis 6: Also we hypothesized that patients are satisfied with Physical Environment of the National Referral Hospital in the Solomon Islands.
3.4 : Operational definitions
Table1:
Variables Operational definition
Scale
Dependent variables
Satisfaction
To ask whether patient is fully satisfied with care Score: 1-10, not satisfied at all to very satisfied.
Continuous Independent variable
Medical care quality Professional skills performance out come with
range not satisfied at all = 1 to very satisfied = 10 Continuous Treatment by doctor How patient rate doctors‟ care with range not
satisfied at all = 1 to very satisfied =10 Continuous Treatment by nurse Patient rate the nurses‟ care with range not
satisfied at all = 1 to satisfied =10 Continuous Information Patient informed about procedures done to them
21
Table1: (Cont’d)
Participation Patient involvement in decision making, not
satisfied at all = 1 to very satisfied = 10 Continuous
Environment Tidiness and the comfort of the unit atmosphere,
not satisfied at all =1 to very satisfied =10 Continuous Confounding factors
Wards Medical = 1, Surgical = 2, Gynecological= 3,
Pediatric= 4, Orthopedic= 5, Tuberculosis= 6,
Obstetric ward = 7 Discrete
Age
The age of the patient in a cut of points. 0-19= 1, 20-30=2, 31-40=3, >41=4
Continuous
Gender
The ID use is SEX to determine their gender.
M =1 & F = 0 Discrete
Education
Subdivide the level of education in four categories. Junior = 1, Senior = 2,
Tertiary = 3 , No formal education = 4 Discrete
22
3.5 Instrument
This instrument was genesis from the study which has been went through massive extensive interviews conducted by Jorgen N. B., & colleagues, 2001) consisting of open ended, and individually adapted follow up questions covering the following themes: (a) Issues of importance with regard to the care the patient received; (b) what the patient perceived as satisfied or dissatisfied in connection with the care; (c) period of care; and (d) whether the patient wished to change anything regarding the care. After successful completed the pilot study with open ended questions in order to see what issues were regarded as important by the patients, after shortly the most important domains, and questions were identified. Therefore, this instrument is said to be valid and reliable.
In our research, patients were asked to answer questionnaires related to the quality of care in the hospital observation units, during the commencement of the program. 10 point scale with the extreme labeled „not satisfied at all‟ (1) to „very satisfied‟ (10) was used, refer appendix (2).Total of 33 questions were asked, of which 4 questions for „Medical care‟ dimension, 7 questions for „treatment done by the physician‟ (doctor), 7 questions for the „Treatment by the nurse care‟, 6 for the „Information‟ given, 4 for the „ Participation‟, and 5 for the hospital ward „Environment‟ dimensions respectively. An additional question was asked for the overall satisfaction. This will include a question such as, „are you fully you satisfied with the care you received so far, it also measured on the 10 point scale rating. In this circumstance, we had total of 34. This single dependent variable question was supposed to be defined as the total average score of quality care for patient satisfaction.
23
3.6 Convenience Sampling
Convenient sampling was used for this research survey. This hospital currently involves with both primary and secondary care. Patients all over the Solomon Islands are beneficial from this hospital. Patients are group according to different type of medical diagnoses and conditions, gender, and age groups such as the pediatric unit which less than five years. All patients were given the opportunity to fill in the questionnaires form.
Therefore, 260 sets of copies were distributed. Later we identify our sample size when all the forms returned. This was done to calculate and confirmed our sample size. On the other hand, this convenient sampling more feasible in terms of the reliability of the questionnaires that focus on diverse quality factors which can determine the outcome of health care satisfaction perceived by the respondents in the caring units. It considers more areas of diverse quality satisfaction factors, and described prior to the reliability, as far as patient satisfaction in health care quality is concern.
3.7 Design and Unit of Analysis
We performed cross sectional study design. All the caring observation units are part of the study, restricted to patients only, exclusive of the health care personals. Patient in the observation units for more than 48hours of hospital stay are highly encouraged to participate in responding to the questionnaires. Each patient received a copy of structured questionnaires, expecting to complete within the limit of ten minutes. For the illiterate participants, and those who are too old, physically weak, the researcher read the questionnaires to them; providing they respond positively, otherwise the proxy or their guardians answer the questionnaires for them instead.
24
The administration of the questionnaires was by the researcher, and possibly to scrutinize the respondents when answering the questionnaires. Daily out-patient department patients are not involved so as psychiatric ward on the other hand, because mentally retarded capability of judgment, and conductivity, as the nature of medical diagnoses was concerned. But in the case of the pediatric unit involvement, the parents or guidance was responsible.
3.8: Data Source
We collect the primary data from National Referral Hospital, the only urban hospital. This facility said to received the bulk of highly specialized health workers locally and internationally. For the years. The researcher decided to picked on it because for connivance, and most attended facility in the country. It provides the most comprehensive range of services as compared to other facilities.
3.9: Data Analysis
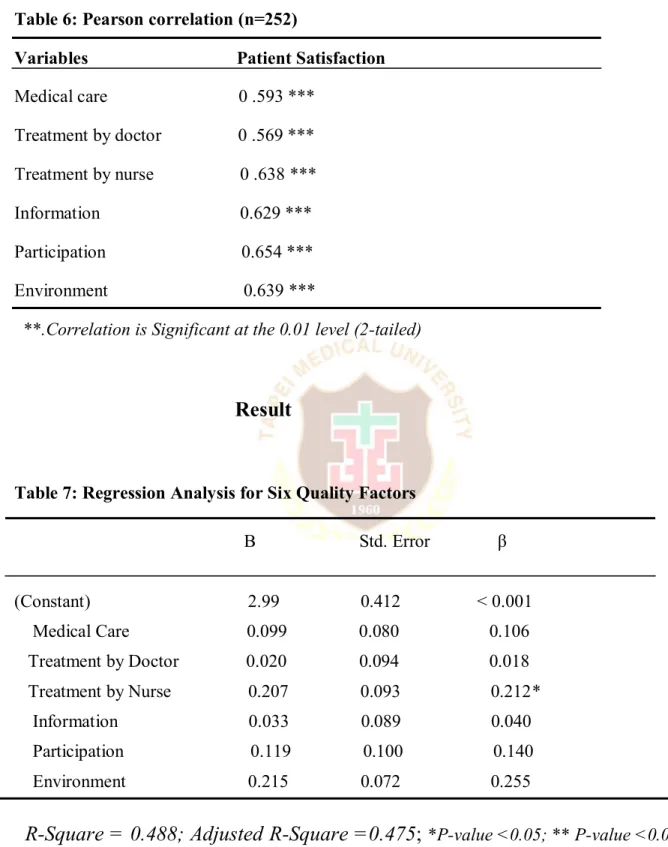
The numerical descriptive statistic was used to summarize the sample data, including the “mean” and “standard deviation” etc, and calculated for the continuous data while for the categorical data “frequency” and “percentage” was used to show the distribution of discrete and continuous variables. Then we determined to find the relationships between the quality factors and „patient satisfaction‟ were estimated by performing the One-way ANOVA with Scheffe‟s post hoc was used to estimate the possible differences in mean index values between the variables. Also we performed Pearson correlation with quality factors. Because the study objective is to evaluate the patient satisfaction of quality health care, all the quality factors
25
therefore, be incorporated in which we used liner regression statistical analytical method, and the proposed (P<0.05) for significant level.
3.10: Ethical Considerations
Formal permission was granted from the responsible National Research Health Ethic Committee in the Ministry of Health. Consent form for the patient to sign before participating was also introduced, with its objectives, and the purpose of the study. Subsequently the significance of the survey research. Participants within the respective observation units in the hospital were reassured of confidentiality, and the anonymity to highly upheld, not recommended for any unnecessary disclosure of the information at any given circumstances which might arise
26
Chapter 4 Result:
This chapter presents the results of the research findings. We began collecting data from10th Jan- 21st February 2011. This particular hospital has the largest admissions for years, known to be the largest and the only national health Referral center in the country. There are 260 questionnaires were prepared and distributed to the participated participants. Four questionnaires were not returned, and another four questionnaires though returned, but with uncompleted data, then excluded in our final data analysis, After all the questionnaires were returned, we found that only 252 questionnaires were entered in to the computer for statistical analysis by which SPSS Software package (version16.for Windows) was used.
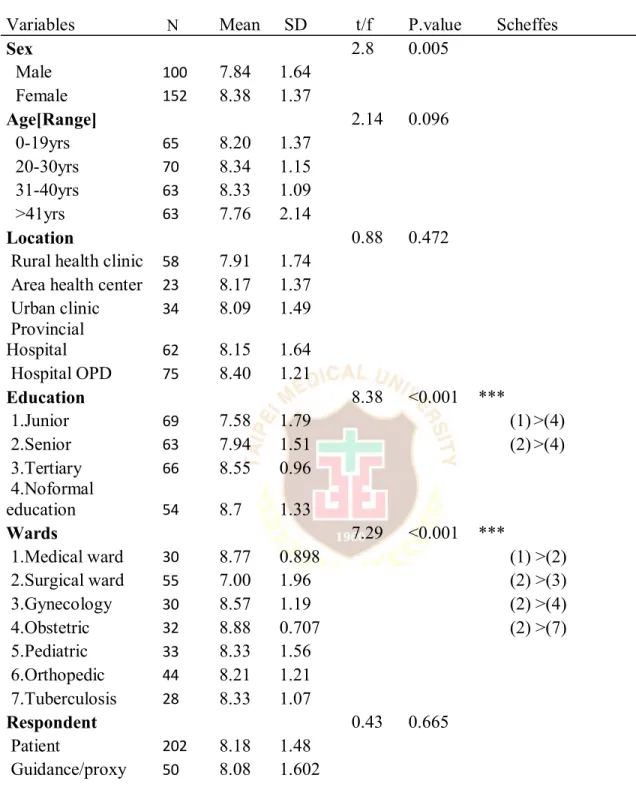
The Statistical significance was set at 0.05 (two tailed) for the analysis used to define a strong correlation of patient satisfaction. Total of seven wards were participated in the survey research. Our statistical analysis of patient satisfaction focused on descriptive analysis, which inclusive of patient‟s frequency and percentages, subsequently the Pearson correlation, then finally the Statistical Regression Analysis to identify the quality factors that has an influence on patient satisfaction of quality health care in the Hospital.
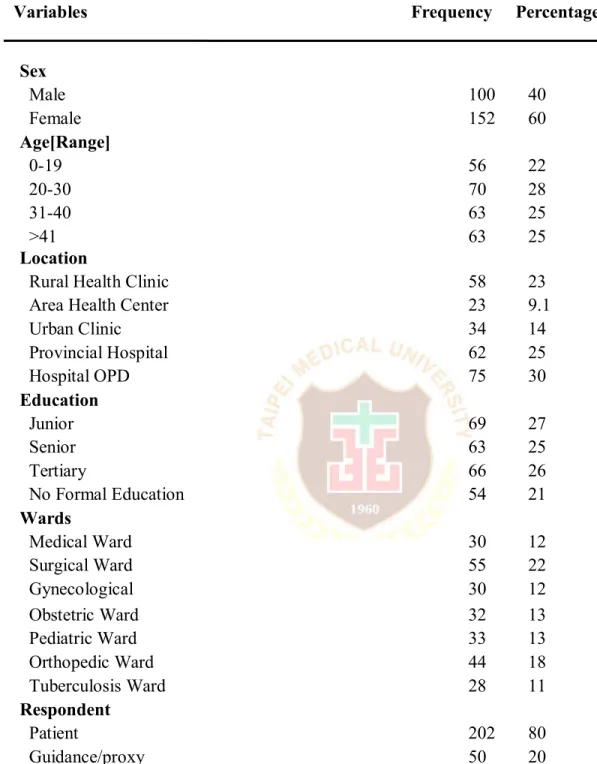
4.1: The Respondents‟ characteristics
Table 2, for gender we found that female patients are more compared to male patients. Age
we have categorized them in cut of age groups, those patients age 20-30years accounted for (27.8%), and 0-19years least accounted for (22.2%). The „Location‟, hospital Outpatient department (OPD) with the highest of (29.8%) patients referred from to the admission units, compared to other health centers; otherwise the least was Area Health Center with (9.1%). For
27
„Education‟ background of all the patients, we found majority patients were from „Junior‟ high schools ( 27.4%), while on the other side, patients with „ No formal education‟ has the least (21.4%). For the „Wards‟, the surgical ward have the highest number of patients, (21.8%) against the Tuberculosis ward of only (11.1%). Having said, the numbers we got for each ward was the standard admission number of patients in each ward respectively.
For the respondents, the patients, and proxy, patient on the other hand have (80.2%) responsible to rate their own health care satisfaction standard, in regards to health care quality in the hospital caring units. However, in this scenario we assumed that the proxy had response to the quality patient satisfaction questionnaires exactly according to what, and how‟s the patient feels about the care she or he has received while in the hospital ward.
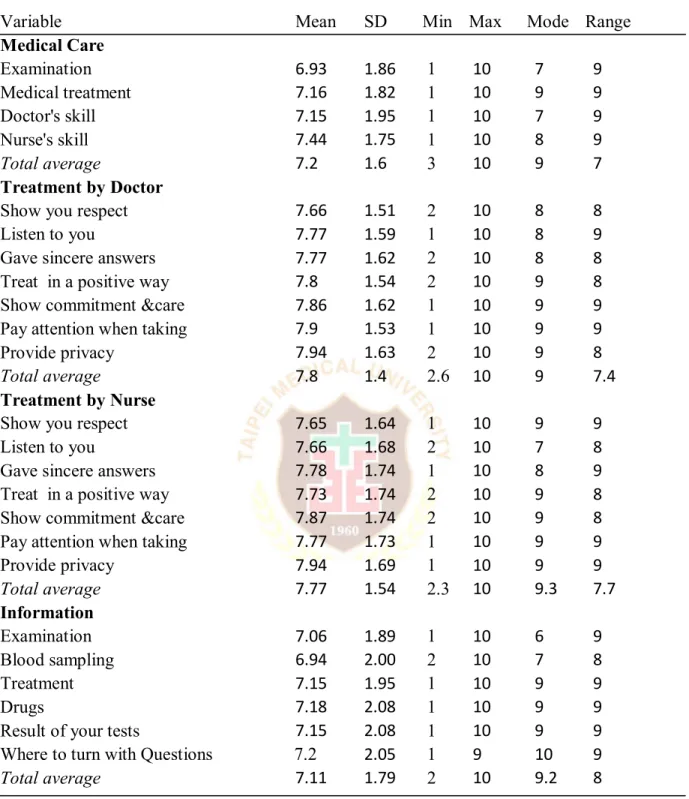
Table 3, for „Medical care‟ quality factor, the average (= 7.2) with the standard deviation (=1.6). With that, we said, the majority of the patients have answered the questionnaires on a higher satisfaction scale. „Treatment by doctor‟, patients has the average score of (= 7.8), and standard deviation (=1.4) respectively. In this circumstance, we could tell that majority of the respondents are rating high scale satisfaction. For the Nurse‟s treatment, we found that it was very encouraging, and satisfactory with the mean (= 7.8), & standard deviation (=1.5). For „Information‟, however, we found average (= 7.11), & standard deviation (=1.8).
„Participation‟ we discovered that the mean score was (=7.3) & standard deviation (=1.7). The „Physical Environment‟, patients‟ mean score (=7.4), & standard deviation (=1.8). Therefore, healthcare consumers are still happy of making their way to the hospital, and they really appreciate the tidiness of the wards, and its comfort ability, opportunity in talking with their doctor in private, the quietness of the wards was good for the healing process. We also have one
28
total satisfaction question in addition; basically to know exactly the respondents view plight to the overall „Patients Satisfaction‟ regards to the healthcare they received after the 48hours prior to the admission. With this single question, we found that the mean was (=8.2), standard deviation (=1.5). Henceforth, these results reflect high scale rating in regards to the „Patient Satisfaction‟ quality health care perceived in the hospital caring units.
29
Table 2:.Frequency and percentages of respondents’ characteristics (n=252) Variables Frequency Percentage
Sex Male 100 40 Female 152 60 Age[Range] 0-19 56 22 20-30 70 28 31-40 63 25 >41 63 25 Location
Rural Health Clinic 58 23
Area Health Center 23 9.1
Urban Clinic 34 14 Provincial Hospital 62 25 Hospital OPD 75 30 Education Junior 69 27 Senior 63 25 Tertiary 66 26 No Formal Education 54 21 Wards Medical Ward 30 12 Surgical Ward 55 22 Gynecological 30 12 Obstetric Ward 32 13 Pediatric Ward 33 13 Orthopedic Ward 44 18 Tuberculosis Ward 28 11 Respondent Patient 202 80 Guidance/proxy 50 20
30
Table 3: The average mean and standard deviation of Respondents (n=252)
Variable Mean SD Min Max Mode Range
Medical Care Examination 6.93 1.86 1 10 7 9 Medical treatment 7.16 1.82 1 10 9 9 Doctor's skill 7.15 1.95 1 10 7 9 Nurse's skill 7.44 1.75 1 10 8 9 Total average 7.2 1.6 3 10 9 7 Treatment by Doctor
Show you respect 7.66 1.51 2 10 8 8
Listen to you 7.77 1.59 1 10 8 9
Gave sincere answers 7.77 1.62 2 10 8 8
Treat in a positive way 7.8 1.54 2 10 9 8
Show commitment &care 7.86 1.62 1 10 9 9
Pay attention when taking 7.9 1.53 1 10 9 9
Provide privacy 7.94 1.63 2 10 9 8
Total average 7.8 1.4 2.6 10 9 7.4
Treatment by Nurse
Show you respect 7.65 1.64 1 10 9 9
Listen to you 7.66 1.68 2 10 7 8
Gave sincere answers 7.78 1.74 1 10 8 9
Treat in a positive way 7.73 1.74 2 10 9 8
Show commitment &care 7.87 1.74 2 10 9 8
Pay attention when taking 7.77 1.73 1 10 9 9
Provide privacy 7.94 1.69 1 10 9 9 Total average 7.77 1.54 2.3 10 9.3 7.7 Information Examination 7.06 1.89 1 10 6 9 Blood sampling 6.94 2.00 2 10 7 8 Treatment 7.15 1.95 1 10 9 9 Drugs 7.18 2.08 1 10 9 9
Result of your tests 7.15 2.08 1 10 9 9
Where to turn with Questions 7.2 2.05 1 9 10 9
31 Table 3: Cont’d).
Variable Mean SD Min Max Mode Range
Participation
Appointment prior admission 7.2 1.99 1 10 9 9
Choose of Doctor 7.31 1.92 1 10 9 9
Discuss alternative treatment 7.3 1.92 1 10 9 9 Student should be present or
not during examination 7.43 1.94 1 10 9 9
Total average 7.32 1.81 1.3 10 9 8.8
Environment
Finding way to the Hospital 7.3 2.04 1 10 9 9
Tidiness at the ward 7.32 1.98 1 10 9 9
Comfort at the Hospital ward 7.9 1.96 1 10 9 9
Atmosphere 7.33 2.04 1 10 9 9
Possibility with talking with 7.45 1.93 1 10 8 9
the doctor in private
Total average 7.38 1.78 1.6 10 9.2 8.4
Total satisfaction
32
4.2: Patient Responds to Quality Satisfaction items
In table 4, we did extra work by regrouped the 10 point scale in three categories. i.e., 1-4 (=Dissatisfied), 5-6 (= Undetermined), and 7-10 (= Very satisfied). However, the single overall patients‟ satisfaction question‟, like, „are you fully satisfied with the care given to you in the ward, was accounted for (= 89.7%). For the quality dimensions we found patient satisfaction with „Medical care‟ quality factor, shows all the health care variables involved were all rated satisfied from 60%-70% 0nly. On the same note, very few were dissatisfied, and undetermined with the care given to them. „Treatment by doctor‟ it was also convincing as majority of the respondents are satisfied with all the rating variables therein. Otherwise, only few respondents are dissatisfied, and undetermined.
„Treatment by nurse‟, shows higher satisfaction of 80% in which majority of the patients were satisfied with the healthcare given in the wards, on this juncture only very handful of patients are not satisfied, and even some are undetermined of the care provided. For „Information‟ quality factor, we found majority of variables involved were 60% satisfied, otherwise. For „participation‟ quality factor, also said to be satisfied ranges from 60%-70% as far as the variables involved are concern. The „Environment‟ quality factor also range from 60%-70% in rating satisfaction. So only minorities of the respondents were dissatisfied and undetermined whether the environment was good or otherwise.