www.elsevier.com / locate / euroneuro
O
mega-3 fatty acids in major depressive disorder
A preliminary double-blind, placebo-controlled trial
a ,
*
b ,*
b,d cKuan-Pin Su
, Shih-Yi Huang
, Chih-Chiang Chiu
, Winston W. Shen
aDepartment of Psychiatry, China Medical College Hospital, No. 2, Yuh-Der Road, Taichung 404, Taiwan
b
Graduate Institute of Nutrition and Health Sciences, Taipei, Taiwan
c
Department of Psychiatry, Taipei Medical University Wan Fang Hospital, School of Medicine, and Taipei Medical University Hospital,
Taipei Medical University, Taipei, Taiwan
d
Laboratory of Biological Psychiatry, Taipei City Psychiatric Center, Taipei, Taiwan
Received 8 October 2002; received in revised form 28 January 2003; accepted 28 January 2003
Abstract
Patients with depression have been extensively reported to be associated with the abnormality of omega-3 polyunsaturated fatty acids (PUFAs), including significantly low eicosapentaenoic acid and docosahexaenoic acid in cell tissue contents (red blood cell membrane, plasma, etc.) and dietary intake. However, more evidence is needed to support its relation. In this study, we conducted an 8-week, double-blind, placebo-controlled trial, comparing omega-3 PUFAs (9.6 g / day) with placebo, on the top of the usual treatment, in 28 patients with major depressive disorder. Patients in the omega-3 PUFA group had a significantly decreased score on the 21-item Hamilton Rating Scale for Depression than those in the placebo group (P,0.001). From the preliminary findings in this study, omega-3 PUFAs could improve the short-term course of illness and were well tolerated in patients with major depressive disorder.
2003 Elsevier B.V./ECNP. All rights reserved.
Keywords: Omega-3 polyunsaturated fatty acids; Major depressive disorder; Taiwan; Fish intake; Nutrition therapy; Diet
1 . Introduction appear to have a lower prevalence of major depressive
disorder (Hibbeln, 1998; Tanskanen et al., 2001).
WHO (World Health Organization) estimates that major Polyunsaturated fatty acids (PUFAs) have been reported
depressive disorder will become the second leading cause recently to be effective in treatment of various psychiatric of disability worldwide by 2020, which is only second to disorders. A mixture of eicosapentaenoic acid (EPA) and ischemic heart disease, and the leading cause in developing docosahexaenoic acid (DHA) in a high dosage was effec-regions (Murray and Lopez, 1997). The annual prevalence tive in a case of a pregnant schizophrenic woman (Su et
of major depressive disorder shows nearly a 60-fold al., 2001). EPA has been reported to have positive effects
variation across countries (Weissman et al., 1996). It is for patients with schizophrenia in several studies (Peet et
similar to the cross-national difference in mortality from al., 2001; Peet and Horrobin, 2002a; Emsley et al., 2002). coronary artery disease, which might suggest that similar However, one study on EPA (Fenton et al., 2001) and the dietary risk factors could be important (Hibbeln, 1998). arm of DHA in another study (Peet et al., 2001) showed no Based on the epidemiological data, societies with a high effect. In their preliminary trial, Stoll et al. (1999)
con-consumption of fish, which contain more omega-3 PUFAs, cluded that omega-3 PUFAs could improve the 4-month
course of illness in patients with bipolar disorder. We further found, from Stoll’s data, that omega-3 PUFAs seem to prevent depression but not mania among the patients
*Corresponding author. Tel.: 4-2206-2121 ext. 5076; fax:
1886-with bipolar disorder (Su et al., 2000).
4-2236-1230 (K.-P. Su), Tel.: 1886-2-2736-1661 (H.-Y. Huang).
The PUFAs are classified mainly into omega-3 (or n23)
E-mail addresses: [email protected] (K.-P. Su),
[email protected](S.-Y. Huang). and omega-6 (or n26) groups, of which the parent
0924-977X / 03 / $ – see front matter 2003 Elsevier B.V./ECNP. All rights reserved. doi:10.1016 / S0924-977X(03)00032-4
essential fatty acid is a-linolenic acid (ALA; C18:3n23) in HRSD score (placebo responders) were excluded. After
and linoleic acid (LA; C18:2n26). As we know that placebo-lead-in phase, participants were randomized to
cerebral cell membranes are composed of certain PUFAs, receive five identical gelatin capsules containing either which cannot be synthesized and must be obtained from omega-3 fatty acids or placebo (olive oil ethyl esters) twice
the diet. Therefore, the abnormalities of PUFA composi- daily in Week 0. Each capsule of omega-3 fatty acid
tion in cell membranes can alter membrane microstructure, concentrate contains 440 mg of eicosapentanoic acid
and then result in abnormal signal transduction and (C20:5v3) and 220 mg of docosahexanoic acid (C22:6v3).
immunological regulation. There are studies revealing All capsules, either v3 fatty acids or placebo, were
abnormalities in PUFA composition may vary in different vacuumed to deodorize, amended by blending with orange
major psychiatric disorders (Chiu et al., 2003a). In depres- flavor, and supplemented with tert.-butylhydroquinone, 0.2
sive disorders, the major abnormality is seen as lower mg / g, and tocopherols, 2 mg / g, as antioxidants. The
erythrocyte membrane omega-3 PUFAs, including signifi- omega-3 fatty acid used in this study is made of the body cant decrease of EPA and DHA levels (Adams et al., 1996; oil of menhaden fishes, produced by China Chemical and
Maes et al., 1996, 1999; Edwards et al., 1998; Peet et al., Pharmaceutical Company in Taipei, Taiwan.
1998). EPA monotherapy was then reported its antidepres- We performed the 21-item HRSD and the brief
adverse-sant effect in a case of treatment-resistant major depressive effect rating in Weeks 21 (placebo-lead-in phase), 0 disorder (Puri et al., 2002). Benefits of omega-3 PUFAs (baseline), 2, 4, 6, and 8. We applied dietary frequency
augmentation with antidepressant medications were also rating scales, recorded food diary and took the blood
reported in the recent studies (Nemets et al., 2002; Peet samples for RBC omega-3 PUFA analysis in Weeks 21
and Horrobin, 2002b), though the dietary frequency and and 8. Participants, receiving medications when entering
erythrocyte omega-3 fatty acid composition were not this study, continued the same medications in constant
measured then. In addition, we suggest that the patients in dosages whether they were in the therapeutic range. The
the placebo group should also receive tertiary only medication allowed for addition were oral sedatives /
butylhydroquinone and tocopherols as they did in the hypnotics (lorazepam or zolpidem) for intolerable anxiety
omega-3 fatty acids group, to avoid the possible therapeu- and insomnia. Participants on any antipsychotics or mood tic effect from these compound as a confounding factor stabilizers are excluded in this study.
(Su et al., 2000). Data were analyzed with the SPSS statistical software.
To provide more evidence to uncover the relation The effect of the addition of omega-3 PUFAs was
ex-between pathogenesis in major depression and omega-3 amined by repeated-measures analysis of variance with
PUFAs and then establish an efficient treatment for it, we time as repeated factor, treatment (placebo or omega-3 conducted an 8-week, preliminary double-blind, placebo- PUFAs) as independent factor, and clinical data (age, onset controlled trial. Our hypothesis is that giving a high dosage of age, body mass index, duration of current episode,
of DHA and EPA is effective when treating depressive numbers of previous depressive episodes, duration of
symptoms. antidepressant treatment before enrollment, dose of
antide-pressants at inclusion, and RBC omega-3 PUFA com-positions) as covariates. Treatment differences in the score
2 . Method of severity were assessed by Mann–Whitney test
(Wilcox-on signed rank test). The difference is c(Wilcox-onsidered statisti-Participants were outpatients, ranging from 18 to 60 cally significant if P value is equal to or greater than 0.05. years old, referred by Taipei Medical University–Wan
Fang Hospital. They were enrolled if they met the
follow-ing criteria: (1) they were diagnosed with DSM-IV as 3 . Results
major depressive disorder and had no other comorbid Axis
I or Axis II psychiatric disorders, (2) they were rated over Thirty-two patients were enrolled in this study, but four
18 on the 21-item Hamilton Rating Scale for Depression were excluded at the stage of placebo lead-in.
Twenty-(HRSD), (3) there was no change in their medications or eight patients were randomized to either omega-3 PUFAs
psychotherapy 4 weeks before the enrollment, (4) they had (n514) or placebo (n514), while 22 patients (12 of the
to be physically healthy under comprehensive evaluations omega-3 group and 10 of the placebo group) completed
of medical history, physical examination and laboratory this 8-week study. Six patients dropped out prior to Week
tests, and (5) they were competent to understand the study 8. Of the six, two received omega-3 (one was lost in
and were given written informed consents. The Institution- follow-up and the other was lost due to noncompliance),
al Review Board of Taipei Medical University–Wan Fang and four received placebo (three were lost in follow-up
Hospital has approved this research before it underwent. and the other was lost due to noncompliance). Table 1
Before randomized grouping, all the qualified particip- shows no statistical differences in demographic, clinical
ants received single-blind placebo capsules for 1 week (in characteristics or omega-3 PUFA composition in RBC.
T able 1 mean post-treatment value6S.D. of DHA (5.863.4, n57) Demographic and clinical characteristics of patients who received omega- of patients in omega-3 PUFA group was significantly 3 PUFA treatment (v3) or placebo
much higher (P50.03) than that of (2.462.6, n57) in the
a a
v3 Placebo P period of pre-treatment. The mean post-treatment
(n512) (n510)
value6S.D. of EPA (2.762.5, n57) of patients in omega-3
Age (years) 35.2611.6 42.3610.7 0.25 PUFA group is not significantly different (P50.87) from Sex (no. F:M) 10:2 8:2 0.92 that of in the period of pre-treatment (2.563.1, n57). Body mass index 21.464.6 23.062.7 0.10
There is no significant difference between pre- and
post-Age of onset (years) 30.6610.7 35.168.6 0.31
treatment levels of DHA or EPA for participants in placebo
Duration of current episode 22.8615.5 21.5613.0 0.97
(weeks) group (n56).
No. of previous depressive 2.561.0 2.361.2 0.54 episodes
Duration of antidepressant 9.364.9 10.467.5 0.87 treatment before enrollment
4 . Discussion
Dose of antidepressants while 23.068.2 17.164.9 0.19 being enrolled (fluoxetine
b
equivalent) Although this study is limited by its small sample size
RBC omega-3 PUFA and the possible confounding factor of uncontrolled
com-compositions
bined medications, the findings do provide a rationale
EPA 3.063.2 4.463.4 0.46
perspective to conduct further large-scale trials of omega-3
DHA 2.962.8 2.262.0 0.78
c
HRSD score PUFAs monotherapy.
Pretreatment (week 0) 22.563.9 22.163.9 0.77 It is interesting to notice that EPA, but not DHA, Posttreatment (week 8) 8.963.7 15.763.2 0.001 improves schizophrenic symptoms (Peet et al., 2001; Peet
a
Mean6SD unless otherwise specified. Mann–Whitney U-test, except and Horrobin, 2002a; Emsley et al., 2002) and major
where otherwise noted. depressive disorder (Marangell et al., 2000; Nemets et al.,
b
The antidepressant doses are converted into fluoxetine equivalents
2002; Peet and Horrobin, 2002b) as well. Furthermore,
according to practice guideline by American Psychiatric Association
EPA, but not DHA, has been reported to be an effective
(2000).
c substrate for cyclooxygenase and inhibitor for
phosphlip-HRSD, Hamilton Rating Scale for Depression.
ase A2, which may play an important role in psycho-physiology of depression (Peet and Horrobin, 2002b). from medications. The dosages of fluvoxamine (n52, 1 in However,Maes et al. (1996, 1999) reported that patients omega-3 group), trazodone (n52, 1 in omega-3 group), or with major depression had a lower level of EPA and total
moclobemide (n55, 3 in omega-3 group) used were n23 PUFAs and elevated ratio of ecosapentaenoic acid
converted into fluoxetine (n511, 6 in omega-3 group) (EPA; 20:5n23) / docosahexaenoic acid (DHA; 22:6n23)
equivalents (American Psychiatric Association, 2000), and in serum cholesteryl esters and phospholipids. Similar there were no difference in the doses of antidepressant use. findings were revealed in terms of fatty acid compositions There is no difference in the dietary frequency on fish on erythrocyte membrane (Adams et al., 1996; Edwards et
intake or total unsaturated fatty acids in 24-h dietary recall al., 1998; Peet et al., 1998). These results implied that the and 3-day dietary record of participants in both groups as deficiency of DHA is more prominent than that of EPA.
well. Furthermore, EPA exists with a very small quantity in
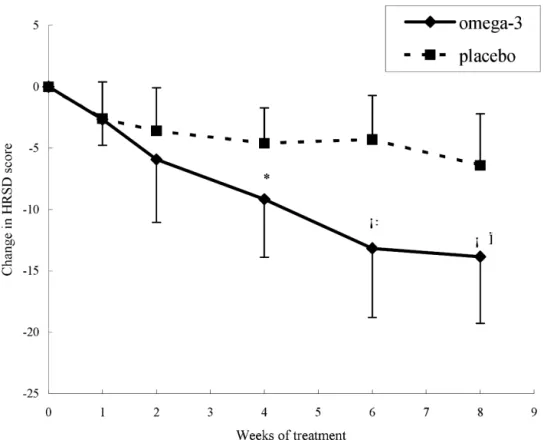
As shown in Fig. 1, participants in omega-3 PUFA neuronal membranes, while DHA is a major constituent of
group had significant differences in the HRSD score from neuronal membrane phospholipid, and it plays an
im-the fourth week after treatment. The percentage of reduc- portant role in functioning of neurotransmitters, including
ing HRSD total scores in omega-3 PUFA group was serotonin (Hibbeln and Salem, 1995, Hibbeln et al., 1998).
significantly much greater than that of in placebo group. In the frontal cortex, rats with low brain concentrations of
The difference was unrelated to the demographic and DHA were found to have a 44% increase in serotonin-2A
clinical covariates. One participant (in omega-3 PUFA receptor number (Delion et al., 1994), which is a potential group) had mild excitement during Weeks 1 and 2, another marker of reduced serotonin function. In this study, it is
one (in omega-3 PUFA group) had mild diarrhea during rational to use combination for omega-3 fatty acid
treat-Weeks 2 and 4, and one (in placebo group) had insomnia ment. However, it needs further investigation to see if EPA
during Weeks 2 and 4. None of them did have any major is more effective than DHA or EPA / DHA combination
adverse effects, such as abnormal bleeding time. when using as antidepressants.
The effect of omega-3 PUFA and placebo supplement With the previous findings of abnormal PUFA levels in
on RBC fatty acid composition were also examined. The depressive patients (Adams et al., 1996; Maes et al., 1996,
RBC fatty acid composition of both pre- and post-treat- 1999; Edwards et al., 1998; Peet et al., 1998) and
ment was available only for seven participants in omega-3 epidemiological findings (Hibbeln, 1998; Tanskanen et al.,
Fig. 1. Evolution of the 21-item Hamilton Rating Scale for Depression (HAM-D) score in depressive patients treated additionally with omega-3 PUFAs or
§
placebo during the trial period. The significant differences were noted at week 4 (z522.04, P50.0043)*, 6 (z523.20, P50.001) and week 8 (z523.34,
†
P50.001) by Mann–Whitney U-test. The rate of reduction in HRSD total scores in omega-3 PUFA group is significantly greater than that in placebo
group (F56.62, P50.024) by repeated-measures analysis of variance.
provide more evidences to support phospholipid hypothesis lack of teratogenicity. Hopefully, the clinical trial of
in depression (Horrobin and Bennett, 1999). omega-3 PUFAs may help shed some light on the
under-The mechanism of omega-3 PUFA augmentation effect standing of the disease pathophysiology of major
depres-on depressidepres-on is still unknown. One of the hypotheses is sive disorder and may benefit special psychiatric
popula-that omega-3 PUFAs can normalize the altered membrane tions, such as pregnant and lactating women (Su et al.,
microstructure and neurotransmission in patients with 2001; Chiu et al., 2003b).
depression. For example, the changes in brain fatty acid concentration, induced by chronic dietary omega-3 fatty acid deficiency alter serotonergic and dopaminergic
neuro-A
cknowledgements transmission (Delion et al., 1994) and induces an increase
in 5-HT2 and decrease in D2 frontal cortex receptor The work was supported by the grants of NSC
90-2314-density (Delion et al., 1996). The upregulation of
5-B-109-005, NSC 90-2320-B-039-042 and NSC 91-2320-B-HT2A / C is thought to play a role in the pathophysiology of 039-010 from the National Science Council, and China depression (Maes and Meltzer, 1995). Biochemical studies
Chemical and Pharmaceutical Company, Taipei, Taiwan. have shown that omega-3 PUFAs increased CSF 5-HIAA
The authors thank Miss Chin-Hua Liu for data collection. concentrations and somatotrophin release (Nizzo et al.,
1978), which is usually seen with the improvement of depressive symptoms. The other hypothesis is that
omega-3 PUFAs play an important role in the mechanism of mood R eferences stabilization by targeting parts of the ‘arachidonic acid
cascade’ (Rapoport and Bosetti, 2002). A dams, P.B., Lawson, S., Sanigorski, A., Sinclair, A.J., 1996. Arach-idonic acid to eicosapentaenoic acid ratio in blood correlates positively
Although there is not much incentive for pharmaceutical
with clinical symptoms of depression. Lipids 31, S157–S161.
companies to support a research of a non-patentable
A
merican Psychiatric Association, 2000. Practice guideline for the
compound, such as omega-3 PUFAs, further data collec- treatment of patients with major depressive disorder (revision). Am. J. tion are crucial for both humanistic and scientific reasons Psychiatry 157 (Suppl. 4), 1–45.
Shen, W.W., 2003a. Polyunsaturated fatty acid deficit in patients with phospholipids and cholesteryl esters of depressed patients. Psychiatr. bipolar mania. Eur. Neuropsychopharm. 13 (2), 99–103. Res. 85, 275–291.
C hiu, C.C., Huang, S.Y., Shen, W.W., Su, K.P., 2003b. Omega-3 fatty acid M arangell, L.B., Zboyan, H.A., Cress, K.K., Vogelson, L., Puryear, L.J., monotherapy for a pregnant patient with major depressive disorder. Jensen, C., Arterburn, L., 2000. A double blind, placebo-controlled Am. J. Psychiatry 160 (2), 385. study of docosahexaenoic acid in the treatment of depression [ab-D elion, S., Chalon, S., Herault, J., Guilloteau, D., Besnard, J.C., Durand, stract]. Inform. 11, S78.
G., 1994. Chronic dietary alpha-linolenic acid deficiency alters dopa- M urray, C.J.L., Lopez, A.D., 1997. Alternative projections of mortality minergic and serotonergic neurotransmission in rats. J. Nutr. 124, and disability by cause 1990–2020: Global Burden of Disease Study.
2466–2475. Lancet 349, 1498–1504.
D elion, S., Chalon, S., Guilloteau, D., Besnard, J.C., Durand, G., 1996. N emets, B., Stahl, Z., Belmaker, R.H., 2002. Addition of omega-3 fatty Alpha-linolenic acid deficiency alters age-related changes of dopa- acid to maintenance medication treatment for recurrent unipolar minergic and serotonergic neurotransmission in the rat frontal cortex. depressive disorder. Am. J. Psychiatry 159, 477–479.
J. Neurochem. 66, 1582–1591. N izzo, M.C., Tegos, S., Gallamini, A., Toffano, G., Polleri, A., Massarot-E dwards, R., Peet, M., Shay, J., Horrobin, D., 1998. Omega-3 polyunsatu- ti, M., 1978. Brain cortex phospholipids liposomes effects on CSF rated fatty acid levels in the diet and in red blood cell membranes of HVA, 5-HIAA and on prolactin and somatotropin secretion in man. J. depressed patients. J. Affect. Disord. 48, 149–155. Neural. Transm. 43, 93–102.
E msley, R., Myburgh, C., Oosthuizen, P., van Rensburg, S.J., 2002. P eet, M., Murphy, B., Shay, J., Horrobin, D., 1998. Depletion of omega-3 Randomized, placebo-controlled study of ethyl-eicosapentaenoic acid fatty acid levels in red blood cell membranes of depressive patients. as supplemental treatment in schizophrenia. Am. J. Psychiatry 159, Biol. Psychiatry 43, 315–319.
1596–1598. P eet, M., Brind, J., Ramchand, C.N., Shah, S., Vankar, G.K., 2001. Two F enton, W.S., Dickerson, F., Boronow, J., Hibbeln, J.R., Knable, M., double-blind placebo-controlled pilot studies of eicosapentaenoic acid
2001. A placebo-controlled trial of omega-3 fatty acid (ethyl in the treatment of schizophrenia. Schizophr. Res. 49, 243–251. eicosapentaenoic acid) supplementation for residual symptoms and P eet, M., Horrobin, D., 2002a. A dose-ranging exploratory study of the cognitive impairment in schizophrenia. Am. J. Psychiatry 158, 2071– effects of ethyl-eicosapentaenoate in patients with persistent
schizo-2074. phrenic symptoms. J. Psychiatr. Res. 36, 7–18.
H ibbeln, J.R., Salem, N., 1995. Dietary polyunsaturated fats and depres- P eet, M., Horrobin, D., 2002b. A dose-ranging study of the effects of sion: when cholesterol does not satisfy. Am. J. Chin. Nutr. 62, 1–9. ethyl-eicosapentaenoate in patients with ongoing depression despite H ibbeln, H.R., 1998. Fish consumption and major depression. Lancet 351, apparently adequate treatment with standard drugs. Arch. Gen.
Psychi-1213. atry 59, 913–919.
H ibbeln, H.R., Umhau, J.C., Linnoila, M., George, D.T., Ragan, P.W., P uri, B.K., Counsell, S.J., Richardson, A.J., Horrobin, D.F., 2002. Shoaf, S.E., Vaughan, M.R., Salem, N., 1998. A replication study of Eicosapentaenoic acid in treatment-resistant depression. Arch. Gen. violent and nonviolent subjects: cerebrospinal fluid metabolites of Psychiatry 59, 91–92.
serotonin and dopamine are predicted by plasma essential fatty acids. R apoport, S.I., Bosetti, F., 2002. Do lithium and anticonvulsants target Biol. Psychiatry 44, 243–249. the brain arachidonic acid cascade in bipolar disorder? Arch. Gen. H orrobin, D.F., Bennett, C.N., 1999. Depression and bipolar disorder: Psychiatry 59, 592–596.
relationships to impaired fatty acid and phospholipid metabolism and S toll, A.L., Severus, W.E., Freeman, M.P., Rueter, S., Zboyan, H.A., diabetes, cardiovascular disease, immunological abnormalities, cancer, Diamond, E., Cress, K.K., Marangell, L.B., 1999. Omega 3 fatty acids ageing and osteoporosis. Possible candidate genes. Postaglandins in bipolar disorder: a preliminary double-blind, placebo-controlled Leukot. Essent. Fatty Acids 60, 217–234. trial. Arch. Gen. Psychiatry 56, 407–412.
M aes, M., Meltzer, H.Y.M., 1995. The serotonin hypothesis of major S u, K.P., Huang, S.Y., Shen, W.W., 2000. Is omega 3 fatty acids beneficial depression. In: Bloom, F.E., Kupfer, D.J. (Eds.), Psychopharmacology, in depression but not mania? Arch. Gen. Psychiatry 57, 716. The Fourth Generation of Progress. Raven Press, New York, pp. S u, K.P., Huang, S.Y., Shen, W.W., 2001. Omega-3 fatty acids as a 933–941. psychotherapeutic agent for a pregnant schizophrenic patient. Eur. M aes, M., Smith, R., Christophe, A., Cosyns, P., Desnyder, R., Meltzer, Neuropsychopharm. 11, 295–299.
H.J., 1996. Fatty acid composition in major depression: decreased T anskanen, A., Hibbeln, J.R., Hintikka, J., Haatainen, K., Honkalampi, omega three fractions in cholesteryl esters and increased C20: 4 omega K., Viinamaki, H., 2001. Fish consumption, depression, and suicidality 6 / C20:5 omega 3 ratio in cholesteryl esters and phospholipids. J. in a general population. Arch. Gen. Psychiatry 58, 512–513. Affect. Disord. 38, 35–46. W eissman, M.M., Bland, R.C., Canino, G.J. et al., 1996. Cross-national M aes, M., Christophe, A., Delanghe, J., Altamura, C., Neels, H., Meltzer, epidemiology of major depression and bipolar disorder. J. Am. Med.