行政院國家科學委員會專題研究計畫 成果報告
社區服務學習課程的設計執行與評估〈2/2〉
計畫類別: 個別型計畫 計畫編號: NSC91-2516-S-002-001- 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院家庭醫學科 計畫主持人: 梁繼權 共同主持人: 謝博生,陳慶餘,劉文俊 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 92 年 11 月 3 日
目錄 Contents
目錄
--- 1中文摘要
--- 2英文摘要
--- 4前言
--- 6研究目的
--- 8文獻探討
--- 9研究方法
--- 10結果
--- 12討論
--- 14參考文獻
--- 15附表
--- 17中文摘要
醫學教育中,如何加強學生對社會的關懷,與了解社會的需要是重要的課 題。服務學習是具有服務(Service)與學習(Learning)兩種活動的過程,透過服務學 習可以培養人性關懷、社會關懷與公民情操,是一種改變觀念與態度的學習方式。 服務學習是一種透過經驗學習的教育方法,學生在一個經過特別安排的學習 環境下,從事與人及社區需求有關之工作,以增進學生的學習能力與自我成長、 反省(Reflection)與互惠(Reciprocity),是服務學習的關鍵概念。反省是一種把經 驗與動機,經驗與學習相連繫的教學方法,反省是學習經驗的一種整理與回饋, 從經驗中萃取與沈澱出學問。而互惠是服務者與受服務者的相互學習與彼此為 師,服務者對社區產生認同與責任,而受服務者則學會對自己的需求負責,發展 出自我解決問題的能力,達到學生與社區互利的結果。 服務學習讓學生有機會去學習收集資料的能力、有創意的解決問題、有組織 的團隊工作、有效的溝通、合理的決策、談判與折衷技能。除此之外,還可以培 養學生自動自發、富有彈性、適應能力、開放的想法與同理心等特質,在職等訓 練方面,可以培養醫師、律師、公務員、企業管理人員的社會責任心。 本研究乃利用醫五學生在「家庭、社區與醫療」的社區實習課程,發展成為 一個符合服務學習理論的社區服務學習,並評估課程可行性、對社區及學生的影 響等。本研究利用自填式問卷收集資料。前測問卷(Social Attitude Scale, SAS)在學 生開始社區服務課程前一週施測,內容分為六個向度,共有 27 題。後側問卷在 學 生 完 成 兩 週 課 程 回 台 北 的 途 中 施 測 , 問 卷 分 兩 部 分 , Program Character Scale(PCS)及 Ability Scale(AS)。PCS 的內容分為六個向度,共有 25 題;AS 的 內容分為 7 個向度,共有 22 題。三個問卷皆採用 Likert 五點評量計分。 在 2001 及 2002 兩個學年度中共有 249 位醫五學生參與本課程並完成評估, 男生佔大多數共有 195 位(78.3%);女生在「社區效能」及「服務價值」兩項 得分較男生低,其餘並無男女性別差異。 學生對於社會服務普遍有正向的態度,但對於日後從事社會服務工作則有較 保留的態度。對於社區服務課程的特質方面,學生皆有正面的評價,認為本課程 達到評估中所要求的標準,其中又以老師對學生作口頭及書面之反省最受肯定。 在技能學習方面,以溝通技巧與發現社會問題能力兩方面,是學生認為學習最多 的部分。 在相關分析方面,對社會服務學習有較多預期和重視社會服務價值的學生, 對課程的學習環境與社區參與兩項特質有較高的評價。 對於社區服務的態度也會影響部分技巧的學習效果,課程特質與學習效果具 有高度相關,唯一相關較低的項目是批判思考能力,只和學習環境與內容的變因 性有關。 本研究發現社區服務學習是可以為學生所接受,而且學生可以從中學習得到
一些傳統課程所無法提供的知識技能,學生對社會服務的態度會影響他們對課程 的評價與學習教學,良好的學習效果與課程是否能滿足社區服務學習的各項必須 具備的性質有密切關係。 本研究結果可以作為本課程改進,及其他相關課程在設計上及課程評估上的 參考。 關鍵詞:醫學教育、服務學習、社區醫學
英文摘要
The reinforcement of social awareness and responsibility are two important issues in medical education. Service-learning is a learning activity with a balance between service to the community and academic learning and that each activity enhances the other for all participants.
Service-learning is learning from experience. An educative experience is one that fosters student development by capturing student interest and passion. Experience enhances understanding and understanding leads to more effective action. Real-world learning tends to be more cooperative or communal than individualistic, link personal and interpersonal development with academic and cognitive development. Service-learning also enhances students' social problem solving skill, critical thinking, and educates for civic responsibility.
Reflection and reciprocity are two critical components of service-learning. Reflection is a process explicitly designed to foster learning and development. It is the link that ties student experience in the community to academic learning. Reciprocity is something gained by the server and people being served through the process of service-learning. Through reciprocity, students develop a greater sense of belonging and responsibility as member of a larger community. Community members being served learn how to take responsibility for their own needs and become empowered to develop mechanism and relationship to address them.
From service-learning, students learning to gather information, creative problem-solving, organized team work, effective communication, reasonable decision-making. It can foster initiation, elasticity, adaptability, opened thinking, and empathy. For vocational training, it can foster social responsibility in occupations such as physician, lawyer, civil servant, and business manager, etc.
This study is to design, implement, and evaluation a service-learning curriculum for grade 5 medical students participate in community education program located in remote villages in Dou-Liou and Lu-Ku community.
Study instruments included Social Attitude Scale (SAS), Program Characteristic Scale (PCS) and Ability Scale (AS). SAS has 27 items covering six dimensions about student’s attitude on social issues and social service. It was rated by the students in the week before the beginning of the community service activities. Program Characteristic Scale (PCS) and the Ability Scale (AS) were rated at the end of the community rotation. The PCS contains 6 dimensions that measured the quality of the community placement and the academic linkage of the community experience and learning. The AS measured the skills acquired in the community-service learning program. It contains 7 dimensions.
Two hundred and forty nine 5-year medical students finished the community training programs and completed the questionnaire during the 2001 and 2002 academic year. Of them, 7.3% were male students. Gender differences were observed in two of the SAS dimensions (community efficacy and value) but not among the PCS and AS. Most of the medical students have a positive attitude towards social service and citizenship but conservative towards taking the role and commitment to serve people in the community by themselves. For the evaluations after the community service-learning program, most of the students agreed that the program fulfilled all dimensions of the PCS. They also agreed that they have gained the abilities they supposed to learning. Students attitude towards social service were related to their rating of the PCS and AS on several dimensions. Program characteristics which were measured by the PCS had a moderate to high correlation with the abilities learned in the community service program.
We found that community service program can become an effective way to teach community medicine and social responsibility to medical students. Both the students’ attitude and program characteristics are important factors for learning in the community-service learning curriculum.
前言 Introduction
Universities and medical schools have dual responsibilities: academic advancement and social accountability. By fulfilling their social accountability, medical schools should prepare medical professionals for the prospective needs and demands of society. While our present medical educational system was success in training technically competent physicians, our students lack the moral commitment, social responsibility, and human compassion as they are socialized into the profession.
The injection of community elements into our medical curriculum may be an antidote to the treatment of what Charles Taylor calls the three “malaise of modernity”. Service-learning is defined as a structured learning experience that combines community service with explicit learning objectives, preparation, and reflection. It is a strategy for preparing community responsive and competent health professionals and at the same time, changing the relationship between communities and academic schools, foster citizenship, and achieving social change .
Community service has been shown to have positive effect on the training of health professionals since long time ago. In Taiwan, there were many different types of community service provided by students in medical schools. Most of these programs were initiated by student societies aiming to educate and to provide help to medically under-service community and minorities. In this kind of programs, schools and faculties were served as consultants and provided logistic supports to the service activities. However, nearly all of these community service programs were not part of the formal curriculum and had no structured design and evaluation. Most of the learning was arbitrary and the students did not receive formal reflections from faculties.
Three years ago, the National Taiwan University College of Medicine (NTUCM) began the first community-service curriculum. The establishment of this program was initiated by the major earthquake on the night of September 21, 1999. Shortly after the insult, NTUCM affiliated hospital responded to the request of the health authority and provided emergency medical service to the earthquake damage area in Nan-Tou. Since it was a very good learning opportunity for medical students, a community medicine program was set up for 5-year medical students. Students can select to go to an earthquake damage area to work with the emergency medical team under the supervision of a responsible faculty for two weeks during their family medicine rotation or to continue their formal family medicine program. This community learning experience was highly appreciated by the students and many students called for a formal program in their curriculum. In the next academic year, a six weeks required course, “Family, society and medicine”, for the 5-year medical students was
established. The objectives of this course are to provide basic understanding how family and community affect health and diseases, differences between community and hospital medicine, and the relationship of science and humanity in clinical medicine. In this course, all students are required to take a two weeks community service program in one of the two selected communities (Dou-Liou and Lu-Ku). Lu-Ku community is a small village in the Nan-Tou County located at the middle mountain area of the island. This tea-tree planting village was severely damaged during the 1999 earthquake. After the acute phrase of the disaster and the withdrawal of the emergency medical team, the medical college continued to give support to the re-construction of the community. Dou-Liou was a small town in Yuen-Lin County located at the mid-west coast of Taiwan main island. The relationship of the local community and the medical college was built on the project of setting up a new campus in the community. This project began the dialogue between the two sides on how to address community health care needs and opened a venue for the joint program of community service learning. The project promoted a throw of faculties and medical professional manpower from the NTUCM and the affiliated hospital to the community. On the other side, the community gave full logistic supports to the students’ service-learning activities and provided community health workers as tutors. These community service programs were designed and organized by a jointed effort of the community health center, the local practitioners, and faculty of the family medicine department of NTUCM. Community tutors were appointed as part-time faculty of the medical college. Their roles are to coordinate all the community service activities, give immediate reflections to the students, keep students engage to their work, and maintain a safe environment. All students live in the community during the two weeks of community placement. They work side-by-side with the community health workers to give home care to the sick people, or work independently in the community after careful planning with the responsible faculties and the community tutors. Most of the students found the community service program is the most interesting part of the curriculum.
研究目的
This study was designed to understand the students’ attitude about community service before they attained the program and to evaluate their learning experiences after two weeks of community service.
文獻探討
服務學習(Service Learning)顧名思義是具有服務(Service)與學習(Learning)兩 種活動的過程。有趣的是,過去有關服務學習並沒有一個統一的看法,而不同的 服務學習課程也有很大的差異,有些是服務多於學習,有些是學習重於服務,而 且規劃方式沒有一定的標準。一個理想的服務學習課程依 Sigmon(1996)的意見, 應該是服務與學習兩者有平衡的比重,不但兩者兼顧,同時要達到以學習指導服 務,由服務加強學習的相得益彰的效果。 認知心理學家發現,在一般課堂學習中,學生往往無法把課堂上所學到的知 識與理論應用到實際的問題解決上,就算所學到的知識與新的問題有很多相似的 地方,在應用的時候也常常會感到十分困難(Bransford, 1993)。而透過現實狀況 下的學習則有較多的好處,如比較易於達到團隊合作與學習人際溝通的效果,學 會使用各種工具而非單純的思考,能夠把事件放在一個複雜的、實際的環境中考 慮而非處理單獨的事件,應用特定的、與實際狀況有關聯的知識而非一般抽象的 理論等。在複雜的現實環境中,學生常常遇到困難,這些困境是在光讀書時無法 想像與考慮到的,但這些困難會讓學生有機會了解自己能力的限制,給與學生進 一步學習的壓力與動力。而服務學習的目標是讓學生在真實的環境中學習,有機 會和別人合作,透過行動與回饋來達到社區的實質目標,同時增加對自己的了解 與能力。研究方法 Method
In the “Family, society and medicine” program, students are divided into small groups of about 10 to 12 people for two weeks of community training. There are two community training sites in this program. Students can choose one community as their learning site. The capacity of the each community program was about 6 students in each rotation.
Before and after the community rotation, students were asked to complete a questionnaire as a part of their evaluation. The pre-training and post-training questionnaire was modified and culturally adapted from the Fund for the Improvement of Postsecondary Education (FIPSE) survey instrument.
Pre-training questionnaire (Social Attitude Scale, SAS) included 27 items covering six dimensions about student’s attitude on social issues and social service. The “citizenship” dimension has 11 items probing the feeling of connectedness with the community (4 items), a sense of personal efficacy in affecting community issue (4 items), and a belief that the community can solve its problems effectively (3 items). The “locus of community problems” dimension has 3 items. It measured whether students take social problems as a systemic issue or blame solely to the individual facing the problem. The “social justice and political structure” dimension has 5 items measured how student viewed social justice, policy, and government agency affected the community. The “personal value” dimension has 5 items measured how student valued their role and commitment to serve people. The “personal gains” dimension has 2 items measured how students expected to achieve after the community rotation. The “tolerance” dimension has one item measured the student’s ability to work with others in the community. Principle factor analysis of the “citizenship” subscale obtained 2 factors that explained 42.2% of the total variance. All community connectedness items were grouped in factor 1 and all except two personal efficacy items were grouped in factor 2. The community efficacy items were dispersed into two factors.
The post-training questionnaire was divided into two parts, the Program Characteristic Scale (PCS) and the Ability Scale (AS). Information was collected at the end of the community rotation directly from the students.
The PCS contains 6 dimensions that measured the quality of the community placement and the academic linkage of the community experience and learning. These six dimensions are: Reflection/discussion (6 items), reflection/writing (3 items), placement quality (12 items), community voice (2 items), application (2 items), and diversity (one item). Principle factor analysis of the whole scale obtained 3 factors that explained 52.2% of the total variance. Except 2 items, the entire
reflection/discussion and reflection/writing dimension grouped in factor 1. The placement items and the other items grouped into factor 2 and 3. Internal reliability study reviewed a α value of 0.91 for the whole scale, 0.88 for the reflection/discussion, 0.75 for the reflection/writing, and 0.84 for the placement quality.
The AS measured the skills acquired in the community-service learning program. It contains 7 dimensions: Leadership skills (4 items), community skills (5 items), tolerance (7 items), prospective thinking (2 items), critical thinking (one item), identify social issues (one item) and action skills (2 items). Principle factor analysis of the whole scale obtained 4 factors that can explain 55.8% of the total variance. Four out of 5 community skills items, 4 out of 7 tolerance items, and 3 out of 4 leadership skills items grouped in the first three factors respectively. Internal reliability test reviewed a α value of 0.92 for the whole scale, 0.73 for the leadership dimension, 0.77 for the communication dimension, and 0.79 for the tolerance dimension.
All items in the questionnaires were answered in a 5-point Likert-type scale with the highest point for “very agree” and the lowest point for “very disagree”. Items with an opposite meaning from the majority of the items in the same dimension were scored in an opposite direction with the highest point for “very disagree”. The mean score of each dimension was calculated by adding the score of all the items in the dimension and divided by the numbers of items in that dimension.
結果 Results
Two hundred and forty nine 5-year medical students finished the community training programs and completed the questionnaire during the 2001 and 2002 academic year. Of them, 126 students (104 boys and 22 girls) were in the Dou-Liou program and 123 students (91 boys and 32 girls) were in the Lu-Ku program. Gender differences were observed in two of the SAS dimensions but not among the PCS and AS. Girls have lower scores in the community efficacy dimension (3.28±0.45 vs. 3.48±0.49, P>0.01) and value dimension (2.81±0.50 vs. 3.06±0.59, P>0.01) than boys.
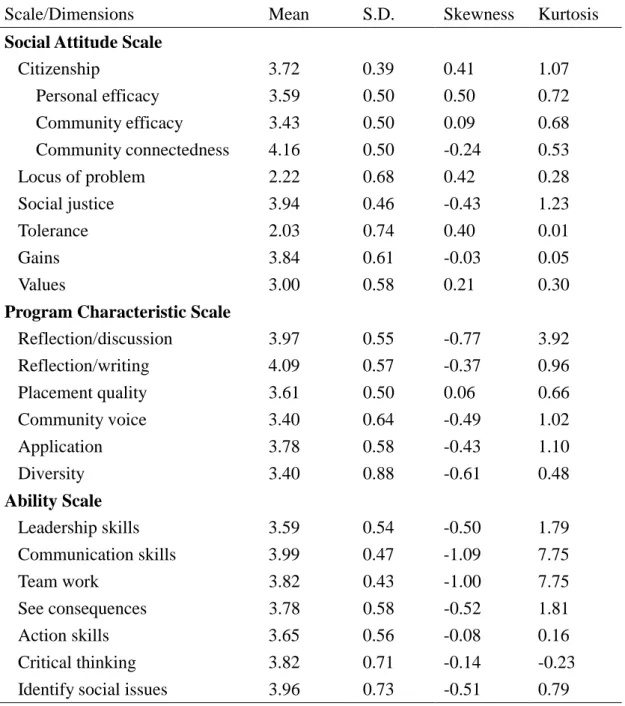
Table 1 revealed the descriptive statistics of the SAS, PCS and AS. For the SAS, community connectedness has the highest mean score (4.16±0.50) among all social attitude items. Except for the personal value dimension that has a mean score of 3.0, all positive attitude dimensions have a mean score of more than 3.4 and all negative attitude dimension have a mean score of less than 2.3. These results indicated that most of the medical students have a positive attitude towards social service and citizenship but conservative towards taking the role and commitment to serve people in the community by themselves. For the evaluations after the community service-learning program, all dimensions of the PCS have a mean score of equal and greater than 3.4. It implied that from the students point of view, the quality of Dou-Liou and Lu-Ku community service-learning program have reached a more than average level in all characteristic dimensions especially the reflection/writing and reflection/discussion dimension which have mean scores of more than 3.9. For the evaluation of what the students have learnt from the community service-learning program, all dimensions in the AS have mean scores more than average level. Two dimensions, the communication skills and ability to identify social issues, have mean scores of more than 3.9.
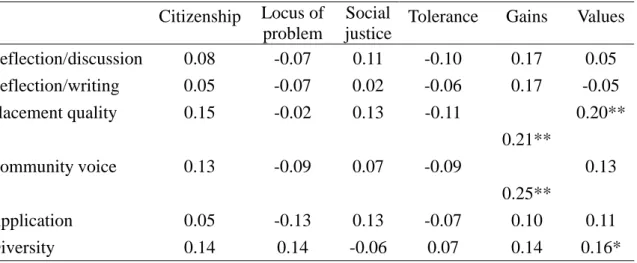
Table 2 presented the correlations between the dimensions of the SAS and PCS. Learning gains from community service are moderately correlated to the placement quality and community voice dimension. The value dimension is moderately correlated to the placement quality dimension and weakly correlated to the diversity dimension. All other dimensions of the two scales are not statistically correlated.
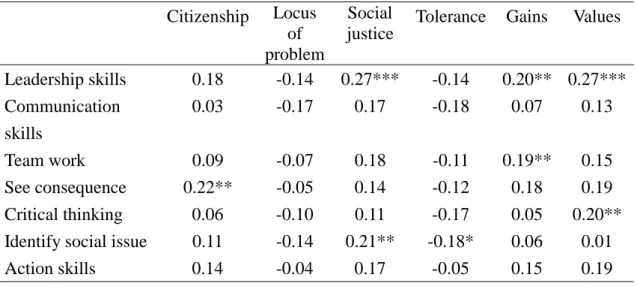
Table 3 presented the correlations between the dimensions of the SAS and AS. Citizenship dimension is moderately correlated to the ability to see consequence. Social justice is moderately correlated to leadership skills and ability to identify social issue. Tolerance is weakly and negatively correlated to ability to identify social issue. Learning dimension is moderately correlated to leadership and weakly correlated to team work. The values dimension is moderately correlated to leadership skills and
critical thinking dimension.
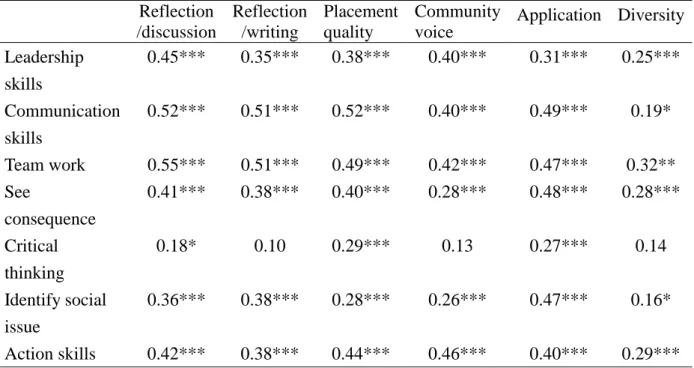
Table 4 presented the correlation between the dimensions of the PCS and AS. Leadership skills dimension is highly correlated to all dimensions of the PCS. Communication skills dimension is weakly correlated to the diversity dimension but highly correlated to the other dimensions of the PCS. The dimension of teamwork skills is highly correlated to all dimensions of the PCS. The ability to see consequence and action skills dimension are moderately and highly correlated to the dimensions of the PCS. The ability to identify social issue is weakly correlated to the diversity dimension but is moderately and highly correlated to all other dimensions in the PCS. Critical thinking is weakly correlated to reflection/discussion dimension and moderately correlated to the placement quality and application dimension. This result indicated that the quality of the community service-learning program is highly related to the results of students’ learning in the community.
討論 Discussion
The purpose of Community service learning in medical education is to prepare community responsible health professionals. It should equipped the students the ability and experiences in working within a community, understanding community health problems, knowing community resources and cooperating with the community to make necessary changes. In order to reach our learning objectives, the design and implementation of the community learning program is of upmost important. There were very few studies evaluating the community-service learning curriculum in the literature and most of these studies were qualitative.
Our results revealed that most of the 5-year medical students has positive attitude towards community service. However, girls were less aggressive than boys for taking the role of community service. It may due to the traditional role of female in Chinese culture that women should serve their family. From the students’ point-of-view, the community service curriculum has reached an above average level in all community service characteristics especially in the reflection/discussion given by faculties and tutors. In this study, we discovered that for those who had higher motivation to gain from the service learning and had a personal value to serve people were more satisfied with the community service program. These students were also gained more from the program. They developed more leadership skills, team works, and critical thinking ability. Characteristics of the program are highly associated with the ability learned from the program. Placement quality and application are important to all of the acquired abilities and they are the only two program characteristics related to the learning of critical thinking ability.
In summary, we found that both the students’ attitude and program characteristics are important factors for learning in the community-service learning curriculum.
參考文獻 Reference
1. Boelen C. Prospects for change in medical education in the twenty-first century. Acad Med. 1995;70:S21-8.
2. Taylor C. The Ethics of Authenticity. Cambridge, MA: Harvard University Press, 1992.
3. Seifer SD. Service-learning: Community-campus partnerships for health professions education. Acad Med. 1998;73:273-7.
4. Quinn SC, Gamble D, Denham A: Ethics and community-based education: balancing respect for the community with professional preparation. Fam Community Health 2001;23:9-23.
5. Howe A: Patient-centred medicine through student-centred teaching: a student perspective on the key impacts of community-based learning in undergraduate medical education. Med Educ 2001;35:666-72.
6. Steiner B, Sands R: Responding to a natural disaster with service learning. Fam Med 2000:32:645-9.
7. Redman RW, Clark L: Service-learning as a model for integrating social justice in the nursing curriculum. J Nurs Educ 2002;41:446-9.
8. Rubenstein HL, Franklin ED, Zarro VJ: Opportunities and challenges in educating community-responsive physicians. Am J Prev Med 1997;13:104-8.
9. Eyler J, Giles DE. Where's the Learning in Service-Learning. San Francisco, Jossey-Bass, 1999.
10. Jacoby B, eds. Service-Learning in Higher Education: Concepts and Practices. San Francisco, Jossey-Bass, 1996.
11. Kolb DA, Rubin IM, McIntyre JM. Organizational Psychology: an Experiential Approach. New Jersey, Prentice-Hall, 1971.
12. Steiner B, Sands R. Responding to a natural disaster with service learning. Fam Med 2000;32:645-9.
13. Bandura A. Self-Efficacy: The Exercise of Control. New York; Freeman, 1997. 14. Sigmon R. The Problem of Definition in Service-Learning. In Sigmon R et al. Eds. The Journey to Service-Learning Washington, D.C.: Council of Independent College,
Education. Racine, Wisc. : Johnson Foundation, 1987.
18. Sigmon R. Service-Learning: Three Principles. Synergist 1979;8(1).
19. Howard J eds. Praxis I: A Faculty Casebook on Community Service Learning. Ann Arbor: OCSL Press, 1993.
20. Krumboltz JD, Mitchell AM, Jones GB. A Social Learning Theory of Career Selection. Counseling Psychologist 1976;6:71-81.
21. Sanford N. Where College Fail: A Study of the Student as a Person. San Francisco: Jossey-Bass, 1967.
22. Kohlberg L. The Cognitive-Development Approach to Moral Education. Phi Delta Kappan, 1975;56:670-7.
23. Eckenfels EJ. Contemporary medical students' quest for self-fulfillment through community service. Acad Med 1997;72:1043-50.
Table 1. Descriptive statistics of the Social Attitude Scale, Program Characteristic Scale and Ability Scale
Scale/Dimensions Mean S.D. Skewness Kurtosis
Social Attitude Scale
Citizenship 3.72 0.39 0.41 1.07 Personal efficacy 3.59 0.50 0.50 0.72 Community efficacy 3.43 0.50 0.09 0.68 Community connectedness 4.16 0.50 -0.24 0.53 Locus of problem 2.22 0.68 0.42 0.28 Social justice 3.94 0.46 -0.43 1.23 Tolerance 2.03 0.74 0.40 0.01 Gains 3.84 0.61 -0.03 0.05 Values 3.00 0.58 0.21 0.30
Program Characteristic Scale
Reflection/discussion 3.97 0.55 -0.77 3.92 Reflection/writing 4.09 0.57 -0.37 0.96 Placement quality 3.61 0.50 0.06 0.66 Community voice 3.40 0.64 -0.49 1.02 Application 3.78 0.58 -0.43 1.10 Diversity 3.40 0.88 -0.61 0.48 Ability Scale Leadership skills 3.59 0.54 -0.50 1.79 Communication skills 3.99 0.47 -1.09 7.75 Team work 3.82 0.43 -1.00 7.75 See consequences 3.78 0.58 -0.52 1.81 Action skills 3.65 0.56 -0.08 0.16 Critical thinking 3.82 0.71 -0.14 -0.23 Identify social issues 3.96 0.73 -0.51 0.79
Table 2. Correlation between social attitude and program characteristics
Two-tailed Pearson correlation coefficients * P< 0.05; ** P< 0.01; ***P< 0.001
Citizenship Locus of problem
Social justice
Tolerance Gains Values Reflection/discussion 0.08 -0.07 0.11 -0.10 0.17 0.05 Reflection/writing 0.05 -0.07 0.02 -0.06 0.17 -0.05 Placement quality 0.15 -0.02 0.13 -0.11 0.21** 0.20** Community voice 0.13 -0.09 0.07 -0.09 0.25** 0.13 Application 0.05 -0.13 0.13 -0.07 0.10 0.11 Diversity 0.14 0.14 -0.06 0.07 0.14 0.16*
Table 3. Correlation between social attitude and acquired abilities Citizenship Locus of problem Social justice
Tolerance Gains Values
Leadership skills 0.18 -0.14 0.27*** -0.14 0.20** 0.27*** Communication skills 0.03 -0.17 0.17 -0.18 0.07 0.13 Team work 0.09 -0.07 0.18 -0.11 0.19** 0.15 See consequence 0.22** -0.05 0.14 -0.12 0.18 0.19 Critical thinking 0.06 -0.10 0.11 -0.17 0.05 0.20** Identify social issue 0.11 -0.14 0.21** -0.18* 0.06 0.01 Action skills 0.14 -0.04 0.17 -0.05 0.15 0.19 Two-tailed Pearson correlation coefficients
Table 4. Correlation between program characteristics and acquired abilities Reflection /discussion Reflection /writing Placement quality Community voice Application Diversity Leadership skills 0.45*** 0.35*** 0.38*** 0.40*** 0.31*** 0.25*** Communication skills 0.52*** 0.51*** 0.52*** 0.40*** 0.49*** 0.19* Team work 0.55*** 0.51*** 0.49*** 0.42*** 0.47*** 0.32** See consequence 0.41*** 0.38*** 0.40*** 0.28*** 0.48*** 0.28*** Critical thinking 0.18* 0.10 0.29*** 0.13 0.27*** 0.14 Identify social issue 0.36*** 0.38*** 0.28*** 0.26*** 0.47*** 0.16* Action skills 0.42*** 0.38*** 0.44*** 0.46*** 0.40*** 0.29*** Two-tailed Pearson correlation coefficients