The use of 3D-CT angiography to measure the normal angle formed by the aorta and the SMA: the value and application of 3D-CT angiography in SMA syndrome
5
0
0
全文
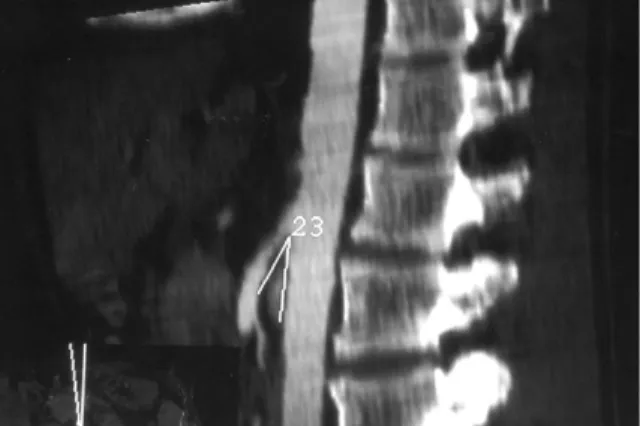
(2) 74. 3D-CTA in SMA Syndrome. Fig. 1. A 40-year-old man from the control group. Multiplanar reformation reveals a normal aorta-SMA angle of 23 degrees.. Fig. 2. A 23-year-old woman with superior mesenteric artery syndrome. Maximum intensity projection shows a sharp aorta-SMA angle of 14 degrees.. upper gastrointestinal tract, but findings are not specific and often are non-diagnostic [5,6]. Hypotonic duodenography combined with simultaneous SMA arteriography has been suggested as the most efficient radiologic technique [7,8], but it is invasive, and some patients are unable to tolerate the angiographic procedure. However, CT angiography is a useful noninvasive diagnostic procedure which all patients are able to undergo. Konen et al first described the use of 3DCTA in the evaluation of SMA syndrome in 1998 [9]. In their series, three types of reformatted images were used: shade-surface displays, maximum intensity projections, and multiplanar reformations. The mean measured aortomesenteric angle was 9 in the patient group and 44.4 in the control group. The mean measured aortomesenteric angle was 45 in the normal group in our study. The result is compatible with that of a previous study [9]. In this study, we analyzed the use of CT angiography with two types of reformatted images (maximum intensity projections and multiplanar reformations) to measure the angle between the aorta and the SMA in the normal group, and evaluated the value and applications of 3D-CTA for diagnosing SMA syndrome.. or other abdominal symptoms were prospectively studied. None of the patients had previously undergone abdominal surgical procedures. There were 57 males and 39 females (age range, 20 to 68 years; mean, 51 years) who underwent CT angiography. Helical CT angiography was performed on a CT scanner (Elscint, CT Twin, Israel) with the following parameters: maximum scan time, 32.1 sec; dual pitch, 1; table speed, 5 mm/sec; and effective slice thickness, 6.5 mm. Through a large-bore peripheral intravenous line, 90 mL of contrast medium (Omnipaque, Nycomed, Oslo, Norway) was administered rapidly by power injector at 3.2 mL/sec. Scanning delay time was 27 sec after initiation of the bolus. The 3D reconstructions were performed on an independent workstation (Elscint, Omnipro2). We used two types of reformatted images: maximum intensity projections, and multiplanar reformations. The tangent of the aorta-SMA angle was measured on the basis of the maximum intensity projections and multiplanar reformations. We studied two patients with radiologic signs of relative obstruction at the level of the third portion of the duodenum with a similar protocol.. MATERIALS AND METHODS. RESULTS. From July 1999 to June 2000, 96 patients referred to our CT center because of hepatic mass. No difficulties were encountered in most of our patients when ventilation was suspended for.
(3) Yung-Fang Chen, et al.. 32 seconds. Although a few of the patients were not able to hold their breath for 32 seconds, it did not affect the measurement of the aortomesenteric angle. No definite extravasation of contrast medium was noted during injection. Timing of the contrast bolus was also controlled to achieve maximal vascular opacification. With this technique, the angle between the aorta and the SMA was displayed reliably with 3D-CTA. Parasagittal reformations and maximum intensity projections were found to be useful for measuring the aorta-SMA angle at the level of the duodenum. The mean measured normal aortaSMA angle was 45 (range, 23 to 85 ) (Fig. 1). In the two patients with related obstruction at the level of the third portion of the duodenum, the mean measured aorta-SMA angle was 15 (range, 14 to 16 ) (Fig. 2). DISCUSSION. SMA syndrome is a rare disease. There are multiple predisposing factors, including a) congenital anomalies such as high insertion or hypertrophy of the Treitz ligament [10], b) marked weight loss due to severe wasting diseases such as cancer and burns [11], c) the application of a body cast to treat scoliosis or vertebral fracture [12], and d) idiopathy due to emaciation, and loss of mesenteric fat [4,13]. There are a number of therapeutic approaches to superior mesenteric artery syndrome. For example, nonoperative treatment should be attempted first [14,15]. Simple gravitational maneuvers, such as placing the patient into the prone knee-chest or left lateral decubitus position after eating, may relieve the problem. For patients in whom conservative methods fail, operative relief of superior mesenteric artery syndrome has been described. Three operations have been found to be useful: gastrojejunostomy, duodenojejunostomy, and Strong's operation [15]. Obstruction of the duodenum in SMA syndrome is caused by narrowing of the angle between the aorta and the SMA [1,3]. Conventional barium meal and hypotonic duodenography have been recommended as screening methods. Positive findings include. 75. dilatation of the first, second, and third portion of the duodenum, an abrupt vertical filling defect at the level of the SMA, retention of barium within the duodenum, and frequent relief of obstruction in the left lateral decubitus or prone positions [4,16,17]. Unfortunately, these radiologic appearances are non-specific for SMA syndrome and have been reported in various conditions such as slceroderma, diabetes, pancreatitis, peptic ulcer, lupus erythematosis and idiopathic intestinal pseudoobstruction [4-6,18]. In the past, angiographic measurement of the aortomesenteric angle was noted as being a more accurate investigation than a routine barium meal examination [7,8]. However, the procedure is invasive, and some patients are unable to tolerate it. More recently, the development of spiral CT has made CT angiography a wellrecognized and reliable technique which obtains excellent anatomic detail of the aorta and its branches [19]. The main advantage of spiral CT angiography is its ability to construct high-quality 3D renderings of the abdominal vasculature without the need for invasive angiography. Measurements of the aortomesenteric angle obtained in our series, based on CT angiography 3D reformations, were similar to those of previous angiographically based reports [2,7,8]. Although conventional angiography probably will remain the diagnostic gold standard, spiral CT angiography is less invasive, less expensive, easier to perform, and quicker than conventional angiography. The reconstructed images provide excellent anatomic detail that easily enables accurate diagnosis and preoperative planning. Spiral CT angiography reduces the risk of invasive diagnosis and is not dependent on the catheterization skills of the operator. In conclusion, our initial experience has shown that spiral CT angiography with 3D reconstruction is a safe, reliable, and useful noninvasive diagnostic technique. With the rapid explosion of clinical testing and refinement in techniques, spiral CT angiography with 3D reconstruction undoubtedly will become a routine diagnostic tool in the feature..
(4) 76. 3D-CTA in SMA Syndrome REFERENCES. 1. Jones SA, Carter R, Smith LL, et al. Arteriomesenteric duodenal compression. Am J Surg 1960;100:262-77. 2. Mansberger AR Jr, Hearn JB, Byers RM, et al. Vascular compression of the duodenum. Emphasis on accurate diagnosis. Am J Surg 1968;115:89-96. 3. Marchant EA, Alvear DT, Fagelman KM. True clinical entity of vascular compression of the duodenum in adolescence. Surg Gynecol Obstet 1989;168:381-6. 4. Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg 1984;148:630-2. 5. Gondos B. Duodenal compression defect and the "superior mesenteric artery syndrome" 1. Radiology 1977;123:575-80. 6. Anderson JR, Earnshaw PM, Fraser GM. Extrinsic compression of the third part of the duodenum. Clin Radiol 1982;33:75-81. 7. Lukes PJ, Rolny P, Nilson AE, et al. Diagnostic value of hypotonic duodenography in superior mesenteric artery syndrome. Acta Chir Scand 1978;144:39-43. 8. Gustafsson L, Falk A, Lukes PJ, et al. Diagnosis and treatment of superior mesenteric artery syndrome. Br J Surg 1984;71:499-501. 9. Konen E, Amitai M, Apter S, et al. CT angiography of superior mesenteric artery syndrome. AJR Am J Roentgenol 1998;171:1279-81 10.Lin SP, Huang FY, Lee HC, et al. Superior mesenteric artery in newborn: two cases report. Acta Paediatrica. Sinica 1986;27:585-9. 11. Chen SH, Chen WS, Chuang JH. Superior mesenteric artery syndrome as a complication in hip spica application for immobilization: report of a case. J Formos Med Assoc 1992;91:731-3. 12. Berk RN, Coulson DB. The cast syndrome. Radiology 1970;94:303-3. 13.Ylinen P, Kinnunen J, Hockerstedt K. Superior mesenteric artery syndrome. A follow-up study of 16 operated patient. J Clin Gastroenterol 1989;11:386-91. 14. Burrington JD. Superior mesenteric artery syndrome in children. Am J Dis Child 1976;130:579-617. 15. Strong EK. Mechanics of arteriomesenteric duodenal obstruction and direct surgical attack upon etiology. Ann Surg 1958;148:725-30. 16. Griffiths GJ, Whitehouse GH. Radiological features of vascular compression of the duodenum occurring as a complication of the treatment of scoliosis (the cast syndrome). Clin Radiol 1978;29:77-83. 17. Wang YH, Hanyu F. The superior mesenteric artery syndrome. Taiwan Yi Xue Hui Za Zhi 1982;81:9-17. 18.Cohen LB, Field SP, Sachar DB. The superior mesenteric artery syndrome. The disease that isn't, or is it? J Clin Gastroenterol 1985;7:113-6. 19.Rubin GD, Dake MD, Napel SA, et al. Threedimensional spiral CT angiography of the abdomen: initial clinical experience. Radiology 1993;186:14752..
(5) 77. 1. 2 1. 1999. 2000. 2. 96 94. 45 (. 23. 85 ). 15. 2003;8:73-7. 404. 2. 2002. 7. 5. 2003. 1. 17. 2002. 10. 17. (. 14. 16 ).
(6)
數據
相關文件
6 《中論·觀因緣品》,《佛藏要籍選刊》第 9 冊,上海古籍出版社 1994 年版,第 1
You are given the wavelength and total energy of a light pulse and asked to find the number of photons it
Reading Task 6: Genre Structure and Language Features. • Now let’s look at how language features (e.g. sentence patterns) are connected to the structure
• To introduce the use of the LPF as a tool for planning the school English Language curriculum; and
Understanding and inferring information, ideas, feelings and opinions in a range of texts with some degree of complexity, using and integrating a small range of reading
Promote project learning, mathematical modeling, and problem-based learning to strengthen the ability to integrate and apply knowledge and skills, and make. calculated
Wang, Solving pseudomonotone variational inequalities and pseudocon- vex optimization problems using the projection neural network, IEEE Transactions on Neural Networks 17
Hope theory: A member of the positive psychology family. Lopez (Eds.), Handbook of positive
volume suppressed mass: (TeV) 2 /M P ∼ 10 −4 eV → mm range can be experimentally tested for any number of extra dimensions - Light U(1) gauge bosons: no derivative couplings. =>
