in Hemodialysis Patients
Jinn-Yuh Guh, MD, Hung-Chun Chen, MD, Hung-Yi Chuang, MD, Su-Chen Huang, RN, Li-Chu Chien, RN, and Yung-Hsiung Lai, MD
● Relative hypoparathyroidism (parathyroid hormone [PTH] < 200 pg/mL) is prevalent in hemodialysis (HD) patients, with unknown pathogenesis and prognosis. Thus, to clarify risk factors and prognosis of time-dependent relative hypoparathyroidism in HD patients, a retrospective cohort study was performed for 126 HD patients with four or more PTH determinations and no previous total or subtotal parathyroidectomy. Values for intact PTH, ionized calcium, phosphate, magnesium, albumin, creatinine, urea reduction ratio (URR), glucose, hemoglobin A1c
(HbA1c), aluminum, and 1,25(OH)2D were obtained at enrollment and at some time during follow-up. The prevalence
of relative hypoparathyroidism at entry was 76 of 126 patients (60.3%). Univariate analysis showed that patients with hypoparathyroidism were older, more likely to have diabetes, and had greater ionized calcium levels and lower phosphate, albumin, blood urea nitrogen (BUN), and creatinine levels. Patients with diabetes were older and had a shorter duration of dialysis therapy and lower PTH, phosphate, albumin, BUN, and creatinine levels and URRs. Conversely, multivariate analysis showed that PTH levels at entry were associated directly with creatinine levels and inversely with age and ionized calcium levels (but not diabetes). During follow-up, PTH levels fluctuated concomitantly with ionized calcium and phosphate levels over time in all patients. Time-dependent PTH levels were associated directly with duration of dialysis therapy and use of vitamin D and phosphate and albumin levels, but inversely with age and ionized calcium and magnesium levels (but not glucose or HbA1clevels). Interestingly, time-dependent PTH levels were independently associated with survival after adjusting
for traditional risk factors (diabetes, age, albumin and creatinine levels, and URR) and duration of dialysis therapy. We conclude that in HD patients, relative hypoparathyroidism was not associated with diabetes per se. Time-dependent PTH levels were associated with age, duration of dialysis, and levels of ionized calcium, phosphate, albumin, and magnesium. Moreover, relative hypoparathyroidism at entry and lower time-dependent PTH levels predict mortality.
©2002 by the National Kidney Foundation, Inc.
INDEX WORDS: Hemodialysis (HD); mortality; hypoparathyroidism; retrospective cohort study.
T
HE PREVALENCE OF relativehypopara-thyroidism is increasing to as high as 64.4% among hemodialysis (HD) patients.1Its clinical significance is not known, although it has been associated with adynamic bone disease.2 Ady-namic bone disease has emerged as the most common form of renal osteodystrophy in dialysis patients.2 Conversely, secondary hyperparathy-roidism has been studied thoroughly and is con-sidered detrimental to uremic patients,3although it has never been independently associated with mortality in dialysis patients.
Several researchers have studied risk factors for relative hypoparathyroidism in HD pa-tients.1,4-7Unfortunately, all used univariate anal-yses in cross-sectional studies and failed to ac-count for many factors that affect parathyroid hormone (PTH) levels.8 In addition, although multiple regression was used in a relevant study,5 it was only a cross-sectional case-control study and therefore failed to detect changes over time in individual patients. Also, cross-sectional stud-ies have inherent disadvantages, whereas the study of events in time and an appreciation of the picture of health and disease over time are
funda-mental to biomedical research and public health surveillance.9,10Moreover, the natural history of uremic relative hypoparathyroidism remains un-known.
Therefore, in a retrospective cohort study of HD patients, we attempted to determine: (1) risk factors for enrollment and time-dependent rela-tive hypoparathyroidism, (2) whether relarela-tive hypoparathyroidism was a fixed or dynamic state during serial follow-ups, and (3) whether time-dependent PTH levels were associated with mor-tality.
From the Departments of Internal Medicine and Occupa-tional Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Received September 24, 2001; accepted in revised form December 19, 2001.
Address reprint requests to Yung-Hsiung Lai, MD, Divi-sion of Nephrology, Department of Internal Medicine, Kaohsiung Medical University, 100 Shi-Chuan First Rd, Kaohsiung, Taiwan. E-mail: [email protected]
© 2002 by the National Kidney Foundation, Inc. 0272-6386/02/3906-0017$35.00/0
doi:10.1053/ajkd.2002.33398
METHODS
We reviewed records of 212 maintenance HD patients in April 2000. Patients were included if they met the following criteria: (1) older than 18 years, (2) four or more intact PTH measurements available after April 1990, (3) alive for 1 year or longer, (4) never underwent total or subtotal parathyroid-ectomy, and (5) never administered pulse intravenous high-dose active vitamin D treatment. Criteria as listed excluded 86 patients, including 14patients with total or subtotal parathyroidectomy, 18 patients administered pulse intrave-nous high-dose active vitamin D treatment, 17 patients who survived less than 1 year, 2 patients younger than 18 years, and 35 patients with fewer than four intact PTH determina-tions after April 1990. Accordingly, 40 patients with diabetes and 86 patients without diabetes were recruited. Because serum PTH level was the main outcome, we limited the study to patients with at least four PTH measurements, the minimum number of observations required for a meaningful statistical assessment.
The study protocol was approved by the institutional review board. Participants underwent HD three times weekly using hollow-fiber dialyzers and bicarbonate dialysates con-taining calcium and magnesium at concentrations of 2.5 to 3.5 and 1.0 mEq/L, respectively. Patients were administered calcium carbonate (n⫽ 112) and aluminum hydroxide (n ⫽ 36) as phosphate binders. Note that some patients (n⫽ 24) were administered a combination of calcium carbonate and aluminum hydroxide. Oral active vitamin D (1, ␣-(OH)-vitamin D3; Chugai Co, Tokyo, Japan) was administered to
11 patients at dosages of 0.25 to 1.0g/d. According to the regulations of Health Insurance Agencies, recombinant hu-man erythropoietin (rHuEPO) was administered (0 to 20,000 U/mon intravenously or subcutaneously) to keep hemoglo-bin at a target level of 10 g/dL since July 1993. Thus, rHuEPO dosage was coded as 0 for data before July 1993.
Diabetes mellitus was diagnosed based on one of the following criteria: (1) history of physician-diagnosed diabe-tes, (2) history of insulin therapy, (3) history of oral hypogly-cemic therapy, or (4) history of fasting glucose level of 126 mg/dL or greater or postprandial glucose level of 200 mg/dL or greater on at least two occasions. For patients with diabetes, fasting plasma glucose levels were used as a measure of short-term glycemic control, whereas hemoglo-bin A1c(HbA1c) levels were used as an index of long-term
glycemic control. Blood urea nitrogen (BUN), creatinine, ionized calcium, phosphate, albumin, and glucose (for pa-tients with diabetes) were measured every month, whereas PTH was measured every 3 months. Magnesium and alumi-num were measured every 6 months.
Cross-Sectional (enrollment) Data and Retrospective Cohort Study
Data for 126 patients (55 men, 71 women; age, 53.1⫾ 1.24years; HD duration, 16⫾ 1.9 months) who first met inclusion criteria were enrolled onto a cross-sectional study. These patients were followed up for serial levels of PTH, ionized calcium, phosphate, and the other variables in a retrospective observational cohort study.
Laboratory Measurements
Predialysis fasting samples were measured. Serum in-tact PTH was measured using the Allegro Immunoradio-metric Assay (Nichols Institute, San Juan Capistrano, CA; reference range, 10 to 65 pg/mL) with a sensitivity of 1.8 pg/mL and intra-assay and interassay coefficients of varia-tion of 5.6% and 7.7%, respectively.11
Hypoparathyroid-ism was arbitrarily defined as a PTH level of 200 pg/mL or less based on two considerations. First, recent consen-sus suggests that PTH levels should be kept at 100 to 200 pg/mL to maintain normal skeletal bone turnover.12
Sec-ond, a recent study showed that absolute (PTH ⬍ 65 pg/mL), but not relative (PTH, 65 to 200 pg/mL), hypo-parathyroidism is associated with mortality13; therefore,
we designed the study to establish the relationship be-tween PTH levels and mortality.
Serum BUN, creatinine, phosphate (reference range, 2.5 to 4.5 mg/dL), plasma glucose, and complete blood count were measured using a routine autoanalyzer (Hita-chi 736-40, Tokyo, Japan). Ionized calcium was measured using an ionized calcium analyzer (reference range, 4.2⬃ 5.3 mg/dL; Nova Biomedical, Waltham, MA). Serum magnesium was measured using the atomic absorption method (reference range, 1.7⬃ 2.3 mEq/L; Perkin-Elmer Corp, Shelton, CT). HbA1c (reference range, 4.3% to
6.1%) was tested every 4months in patients with diabetes by means of the high-performance liquid chromatography (HPLC) method (Hemoglobin A1cby HPLC; Bio-Rad Co,
Hercules, CA). Serum aluminum (reference range,⬍10 g/L) was measured by flameless atomic absorption spec-trophotometry, whereas serum 1,25(OH)2D was measured
using a radioreceptor assay kit for a subset of patients (reference range, 26.9⫾ 2.5 pg/mL; Incstar Corp, Stillwa-ter, MN). Normalized protein catabolic rate (nPCR) was calculated from urea generation rate and urea distribution volume by urea kinetic modeling.14Urea reduction ratio
(URR) and nPCR were averaged for 3 months at enroll-ment. Note that because this was a dynamic cohort (in which patients entered the cohort at different times), only a subset of patients was assayed for serum aluminum and 1,25-(OH)2D, which were available only after January
1992.
Statistics
Statistical packages SPSS (version 10.0; SPSS Inc, Chi-cago, IL) and R (Available at: http://www.ci.tuwien.ac.at/ ⬃hornik/R/R-FAQ.html) were used. Results are expressed as mean⫾ SEM. Two-tailed tests were used. P less than 0.05 is considered statistically significant.
Because PTH level was not normally distributed, it was logarithmically transformed before statistical tests. In enrollment data, unpaired Student’s t-tests were used to compare means between two groups, considering Lev-ene’s test for equality of variances. One-way analysis of variance, followed by Bonferroni test, was used for com-parison among three groups. Chi-square tests with conti-nuity correction were used for categorical variables. Pear-son’s product-moment correlation was performed for the relationship between two continuous variables. Multiple regression (dependent variable, PTH) was used to adjust
for multiple variables (diabetes, use of vitamin D, age, duration of dialysis therapy, rHuEPO dosage, hemoglobin level, ionized calcium level, phosphate level, albumin level, BUN level, creatinine level, and URR). Categorical variables (diabetes and use of vitamin D) were coded as 0 (absent) or 1 (present). Collinearity of independent vari-ables was assessed by the variance inflation factor. In general, a variance inflation factor greater than 10 indi-cates significant collinearity.
In the longitudinal study, ordinary least squares are not adequate because serial data tend to be autocorrelated, and data within clusters (individuals) also are correlat-ed.15Therefore, a generalized estimating equation15
(de-pendent variable, PTH; inde(de-pendent variables, diabetes, use of vitamin D, age, duration of dialysis therapy, rHuEPO dosage, hemoglobin level, ionized calcium level, phosphate level, magnesium level, albumin level, creati-nine level, aluminum level) was used to study factors affecting PTH. Survival analysis was performed using the Kaplan-Meier method (with log-rank test). Moreover, Cox proportional hazards regression (predictors: diabe-tes, age, duration of dialysis therapy, rHuEPO dosage, PTH levels at entry or serial PTH levels, hemoglobin level, albumin level, creatinine level, URR) was used, in which serial PTH levels were treated as time-dependent covariates. Patients studied were either dead, prematurely censored before April 2000 (eg, transferred to other hospitals, on peritoneal dialysis therapy, underwent renal transplantation), or censored on April 2000 (ie, alive by April 2000).
RESULTS
Risk Factors for Relative Hypoparathyroidism Cross-sectional study in enrollment. Preva-lences of absolute (PTH⬍ 65 pg/mL) and rela-tive hypoparathyroidism (PTH, 65 to 200 pg/ mL) were 32 of 126 (25.4%) and 44 of 126 patients (34.9%), respectively. Mean PTH levels were 135⫾ 1.1 pg/mL in patients administered calcium carbonate (n ⫽ 88) as the phosphate binder and 168⫾ 1.4pg/mL (P ⫽ not significant [NS]) in patients administered aluminum hydrox-ide (n⫽ 12). As listed in Table 1, patients with a PTH level greater than 200 pg/mL were less likely to have diabetes and had lower ionized calcium and greater creatinine levels than those with a PTH level of 200 pg/mL or less. Patients with a PTH level greater than 200 pg/mL also had greater phosphate and albumin levels than those with a PTH level less than 65 pg/mL. Patients with a PTH level less than 65 pg/mL were older and had greater ionized calcium lev-els than those with a PTH level of 65 pg/mL or greater. Patients with a PTH level less than 65 pg/mL had lower nPCRs than those with a PTH Table 1. Demographic and Biochemical Features in 126 HD Patients With and Without
Enrollment Hypoparathyroidism Variables PTH⬍65 pg/mL No. of Patients PTH⫽65-200 pg/mL No. of Patients PTH⬎200 pg/mL No. of Patients PTH (pg/mL) 32.4⫾2.9 32 132.1⫾6.26* 44 430⫾27.9*† 50 Age (y) 60.9⫾2.4 32 51.7⫾1.7* 44 50⫾2.1* 50 Duration (mon) 16.5⫾4.7 32 11.8⫾4.5 44 18.2⫾3.2 50 Men (%) 34.4 32 46.5 44 45.1 50 Vitamin D use (%) 6.3 32 13.8 44 8.2 50
rHuEPO dosage (U/mon) 8,985⫾1,085 32 8,261⫾862 44 9,970⫾786 50
Diabetes (%) 5032 42.8 44 18*‡ 50 Hemoglobin (g/dL) 9.37⫾0.58 32 8.56⫾0.39 44 9.47⫾0.37 50 Ionized calcium (mg/dL) 5.08⫾0.08 32 4.7⫾0.06§ 44 4.45⫾0.05*‡ 50 Phosphate (mg/dL) 4.46⫾0.34 32 5.28⫾0.23 44 6.18⫾0.28* 50 Magnesium (mEq/L) 2.5⫾0.1 19 2.3⫾0.08 28 2.48⫾0.09 41 Albumin (g/dL) 3.72⫾0.08 32 3.76⫾0.08 44 4.08⫾0.08* 50 BUN (mg/dL) 89.4⫾6.7 32 84.7⫾3.1 44 101⫾3.7‡ 50 nPCR (g/kg/d) 1.0⫾0.04 32 1.11⫾0.03 44 1.18⫾0.04* 50 URR 0.69⫾0.03 32 0.68⫾0.02 44 0.72⫾0.01 50 Creatinine (mg/dL) 9.23⫾0.39 32 11.2⫾0.46§ 44 13.4⫾0.48*† 50 Aluminum (g/L) 59.4⫾4.3 22 54.8⫾6.8 28 61⫾4.23 31 1,25(OH)2D (pg/mL) 8.3⫾2.8 208.1⫾2.8 21 7.68⫾4.2 23
NOTE. Values expressed as mean⫾SEM. *P⬍0.01 versus PTH level less than 65 pg/mL. †P⬍0.01 versus PTH level of 65 to 200 pg/mL. ‡P⬍0.05 versus PTH level of 65 to 200 pg/mL. §P⬍0.05 versus PTH level less than 65 pg/mL.
level greater than 200 pg/mL. Patients with a PTH level of 65 to 200 pg/mL had lower BUN levels than those with a PTH level greater than 200 pg/mL. However, there were no differences in duration of dialysis therapy, distribution of sex or vitamin D use, URR, or serum magnesium, aluminum, and 1,25(OH)2D levels among these three groups of patients. Note that results are similar when the arbitrary cutoff value for PTH was changed from 200 to 162.5 pg/mL (2.5 times the normal upper limit).
As listed in Table 2, patients with diabetes had lower PTH levels and were older and had a shorter duration of dialysis therapy than patients without diabetes. Moreover, patients with diabe-tes had lower albumin, BUN, creatinine, and phosphate levels and URRs than those without diabetes. Conversely, no difference was found in sex, use of vitamin D, or levels of ionized cal-cium, magnesium, aluminum, or 1,25(OH)2D between these two groups.
PTH level correlated with age (r ⫽ ⫺0.41; P ⬍ 0.001), BUN level (r ⫽ 0.26; P ⬍ 0.01), creatinine level (r⫽ 0.56; P ⬍ 0.001), URR (r ⫽ 0.22; P ⬍ 0.05), albumin level (r ⫽ 0.40; P ⬍ 0.001), ionized calcium level (r ⫽ ⫺0.58; P⬍ 0.001), and phosphate level (r ⫽ 0.42; P ⬍ 0.001) by univariate correlation analyses. Con-versely, multiple regression analysis (Table 3) showed that PTH level correlated only with age (P⬍ 0.01), ionized calcium level (P ⬍ 0.001), and creatinine level (P⬍ 0.001). In the subset of data with no missing magnesium (n ⫽ 88) or
aluminum values (n⫽ 81), PTH level was not associated with magnesium or aluminum level. Collinearity diagnostics of independent variables showed that all variance inflation factors (range, 1.0 to 1.52) were much less than 10. In other words, there was no significant multicollinearity among independent variables.
Longitudinal study. PTH levels fluctuated in all patients, whereas 39 of 76 relatively hypopara-thyroid (PTH ⱕ 200 pg/mL) patients (51%) remained persistently hypoparathyroid. As listed in Table 4, a generalized estimating equation showed that time-dependent PTH levels were associated inversely with age and ionized cal-cium levels and directly with albumin and phos-phate levels, duration of dialysis therapy, and use of vitamin D. The association between PTH and Table 2. Demographic and Biochemical Features in 126 HD Patients With and Without Diabetes
Variables No Diabetes No. of Patients Diabetes No. of Patients P PTH (pg/mL) 176⫾1.13 86 76.7⫾1.17 40 ⬍0.001 Age (y) 50.4⫾1.5 86 59.8⫾1.6 40 ⬍0.001 Duration (mon) 19.2⫾2.6 86 9.3⫾2.2 40 ⬍0.01 Men/total 38/86 (44) 86 17/40(43) 40 NS Use of vitamin D 10/86 (12) 86 1/40 (2.5) 40 NS Ionized calcium (mg/dL) 4.64⫾0.04 86 4.8⫾0.08 40 NS Phosphate (mg/dL) 5.76⫾0.19 86 4.71⫾0.34 40 ⬍0.01 Magnesium (mEq/L) 2.48⫾0.28 63 2.38⫾0.08 25 NS Albumin (g/dL) 4.01⫾0.05 86 3.54⫾0.08 40 ⬍0.001 BUN (mg/dL) 98⫾2.7 86 80⫾5 40 ⬍0.01 URR 0.73⫾0.01 86 0.63⫾0.02 40 ⬍0.001 Creatinine (mg/dL) 12.7⫾0.34 86 9.2⫾0.43 40 ⬍0.001 Aluminum (g/L) 61.3⫾4.6 58 59.7⫾8.4 23 NS 1,25(OH)2D (pg/mL) 8.5⫾0.45 43 8⫾0.71 21 NS
NOTE. Results expressed as mean⫾SEM or number of total (percent).
Table 3. Stepwise Multiple Regression for Factors Associated with logPTH in 126 HD Patients
in Enrollment Variable Coefficient⫾SE P No. of Patients Age (y) ⫺0.016⫾0.006 ⬍0.01 126 Ionized calcium (mg/dL) ⫺0.96⫾0.16 ⬍0.001 126 Creatinine (mg/dL) 0.11⫾0.03 ⬍0.001 126 NOTE. Dependent variable is logPTH; independent vari-ables are diabetes, use of vitamin D, age, duration of dialysis therapy, rHuEPO dosage, hemoglobin level, albu-min level, BUN level, creatinine level, PCR, URR, and ionized calcium and phosphate levels. Only results with P less than 0.05 are listed.
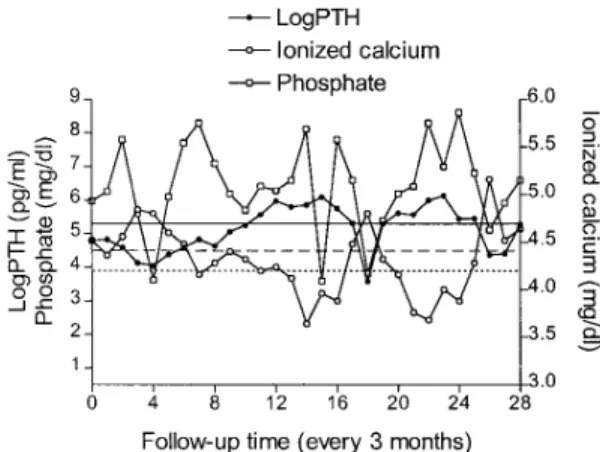
ionized calcium/phosphate levels over time is shown in a representative patient (Fig 1). In subsets of data with no missing magnesium or aluminum values, time-dependent PTH levels also were associated inversely with magnesium levels (n⫽ 915), but not aluminum levels (n ⫽ 601).
Glycemic Control and Hypoparathyroidism in Patients With Diabetes
In cross-sectional enrollment data, PTH level was not associated with either HbA1cor glucose level in stepwise multiple regression. In the lon-gitudinal study, time-dependent PTH levels also were not associated with glucose levels in data with no missing glucose (n ⫽ 1,067) or HbA1c values (n ⫽ 261) in a generalized estimating equation.
Impact of PTH Levels at Entry and Time-Dependent PTH Levels on Mortality
During the 10-year follow-up of 126 patients, 46 patients (36.5%) died. Fifty-three of 126 patients (42.1%) were alive by April 2000, whereas 27 of 126 patients (21.4%) were cen-sored before April 2000. Thirty-nine of 46 pa-tients (84.8%) with enrollment hypoparathyroid-ism were among patients who died. Cause of death was cardiovascular in 19 of 46 patients (41.3%).
For a meaningful analysis of the following
data, we must have enough patients while exclud-ing those prematurely censored (eg, transferred to other hospitals, on peritoneal dialysis therapy, underwent renal transplantation) for whom data were not available. Therefore, the following anal-yses are performed in the 101 patients who were not censored, ie, either alive (n ⫽ 56) or dead (n⫽ 45), by year 5 of follow-up. In patients with and without enrollment hypoparathyroidism, 17 of 63 (27%) and 2 of 38 patients (5.3%) had cardiovascular deaths (P ⬍ 0.02) and 5 of 63 (7.94%) and 2 of 38 patients (5.3%) had fractures (P⫽ NS), respectively. Three of 45 (6.7%) and 4 of 56 patients (7.1%) had fractures among those who died or survived, respectively (P ⫽ NS). Patients who died had significantly lower values for albumin (3.6 ⫾ 0.07 versus 3.95 ⫾ 0.06 g/dL; P⬍ 0.01) and nPCR (1.0 ⫾ 0.03 versus 1.14⫾ 0.04g/kg/d; P ⬍ 0.02) than those who survived. As shown in Fig 2A, PTH levels in-creased with time only in patients who survived. Furthermore, as shown in Fig 2B, in patients with enrollment hypoparathyroidism (n⫽ 63), persistence of hypoparathyroidism during the study only occurred in patients who died (n⫽ 30).
Kaplan-Meier analysis showed that enroll-ment hypoparathyroidism (Fig 3A) was associ-ated with mortality. Cox regression showed that enrollment hypoparathyroidism, but not nPCR, was independently associated with mortality
af-Fig 1. Serial PTH, ionized calcium, and phosphate levels in a representative patient. Note that PTH levels changed in the same and opposite directions of phos-phate and ionized calcium levels. Horizontal lines are cutoff values for PTH (200 pg/mL; solid line), ionized calcium (4.2 mg/dL; lower broken line), and phosphate (4.5 mg/dL; upper broken line).
Table 4. Results of a Generalized Estimating Equation in the Longitudinal Study
Variable Coefficient⫾SE P No. of Data Vitamin D use 0.4⫾0.195 ⬍0.05 1,971 Age (y) ⫺0.018⫾0.0048 ⬍0.02 1,971 Duration (y) 0.059⫾0.025 ⬍0.02 1,971 Ionized calcium (mg/dL) ⫺0.97⫾0.1 ⬍0.001 1,971 Phosphate (mg/dL) 0.11⫾0.017 ⬍0.01 1,971 Albumin (g/dL) 0.23⫾0.07 ⬍0.02 1,971 Magnesium (mEq/L) ⫺0.19⫾0.09 ⬍0.05 915 NOTE. Dependent variable is logPTH level (1,971 data points); independent variables are diabetes, vitamin D use, age, duration of dialysis therapy, rHuEPO dosage, and hemoglobin, albumin, creatinine, ionized calcium, and phos-phate levels. Note that magnesium level was included in only a subset of patients with no missing magnesium values (915 data points). Only results with P less than 0.05 are listed.
ter adjusting for five traditional risk factors (dia-betes, age, albumin level, creatinine level, and URR) and duration of dialysis therapy (Fig 3B).
In addition, time-dependent PTH levels (hazard ratio, 0.63 [range, 0.48⬃ 0.84]; P ⬍ 0.005) also were independently associated with less mor-tality.
DISCUSSION
In the cross-sectional study, relatively hypo-parathyroid patients were older, more likely to have diabetes, and had greater ionized calcium and lower phosphate, albumin, BUN, and creati-nine levels. However, there was no difference in aluminum or 1,25(OH)2D levels or URRs be-tween patients with and without relative hypo-parathyroidism. There also was no difference in PTH levels between patients administered either calcium carbonate or aluminum hydroxide alone as phosphate binders. Multiple regression showed that PTH level was only associated directly with creatinine level and inversely with age and ion-ized calcium level. In addition, mean enrollment serum aluminum level was high (53.5 to 62.1 g/L) in patients. However, serum aluminum levels decreased with time (56.7⫾ 7 and 24.3 ⫾ 9.5 g/L in 1992 and 2000, respectively) be-cause of the increasing awareness of aluminum toxicity.
This was the first use of a longitudinal study to examine factors associated with time-dependent PTH levels within clusters (individual patients and subgroups of patients) and between clusters over time in HD patients. Thus, we found that uremic hypoparathyroidism was a time-depen-dent phenomenon modifiable by multiple fac-tors. In addition, by increasing the number of observations (from 126 to 1,971 observations) and statistical power, five more risk factors (vita-min D use, duration of dialysis therapy, and albumin, phosphate, and magnesium levels) were Fig 2. (A) Serial PTH lev-els in 101 patients who were not censored, ie, alive (nⴝ 56) or dead (nⴝ45) by year 5 of follow-up. (B) Serial PTH levels in 63 patients with ini-tial hypoparathyroidism who were either alive (nⴝ33) or dead (nⴝ30) by year 5 of follow-up. Horizontal line is the cutoff value for PTH (200 pg/mL).
Fig 3. Cumulative survival by (A) Kaplan-Meier and (B) Cox proportional hazards survival analysis in 126 HD patients. Mortality was highest in patients with initial PTH levels less than 65 pg/mL and lowest in patients with initial PTH levels greater than 200 pg/mL either (A) before or (B) after adjustment for traditional risk factors (diabetes, age, albumin and creatinine levels, and URR) and duration of dialysis therapy.
found in the longitudinal study than in the cross-sectional study.
The association between PTH and ionized calcium, phosphate, and magnesium levels in previous cross-sectional studies4,5,16 was con-firmed by our longitudinal study. This is impor-tant because we are concerned with relationships between PTH levels and these variables in indi-vidual patients over time instead of a population in cross-section. We also found that time-depen-dent PTH levels were associated directly with time-dependent serum albumin levels. Interest-ingly, albumin, BUN, creatinine, and phosphate are markers of nutrition.17-19Because relatively hypoparathyroid patients were older and had lower albumin, BUN, creatinine, and phosphate levels, whereas absolutely hypoparathyroid pa-tients had lower nPCRs, we speculate that they were malnourished. PTH level was inversely associated with modified subjective global assess-ment in a recent cohort of our HD patients (n⫽ 79; P⬍ 0.05), in which a high score indicates malnutrition.20 Similar speculation has been raised by a recent review on adynamic bone diseases with low PTH levels.21Two recent stud-ies also showed that a low-protein diet induced uremic hypoparathyroidism.22,23
Note that attending physicians prescribed vita-min D in hyperparathyroid patients and withheld vitamin D in hypoparathyroid patients during the longitudinal study; therefore, vitamin D use was associated directly with PTH level. A recent study also failed to increase PTH levels in ure-mic hypoparathyroid patients despite withhold-ing vitamin D for 11 months.24 Of course, vita-min D treatment would predispose dialysis patients to hypoparathyroidism and adynamic bone disease in prospective studies.25
Diabetes has been associated with uremic hy-poparathyroidism.1,6,26A 1990 study found that a high glucose level inhibits PTH secretion in cultured parathyroid cells.27 A cross-sectional study also found an inverse association between plasma glucose and PTH levels in predialytic patients with diabetes by univariate analyses.28 However, by using multivariate analyses, our cross-sectional and longitudinal studies did not show a relationship between diabetes per se and PTH level or glycemic control (short or long term) and PTH level. Therefore, we suggest that aging, short duration of dialysis therapy,
hy-pophosphatemia, and hypoalbuminemia ac-counted for uremic hypoparathyroidism in pa-tients with diabetes.
Secondary hyperparathyroidism is associated with rHuEPO resistance, whereas rHuEPO in-creases survival in prospective studies.29 How-ever, we found no association between PTH level, survival, and rHuEPO use and/or hemoglo-bin level in cross-sectional and longitudinal stud-ies. We also have shown that rHuEPO failed to affect PTH level in a previous prospective study.11 The lack of association between survival and rHuEPO use and/or hemoglobin level can be explained because this was a retrospective study, whereas Health Insurance Agencies require that the maximum hemoglobin level and rHuEPO dosage be kept at 10 g/dL and 20,000 U/mon, respectively.
The mechanism of uremic hypoparathyroid-ism is not known, although vitamin D receptor gene polymorphism has been proposed.30In addi-tion, as in secondary hyperparathyroidism, a cal-cium-sensing receptor abnormality also is an intriguing possibility.31 Decreased PTH respon-siveness to hypocalcemia was even suggested by a study using the less specific C-terminal PTH assay in HD patients.32However, we did not find a difference in the slope of the PTH-ionized calcium regression curve between patients with and without hypoparathyroidism in the cross-sectional study. A similar finding was shown by a study of adynamic bone diseases.33
After adjusting for traditional risk factors (dia-betes, age, albumin level, creatinine level, and URR)16 and duration of dialysis therapy,34 we found that hypoparathyroidism was indepen-dently associated with mortality in HD patients. Moreover, lower time-dependent PTH levels were independently associated with mortality. This observation is surprising because secondary hy-perparathyroidism has been associated with many adverse effects in uremic patients.3
Because patients with adynamic bone disease can develop hypercalcemia,35one explanation is that uremic hypoparathyroidism is associated with vascular calcifications and cardiovascular complications.36,37 Vascular calcification may cause arterial stiffening,35,38atherosclerosis, and mortality38-40 in HD patients. Administration of calcium and vitamin D often leads to hypercalce-mia, relative hypoparathyroidism, and tissue
cal-cification.37,38,41 We found that cardiovascular mortality was more prevalent in patients with enrollment hypoparathyroidism.
A second explanation is that uremic hypopara-thyroidism may be associated indirectly with mortality by its association with malnutrition. Thus, we found that patients who died had lower albumin levels and nPCRs than those who sur-vived by year 5. However, multivariate survival analysis showed that survival was associated with albumin level, but not nPCR. This observa-tion was corroborated by another large study.42 Dissociation of albumin level and nPCR in sur-vival analysis may be explained because hy-poalbuminemia is the combined result of malnu-trition and inflammation, whereas inflammation per se also can increase mortality in HD pa-tients.18
A third explanation is that uremic hypoparathy-roidism is associated with increased fractures, which have high mortality rates.43,44 However, we found that fracture was not more prevalent in patients who died or those with enrollment hypo-parathyroidism by year 5 of follow-up. Finally, the possibility that severe hyperparathyroidism may be associated with mortality cannot be ruled out in this study because we excluded patients with a previous parathyroidectomy and intrave-nous high-dose active vitamin D treatment.
It is tempting to speculate that treating uremic hypoparathyroidism may decrease mortality. Un-fortunately, there is no known treatment for ure-mic hypoparathyroidism.2 However, we found that PTH levels fluctuated and the state of rela-tive hypoparathyroidism was changeable in 49% of hypoparathyroid patients. In addition, among risk factors found in the longitudinal study, cal-cium, phosphate, and magnesium levels can be modulated. Unfortunately, traditional therapies for renal osteodystrophy have potentially ad-verse clinical consequences.35-38,41,45 For ex-ample, it is almost impossible to control hyper-phosphatemia with diet without inducing malnutrition.46Accordingly, novel therapies (cal-cium and aluminum-free phosphate binders, vita-min D analogues with vita-minimal calcemic effects, and calcimimetic agents) have been designed to reduce the risk for calcification.45 It remains to be seen whether these therapies will prevent relative hypoparathyroidism in HD patients.
We used dialysate calcium concentrations of
2.5 to 3.5 mEq/L. Current recommendations for dialysate calcium are approximately 2.5 to 3.5 mEq/L for patients administered calcium, 3.3 to 3.5 mEq/L for patients not administered calcium, and 2.5 to 3.0 mEq/L for patients on vigorous vitamin D therapy or with hypercalcemia.47 A low calcium dialysate level (2.5 mEq/L)48,49and phosphate supplement can reverse uremic hypo-parathyroidism.4Avoidance of vitamin D over-use also is a prudent choice. Finally, it remains to be seen whether improving nutrition ameliorates uremic hypoparathyroidism.
We conclude that relative hypoparathyroidism was prevalent in HD patients, although not asso-ciated with diabetes per se. Time-dependent PTH levels fluctuated with time and were associated with age, duration of dialysis therapy, and time-dependent ionized calcium, phosphate, albumin, and magnesium levels. Moreover, relative hypo-parathyroidism at entry and lower time-depen-dent PTH levels predict mortality.
ACKNOWLEDGMENT
The authors thank the staff in the Dialysis Units of Kaohsiung Medical University and Sin-Lau Christian Hospi-tal for help in recruiting patients.
REFERENCES
1. Akizawa T, Kinugasa E, Akiba T, Tsukamoto Y, Kuro-kawa K: Incidence and clinical characteristics of hypopara-thyroidism in dialysis patients. Kidney Int 52:S72-S74, 1997 (suppl 62)
2. Cannata Andia JB: Adynamic bone and chronic renal failure: An overview. Am J Med Sci 320:81-84, 2000
3. Hruska KA, Teitelbaum SL: Renal osteodystrophy. N Engl J Med 333:166-174, 1995
4. Carvalho AB, Lobao RR, Cuppari L, Draibe SA, Ajzen H: Does hypophosphataemia induce hypoparathyroidism in pre-dialysis patients? Nephrol Dial Transplant 13:S12-S14, 1998 (suppl 3)
5. Navarro JF, Mora C, Jimenez A, Torres A, Macia M, Garcia J: Relationship between serum magnesium and para-thyroid hormone levels in hemodialysis patients. Am J Kidney Dis 34:43-48, 1999
6. Niikura K, Akizawa T, Satoh Y, et al: Relative hypopara-thyroidism in hemodialysis patients. Miner Electrolyte Metab 21:101-103, 1995
7. Takeuchi M, Kurihara S, Iino Y, Terashi A: Hypopara-thyroidism in maintenance dialysis patients (Pts)—A clini-cal study. Nippon Ika Daigaku Zasshi 65:236-240, 1998
8. Silver J, Sela SB, Naveh MT: Regulation of parathy-roid cell proliferation. Curr Opin Nephrol Hypertens 6:321-326, 1997
9. Samet JM: Concepts of time in clinical research. Ann Intern Med 132:37-44, 2000
kinetic modeling exaggerates the relationship between nutri-tion and dialysis in CAPD patients. (The hazards of cross-sectional analysis). Perit Dial Int 15:105-109, 1995
11. Lai YH, Tsai JC, Chen HC, Guh JY, Hwang SJ, Tsai JH: Lack of influence of recombinant human erythropoietin on parathyroid function in hemodialysis patients with second-ary hyperparathyroidism. Nephron 70:223-228, 1995
12. Sakhaee K: Is there an optimal parathyroid hormone level in end-stage renal failure: The lower the better? Curr Opin Nephrol Hypertens 10:421-427, 2001
13. Avram MM, Sreedhara R, Avram DK, Muchnick RA, Fein P: Enrollment parathyroid hormone level is a new marker of survival in hemodialysis and peritoneal dialysis therapy for uremia. Am J Kidney Dis 28:924-930, 1996
14. Guh JY, Yang CY, Yang JM, Chen LM, Lai YH: Prediction of equilibrated postdialysis BUN by an artificial neural network in high-efficiency hemodialysis. Am J Kid-ney Dis 31:638-646, 1998
15. Zeger SL, Liang KY: An overview of methods for the analysis of longitudinal data. Stat Med 11:1825-1839, 1992 16. Heaf JG, Lokkegard H: Parathyroid hormone during maintenance dialysis: Influence of low calcium dialysate, plasma albumin and age. J Nephrol 11:203-210, 1998
17. Lowrie EG: Chronic dialysis treatment: Clinical out-come and related processes of care. Am J Kidney Dis 24:255-266, 1994
18. Don BR, Kaysen GA: Assessment of inflammation and nutrition in patients with end-stage renal disease. J Nephrol 13:249-259, 2000
19. Subramanian R, Khardori R: Severe hypophos-phatemia. Pathophysiologic implications, clinical presenta-tions, and treatment. Medicine 79:1-8, 2000
20. Kalantar-Zadeh K, Kleiner M, Dunne E, Lee GH, Luft FC: A modified quantitative subjective global assess-ment of nutrition for dialysis patients. Nephrol Dial Trans-plant 14:1732-1738, 1999
21. Fukagawa M, Akizawa T, Kurokawa K: Is aplastic osteodystrophy a disease of malnutrition? Curr Opin Neph-rol Hypertens 9:363-367, 2000
22. Lafage-Proust MH, Combe C, Barthe N, Aparicio M: Bone mass and dynamic parathyroid function according to bone histology in nondialyzed uremic patients after long-term protein and phosphorus restriction. J Clin Endocrinol Metab 84:512-519, 1999
23. Lorenzo V, Martin M, Rufino M, et al: Protein intake, control of serum phosphorus, and relatively low levels of parathyroid hormone in elderly hemodialysis patients. Am J Kidney Dis 37:1260-1266, 2001
24. Kondo M, Hyodo T, Sakai T: Vitamin D3withdrawal
in hemodialysis patients with adynamic bone disease. Nephron 80:89, 1998
25. Goodman WG, Ramirez JA, Belin TR, et al: Develop-ment of adynamic bone in patients with secondary hyperpara-thyroidism after intermittent calcitriol therapy. Kidney Int 46:1160-1166, 1994
26. Pei Y, Hercz G, Greenwood C, et al: Renal osteodys-trophy in diabetic patients. Kidney Int 44:159-164, 1993
27. Sugimoto T, Ritter C, Morrissey J, Hayes C, Slatopol-sky E: Effects of high concentrations of glucose on PTH secretion in parathyroid cells. Kidney Int 37:1522-1527, 1990
28. Martinez I, Saracho R, Moina I, Montenegro J, Llach F: Is there a lesser hyperparathyroidism in diabetic patients with chronic renal failure? Nephrol Dial Transplant 13:S9-S11, 1998 (suppl 3)
29. Sunder-Plassmann G, Horl WH: Novel aspects of erythropoietin response in renal failure patients. Nephrol Dial Transplant 16:S40-S44, 2001 (suppl 5)
30. Fernandez E, Fibla J, Betriu A, Piulats JM, Almirall J, Montoliu J: Association between vitamin D receptor gene polymorphism and relative hypoparathyroidism in patients with chronic renal failure. J Am Soc Nephrol 8:1546-1552, 1997
31. Brown EM: Physiology and pathophysiology of the extracellular calcium-sensing receptor. Am J Med 106:238-253, 1999
32. Heidbreder E, Gotz R, Schafferhans K, Heidland A: Diminished parathyroid gland responsiveness to hypocalce-mia in diabetic patients with urehypocalce-mia. Nephron 42:285-289, 1986
33. Goodman WG, Veldhuis JD, Belin TR, Juppner H, Salusky IB: Suppressive effect of calcium on parathyroid hormone release in adynamic renal osteodystrophy and secondary hyperparathyroidism. Kidney Int 51:1590-1595, 1997
34. Block GA, Hulbert-Shearon TE, Levin NW, Port FK: Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: A national study. Am J Kidney Dis 31:607-617, 1998
35. Guerin AP, London GM, Marchais SJ, Metivier F: Arterial stiffening and vascular calcifications in end-stage renal disease. Nephron Dial Transplant 15:1014-1021, 2000 36. Urena P, Malergue MC, Goldfarb B, et al: Evolutive aortic stenosis in hemodialysis patients: Analysis of risk factors. Nephrologie 20:217-225, 1999
37. Tsuchihashi K, Takizawa H, Torii T, et al: Hypopara-thyroidism potentiates cardiovascular complications through disturbed calcium metabolism: Possible risk of vitamin D(3) analog administration in dialysis patients with end-stage renal disease. Nephron 84:13-20, 2000
38. Meeus F, Kourilsky O, Guerin AP, Gaudry C, Mar-chais SJ, London GM: Pathophysiology of cardiovascular disease in hemodialysis patients. Kidney Int 58:S140-S147, 2000 (suppl 76)
39. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM: Impact of aortic stiffness on survival in end-stage renal disease. Circulation 99:2434-2439, 1999
40. van Popele NM, Grobbee DE, Bots ML, et al: Asso-ciation between arterial stiffness and atherosclerosis: The Rotterdam Study. Stroke 32:454-460, 2001
41. Hsu CH: Are we mismanaging calcium and phos-phate metabolism in renal failure? Am J Kidney Dis 29:641-649, 1997
42. Combe C, Chauveau P, Laville M, et al: Influence of nutritional factors and hemodialysis adequacy on the sur-vival of 1,610 French patients. Am J Kidney Dis 37:S81-S88, 2001 (suppl 2)
43. Atusmi K, Kushida K, Yamazaki K, Shimizu S, Ohmura A, Inoue T: Risk factors for vertebral fractures in renal osteodystrophy. Am J Kidney Dis 33:287-293, 1999
in dialysis patients with low serum parathyroid hormone. Am J Kidney Dis 36:1115-1121, 2000
45. Goodman WG: Recent developments in the manage-ment of secondary hyperparathyroidism. Kidney Int 59:1187-1201, 2001
46. Rufino M, de Bonis E, Martin M, et al: Is it possible to control hyperphosphataemia with diet, without inducing protein malnutrition? Nephrol Dial Transplant 13:S65-S67, 1998 (suppl 3)
47. Cunningham J: Calcium concentration in the
dialy-sate and calcium supplements. Nephrol Dial Transplant 15:S34-S35, 2000 (suppl 5)
48. Holgado R, Haire H, Ross D, et al: Effect of a low calcium dialysate on parathyroid hormone secretion in dia-betic patients on maintenance hemodialysis. J Bone Miner Res 15:927-935, 2000
49. Sanchez Perales MC, Garcia Cortes MJ, Borrego FJ, et al: Hemodialysis with 2.5 mEq/L of calcium in relative hypoparathyroidism: Long-term effects on bone mass. Nefro-logia 20:254-261, 2000