Many studies have documented significant cardiovascular effects by coarse particles with diameters < 10 µm (PM10) and fine particles
with diameters < 2.5 µm (PM2.5) (Pope and
Dockery 1999; Samet et al. 2000). By con-trast, relatively few studies reported such effects from either submicrometer particles with particle sizes < 1.0 µm in diameter (PM1.0) or ultrafine particles with particle
sizes < 0.1 µm in diameter. One recent epi-demiologic study showed that exposure to ultrafine particles measured by number con-centrations can also increase cardiorespiratory symptoms for elderly patients with coronary heart disease (de Hartog et al. 2003). It was previously proposed that ultrafine particle lev-els measured by number concentrations increase the probability of death for persons with cardiovascular diseases, probably as a result of PM-induced inflammatory response (Seaton et al. 1995). The toxicity of ultrafine and submicrometer particles was also sup-ported by several previous toxicologic studies. Studies have shown that ultrafine particles caused damage to epithelial cells, pulmonary edema, and eventually fibrosis (Churg 1996; Ferin 1994) and that submicrometer particles induced cytokine production and lipid peroxidation of human bronchial epithelial cells (Huang et al. 2003). One animal study showed that there was far more broncho-alveolar inflammation in rats exposed to ultrafine particles when they were exposed to
an equal mass concentration of fine and ultra-fine titanium dioxide (Ferin et al. 1992).
Several panel studies on heart rate variabil-ity (HRV) in human subjects exposed to PM10and PM2.5have demonstrated that
autonomic imbalance was another possible mechanism of PM-induced cardiovascular effects. Increased mass concentrations of PM10 and PM2.5 were associated with
decreased standard deviations of all normal-to-normal (NN) intervals (SDNN) and square root of the mean of the sum of the squares of differences between adjacent NN intervals (r-MSSD) in the elderly with preexisting chronic obstructive pulmonary disease or cardiovascular disease (Gold et al. 2000; Pope et al. 1999). Increased PM2.5mass
concentra-tions were also related to the decrease in low frequency (LF; 0.04–0.15 Hz) and high fre-quency (HF; 0.15–0.40 Hz) in the elderly (Liao et al. 1999). One study also found that healthy worker’s SDNN was significantly decreased by high occupational and environ-mental PM2.5mass concentration exposures
(Magari et al. 2001, 2002). However, it is still unclear whether smaller ambient particles, such as PM1.0and ultrafine particles, have the
same effects on HRV as do coarse and fine particles in the elderly and in healthy sub-jects. Therefore, we designed this panel study to investigate whether submicrometer parti-cles with a size range of 0.02–1 µm measured by number concentrations (NC0.02–1) are
associated with HRV changes in both young adults and the elderly patients with lung function impairments.
Materials and Methods
Subjects. This panel study was designed to monitor changes in PM concentrations and HRV continuously and simultaneously in study subjects in general environments. There were two panels of our study subjects: 9 young adults and 10 elderly patients with lung function impairments. Young and healthy adults were recruited through on-campus advertisement at National Taiwan University. Fifteen students responded to our advertisement, but only nine were willing to participate in our study after we explained to them our monitoring protocols (response rate = 60%). The elderly patients were recruited from the Chest Department of Taipei Veterans General Hospital. Our selec-tion criteria for lung funcselec-tion impairment was that the patient’s ratios of forced expira-tory volume in 1 sec (FEV1) to forced vital
capacity (FVC), FEV1/FVC, should be
< 85%. To avoid the effects of coexisting dis-eases on HRV, we selected our elderly sub-jects based on the following exclusion criteria: those with hyperthyroidism, acute cardiopulmonary failure, paced cardiac rhythm, or using medications that may affect cardiac rhythm, such as anticholinergics, beta-blockers, anti-arrhythmic agents, and so forth. Nineteen patients met our selection criteria, but only 10 were willing to partici-pate in our study after we explained to them our monitoring protocols (response rate = 53%). The FEV1/FVC values for these 10
elderly patients were all < 84%. No partici-pant used cardiac-rhythm–related medica-tion during the monitoring period. The Institutional Review Board of Taipei Veterans General Hospital approved the Address correspondence to C.-C. Chan, Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, Room 1447, 1st Section, No. 1 Jen-ai Rd., Taipei 100, Taiwan. Telephone/Fax: 886-2-2322-2362. E-mail: [email protected]
This study was supported by a grant from the National Science Council of Taiwan (NSC90-2320-B-002-126).
The authors declare they have no competing financial interests.
Received 8 December 2003; accepted 4 March 2004.
Personal Exposure to Submicrometer Particles and Heart Rate Variability in
Human Subjects
Chang-Chuan Chan,1Kai-Jen Chuang,1Guang-Ming Shiao,2and Lian-Yu Lin3
1Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan; 2Chest Department, Taipei Veterans General Hospital, Taipei, Taiwan; 3Internal Medicine Department, National Taiwan University
Hospital, Taipei, Taiwan
We conducted a study on two panels of human subjects—9 young adults and 10 elderly patients with lung function impairments—to evaluate whether submicrometer particulate air pollution was associated with heart rate variability (HRV). We measured these subjects’ electrocardiography and personal exposure to number concentrations of submicrometer particles with a size range of 0.02–1 µm (NC0.02–1) continuously during daytime periods. We used linear mixed-effects models
to estimate the relationship between NC0.02–1and log10-transformed HRV, including standard
deviation of all normal-to-normal intervals (SDNN), square root of the mean of the sum of the squares of differences between adjacent NN intervals (r-MSSD), low frequency (LF, 0.04–0.15 Hz), and high frequency (HF, 0.15–0.40 Hz), adjusted for age, sex, body mass index, tobacco exposure, and temperature. For the young panel, a 10,000-particle/cm3increase in NC
0.02–1with 1–4 hr
moving average exposure was associated with 0.68–1.35% decreases in SDNN, 1.85–2.58% decreases in r-MSSD, 1.32–1.61% decreases in LF, and 1.57–2.60% decreases in HF. For the elderly panel, a 10,000-particle/cm3increase in NC
0.02–1with 1–3 hr moving average exposure
was associated with 1.72–3.00% decreases in SDNN, 2.72–4.65% decreases in r-MSSD, 3.34–5.04% decreases in LF, and 3.61–5.61% decreases in HF. In conclusion, exposure to
NC0.02–1was associated with decreases in both time-domain and frequency-domain HRV indices
in human subjects. Key words: air pollution, autonomic system, epidemiology, heart rate variability, submicrometer particle. Environ Health Perspect 112:1063–1067 (2004). doi:10.1289/ehp.6897 available via http://dx.doi.org/ [Online 4 March 2004]
research protocol, and a written informed consent was obtained from each participant.
Continuous Holter monitoring and tape processing. We performed continuous ambula-tory electrocardiographic (ECG) monitoring on each study subject by using a three-channel ambulatory ECG recorder (PacerCorder model 461A; Del Mar Medical Systems LLC., Irvine, CA, USA) with a sampling rate of 250 Hz (4 msec). We sent ECG tapes to National Taiwan University Hospital and analyzed them by using a Delmar 563 Holter analysis system (version 2.47; Del Mar). The electro-cardiographic wave complexes (QRS) were automatically classified and manually verified as normal sinus rhythm, arterial or ventricular premature beats, or noise by comparison of the adjacent QRS morphologic features. The NN intervals were deduced from the adjacent normal sinus beats. The NN interval time series were then transferred to a personal computer and postprocessed by a program written in Matlab language (version 5.2; MathWorks Inc., Natick, MA, USA). The missing intervals of the raw NN data were linearly interpolated and resampled at 4 Hz by the Ron-Berger method. Each 5-min segment of NN intervals was taken for HRV analysis. The time-domain measurements of HRV were SDNN and r-MSSD. The frequency-domain measurements of HRV were LF and HF, which were calculated by Welch’s aver-aged periodogram of the NN intervals (Task Force 1996; Welch 1967). To avoid sleep effects on HRV, we used the Holter measure-ments when the subjects were awake between 0700 hr and 2300 hr for data analysis in this study.
Exposure measurements. We performed personal monitoring of NC0.02–1for each
study subject by using a P-TRAK Ultrafine Particle Counter (model 8525; TSI Inc., Shoreview, MN, USA), which measured and reported 1-min NC0.02–1continuously. The
1-min raw data were then summarized to
5-min segments for statistical analysis. We asked each young adult to carry the P-TRAK personally and assigned a technician carrying a P-TRAK to accompany each elderly patient from 0700 hr and 2300 hr to measure per-sonal NC0.02–1exposure during participants’
daytime normal activities. We used a general-purpose condensation particle counter (CPC; model 3022A; TSI Inc.), which measured NC0.005–1, to validate the measurements of
NC0.02–1by the P-TRAK before performing
the study. Concurrent measurements of sub-micrometer particles by the CPC and the P-TRAK in our aerosol laboratory showed high association between two monitors in total counts of submicrometer particles (r2=
0.99) during the experimental period. The CPC with a wider size range also consistently reported approximately 30% more counts of submicrometer particles than the P-TRAK in our validation test. We also performed a zero check on P-TRAK by measuring HEPA-filtered air before each field application.
Other personal variables. Each partici-pant’s age, sex, body mass index (BMI), and medical history were recorded by a standard-ized questionnaire. Young adults themselves and the technician for the elderly recorded the participant’s time–activity patterns and envi-ronmental tobacco smoke exposures during the monitoring period.
Statistical analysis. We first plotted NC0.02–1by HRV indices for individual
sub-jects to determine whether there were observed associations between these two vari-ables and whether such associations were heavily influenced by any outliers or were homogeneous across subjects. We then applied linear mixed-effects regression models to estimate the association between NC0.02–1
and log10-transformed HRV measurements
by using general additive procedures in the S-PLUS 2000 program (MathSoft Inc., Cambridge, MA, USA). We treated subjects’ sex, age, BMI, and tobacco exposure as
time-invariant variables, and NC0.02–1,
tem-perature, and HRV as time-varying variables, in our data analysis. The exposure variables were 1–4 hr moving averages of NC0.02–1in
our models. The outcome variables were log10-transformed HRV, which were SDNN,
r-MSSD, LF, and HF. Such mixed-effects models had the advantage of adjusting for invariant variables by fixed-effects models and accounting for individual differences by random-effects models. In our mixed-effects models, we treated subjects’ sex, age, BMI, tobacco exposure, ambient temperature, and NC0.02–1as fixed effects and each subject as a
random effect. To control all key variables in a relatively small sample size, we stratified the age variable at 65 years of age for the elderly panel and the BMI variable at 22 kg/m2for
both panels in our models. A total of eight sets of mixed-effects models were constructed separately to estimate NC0.02–1effects on
HRV at 1–4 hr moving averages for the young panel and the elderly panel.
Results
Study participants’ personal characteristics and environmental exposures of two study panels are summarized in Table 1. The 9 young adults (7 males, 2 females) were 19–29 years of age (mean ± SD, 23.2 ± 2.9 years), and their BMI ranged from 20.1 to 34.4 kg/m2(mean ±
SD, 24.8 ± 4.3 kg/m2). The 10 elderly patients
were all male and were from 42 to 79 years of age (mean ± SD, 58.3 ± 13.4 years), and their BMI values were from 20.6 to 33.8 kg/m2
(26.9 ± 3.9 kg/m2). Subjects in the elderly
panel averaged about 35 years older than those in the young panel.
The values of HRV indices in Table 1 were the means of the averages for each par-ticipant during the 16-hr monitoring period. Average heart rates were 87.5 ± 9.2 beats per minute (bpm) in the 9 young adults and 75.9 ± 8.6 bpm in the 10 elderly patients. The log10 SDNN, log10 r-MSSD, log10LF, and
log10HF in the two panels were, respectively,
1.66 ± 0.15 msec, 0.99 ± 0.15 msec, 3.02 ± 0.50 msec2, and 2.45 ± 0.51 msec2in the
young panel, and 1.61 ± 0.25 msec, 1.01 ± 0.28 msec, 2.42 ± 0.59 msec2, and 2.11 ±
0.67 msec2in the elderly panel. The heart
rate and most HRV indices in the young panel were significantly higher than those in the elderly panel, except for r-MSSD.
Also presented in Table 1 are the personal monitoring results of 5-min NC0.02–1. The
5-min NC0.02–1 ranged from 6,127 to
351,003 particles/cm3for the young panel and
from 1,712 to 210,973 particles/cm3for the
elderly panel. Means of 5-min NC0.02–1
expo-sures were comparable between the young panel (23,407 ± 19,836 particles/cm3) and the
elderly panel (25,529 ± 20,783 particles/cm3)
during the study. However, wide fluctuation
Table 1. Study participants’ personal characteristics and environmental exposures [mean ± SD (range)].
Difference Characteristics Young panel Elderly panel between panels
No. of subjects 9 10 Sex (no.) Female 2 0 Male 7 10 Age (years) 23.2 ± 2.9 (19–29) 58.3 ± 13.4 (42–79) * BMI (kg/m2) 24.8 ± 4.3 (20.1–34.4) 26.9 ± 3.9 (20.6–33.8) * Heart rate (bpm) 87.5 ± 9.2 (70–130) 75.9 ± 8.6 (61–89) * Time-domain HRV (msec) Log10SDNN 1.66 ± 0.15 (1.10–2.02) 1.61 ± 0.25 (0.88–2.05) * Log10r-MSSD 0.99 ± 0.15 (0.54–1.48) 1.01 ± 0.28 (0.42–1.64) * Frequency-domain HRV (msec2) Log10LF 3.02 ± 0.50 (0.96–3.90) 2.42 ± 0.59 (1.00–3.88) * Log10HF 2.45 ± 0.51 (0.44–3.33) 2.11 ± 0.67 (0.48–3.85) * NC0.02–15-min mean (particles/cm3) 23,407 ± 19,836 (6,127–351,003) 25,529 ± 20,783 (1,712–210,973) * Temperature (°C) 25.6 ± 2.4 (18.9–30.8) 24.4 ± 5.7 (12.6–34.4) *
in NC0.02–1as expressed in large standard
deviations in particle statistics indicated wide within-subject and between-subject varia-tions in NC0.02–1exposure during the study
period. The hourly ambient temperature dur-ing each participant’s monitordur-ing period ranged from 18.9 to 30.8°C for the 9 young adults and from 12.6 to 34.4°C for the 10 elderly patients.
The plots of NC0.02–1by HRV indices
revealed consistently negative associations between these two variables across all study subjects (data not shown). The observed asso-ciations seemed not to be influenced by any outlier observations. In our modeling results, regression of time-domain HRV indices on previous moving averages adjusted for potential confounders showed significantly negative asso-ciations between NC0.02–1moving averages and
5-min SDNN and r-MSSD values. Personal characteristics such as age, BMI, sex, and tobacco exposure did not affect the observed associations between NC0.02–1 and
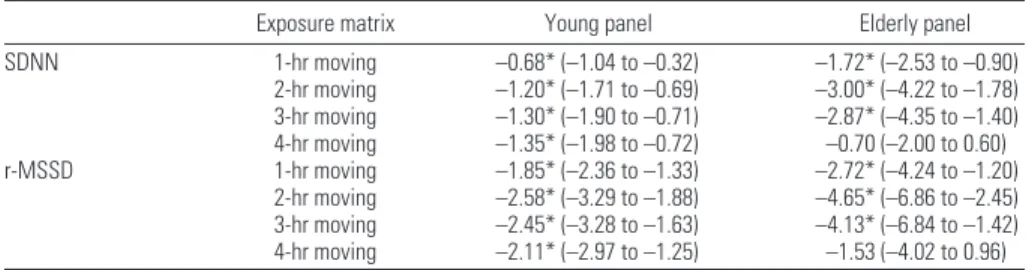
time-domain HRV indices. However, temperature was negatively associated with time-domain HRV indices. Table 2 lists percent changes in time-domain HRV indices for 10,000 particle/cm3NC
0.02–1exposures at 1-hr to
4-hr moving averages estimated by the mixed-effects models for the young and the elderly panels, respectively. NC0.02–1exposures
sig-nificantly decreased SDNN at 1-hr to 4-hr moving averages for the young panel and at 1-hr to 3-hr moving averages for the elderly panel. NC0.02–1exposures also significantly
decreased r-MSSD at 1-hr to 4-hr moving averages for the young panel and at 1-hr to 3-hr moving averages for the elderly panel. For 10,000-particle/cm3NC
0.02–1exposures,
SDNN was decreased by 0.68–1.35% for the young panel and 1.72–3.00% for the elderly panel. For 10,000-particle/cm3NC
0.02–1
expo-sures, r-MSSD was decreased by 1.85–2.58% for the young panel and 2.72–4.65% for the elderly panel. For the same hours of moving averages, the elderly panel’s regression coeffi-cients were consistently more negative than were the young panel’s coefficients. Our models also showed that 1-hr NC0.02–1
mov-ing averages had smaller effects on decreasmov-ing SDNN and r-MSSD compared with 2-hr and 3-hr NC0.02–1moving averages. We examined
the time course of NC0.02–1exposures only
up to 4-hr moving averages because available data were substantially decreased for moving averages > 5 hr.
Our models showed that NC0.02–1
expo-sure effects on frequency-domain HRV indices were similar to those of time-domain HRV indices described above. Frequency-domain HRV indices on previous moving averages adjusted for potential confounders showed significantly negative associations between NC0.02–1moving averages and the
5-min HF and LF. Again, temperature was the only confounder that was negatively asso-ciated with frequency-domain HRV indices. Table 3 lists percent changes in frequency-domain HRV indices for 10,000-particle/cm3
NC0.02–1exposures at 1-hr to 4-hr moving
averages estimated by the mixed-effects models for the young and the elderly panels, respec-tively. NC0.02–1 exposures significantly
decreased LF and HF at 1-hr to 4-hr moving averages for the young panel, but significantly decreased LF and HF at 1-hr to 3-hr moving averages for the elderly panel. For 10,000-particle/cm3NC
0.02–1exposures, LF was
decreased by 1.41–1.61% for the young panel and 3.34–5.04% for the elderly panel. For 10,000-particle/cm3NC
0.02–1exposures, HF
was decreased by 1.57–2.60% for the young panel and 3.61–5.61% for the elderly panel. The elderly panel had greater decreases in frequency-domain HRV indices in response to NC0.02–1exposure than did the young
panel. Only the elderly panel exhibited a time course effect of NC0.02–1on
frequency-domain HRV indices. The magnitude of decreasing LF and HF was the greatest at 2-hr moving averages for the elderly panel.
Discussion
This is the first study to demonstrate that per-sonal measurements of environmental expo-sure to NC0.02–1can affect HRV in human
subjects. The main effects of NC0.02–1are to
decrease both time-domain indices (SDNN, r-MSSD) and frequency-domain indices (HF,
LF), which are consistent with the effects by PM2.5 in one previous study (Liao et al.
1999). Another interesting finding of our study is that NC0.02–1seems to exert similar
effects on HRV for both young adults and elderly patients. Our results further confirm that environmental PM can affect HRV both in the elderly with preexisting diseases (Gold et al. 2000; Pope et al. 1999) and in adults between 19 and 59 years of age (Magari et al. 2001). Our findings also support that the magnitudes of PM effects on HRV differ between elderly/less healthy and younger/ healthy groups. For 1-mg/m3PM
2.5
expo-sures in 4-hr moving average, Gold et al. (2000) reported a 17.4-msec decrease in SDNN among the elderly, whereas Magari et al. (2001) reported a 4.5-msec decrease in SDNN among the young adults. The com-parisons of these studies showed PM2.5
-induced autonomic function imbalance in the elderly was approximately four times stronger than that in young, healthy adults. Our study showed that percent decreases in log10SDNN
were two times greater among the elderly than among the young adults for 10,000-par-ticle/cm3NC
0.02–1exposures at 1-hr to 3-hr
moving averages. Apparently, these findings consistently show that the association between PM and HRV seems to be more pronounced among the elderly/less healthy population than among the younger/healthy population.
The profiles of cardiac autonomic altera-tion associated with submicrometer particle
Table 3. Percent changes (95% CI)ain frequency-domain HRV indices for NC
0.02–1exposures of 10,000
par-ticles/cm3estimated by mixed-effects models.
Exposure matrix Young panel Elderly panel LF 1-hr moving –1.41* (–2.11 to –0.71) –3.34* (–4.64 to –2.07) 2-hr moving –1.32* (–2.29 to –0.35) –5.04* (–6.96 to –3.12) 3-hr moving –1.03 (–2.09 to 0.02) –4.35* (–6.77 to –1.94) 4-hr moving –1.61* (–2.69 to –0.54) –0.57 (–2.66 to 1.52) HF 1-hr moving –2.60* (–3.45 to –1.75) –3.61* (–5.23 to –2.00) 2-hr moving –2.22* (–3.43 to –1.00) –5.61* (–8.03 to –3.19) 3-hr moving –1.57* (–2.99 to –0.15) –4.97* (–7.93 to –2.00) 4-hr moving –2.01* (–3.46 to –0.56) –1.51 (–4.13 to 1.11)
CI, confidence interval.
aThe model of the young panel was adjusted for sex, BMI, tobacco exposure, and temperature, whereas the model of the
elderly panel was adjusted for age, BMI, tobacco exposure, and temperature. *p < 0.05.
Table 2. Percent changes (95% CI)ain time-domain HRV indices for NC
0.02–1exposures of 10,000 particles/cm3
estimated by mixed-effects models.
Exposure matrix Young panel Elderly panel SDNN 1-hr moving –0.68* (–1.04 to –0.32) –1.72* (–2.53 to –0.90) 2-hr moving –1.20* (–1.71 to –0.69) –3.00* (–4.22 to –1.78) 3-hr moving –1.30* (–1.90 to –0.71) –2.87* (–4.35 to –1.40) 4-hr moving –1.35* (–1.98 to –0.72) –0.70 (–2.00 to 0.60) r-MSSD 1-hr moving –1.85* (–2.36 to –1.33) –2.72* (–4.24 to –1.20) 2-hr moving –2.58* (–3.29 to –1.88) –4.65* (–6.86 to –2.45) 3-hr moving –2.45* (–3.28 to –1.63) –4.13* (–6.84 to –1.42) 4-hr moving –2.11* (–2.97 to –1.25) –1.53 (–4.02 to 0.96)
CI, confidence interval.
aThe model of the young panel was adjusted for sex, BMI, tobacco exposure, and temperature, whereas the model of the
exposures are basically the same for both dysautonomic and nondysautonomic subjects. This suggests that there may be a common toxicologic mechanism of causing autonomic imbalance by submicrometer particles among various populations. However, the same physiologic perturbation of NC0.02–1
expo-sures may cause different detrimental effects to each population depending on their preex-isting cardiac conditions. The decrease of r-MSSD and HF components represents the withdrawal of vagal activity, which is an indi-cator of increasing cardiovascular events (Bigger et al. 1992; Kleiger et al. 1987). Even though the LF decrease is previously thought to represent decreased sympathetic activity, its real physiologic meaning remains unclear and is still debatable (Task Force 1996). One possible reason for LF decrease in our study is the decrease in total HRV (SDNN) by NC0.02–1.
The effects of different time course on HRV indicate that the magnitudes of decreas-ing SDNN, r-MSSD, LF, and HF increase as the averaging intervals of NC0.02–1reach
2–3 hr. Our findings suggest that NC0.02–1
can have both immediate and cumulative effects on cardiac autonomic function. It has been reported that particles can affect both sympathetic and parasympathetic nervous sys-tems directly in the immediate phase after exposures (Kodavanti et al. 2000; Lai and Kou 1998). One possible pathway of such a mechanism is the rapid passage of inhaled particles with diameters < 100 nm into the blood circulation reported in one recent study (Nemmar et al. 2002). In that study, ultrafine particles were found to diffuse into healthy volunteers’ systemic circulation 1 min after exposures and reached peak penetrations between 10 and 20 min after exposure. Because translocation of ultrafine particulates from airways into systemic circulation is reported to be very rapid, we speculate that direct myocardial effects rather than upper airway influences from air pollutants account for NC0.02–1effects on HRV in the
immedi-ate phase. The other possible pathway is that ultrafine particles deposited in the alveoli may increase blood coagulation via mechanisms of pulmonary inflammation or direct action on red blood cells (Donaldson et al. 2001; Peters et al. 1997; Seaton et al. 1999). Accordingly, we believe particle-induced pulmonary inflammation can also indirectly result in HRV changes or autonomic imbalance in the delayed phase after NC0.02–1exposures. This
may explain why HRV decreases peaked at 2–3 hr after NC0.02–1exposure in our study.
Short-term and small fluctuations of HRV indices have not been associated with higher risks of cardiovascular disease clinically. Cardiac death is a consequence of a complex interaction between the autonomic nervous
system, a myocardial substrate altered in the course of disease processes, and myocardial vulnerability leading to arrhythmogenic or ischemic response. The presence of a single condition is usually not sufficient to trigger death by cardiovascular disease (Zareba et al. 2001). Our findings, however, show that sub-micrometer particles are an environmental stressor, which may trigger a cascade of events by increasing sympathetic activation and may potentially lead to ischemia or fatal arrhythmia in high-risk patients with underlying cardiac abnormalities.
We believe that some key physiologic and environmental information, which was not available in our study, could possibly con-found our findings of HRV imbalance by NC0.02–1. First, we could not adjust the effect
of breathing patterns on HRV because they were not measured during the monitoring period. It has been reported that the quantity, periodicity, and timing of vagal cardiac out-flow were associated with variations of respi-ratory depth and interval in conscious young adults (Eckberg 1983). Second, we could not adjust respiration-modulated autonomic activity, especially HF and LF, in our study because we were unable to measure key respi-ration parameters, such as nasal and mouth airflow, chest wall movement, and abdominal movement, by polysomnography during the daytime monitoring period. Third, comor-bidity and medication among elderly patients could still confound our findings for NC0.02–1
effects on HRV even though we used very strict criteria to exclude cases with severe chronic diseases and specific medication from our study subjects. Fourth, the “personal cloud” effects of PM measurements could also confound our findings of the HRV effects rel-evant to environmental NC0.02–1(Harrison
et al. 2002; Wallace 1996). Because exposure measurements for two panels were different, the measurement bias attributable to “per-sonal cloud” effects could also be different between these two panels. The young sub-jects, who carried P-TRAK personally to measure their NC0.02–1exposures, were
expected to experience more diverse “personal cloud” effects than the elderly subjects, whose personal NC0.02–1was measured by a single
assistant. Fifth, other unmeasured personal exposures, such as PM2.5, ozone, nitric oxide,
carbon monoxide, and sulfur dioxide, may have confounded our findings of NC0.02–1
effects even though we failed to associate any of them with HRV changes by using exposure proxy from the fixed-site monitoring stations (data not shown), which measured hourly data of these air pollutants. Last, the effects of participants’ sex, age, and BMI on HRV still need further clarification because the sample size of our study may not be large enough to falsify their effects completely.
Regardless of these limitations, we believe our data generally indicate that submicrome-ter particles can disturb autonomic function in human subjects. However, we do not know whether such effects are caused by particle physical size alone or by the combined effects of the chemical/biologic components of parti-cles. We therefore recommend further studies to elucidate the clinical significance, biologic mechanisms, and dose–response relationships of the NC0.02–1effects on HRV.
REFERENCES
Bigger JT Jr, Fleiss JL, Steinman RC, Rolnitzky LM, Kleiger RE, Rottman JN. 1992. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 85:164–171.
Churg A. 1996. The uptake of mineral particles by pulmonary epithelial cell. Am J Respir Crit Care Med 154:1124–1140. de Hartog JJ, Hoek G, Peters A, Timonen KL, Ibald-Mulli B,
Brunekreef B, et al. 2003. Effects of fine and ultrafine particles on cardiorespiratory symptoms in elderly sub-jects with coronary heart disease. Am J Epidemiol 157:613–623.
Donaldson K, Stone V, Seaton A, MacNee W. 2001. Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ Health Perspect 109(suppl 4):523–527. Eckberg DL. 1983. Human sinus arrhythmia as an index of vagal
cardiac outflow. J Appl Physiol 54: 961–966.
Ferin J. 1994. Pulmonary retention and clearance of particles. Toxicol Lett 72:121–125.
Ferin J, Oberdorster G, Penny DP. 1992. Pulmonary retention of ultrafine and fine particle in rats. Am J Respir Cell Mol Biol 6:535–542.
Gold DR, Litonjua A, Schwartz J, Lovett EG, Larson AC, Nearing B, et al. 2000. Ambient pollution and heart rate variability. Circulation 101:1267–1273.
Harrison RM, Thornton CA, Lawrence RG, Mark D, Kinnersley RP, Ayres JG. 2002. Personal exposure monitoring of particulate matter, nitrogen dioxide, and carbon monoxide, including susceptible groups. Occup Environ Med 59:671–679. Huang SL, Hsu MK, Chan CC. 2003. Effects of submicrometer
particle compositions on cytokine production and lipid peroxidation of human bronchial epithelial cells. Environ Health Perspect 111:478–482.
Kleiger RE, Miller JP, Bigger JT Jr, Moss AJ. 1987. Decreased heart rate variability and its association with mortality after myocardial infarction. Am J Cardiol 113: 256–262. Kodavanti UP, Schladweiler MC, Ledbetter AD, Watkinson WP,
Campen MJ, Winsett DW. 2000. The spontaneously hyper-tensive rat as a model of human cardiovascular disease: evidence of exacerbated cardiopulmonary injury and oxidative stress from inhaled emission particulate matter. Toxicol Appl Pharmacol 164:250–263.
Lai CJ, Kou YR. 1998. Stimulation of vagal pulmonary c-fibers by inhaled wood smoke in rats. J Appl Physiol 84(1):30–36. Liao D, Creason J, Shy C, Williams R, Wattes R, Zweidinger R.
1999. Daily variation of particulate air pollution and poor cardiac autonomic control in the elderly. Environ Health Perspect 107:521–525.
Magari SR, Hauser R, Schwartz J, Williams PL, Smith TJ, Christiani DC. 2002. The association between personal measurements of environmental exposure to particulates and heart rate variability. Epidemiology 13:305–310. Magari SR, Hauser R, Schwartz J, Williams PL, Smith TJ,
Christiani DC. 2001. Association of heart rate variability with occupational and environmental exposure to particu-late air pollution. Circulation 104:986–991.
Nemmar A, Hoet PH, Vanquickenborne B, Dinsdale D, Thomeer M, Hoylaerts MF, et al. 2002. Passage of inhaled particles into the blood circulation in humans. Circulation 105:411–414. Peters A, Doring A, Wichmann HE, Koenig W. 1997. Increased
plasma viscosity during the 1985 air pollution episode: a link to mortality? Lancet 349:1582–1587.
Pope CA III, Dockery DW. 1999. Epidemiology of particle effects. In: Air Pollution and Health (Holgate ST, Samet JM, Koren HS, Maynard RL, eds). London:Academic Press, 673–705.
Kanner RE, et al. 1999. Heart rate variability associated with particulate air pollution. Am Heart J 138:890–899. Samet JM, Dominici F, Curriero FC, Coursac I, Zeger SL. 2000.
Fine particulate air pollution and mortality in 20 U.S. cities, 1987–1994. N Engl J Med 343:1742–1749.
Seaton A, MacNee W, Donaldson K, Godden D. 1995. Particulate air pollution and acute health effects. Lancet 345:176–178.
Seaton A, Soutar A, Crawford V, Elton R, McNerlan S, Cherrie J,
et al. 1999. Particulate air pollution and the blood. Thorax 54:1027–1032
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. 1996. Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation 93:1043–1065.
Wallace L. 1996. Indoor particles: a review. J Air Waste Manag Assoc 46:98–126.
Welch PD. 1967. The use of fast Fourier transform for the esti-mation of power spectra: a method based on time averag-ing over short, modified periodograms. IEEE Trans Audio Electroacoust 15:70–73.
Zareba W, Nomura A, Couderc JP. 2001. Cardiovascular effects of air pollution: what to measure in ECG? Environ Health Perspect 109(suppl 4):533–538.