Increased risk of epilepsy among patients diagnosed with chronic
osteomyelitis
Running head: Chronic osteomyelitis versus epilepsy
Chun-Hung Tsenga,d, Wei-Shih Huanga,d, Chih-Hsin Muob, and Chia-Hung Kaoc,d,*
a Department of Neurology, China Medical University Hospital, Taichung
40447, Taiwan
b Management Office for Health Data, China Medical University Hospital,
Taichung 40447, Taiwan
c Department of Nuclear Medicine and PET Center, China Medical University
Hospital, Taichung 40447, Taiwan
d School of Medicine, China Medical University College of Medicine, Taichung
40402, Taiwan
Drs. Tseng and Huang contributed equally to this work.
+886-4-22336174.
Summary
Purpose: Inflammatory processes, which raise the unsteadiness of brain
neuron membrane potentials, might enhance the development of epilepsy. Inflammation is a substantial indicator of epilepsy risk. In this study, we evaluated whether chronic osteomyelitis (COM), a chronic inflammatory disease, increases epilepsy risk.
Materials and Methods: A Taiwanese national insurance claims dataset of
more than 22 million enrollees was used to select 20,996 COM patients and 83,973 randomly selected age- and gender-matched controls to investigate epilepsy development over an 11-year follow-up period, starting on January 1, 2000 and ending on December 31, 2010. The epilepsy risk was analyzed using a Cox proportional hazards regression model.
Results: Comorbidities known to elevate epilepsy risk, including diabetes,
hypertension, head injury, stroke, and cancer, were commonly noted in the COM cohort, which had considerably higher risk of epilepsy than did the control group. Comparing only those without comorbidities, COM patients still exhibited higher epilepsy risk than the control group did (adjusted hazard ratio [aHR] = 3.87, 95% confidence interval [CI]: 3.01-4.98). The younger
4.00-9.30; age ≥ 65 y: aHR = 1.66, 95% CI: 1.28-2.16).
Conclusion: This is the first study linking COM to an increased risk in
epilepsy development. The results demonstrated that COM is a significant predictor of epilepsy. Further study of COM patients, particularly young patients, is recommended to facilitate epilepsy prevention.
KEYWORDS
Inflammation; Epilepsy; Chronic osteomyelitis
Hightlight
1. Epilepsy risks were increased in Chronic osteomyelitis patients. 2. Comorbidities were known to elevate epilepsy risk.
Introduction
Epilepsy is one of the most prevalent chronic neurological disorders worldwide (De Boer, et al., 2008; Pugliatti, et al., 2007; Vezzani, et al., 2011). The early
identification of risk factors for epilepsy, and its subsequent prevention, is a favored method for the lowering of epilepsy-related economic and health care burdens. Epilepsy can be triggered in some diseases by immune responses or inflammation processes that destabilize brain neuron membrane potentials (Vezzani, et al., 2011; Riazi, et al., 2008) and subsequently elicit, in these neurons, the spontaneous firing of excessively synchronous and sustained discharges (Vezzani, et al., 2011; Riazi, et al., 2008; Engelborghs, et al., 2000). Similar pathological discharges of brain neurons can also be induced by conventional risk factors of epilepsy, such as diabetes (Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013), hypertension (Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013), head injury (Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013), stroke (Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013), and cancer (Avila and Graber, 2010; Villanueva, et al., 2008). However, no risk factors are evident for 20%-80% of epilepsy patients, particularly in young populations (Ottman, et al., 1996; Mac, et al., 2007). Risk factors for epilepsy should be more rigorously investigated, in addition to the aforementioned well-documented factors.
Epilepsy caused by the pathogenic influence of chronic inflammatory processes on brain neurons has been observed in certain systemic or focal infectious diseases, such as sepsis (Chelazzi, et al., 2008; Lamar, et al., 2011) and viral hepatitis infections (Weissenborn, et al., 2005; Blei, 2008; Cheung, et al., 2012), and autoimmune
disorders, such as rheumatoid arthritis (RA) (Cojocaru, et al., 2011; Chin and Latov, 2004) and systemic lupus erythematosus (SLE) (Cojocaru, et al., 2011; Chin and Latov, 2004; Borchers, et al., 2005). The pathogenic influence of chronic
inflammation on destabilizing neuronal membrane potentials of the brain is an
established mechanism in the development of epilepsy (Vezzani, et al., 2011; Riazi, et al., 2008). However, previous studies have not completely determined the extent to which diseases delineating chronic inflammation participate in the pathogenesis of epilepsy through the possible mechanism of inflammation-related membrane instability and the spontaneous discharge of brain neurons, apart from conventional epilepsy risk factors.
Chronic osteomyelitis (COM), a disease with powerful chronic inflammation induced by bone infection, can continue for a period of weeks, months, or even years, with persisting pathological characteristics that exhibit strong inflammatory activity in the foci because of the formation of abscesses, bone debris, and sinus tracts
research linking COM, an established chronic inflammatory disease, to the
development of epilepsy.In this national study, we used a large number of enrollees in the National Health Insurance (NHI) claims database, available in Taiwan, to explore the link between COM and epilepsy in a cohort of more than 22 million enrollees for a period of 11 years starting on January 1, 2000 and ending on December 31, 2010.
Methods Data source
This nationwide retrospective cohort study used the beneficiary files of an inpatient claims database obtained for the period of 2000-2010 from the NHI program in Taiwan, which began in 1995. The inpatient claims database employed in this research was extracted from the NHI Research Database (NHIRD) (Wang, et al., 2013). NHI covers more than 98% of the total population of Taiwan. The
identification numbers of the patients in the NHI program are randomized prior to NHIRD assembling. But, we still obtained approval of the institutional review board (or ethics committee) in China Medical University Hospital. International
Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes
Study patients
Based on the NHI database, enrollees who were newly diagnosed with COM (ICD-9-CM code 730.1) between January 1, 2000 and December 31, 2010, but had no previous medical history of epilepsy (ICD-9-CM codes 345), were collected. The dates of their diagnosis were defined as the entry dates. A total of 20,996 patients with COM comprised the study group. The control group was composed of a random selection of age- and gender-matched patients without COM and epilepsy, with corresponding entry dates, and was 4 times the size of the study group (n = 83,973).
Outcome and relevant variables
The end point of this study was epilepsy diagnosis (ICD-9-CM codes 345) during the study period (2000-2010). The relevant variables for epilepsy were age, gender, and comorbidities such as diabetes (ICD-9-CM codes 250), hypertension (ICD-9-CM codes 401-405), head injury (ICD-9-CM codes 310.2, 800, 801, 803, 804, 850, 851, 853, and 854), stroke (ICD-9-CM codes 430-438) and cancer (ICD-9-CM codes 140-208).
Statistical analysis
continuous variables between the COM cohort and the control group. Person-years (person-y) were calculated from the entry dates to the first dates of epilepsy onset, withdrawal from the insurance program, or the end of 2010. The gender- and age-specific incidence rates (per 1000 person-y) of epilepsy were compared between the study and control groups. In the Cox proportional hazards regression model, hazard ratios (HRs) were derived to compare the risk of epilepsy development between groups. The demographic factors and correlating comorbidities were identified for comparison between groups. HRs for epilepsy, with stratification by age, gender, and each of the 5 relevant comorbidities, were compared individually between groups. Using a COM severity index, the correlation between the severity of COM and epilepsy was analyzed. This severity index was defined as the division of total length of hospital stay due to COM during the up period by the length of the follow-up (Tseng, et al., 2014). Using the tertile method, the COM severity was further divided into mild (the first tertile in the COM severity), moderate (the second tertile in the COM severity), and severe (the third tertile in the COM severity). The epilepsy-free rates were plotted in a Kaplan-Meier model and the difference between groups was analyzed using a log-rank test (Figure 1). A 2-tailed P value < .05 was considered significant. SAS Version 9.1 (SAS Institute Inc., Carey, NC, USA) was used in the investigation.
Results
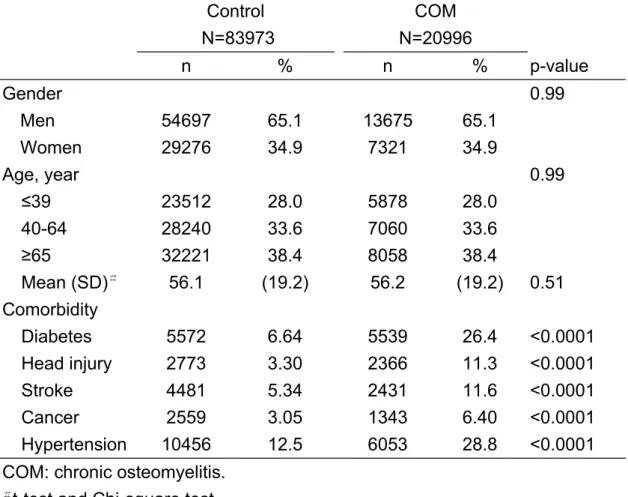
Male patients were more susceptible to COM than female patients were (65.1% vs 34.9%) (Table 1). In comparison with the control group, the familiar comorbidities that are considered risk factors for epilepsy, such as hypertension, diabetes, head injury, stroke, and cancer, were clearly higher in the COM group (P < .0001) (Table 1). With adjustment for age, gender, hypertension, diabetes, head injury, stroke, and cancer, using Cox proportional hazards regression, the overall epilepsy risk was 2.63-fold (95% confidence interval [CI]: 2.20-3.14) in the COM group; significantly higher than the control cohort (Table 2). Age-specific epilepsy risk was highest in the
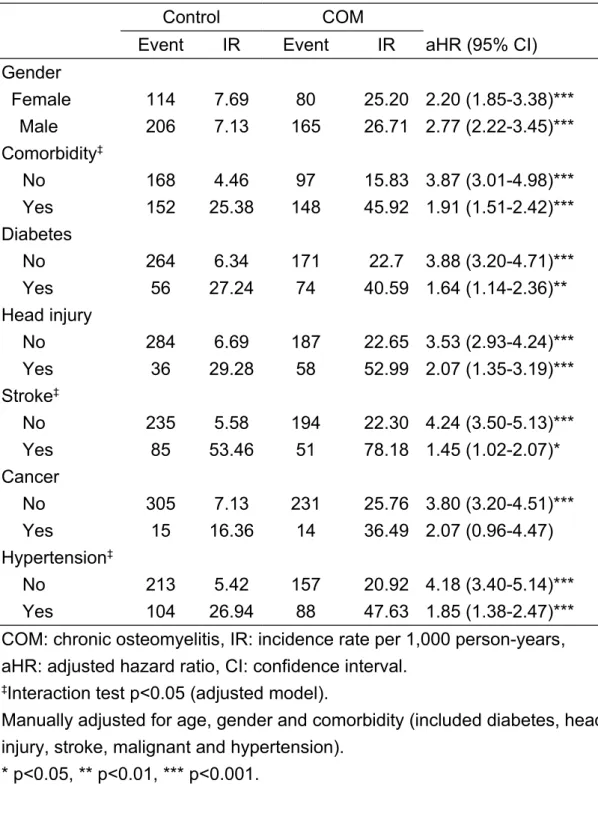
youngest age group (≤ 39 y: 6.10, 95% CI: 4.00-9.30), with a constant decrease with increasing age (≥ 65 y: 1.66, 95% CI: 1.28-2.16) (Table 3). The epilepsy risk in COM group without comorbidities is 3.87 times (95% CI: 3.01-4.98) higher than controls without comorbidities (Table 4). The Kaplan-Meier assessment of the 2 groups revealed that the risk of epilepsy increased during the follow-up period for both groups, with the epilepsy-free rate in the control group being significantly higher than that of the COM group (log-rank P < .0001) (Fig. 1).
Based on the Cox proportional hazards regression model, with adjustment for age, gender, and relevant comorbidities, the stratification analyses of gender, and
comorbidities are displayed in Table 2. Comorbidities that are known to augment epilepsy risk might affect COM as a risk factor of epilepsy. In patients with diabetes, head injury, stroke, cancer, or hypertension, patients with COM still exhibited a significantly higher risk of epilepsy (aHRs: diabetes, 1.64 [95% CI: 1.14-2.36]; head injury, 2.07 [95% CI: 1.35-3.19]; stroke, 1.45 [95% CI: 1.02-2.07]; cancer, 2.07 [95% CI: 0.96-4.47]; hypertension, 1.85 [95% CI: 1.38-2.47]) (Table 4), in agreement with previous studies (Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013; Avila and Graber, 2010; Villanueva, et al., 2008). In comparison with the control group, a severity-dependent risk for epilepsy was observed with the stratifications of COM severity (mild: aHR = 1.40, 95% CI: 1.09-1.80; moderate: aHR = 3.45, 95% CI: 2.67-4.45; severe: aHR = 13.2, 95% CI: 10.1-17.3) (Table 5). Using the same severity-stratification method, similar severity-dependent risks have been seen as well in some other reports, including studies about stroke risk among COM patients (Tseng, et al., 2014), risk of coronary artery disease in COM population (Hsiao, et al., 2014 ) and stroke risk in patients with multiple sclerosis (unpublished data).
Discussion
In addition to the traditional risk factors for epilepsy, previous studies have disclosed that several diseases characterized by infectious processes, for example, sepsis
(Chelazzi, et al., 2008; Lamar, et al., 2011) and viral hepatitis infections
(Weissenborn, et al., 2005; Blei, 2008; Cheung, et al., 2012), and by inflammatory courses, such as RA (Cojocaru, et al., 2011; Chin and Latov, 2004) and SLE
(Cojocaru, et al., 2011; Chin and Latov, 2004; Borchers, et al., 2005), might increase the risk of epilepsy. By using the large patient population in the Taiwan NHI claims dataset, we investigated whether COM, a condition with persistent long-term and high-intensity inflammation, increases epilepsy risk in patients with or without relevant comorbidities of epilepsy.
Similarly to published reports (Smith, et al., 2006; Zuluaga, et al., 2006), the COM group was characterized by male predominance with the majority of COM patients being aged 40 years or older (Table 1). This might be because males and younger people were more susceptible to accidents and traumas. These findings demonstrate the applicability of the COM patient population from the Taiwan NHI database. The diagnosis of COM was correlated with a higher risk of epilepsy (aHR = 2.63, 95% CI: 2.20-3.14) (Table 2). Although male gender was predominant in the COM group, COM increased the epilepsy risk for both genders (Table 3).
Age is an important risk factor for epilepsy (De Boer, et al., 2008; Pugliatti, et al., 2007; Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013; Avila and Graber, 2010; Ottman, et al., 1996; Mac, et al., 2007). The absolute risk of epilepsy
increased constantly with age (Table 2). However, the relative weight of COM in augmenting risk of epilepsy was higher in the younger age group, with the highest aHR of 6.10 observed in the ≤ 39-year age group, which decreased steadily to the lowest aHR (1.66) observed in the ≥ 65-year age group (Table 3). Because the
comorbidities known to increase the risk of epilepsy were less common in the younger population, COM stood out as a more prominent risk factor than in the older patient groups in whom such comorbidities played more substantial roles as age progressed (Table 3). The risk of epilepsy increased steadily with the increase of COM severity, from the lowest risk in the mildest subgroup (aHR = 1.40, 95% CI: 1.09-1.80) to the highest risk in the most severe subgroup (aHR = 13.2, 95% CI: 10.1-17.3) (Table 5). These findings strengthen the causal role of COM in the generation of epilepsy.
Comorbidities of epilepsy
Many risk factors for epilepsy have been identified (De Boer, et al., 2008; Pugliatti, et al., 2007; Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013; Avila and Graber, 2010; Villanueva, et al., 2008; Ottman, et al., 1996; Mac, et al., 2007). Among these, age (De Boer, et al., 2008; Pugliatti, et al., 2007; Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013; Avila and Graber, 2010; Ottman, et al., 1996; Mac, et al., 2007), male gender (Pugliatti, et al., 2007; Ottman, et al., 2011; Ngugi, et
al., 2013; Mac, eta al., 2007), hypertension (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013), diabetes (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013), head injury (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013), stroke (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013), and cancer (Avila and Graber, 2010; Villaneva, et al., 2008) have been observed to be of varying weights. The prevalence of these comorbidities was all much higher in COM group than controls (Table 1). Since in different COM patients, some of the comorbidities began before and some after COM, in this study, we were not sure these comorbidities caused COM, vice versa, or COM and these comorbidities shared a common etiology. The risk of epilepsy increased to various levels in both the COM and control cohorts with superimposed comorbidities (Table 4). These results confirmed the validity of the NHI database for exploring supplementary risk factors of epilepsy, such as COM. COM patients without comorbidities that are known to increase epilepsy risk
exhibited higher risk of epilepsy (aHR = 3.87, 95% CI: 3.01-4.98) than the control group without the same comorbidities did (Table 4). These findings imply that COM is an independent causal factor of epilepsy, affecting younger patients in particular (Tables 2-4).
This population-based cohort study had numerous strengths. First, patients with COM and age- and gender-matched controls were selected from a large dataset of over 22 million enrollees, in a national insurance program comprising more than 98% of the entire population of Taiwan. Insurance claims for reimbursement for in-hospital management undergo rigorous NHI supervision to prevent health care fraud. The NHI monitoring system increases the reliability of diagnoses. Since the NHI system captures 98% of the population in Taiwan, this study is almost a total population study. Therefore, with a cases-to-controls ratio of 1:4, it should have higher precision, validity, reliability and generalization in this study. The demographic profiles
revealing a male predominance and age distribution profile are similar to previous studies (De Boer, et al., 2008; Pugliatti, et al., 2007; Ottman, et al., 2011; Cloyd, et al., 2006; Ngugi, et al., 2013; Avila and Graber, 2010; Ottman, et al., 1996; Mac, et al., 2007). The well-organized display of risk factors of epilepsy, including
hypertension (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013;
LaRoche, et al., 2003; Phabphal, et al, 2013), diabetes (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013; Phabphal, et al, 2013), head injury (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013; LaRoche, et al., 2003), stoke (Ottman, et al., 2011; Cloyd, eta al., 2006; Ngugi, et al., 2013; LaRoche, et al., 2003), and cancer (Avila and Graber, 2010; Villanueva, et al., 2008; Kargiotis, et al., 2011), in
combination with increased incidence rates of epilepsy in both COM and the control groups, supports the reliability of the data used in this study. Second, the large sample size allowed for categorization into subgroups for further statistical analyses, enabling us to confirm the effect of COM on the risk of epilepsy, particularly in younger people for whom the cause of epilepsy might be less clear.
The length of the follow-up, showing time and severity-dependent effects on the epilepsy risk, intensify the role of COM as a risk factor for epilepsy. Finally, the increased incidence of comorbidities that are known to be risk factors for epilepsy, among patients with COM, increases the possibility that the underlying chronic inflammation might also affect patients with COM, leading to a higher risk of developing the pertinent comorbidities of epilepsy.
However, there are still numerous limitations. First, we were unable to exclude the possibility that other vascular risk factors, such as medications prescribed for COM, reduced physical activity and altered immunity, might also increase the risk of epilepsy. Thus, the risks determined in the study might present factors mixed with COM. Second, personal habits that might affect health, including smoking and alcohol consumption, were not obtainable in the Taiwanese NHI dataset. Their effect on the increased risk of epilepsy in the COM group could not be analyzed. However, COM increased the risk of epilepsy for both genders (Table 3), and the considerably
low smoking rate (< 4.5%) among women in Taiwan (Bureau of Health Promotion, Taiwan, 2012) suggests that although smoking is unlikely to be a dominant variable for a noticeable increase in epilepsy risk in patients with COM, but it could still be one of the factors. The higher risk for epilepsy in younger COM patients (Table 3), who potentially have less cumulative smoking and alcohol exposures than their elders, also reduces the likelihood of cigarette smoking and alcohol consumption as factors in epilepsy development in the COM population. Third, this study intended to display an increase in the risk of epilepsy in patients with COM. We noticed a higher prevalence of comorbidities among patients with COM in comparison with those without (Table 1). Results disclosed that even among those without risk factors for epilepsy, COM still imposed higher risk for the development of epilepsy. However, it remains to be established whether there is a causal relationship between COM and epilepsy. Further research is required to resolve this matter.
Conclusion
Results obtained from this study demonstrated, for the first time, that COM is a risk factor of epilepsy. Patients with COM were observed to have higher prevalence rates of comorbidities that are known risk factors of epilepsy. The relative value of COM as a predictor of epilepsy was more significant in the younger patient groups. The
rigorous provision of prevention assessments for epilepsy in patients with COM, such as treatment with adequate antibiotics, effective abscess drainage and wound
debridement of the infected bones, hyperbaric oxygen therapy and, if needed, limb amputation as early as possible (Lankarani-Fard, et al., 2009), is prudent, particularly for those of a younger age. Since COM was more common seen in males and younger people who were more susceptible to accidents and trauma, vigorous casualty
prevention in these two populations might be helpful in epilepsy prevention as well.
Conflict of interest
None.
Acknowledgments
The authors thank the National Health Research Institute in Taiwan for making available the insurance claims data for analyses. We also thank Professors Chung Y. Hsu, Fung-Chang Sung, and Chi-Pang Wen for their critical comments. This study was partially supported by the Department of Health, Executive Yuan, Taiwan (Grant DOH 97-HP-1101, 2008), China Medical University Hospital (Grant 1MS1 ), Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence
(Grant DOH101-TD-B-111-004), and Academia Sinica, Biosignature
(BM102021169). The funders had no role in study design, data collection and
analysis, decision to publish, or preparation of the manuscript. No additional external funding received for this study.
References
Avila, E.K., Graber, J., 2010. Seizures and epilepsy in cancer patients. Curr Neurol Neurosci Rep. 10, 60-67.
Blei, A.T., 2008. Brain edema in acute liver failure. Crit Care Clin. 24, 99-114. Borchers, A.T., Aoki, C.A., Naguwa, S.M., Keen, C.L., Shoenfeld, Y., Gershwin,
M.E., 2005. Neuropsychiatric features of systemic lupus erythematosus. Autoimmun Rev. 4, 329-344.
Bureau of Health Promotion, Taiwan., 2012. Taiwan tobacco control annual report 2012. Taipei: Department of Health, Taiwan.
Chelazzi, C., Consales, G., de Gaudio, A.R., 2008. Sepsis associated encephalopathy. Curr Anaesth Crit Care. 19, 15-21.
Cheung, M.C., Maguire, J., Carey, I., Wendon, J., Agarwal, K., 2012. Review of the neurological manifestations of hepatitis E infection. Ann Hepatol. 11, 618-622. Chin, R.L., Latov, N., 2004. Central nervous system manifestations of rheumatologic
diseases. Curr Opin Rheumatol. 17, 91-99.
Cloyd, J., Hauser, W., Towne, A., Ramsay, R., Mattson, R., Gilliam, F., Walczak, T., 2006. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res. 68S, S39-S48.
Cojocaru, I.M., Cojocaru, M., Silosi, I., Vrabie, C.D., 2011. Central nervous system manifestations in rheumatic diseases. J Med Biochem. 330, 1-4.
De Boer, H.M., Mula, M., Sander, J.W., 2008. The global burden and stigma of epilepsy. Epilepsy Behav. 12, 540-546
Engelborghs, S., D’Hooge, R., De Deyn, P.P., 2000. Pathophysiology of epilepsy. Acta Neurol Belg. 100, 201-213.
Hsiao, L.-C., Muo, C.-H., Chen, Y.-C., Chou, C.-Y., Tseng, C.-H., Chang, K.-C., 2014. Increased risk of coronary heart disease in patients with chronic osteomyelitis: a population-based study in a cohort of 23 million. Heart. (accepted).
Kargiotis, O., Markoula, S., Kyritsis, A.P., 2011. Epilepsy in the cancer patient. Cancer Chemother Pharmacol. 67, 489-501.
Lamar, C.D., Hurley, R.A.,Taber, K.H., 2011. Sepsis-associated encephalopathy: review of the neuropsychiatric manifestations and cognitive outcome. J Neuropsychiatry Clin Neurosci. 23, 236-241.
Lankarani-Fard, A., Liu, P.Y., Fang, M.A., 2009. Osteomyelitis and septic arthritis. In: Yoshikawa TT and Norman DC, eds. Infectious Disease in the Aging: A Clinical Handbook. New York: Humana Press. pp 201-217.
LaRoche, S.M., Helmers, S.L., 2003. Epilepsy in the elderly. Neurologist. 9, 241-249. Mac, T.L., Tran, D.S., Quet, F., Odermatt, P., Preux, P.M., Tan, C.T., 2007.
Epidemiology, aetiology, and clinical management of epilepsy in Asia: a systematic review. Lancet Neurol. 6, 533-543.
Ngugi, A.K., Bottomley, C., Kleinschmidt, I., Wagner, R.G., Kakooza-Mwesige, A., Ae-Ngibise, K., Owusu-Agyei, S., Masanja, H., Kamuyu, G., Odhiambo, R., Chengo, E., Sander, J.W., Newton, C.R., for the SEEDS Group., 2013.
Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol. 12, 253-263. Ottman, R., Annegers, J.F., Risch, N., Hauser, W.A., Susser, M., 1996. Relations of
genetic and environmental factors in the etiology of epilepsy. Ann Neurol. 39, 442-449.
Ottman, R., Lipton, R.B., Ettinger, A.B., Cramer, J.A., Reed, M.L., Morrison, A., Wan, G.J., 2011. Comorbidities of epilepsy: results from the Epilepsy Comorbidities and Health (EPIC) survey. Epilepsia. 52, 308-315.
Phabphal, K., Geater, A., Limapichat, K., Sathirapanya, P., Setthawatcharawanich, S., 2013. Risk factors of recurrent seizure, co-morbidities, and mortality in new onset seizure in elderly. Seizure 22, 577-580.
Pugliatti, M., Beghi, E., Forsgren, L., Ekman, M., Sobocki, P., 2007. Estimating the cost of epilepsy in Europe: a review with economic modeling.Epilepsia. 48, 2224-2233.
Riazi, K., Galic, M.A., Kuzmiski, J.B., Ho, W., Sharkey, K.A., Pittman, Q.J., 2008. Microglial activation and TNFα production mediate altered CNS excitability following peripheral inflammation. Proc Natl Acad Sci USA. 105, 17151-17156.
Smith, I.M., Austin, O.M.B., Batchelor, A.G., 2006. The treatment of chronic osteomyelitis: a 10-year audit. J Plast Reconstr Aesthet Surg. 59, 11-15. Tseng, C.-H., Chen, J.-H., Muo, C.-H., Chang, Y.-J., Sung, F.-C., Hsu, C.Y., 2014.
Increased risk of ischaemic stroke amongst patients with chronic osteomyelitis: a population-based cohort study in Taiwan. Eur J Neurol. (accepted).
Vezzani, A., French, J., Bartfai, T., Baram, T.Z., 2011. The role of inflammation in epilepsy. Nat Rev Neurol. 7, 31-40.
Villanueva, V., Codina, M., Elices, E., 2008. Management of epilepsy in oncological patients. Neurologist. 14, S44-S54.
Wang, I.-K., Muo, C.-H., Chang, Y.-C., Liang, C.-C., Chang, C.-T. Lin, S.-Y., Yen, T.-H., Chuang, F.-R., Chen, P.-C., Huang, C.-C., Wen, C.-P., Sung, F.-C., Morisky DE., 2013. Association between hypertensive disorders during pregnancy and end-stage renal disease: a population-based study. Can Med Assoc J. 185, 207-213.
Weissenborn, K., Bokemeyer, M., Krause, J., Ennen, J., Ahl, B., 2005. Neurological and neuropsychiatric syndromes associated with liver disease.AIDS. 19(suppl 3), S93-S98.
Zuluaga, A.F., Galvis, W., Saldarriaga, J.G., Agudelo, M., Salazar, B.E., Vesga, O., 2006. Etiologic diagnosis of chronic osteomyelitis: a prospective study. Arch Intern Med. 166, 95-100.
Figure Legends:
Figure 1 The comparison of epilepsy-free rates between the chronic osteomyelitis group and the control cohort, using a Kaplan-Meier model.
Table 1 Demographic factors and comorbidities in chronic osteomyelitis and control groups. Control N=83973 COM N=20996 n % n % p-value Gender 0.99 Men 54697 65.1 13675 65.1 Women 29276 34.9 7321 34.9 Age, year 0.99 ≤39 23512 28.0 5878 28.0 40-64 28240 33.6 7060 33.6 ≥65 32221 38.4 8058 38.4 Mean (SD)# 56.1 (19.2) 56.2 (19.2) 0.51 Comorbidity Diabetes 5572 6.64 5539 26.4 <0.0001 Head injury 2773 3.30 2366 11.3 <0.0001 Stroke 4481 5.34 2431 11.6 <0.0001 Cancer 2559 3.05 1343 6.40 <0.0001 Hypertension 10456 12.5 6053 28.8 <0.0001
COM: chronic osteomyelitis. #t-test and Chi-square test.
Table 2 Multivariable Cox proportional regression analysis of
epilepsy predictors.
Event IR aHR (95% CI)
COM No 320 7.32 1.00 Yes 245 26.20 2.63 (2.20-3.14)*** Age, year ≤39 116 6.61 1.00 40-64 155 8.44 1.15 (0.90-1.47) ≥65 294 17.16 1.83 (1.43-2.33)*** Gender Women 194 10.78 1.00 Men 371 10.58 1.14 (0.96-1.36) Comorbidity Diabetes No 435 8.85 1.00 Yes 130 33.52 0.88 (0.22-3.55) Head injury No 471 9.29 1.00 Yes 94 40.45 2.75 (2.19-3.46)*** Stroke No 429 8.44 1.00 Yes 136 60.65 3.36 (2.67-4.24)*** Cancer No 536 10.36 1.00 Yes 29 22.30 1.53 (1.05-2.22)* HTN No 373 7.88 1.00 Yes 192 33.63 1.74 (1.40-2.16)***
COM: chronic osteomyelitis, IR: Incidence rate per 1,000 person-years, aHR: adjusted hazard ratio, CI: confidence interval, HTN: hypertension.
Adjusted for chronic osteomyelitis, age, gender and comorbidity. * p<0.05, ** p<0.01, *** p<0.001.
Table 3 Multivariable Cox proportional regression analysis of epilepsy predictors, stratified
by age.
≤39 years old 40-64 years old ≥65 years old aHR (95% CI) aHR (95% CI) aHR (95% CI) COM (yes vs. no) 6.10 (4.00-9.30)*** 2.79 (1.97-3.97)*** 1.66 (1.28-2.16)*** Gender (men vs. women) 1.23 (0.76-1.99) 1.49 (1.04-2.12)* 1.03 (0.81-1.29) Comorbidity (yes vs. no)
Diabetes 1.23 (0.54-2.79) 1.78 (1.19-2.66)** 1.31 (0.98-1.76) Head injury 3.33 (2.18-5.10)*** 2.81 (1.82-4.33)*** 2.05 (1.42-2.96)***
Stroke 3.86 (1.61-9.25)** 3.45 (2.20-5.41)*** 3.37 (2.54-4.47)*** Cancer 3.35 (1.23-9.19)* 2.45 (1.38-4.53)** 1.00 (0.57-1.75) HTN 1.53 (0.66-3.57) 2.26 (1.49-3.43)*** 1.44 (1.09-1.90)** COM: chronic osteomyelitis, IR: Incidence rate per 1,000 person-years, aHR: adjusted hazard ratio, CI: confidence interval, HTN: hypertension.
Interaction test p<0.001 between chronic osteomyelitis and age group (crude and adjusted model).
Adjusted for chronic osteomyelitis, gender and comorbidity. * p<0.05, ** p<0.01, *** p<0.001.
Table 4 Adjusted hazard ratio for epilepsy between chronic osteomyelitis
and control groups, stratified by epilepsy-associated factors.
Control COM
Event IR Event IR aHR (95% CI)
Gender Female 114 7.69 80 25.20 2.20 (1.85-3.38)*** Male 206 7.13 165 26.71 2.77 (2.22-3.45)*** Comorbidity‡ No 168 4.46 97 15.83 3.87 (3.01-4.98)*** Yes 152 25.38 148 45.92 1.91 (1.51-2.42)*** Diabetes No 264 6.34 171 22.7 3.88 (3.20-4.71)*** Yes 56 27.24 74 40.59 1.64 (1.14-2.36)** Head injury No 284 6.69 187 22.65 3.53 (2.93-4.24)*** Yes 36 29.28 58 52.99 2.07 (1.35-3.19)*** Stroke‡ No 235 5.58 194 22.30 4.24 (3.50-5.13)*** Yes 85 53.46 51 78.18 1.45 (1.02-2.07)* Cancer No 305 7.13 231 25.76 3.80 (3.20-4.51)*** Yes 15 16.36 14 36.49 2.07 (0.96-4.47) Hypertension‡ No 213 5.42 157 20.92 4.18 (3.40-5.14)*** Yes 104 26.94 88 47.63 1.85 (1.38-2.47)***
COM: chronic osteomyelitis, IR: incidence rate per 1,000 person-years, aHR: adjusted hazard ratio, CI: confidence interval.
‡Interaction test p<0.05 (adjusted model).
Manually adjusted for age, gender and comorbidity (included diabetes, head injury, stroke, malignant and hypertension).
Table 5 Incidence rate and hazard ratio for epilepsy, stratified by severity
of chronic osteomyelitis.
COM severity Event IR aHR (95% CI)
Compared group 320 7.32 1.00
Mild (T1) 80 12.27 1.40 (1.09-1.80)**
Moderate (T2) 82 35.52 3.45 (2.67-4.45)***
Severe (T3) 83 157.97 13.2 (10.1-17.3)***
p for trend <0.0001
COM: chronic osteomyelitis, IR: incidence rate per 1,000 person-years, aHR: adjusted hazard ratio, CI: confidence interval, T1: first tertile, T2: second tertile, T3: third tertile.
COM severity = (total length of hospital stay due to chronic osteomyelitis during the follow-up duration) ÷ (length of follow-up duration).
Adjusted for age, gender, diabetes, head injury, stroke, cancer and hypertension.