1 Article Type:A Case Report
1
Clinical Features of Keratouveitis Associated with Cytomegalovirus Infection 2
巨細胞病毒導致角膜葡萄膜炎之臨床表現 3
Peng-Tai Tien, M.D.1, Yi-Yu Tsai, PhD.1, Tsai-Hsiu Lin, M.D.2, Chun-Chi Chiang, 4
MD.1 5
田彭太1,蔡宜佑1,林彩秀2,江鈞綺1
6
1. Department of Ophthalmology, China Medical University Hospital 7
中國醫藥大學附設醫院眼科部 8
2. Department of Laboratory Medicine, China Medical University Hospital 9
中國醫藥大學附設醫院檢驗醫學部 10
Running Title:Cytomegalovirus Keratouveitis 11
簡題:巨細胞病毒角膜葡萄膜炎 12
Reprint Requests:Chun-Chi Chiang, Department of Ophthalmology, China Medical 13
University Hospital, No 2, Yuh–Der Road, Taichung 404, Taiwan 14
聯絡地址:404,台中市育德路 2 號,中國醫藥大學附設醫院眼科部,江鈞綺 15
E-mail address: [email protected] 16 TEL:886–4–22052121 (ext. 1141) 17 FAX:886–4–22052121 (ext. 1139) 18 19
2
Abstract
1
Purpose: To report a case of keratouveitis associated with cytomegalovirus infection 2
Method: Interventional case report 3
Result: We examined a 44-year-old male who had been suffering from recurrent 4
elevated intraocular pressure (IOP) in the left eye for 2 years. The ocular manifestations 5
included stromal and epithelial microcystic corneal edema, keratic precipitates, and 6
elevated IOP. The lesion did not subside after treatment with oral valaciclovir for a 7
week. The cytomegalovirus (CMV) genome was detected in the aqueous humor by 8
means of the polymerase chain reaction (PCR). The IOP was controlled by performing a 9
trabeculectomy. Treatment with intravenous ganciclovir (450 mg, Q12H * 1 week) 10
followed by oral valganciclovir (900 mg BID) for 2 months returned the cornea to 11
complete clarity without keratic precipitates. The IOP also returned to the normal range. 12
However, we detected a low endothelial cell density of the affected cornea by specular 13
microscopy. 14
Conclusion: The clinical presentation of CMV keratouveitis may resemble that of 15
Posner-Schlossman syndrome or Fuchs heterochromic iridocyclitis. If CMV 16
keratouveitis is suspected, then early PCR analysis of the aqueous humor could lower 17
the rate of delayed diagnosis. Compared with intravenous ganciclovir, oral 18
3
valganciclovir not only shortens the hospitalization period but also offers greater 1 convenience to patients. 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
4 摘要 1 目的:報告與巨細胞病毒感染有關之角膜葡萄膜炎一例 2 方法:病例報告 3 結果:一位 44 歲男性左眼眼壓上升反覆發作已兩年,眼部表現包含角膜基質/上 4 皮小泡性水腫、角膜沉降物及眼壓上升。病灶在口服 valaciclovir 一個月後並無消 5 退,經房水聚合酶鏈鎖反應偵測到巨細胞病毒基因組。施行小樑切除術以控制眼 6 壓,在接受靜脈注射 ganciclovir(450 mg,每 12 小時一次共 1 周)並接續口服 7 valganciclovir (900 mg,一天兩次)兩個月後,角膜完全透明且原有角膜沉降物消 8 失,眼壓亦回到正常範圍;然而角膜細胞數目測定儀卻偵測到受影響角膜之低內 9 皮細胞密度。 10 結論:巨細胞病毒角膜葡萄膜炎之臨床表現可能與 Posner-Schlossman syndrome 11
及 Fuchs heterochromic iridocyclitis 類似,當高度懷疑角膜葡萄膜炎時,即早施行 12 單純疱疹病毒及巨細胞病毒房水聚合酶鏈鎖反應檢驗將有助於降低延遲診斷之機 13 率。相較於靜脈注射 ganciclovir,口服 valganciclovir 不單單可縮短住院天數,亦 14 帶給患者較大的便利性。 15 Key words 16
Cytomegalovirus, Keratouveitis, Polymerase chain reaction, Valganciclovir 17
巨細胞病毒,角膜葡萄膜炎,聚合酶鏈鎖反應,克毒癒 18
5
Cytomegalovirus (CMV) infection is very common in humans, and most of the 1
infected patients have no symptoms. Although ocular manifestations (retinitis) are found 2
in immunocompromised patients, involvement of the anterior segment is comparatively 3
mild and less common.1 However, it has been found that ocular CMV infection is 4
associated with corneal endotheliitis and hypertensive anterior uveitis in 5
immunocompetent humans.2, 3 6
We report a rare case of CMV keratouveitis with sector corneal edema, keratic 7
precipitates, iris depigmentation, and elevated intraocular pressure (IOP), which 8
mimicked Posner-Schlossman syndrome (PSS) and Fuchs heterochromic iridocyclitis 9
(FHI) in a relatively healthy man. 10
6
CASE REPORT
1
A 44-year-old Chinese man was referred to our out-patient department (OPD) 2
because he had been suffering from gradually blurring vision in the left eye for the past 3
2 years. An examination revealed that recurrent episodes of elevated IOP occurred 4
during this period. The interval between each occurrence of elevated IOP was 5
approximately 1 month, and each episode initially subsided following topical 6
medication (including steroids). As the symptoms progressed, the intervals shortened 7
and the patient’s response to medical treatment became poorer. 8
At presentation, we noted corneal edema (superior-nasal quadrant). The best-9
corrected visual acuity of the right and left eyes was 20/20 and 20/200, respectively. The 10
IOP was 16 mmHg in the right eye and 74 mmHg in the left. After emergent anti-11
glaucomatic medical management, the IOP in the left eye decreased to 23 mmHg. The 12
initial diagnosis was Posner-Schlossman syndrome (PSS). 13
The patient returned to our OPD the next day; an examination of the cornea at the 14
time revealed microcystic and stromal edema extending to the upper half (Figure 1-A) 15
with keratic precipitates (KPs; Figure 1-B/C). We also observed cells (++) in the 16
anterior chamber. The iris was depigmented compared to the fellow eye, mimicking the 17
presentation of Fuchs heterochromic iridocyclitis (FHI; Figure 1-D). The lens 18
7
demonstrated moderate posterior subcapsular opacity. There was no vitritis or retinitis. 1
The IOP was 18 mmHg in the left eye. 2
We suspected herpes simplex virus (HSV) infection or varicella zoster virus (VZV) 3
infection related to hypertensive anterior uveitis because of the presence of sector 4
corneal edema and KP’s; therefore, we initially prescribed valaciclovir (1 gm twice a 5
day). However, after 1 week of oral valaciclovir treatment, the lesion progressed and 6
extended toward the lower part of the cornea with coin-shaped KPs (Figure 2). Hence, 7
CMV infection was highly suspected, and the aqueous humor tap was performed to 8
investigate this possibility. 9
CMV DNA was extracted with a QIAGEN® Blood DNA mini kit (QIAGEN Inc, CA, 10
USA). Purified viral DNA was resuspended in 60 μl buffer AE. The PCR mixture 11
contained virus DNA, 10x PCR reaction buffer, 3.6 mM MgCl2, 0.2 mM (each) 12
deoxynucleoside triphosphates, 20 pmol of each primer. Then 1 U of Taq DNA 13
polymerase was added after denaturing the DNA at 94°C for 5 min. DNA amplification 14
was performed with 40 cycles, each cycle consisting of denaturation for 2 min at 94°C, 15
primer annealing for 2 min at 63°C, extension for 3 min at 72°C, and a final extension 16
step at 72ºC for 10 min. The PCR products were analyzed by electrophoresis in 2% 17
agarose gels stained with ethidium bromide. The PCR analysis revealed the presence of 18
8 the cytomegalovirus genome. (Figure 3) 1
After the diagnosis of CMV keratouveitis in the left eye, the patient was admitted for 2
intravenous ganciclovir therapy (450 mg Q12H). The corneal edema and KP’s did not 3
resolve after 2 days of hospitalization (Figure 4). The IOP in the left eye remained 4
recalcitrant (37~39 mmHg) despite maximal topical therapy with Cosopt® (dorzolamide 5
and timolol), Alphagan® (brimonidine), and oral Diamox® (acetazolamide). Therefore, a 6
trabeculectomy was performed on the third day of hospitalization. The bleb persisted 7
and the IOP in the left eye returned to the normal range on the following day. 8
Concurrent blood serology provided negative results for CMV immunoglobulin M, 9
human immunodeficiency virus (HIV) antibodies, and CMV antigen (pp65), but 10
positive results for CMV immunoglobulin G antibody. After 7 days of intravenous 11
ganciclovir therapy, the patient was discharged with oral valganciclovir (900 mg BID) 12
and topical Pred Forte® (prednisolone acetate, QID). 13
After oral valganciclovir therapy for a month, corneal edema was found to be 14
confined only to the superior-nasal corner as a crescent lesion (Figure 5-A). The IOP 15
was 17 mmHg in the right eye and 12 mmHg in the left eye. Although iris 16
depigmentation persisted, KPs were no longer observed (Figure 5-B). Specular 17
microscopy showed low endothelial cell density (408/mm2) in the left eye (Figure 5-C). 18
9
The cornea was completely clear after oral valganciclovir therapy for 7 weeks. The IOP 1
in the left eye was 18 mmHg. 2
We ceased all medication after the second month of therapy. Serologic examination 3
revealed normal renal and liver functions. There was no regression of the corneal lesion 4
after valganciclovir treatment had been stopped for 2 months (Figure 6-A). The patient 5
underwent a repeated aqueous humor tap, and PCR analysis revealed negative CMV 6
results (Figure 6-B). 7
10
DISCUSSION
1
Although the pathogenesis of CMV keratouveitis remains poorly understood, 2
Koizumi et al. presumed that anterior chamber-associated immune deviation (ACAID) 3
prevents the control of viral proliferation by cell-mediated immunity while CMV is 4
reactivated in the anterior chamber. Thus, CMV infection may develop in the corneal 5
endothelium.4 6
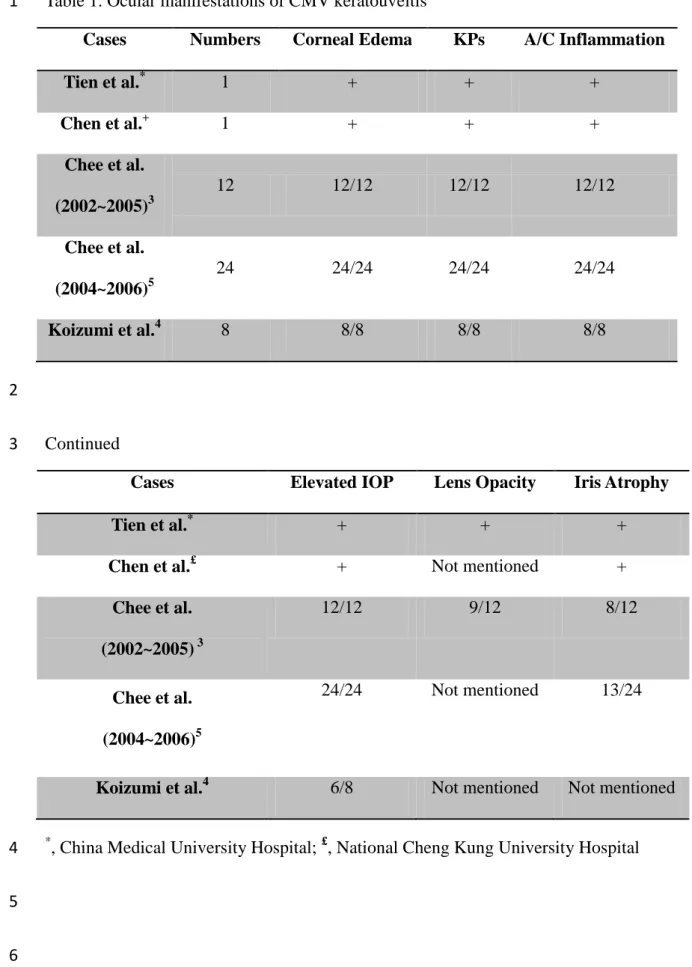
Different ocular manifestations in CMV keratouveitis cases have been observed in 7
other institutions (Table 1). In April 2009, a patient at the National Cheng Kung 8
University Hospital presented with corneal edema and elevated IOP, which was 9
refractory to valaciclovir treatment. A case series from the Singapore National Eye 10
Centre provided the following observations: (1) corneal edema may be focal to diffuse 11
bullous keratopathy, with some cases showing a distinct horizontal curvilinear 12
demarcation on the endothelium; (2) KPs varied in appearance from a linear pattern to a 13
circular (coin-shaped) pattern; (3) mild anterior chamber inflammation; (4) iris atrophy; 14
(5) lens opacity in some cases; and (6) elevated IOP.3, 5, 6 Koizumi et al. also reported 15
that (1) stromal edema of the cornea was found in all CMV infected eyes; (2) linear KPs 16
and coin-shaped lesions were commonly observed in CMV-induced corneal 17
endotheliitis. They also described variously as KPs having a circular pattern or ring 18
11
configuration; (3) anterior chamber inflammation; (4) elevated IOP. 4 1
The 2 common features of the reported CMV keratouveitis cases were elevated IOP 2
and iris atrophy, and they are consistent with the findings of CMV infection in the 3
smooth muscle cells of the iris, ciliary body, and the endothelial cells of Schlemm’s 4
canal.1 However, CMV keratouveitis could easily be misdiagnosed as other conditions 5
with hypertensive anterior uveitis such as PSS and FHI. PSS is characterized by 6
recurrent episodes of mild inflammation with elevated IOP, fine KP’s, and corneal 7
epithelial edema, with the IOP returning to normal between successive episodes. FHI is 8
characterized by iris heterochromia, posterior subcapsular opacity cataract, and satellite 9
KP’s. Chee et al. demonstrated that CMV infection can cause a spectrum of ocular 10
manifestations resembling PSS, FHI, or even corneal endotheliitis.5 A comparison of 11
the CMV-positive PSS and FHI patients in Chee et al.’s case series revealed that the 12
PSS patients were younger, had higher IOP, and were less likely to have iris atrophy or 13
cataracts. Nodular endothelial lesions were more commonly observed in CMV-positive 14
FHI eyes than in CMV-positive PSS eyes, and they probably represent CMV-infected 15
endothelial cells. Reticulate cornea deposits were highly predictive of CMV retinitis as 16
they were observed in all of the potential FHI eyes but not in the potential PSS eyes. 17
Chee and Jap hypothesized that these manifestations are dependent on the ocular 18
12
immune response and/or viral load. Eyes resembling PSS are probably the result of the 1
inflammatory response to CMV infection as they respond to topical steroids alone and 2
may even be self-limiting. On the other hand, eyes resembling FHI may have a larger 3
viral load and/or poorer immune response than eyes resembling PSS, given their poor 4
response to steroids.6 5
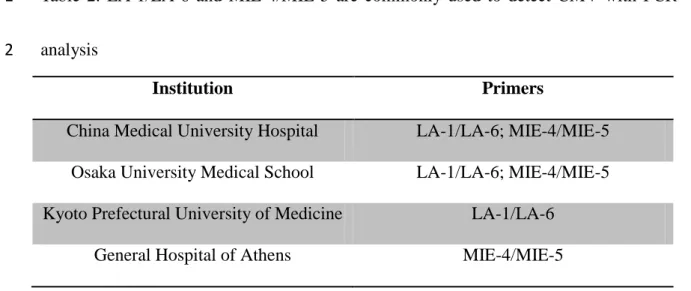
We used 2 pairs of primers for our CMV PCR analysis. One pair amplifies a 400-base-6
pair sequence that codes for a portion of the late antigen (LA) of CMV (AD169 strain) 7
which is composed of LA-1 (5′-CAC CTG TCA CCG CTG CTA TAT TTGC-3′) and 8
LA-6 (5′-CAC CAC GCA GCG GCC CTT GAT GTTT-3′). The other pair amplifies a 9
435-base-pair sequence that codes for a portion of the major immediate-early (MIE) 10
antigen of CMV (Twone strain), which is composed of MIE-4 (5′-CCA AGC GGC CTC 11
TGA TAA CCA AGC C-3′) and MIE-5 (5′-CAG CAC CAT CCT CCT CTT CCT CTG 12
G-3′). The analysis provided a sensitivity of 93% with a specificity of 100%.7 Although 13
these primers for CMV PCR analysis are also used in other institutions4,8,9 (Table 2), 14
other primer sets are also used: 5′-TTA GTG AAC CGT CAG ATC GC and 3′-GCA 15
TGC ATA AGA AGC CAA GG are used in the Ehime University School of Medicine4, 16
while 5′-CAC TTC GGG GTC GCA AT and 5′-CGG GTA TCA ACA ACA GCA 17
AGGA are used in the Tan Tock Seng Hospital10. 18
13
Blood serology provided positive results for the CMV immunoglobulin G antibody 1
and negative for the CMV antigen and immunoglobulin M antibody. These facts 2
revealed that the patient had a prior systemic CMV infection, but the current CMV 3
infection was limited to the eye alone and it was not a spillover from a systemic 4
infection. CMV infection can also be determined by quantifying the levels of intraocular 5
and serum immunoglobulin G antibodies. The ratio of the quantities of intraocular 6
immunoglobulin G antibody to serum immunoglobulin G antibody is called the 7
Goldmann–Witmer coefficient (C). C > 1 indicates the intraocular production of 8
antibodies, while C > 3 is considered significant. This analysis has a sensitivity of 9
47.3% and a specificity of 98.0%.11 10
In order to diagnose CMV keratouveitis, it is necessary to perform PCR analysis or 11
the intraocular antibody assay (Goldmann-Witmer coefficient). In our laboratory, at 12
least 100 μl of aqueous sample was needed for each pathogenic PCR. At least 200 μl of 13
aqueous sample was needed for the intraocular antibody assay. As the amount of tapped 14
aqueous humor was limited and the intraocular antibody assay is not more sensitive than 15
PCR2, we preferred to conduct only the PCR analysis. 16
Although several infective pathogens (such as HSV, VZV, or Toxoplasma spp.) may 17
result in hypertensive uveitis, which has symptoms similar to those of CMV 18
14
keratouveitis, only PCR analyses for CMV and HSV are available in our laboratory. As 1
the patient received refractory valaciclovir therapy for 1 week, we only performed PCR 2
analysis for CMV. However, PCR analyses for both CMV and HSV were performed for 3
suspected keratouveitis cases currently and at least 200 μl of aqueous sample was 4
needed. In recent years, tetraplex PCR analysis was developed by the Singapore General 5
Hospital. It simultaneously detects HSV, VZV, CMV, and T. gondii. Only 100 μl of 6
aqueous sample is needed for this analysis, which has a sensitivity and specificity of 7
more than 95%.3, 5 8
CMV corneal endotheliitis can initially present as hypertensive anterior uveitis and 9
thereafter lead to sustained corneal damage that only responds to treatment with 10
steroids.3 Repeated use of steroids may lead to favorable conditions for viral replication, 11
which leads to increasingly frequent attacks and glaucomatous damage.6 PCR analysis 12
of aqueous humor plays an important role in detecting specific viral infections. We 13
suggest that aqueous humor PCR analysis for HSV/CMV be performed immediately 14
when viral keratouveitis is highly suspected, So that the rate of delayed diagnosis can be 15
decreased. 16
The traditional treatment of CMV infection is intravenous ganciclovir (5 mg/kg
17
Q12H) for 3 weeks and requires the patient to be admitted to a hospital. However, this 18
15
treatment is very inconvenient for the patient. We prescribed oral valganciclovir after 1
the patient was discharged. Valganciclovir is the prodrug of ganciclovir and is available 2
in oral form. The advantage of valganciclovir is not only the reduced period of 3
hospitalization but also a good therapeutic effect. 4
Our patient received intravenous ganciclovir (450 mg twice daily for a week), 5
followed by oral valganciclovir (900 mg twice daily for another 8 weeks). Until now, 6
the patient has had regular follow-ups for 9 months since the cessation of valganciclovir 7
therapy and there have been no recurrent episodes in the absence of antiviral or anti-8
glaucomatic therapy during this period. The subjects from the case series of Chee et al. 9
received oral valganciclovir (900 mg twice daily for 6 weeks, followed by 450 mg twice 10
daily for another 6 weeks) or intravenous ganciclovir (5 mg/kg body weight twice daily 11
for 6 weeks), followed by oral ganciclovir (1 g three times daily for another 6 weeks). 12
However, 77.7% of the subjects had a recurrence within 8 months of stopping the 13
treatment and required further courses of ganciclovir, although it was not specifically 14
mentioned if these subjects belonged to the ganciclovir group or the valganciclovir 15
group, or both. Hence, CMV keratouveitis may require a longer period of treatment.5 16
In conclusion, we identified a case with CMV keratouveitis whose ocular 17
manifestations resembled PSS, FHI, and corneal endotheliitis. It is important to perform 18
16
aqueous humor PCR analysis in order to ensure correct diagnosis of CMV keratouveitis. 1
In addition to intravenous ganciclovir treatment, oral valganciclovir is a new option for 2
treating CMV keratouveitis.3, 5 3
17
REFERENCES
1
1. Daicker B. Cytomegalovirus panuveitis with infection of corneo-trabecular
2
endothelium in AIDS. Ophthalmologica 1988;197:169-75. 3
2. Van Boxtel LA, van der Lelij A, van der Meer J, Los LI. Cytomegalovirus as a 4
cause of anterior uveitis in immunocompetent patients. Ophthalmology 5
2007;114:1358-62. 6
3. Chee SP, Bascal K, Jap A, Se-Thoe SY, Cheng CL, Tan BH. Corneal 7
endotheliitis associated with evidence of cytomegalovirus infection. 8
Ophthalmology 2007;114:798-803. 9
4. Koizumi N, Suzuki T, Uno T, Chihara H, Shiraishi A, Hara Y, et al. 10
Cytomegalovirus as an etiologic factor in corneal endotheliitis. 11
Ophthalmology 2008;115:292-97. 12
5. Chee SP, Bascal K, Jap A, Se-Thoe SY, Cheng CL, Tan BH. Clinical features 13
of cytomegalovirus anterior uveitis in immunocompetent patients. Am J 14
Ophthalmol 2008;145:834-40. 15
6. Chee SP, Jap A. Presumed Fuchs heterochromic iridocyclitis and Posner-16
Schlossman syndrome: Comparison of cytomegalovirus-positive and negative 17
eyes. Am J Ophthalmol 2008;146:883-89. 18
18
7. Demmler GJ, Buffone GJ, Schimbor CM, May RA. Detection of 1
cytomegalovirus in urine from newborns by using polymerase chain reaction 2
DNA amplification. J Infect Dis. 1988;158:1177-84. 3
8. Itoh N, Hanafusa T, Yamagata K, Nakajima H, Tomita K, Tamura S, et al. No 4
detectable cytomegalovirus and Epstein-Barr virus genomes in the pancreas of 5
recent-onset IDDM patients. Diabetologia 1995;38:667-71. 6
9. Markomichelakis NN, Canakis C, Zafirakis P, Marakis T, Mallias I, 7
Theodossiadis G. Cytomegalovirus as a cause of anterior uveitis with sectoral 8
iris atrophy. Ophthalmology 2002;109:879-82. 9
10. Teoh SC-B, Thean L, Koay E. Cytomegalovirus in aetiology of Posner– 10
Schlossman syndrome: evidence from quantitative polymerase chain reaction. 11
Eye 2005;19,1338-40. 12
11. Luyendijk L, Boer JH, Rothova A, Baarsma GS, Jong PTVM, Horn GJ, et al. 13
Sensitivity and specificity of anti-viral antibody determination in the aqueous 14
or vitreous of uveitis patients. Uveitis 1993;265-7. 15
16
17
19
FIGURE LEGENDS
1
FIGURE 1. Patient with keratouveitis. Slit-lamp photograph showing (A) microcystic 2
and stromal edema extending to the upper half of the left cornea. The iris was 3
depigmented. (B/C) Fine keratic precipitates. (D) The right iris was fully pigmented. 4
FIGURE 2. One month after oral acyclovir treatment. (A) The original edema extended 5
towards the lower part of the cornea. (B) A slit lamp revealed coin-shaped keratitic 6
precipitates, stromal edema, and iris depigmentation. 7
FIGURE 3. Electrophoresis of aqueous humor PCR products. CMV pp65 and CMV 8
pp71 were confirmed in the sample (Lane 4/7) 9
FIGURE 4. Two days after intravenous ganciclovir treatment. (A) The original edema 10
did not subside. (B) Iris depigmentation. (C, D) Coin-shaped keratitic precipitates, 11
stromal edema, and epithelial microcystic edema. 12
FIGURE 5. One month after oral valganciclovir treatment. (A) The original edema was 13
confined to the superior-nasal corner as a crescent lesion. (B) There was an absence of 14
keratic precipitates. (C) Low endothelial cell density (408/mm2) in the left eye. 15
FIGURE 6. After ceasing valganciclovir treatment for 2 months. (A) There was no 16
regression of the corneal lesion. (B) Aqueous humor PCR revealed no presence of CMV 17
pp65 or CMV pp71. 18
20
Table 1. Ocular manifestations of CMV keratouveitis 1
Cases Numbers Corneal Edema KPs A/C Inflammation
Tien et al.* 1 + + + Chen et al.+ 1 + + + Chee et al. (2002~2005)3 12 12/12 12/12 12/12 Chee et al. (2004~2006)5 24 24/24 24/24 24/24 Koizumi et al.4 8 8/8 8/8 8/8 2 Continued 3
Cases Elevated IOP Lens Opacity Iris Atrophy
Tien et al.* + + +
Chen et al.£ + Not mentioned +
Chee et al. (2002~2005) 3 12/12 9/12 8/12 Chee et al. (2004~2006)5 24/24 Not mentioned 13/24
Koizumi et al.4 6/8 Not mentioned Not mentioned
*
, China Medical University Hospital; £, National Cheng Kung University Hospital 4
5
21
Table 2. LA-1/LA-6 and MIE-4/MIE-5 are commonly used to detect CMV with PCR 1
analysis 2
Institution Primers
China Medical University Hospital LA-1/LA-6; MIE-4/MIE-5 Osaka University Medical School LA-1/LA-6; MIE-4/MIE-5 Kyoto Prefectural University of Medicine LA-1/LA-6
General Hospital of Athens MIE-4/MIE-5