Mastery and Stigma in Predicting the Subjective Quality of Life of
Patients With Schizophrenia in Taiwan
Ping-Chuan Hsiung, PhD,* Ay-Woan Pan, PhD,†‡ Shi-Kai Liu, MD,§¶
储** Shing-Chia Chen, PhD,††
Szu-Yi Peng, MS,‡ and Lyinn Chung, PhD‡‡
Abstract: A total of 199 outpatients with schizophrenia are assessed in this study for their sense of mastery, stigma, social support, symptom severity, and quality of life (QOL), with path models being used to test the direct and indirect effects of these factors on the physical, psychological, social, and environmental QOL domains. Symptoms, stigma, mastery, and social sup-port are found to be key direct predictors for all 4 QOL domains, with mastery having the greatest direct effect on QOL, whereas stigma has the greatest indirect effect, although mediated by mastery and social support. Such results imply that in nonwestern cultures, mastery and stigma are still crucial factors affecting the QOL of patients with schizophrenia. Our results highlight the importance of enhancing the mastery of such patients and reducing the associated stigma when designing treatment programs. To enhance the QOL of patients with schizophrenia, interventions which can optimize the meaningful use of time may well enhance the mastery of these patients, whereas strategies aimed at improving their ability to cope with perceived stigma, at both individual and community levels, may help to reduce the detrimental effects.
Key Words: Mastery, stigma, quality of life, schizophrenia, path analysis. (J Nerv Ment Dis 2010;198: 494 –500)
N
umerous studies have reported that patients with schizophrenia have poorer quality of life (QOL) than both healthy subjects (Awadalla et al., 2005; Law et al., 2005; Picardi et al., 2006; Akvardar et al., 2006; Ulas et al., 2008) and people with other chronic diseases (Akvardar et al., 2006). QOL has therefore emerged as an important outcome measure for patients with schizophrenia in both naturalistic prospective and intervention studies (Dogan et al., 2004; Sim et al., 2006; Gorna et al., 2008).The results presented in a number of the prior studies indicate that the QOL of patients with schizophrenia may be influenced by a wide variety of demographic and clinical factors, including age (Law et al., 2005), marital and employment status (Makanjuola et al., 2007), and the severity of the patients’ clinical symptoms, including the depressive,
and positive and negative symptoms of schizophrenia (Law et al., 2005; Wegener et al., 2005; Gorna et al., 2008).
Various psychosocial factors have also been shown to have both direct and indirect impacts on the QOL of patients with schizophrenia, including their overall level of satisfaction with social contacts (Bengtsson-Tops and Hansson, 2001) and their sense of self, which essentially refers to their sense of coherence, self esteem, mastery, and locus of control (Eklund et al., 2003; Bejer-holm et al., 2007). Among the diverse range of subjective psycho-social factors, not only does higher perceived stigma lead to lower satisfaction with life (Rosenfield, 1997; Markowitz, 1998), but it is also a reliable predictor of the discontinuation of treatment (Sirey et al., 2001) and the diminution of self-efficacy, empowerment, and self-esteem (Rosenfield, 1997; Link et al., 2001; Vauth et al., 2007). Furthermore, it is also clearly demonstrated within the extant literature that perceived stigma has a strong correlation with the severity of depressive-anxiety symptoms among the mentally ill (Markowitz, 1998; Lysaker et al., 2007). It is probably the case that among all mental illnesses, schizophrenia represents the most neg-ative image to society as a whole; thus, in any attempt at exploring the QOL of patients with schizophrenia, the issue of perceived stigma may be of particular theoretical and practical importance.
All of the recent studies in which attempts are made to disentangle the complex interrelationships between the QOL in the mentally ill and the contributory factors (such as demographic, clinical, and psychosocial factors) have been carried out in western societies (Zissi et al., 1998; Eklund et al., 2003; Eklund and Backstrom, 2005; Vauth et al., 2007). However, given that the key concepts examined, such as stigma, self-esteem, and mastery, are each considered to be highly culturally sensitive, there is a clear need to empirically examine, within specific cultural contexts, whether the causal relationships that have been identified between clinical symptoms, mastery, stigma, social support, and the QOL of patients with schizophrenia within western societies are also appli-cable to Asian cultures. Furthermore, it may well be that the relative contributions of these factors could be found to differ markedly across different cultures.
Nevertheless, despite cultural differences having been shown to have significant influences on the manifestation, range, and magnitude of the impact of perceived stigma (Yang et al., 2007), such reports on Asian societies appear to be something of a rarity. The very few qualitative studies which have been undertaken in Taiwan demonstrate that the mentally ill tend to internalize and suffer from the shame ascribed to them by the public for having contracted such mental illnesses. These studies find that the patients tend to struggle considerably with the stigma associated with mental illness in general, particularly with regard to schizophrenia (Lin et al., 2002; Ma et al., 2005).
Understandably, such a disadvantaged status in society makes it extremely difficult for patients with schizophrenia to exercise any personal control over their own condition, thereby hindering the establishment of their concept of self, including self-esteem, sense of mastery, and self-efficacy (Pearlin and Schooler, 1978; Wright et al., 2000; Vauth et al., 2007). The present study therefore proposes
*Department of Social Work, National Taiwan University, Taipei, Taiwan; †School of Occupational Therapy, National Taiwan University, Taipei, wan; ‡Department of Psychiatry, National Taiwan University Hospital, Tai-pei, Taiwan; §Department of Psychiatry, University of Toronto, Ontario, Canada; ¶Center for Addiction and Mental Health, University of Toronto, Ontario, Canada;㛳Department of Psychiatry, National Taiwan University, Taipei, Taiwan; **Department of Psychiatry, Far Eastern Memorial Hos-pital, Taipei, Taiwan; ††School of Nursing, National Taiwan University, Taipei, Taiwan; and ‡‡Department of Statistics, National Taipei Univer-sity, Taipei County, Taiwan.
Supported by the National Science Council (NSC93–2314-B-002–294, NSC94 – 2314-B-002–223, NSC97–2918-I-002– 004, and NSC97–2628-S-002– 001-MY3), National Taiwan University (NTU98R0506) and the National Health Research Institutes (EX95–9511PP, EX96 –9511PP, and NHRI-EX97–9511PP) within the Executive Yuan of Taiwan.
Send reprint requests to Lyinn Chung, PhD, Department of Statistics, National Taipei University, Sanhsia Township, Taipei County 237, Taiwan. E-mail: [email protected].
Copyright © 2010 by Lippincott Williams & Wilkins ISSN: 0022-3018/10/19807-0494
a hypothetical path model (Pedhazur, 1982), undertaken among a Taiwanese sample of patients with schizophrenia, in an attempt to determine the causal relationships and relative importance of the related variables in a sociocultural context (The particular merits of path analysis are its ability to interpret the linear relationships that exist between a set of variables, and to decompose the correlations into direct and indirect effects (Pedhazur, 1982). Our path analysis results reveal the specific effects of the predictive variables on QOL and the relative importance of each predictor in the causal model. These effects are represented by standardized path coefficients).
Our primary aim is to attempt to provide a causal explanation for the complex relationships between QOL and 6 predictive vari-ables, comprising of age, gender, schizophrenia symptoms, mastery, perceived stigma, and social support. The empirically validated causal model is expected to guide interventions that may ultimately lead to improvements in the QOL of patients with schizophrenia.
As suggested within many of the prior studies, we also expect to find that being younger and being male will each have strong correlations with a higher level of mastery and QOL (Schieman and Turner, 1998; Pearlin et al., 2007), and that a higher level of mastery and social support will also be associated with a higher level of QOL. Furthermore, we predict that a clear correlation will be discernible between higher levels of both symptoms and stigma and lower levels of QOL, whereas we also expect to find that symptoms, stigma, and social support will each have indirect effects on QOL (Fig. 1).
MATERIALS AND METHODS
Subjects
The subjects for the present study were recruited from the psychiatric outpatient clinic at the National Taiwan University Hospital. To qualify for inclusion in this study, the subjects must have been at least 18 years of age at the time the study was carried out, and able to meet the International Classification of Diseases-10 criteria for schizophrenia. The clinical diagnosis of schizophrenia was made by board-certified psychiatrists using International
Clas-sification of Diseases-10 criteria for schizophrenia following a semi-structured 1-hour clinical interview.
Those eligible for inclusion in the study were subsequently referred to a trained psychiatric nurse who independently collected demographic data, rated clinical symptoms, and assessed QOL using standardized questionnaires, as shown later. The clinical diagnosis was then double-checked against the clinical data by another board-certified psychiatrist, with any discrepancies in the diagnoses being clarified and a final diagnosis being reached at a consensus meeting with the referring psychiatrists.
All subjects with other Axis I mental retardation or psychi-atric disorders were excluded from the study sample, as were those who were unable to complete the questionnaire on self-reported measures. Written informed consent was obtained from all partici-pants, and the study protocol was approved by the Institutional Review Board of the National Taiwan University Hospital.
Measures
QOL Scale
QOL was assessed in this study using the 26-item World Health Organization QOL-BREF (WHOQOL-BREF; Yao et al., 2002). The cross-cultural validity of the WHOQOL-BREF has been examined and further confirmed in a cross-study involving 3 Chi-nese subcultures (Skevington et al., 2004; Yao and Wu, 2009), whereas the WHOQOL-BREF has been widely used in prior studies on patients with schizophrenia (Sim et al., 2006; Gorna et al., 2008; Ulas et al., 2008). The instrument used in the present includes 2 general items (G1, covering overall QOL, and G4, covering general health) along with 24 universal items covering the 4 physical, psychological, social, and environmental domains. Responses to the items were scored from 1 (least favorable condition) to 5 (most favorable condition); thus the domain scores, which ranged between 4 and 20, were calculated by taking the average scores for all items in the domain and then multiplying this by 4. A higher score indicates a better QOL on the corresponding domain. The internal consistency reliability levels (Cronbach’s ␣) in this study were found to be 0.77 for the physical domain, 0.83 for the psychological domain, 0.74 for the social domain, and 0.83 for the environmental domain.
Mastery Scale
Mastery, or the extent to which individuals view themselves as being in control of those forces that have substantial effects on their lives, was assessed in this study using a 4-point, 7-item, Likert-type “Mastery” scale (Pearlin and Schooler, 1978; Pearlin et al., 1981). Good internal consistency (Cronbach’s␣ ⫽ 0.87) has been shown by the preliminary results of the Chinese version of the Mastery scale (Chen et al., 2007). The sample items include “I have little control over the things that happen to me” and “there is little I can do to change many of the important things in my life.” Re-sponses to the items were scored from 1 (strongly agree) to 4 (strongly disagree), with a higher score indicating a greater sense of mastery. The internal consistency (Cronbach’s␣) of the items in this study was 0.82.
Social Impact Scale
The personal stigma, as perceived by patients to be associated with their illness, was assessed in the present study using a 4-point, 24-item, Likert-type “Social Impact” scale. This scale has also been shown to have good internal consistency of 0.99 (Pan et al., 2007). The sample items include “I feel others avoid me because of my illness,” “I feel I need to keep my illness a secret,” and “I feel set apart from others who are well.” Responses to the items were scored from 1 (strongly disagree) to 4 (strongly agree), with a higher score indicating a higher perception of stigmatization. The internal
con-FIGURE 1. Initial path model for the 4 quality of life
sistency reliability (Cronbach’s␣) in the present study was found to be 0.93.
Social Support Questionnaire
Social support refers to the level of satisfaction felt by various individuals with regard to the help or support which they perceive as being available to them within their environment. This variable was assessed using the 6-item “Social Support Questionnaire” short form rated by a 6-point Likert type scale (Sarason et al., 1987). The preliminary results of the Chinese version of the Social Support Questionnaire short form (Pan et al., 2008) have again been shown to have good internal consistency (Cronbach’s ␣ ⫽ 0.94). The sample items include “How satisfied are you that you can really count on people to be dependable when you need help?” and “How satisfied are you that you can really count on people to console you when you are very upset?” The responses to the items were scored from 1 (very dissatisfied) to 6 (very satisfied), with a higher score indicating a greater level of satisfaction with the perceived avail-ability of help or support. The internal consistency (Cronbach’s␣) in this study was found to be 0.93.
Symptom Scale for Schizophrenia
The severity of clinical symptoms was assessed in the present study using a 13-item, 4-point Likert-type Symptom Scale for schizophrenia covering both positive (7-item) and negative (6-item) symptoms (Shiau, 1995; Hsu et al., 2005). The responses to these items were scored from 0 (no symptoms) to 3 (severe symptoms), with the symptom rating being based on interviews with the patients and their families carried out by a trained psychiatric nurse. The psychiatric nurse had received prior training to rate the scale and simultaneously rated several patients with the trainer to ensure inter-rater reliability. The internal consistency (Cronbach’s␣) of the scale in the present study was found to be 0.75.
Data Analysis
The statistical analyses carried out in the present study in-cluded descriptive statistics for each determinant within the path model, computation of the correlation coefficients among all of these determinants, and path analysis to validate the hypothetical model. The significance level of the path analysis was set at 0.05 for the overall F statistics, with individual t statistics being obtained both at each step, and for each path.
Each of the QOL domains was explored for its unique path model, with individual examinations being undertaken of the paths in the initial path model (the hypothesized model); any insignificant paths were subsequently deleted, thereby yielding the final model. Similar 2-step approaches were used to identify the models with the best fit for each QOL domain for the sample patients.
The goodness of fit between the data and the models was estimated using root mean square error of approximation (RMSEA), the goodness-of-fit index (GFI), the adjusted goodness-of-fit index (AGFI), the normed fit index (NFI), the comparative fit index (CFI) and p values for the chi square test (Subhash, 1995). The criteria for a good fit were RMSEA⬍0.05, GFI ⬎0.9, AGFI ⬎0.9, NFI ⬎0.9, CFI ⬎0.9, and p ⬎ 0.05. All of the analyses in this study were performed using SPSS (version 11.5) and LISREL 8.3.
This study also presents the decomposition of the direct, indirect, causal, and noncausal components of the final path models. The direct effect provides us with an understanding of the specific effect of one particular independent variable on another, whereas the indirect effect is the effect of one independent variable on another through the remaining (mediating) variables. The total effect, ob-tained by summing the direct and indirect effects of each individual variable, provides us with an understanding of the single unit
change, which occurs in the dependent variable as a result of a single unit change in the independent variable.
RESULTS
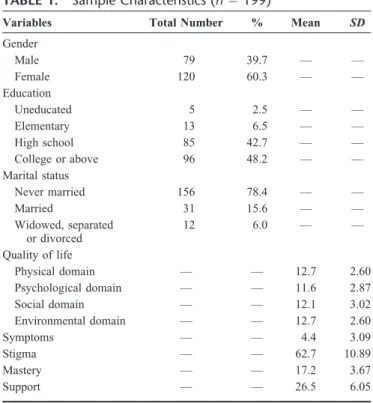
A total of 199 participants were recruited for this study, aged between 19 and 65 years, with a mean age of 36.68 years (standard deviation⫽ 10.34 years); 120 (60.3%) were female, 156 (78.4%) had never been married, and 181 (90.9%) had achieved a high school level of education or above (Table 1). All of the study participants were Taiwanese, with an average of 3.03 hospitaliza-tions per patient (range⫽ 1–7, standard deviation ⫽ 1.71).
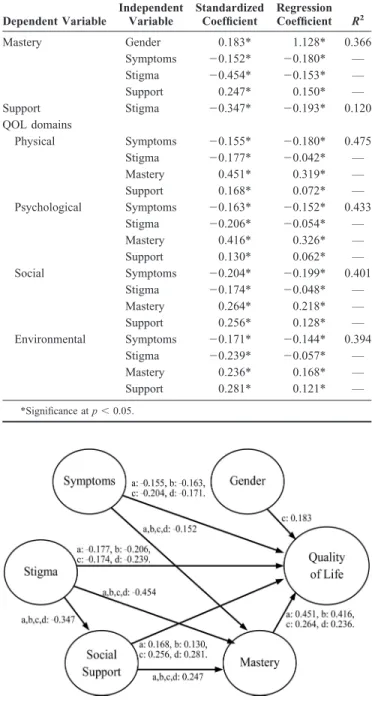
The results of the path analysis for the initial model are presented in Table 2, which reveals that, with the exception of the social domain, age and gender were found to have no association with levels of either mastery or QOL. The results of the final path model are presented in Table 3, whereas Figure 2 illustrates the revised version of the initial path model. The values for the 4 QOL domains in the final path models were RMSEA⬍0.05, GFI ⬎0.9, AGFI⬎0.9, NFI ⬎0.9, CFI ⬎0.9, and p ⬎ 0.05, thereby indicating that the path models fitted the data quite well. As shown in Table 3, the proportion of the variance explained by the predictive variables in the 4 QOL domains ranged between 39.4% and 47.5%.
Symptoms, stigma, mastery, and social support were all found to be key direct predictors in all 4 of the QOL domains, with gender also being found to directly predict the social QOL domain. It is also notable that all 4 QOL domains were indirectly predicted by symp-toms, stigma, and social support (Fig. 2).
Table 4 presents the decomposition of the direct, indirect, causal, and noncausal components of the final path models. Of the 4 QOL domains, mastery was found to have the greatest overall direct effect on QOL, with the one exception of the environmental domain, which was mainly affected by the direct effect of social support.
The results of this study show that patients with schizophrenia who have higher levels of mastery and social support also tend to have higher levels of QOL; conversely, those patients who have
TABLE 1. Sample Characteristics (n⫽ 199)
Variables Total Number % Mean SD
Gender Male 79 39.7 — — Female 120 60.3 — — Education Uneducated 5 2.5 — — Elementary 13 6.5 — — High school 85 42.7 — — College or above 96 48.2 — — Marital status Never married 156 78.4 — — Married 31 15.6 — — Widowed, separated or divorced 12 6.0 — — Quality of life Physical domain — — 12.7 2.60 Psychological domain — — 11.6 2.87 Social domain — — 12.1 3.02 Environmental domain — — 12.7 2.60 Symptoms — — 4.4 3.09 Stigma — — 62.7 10.89 Mastery — — 17.2 3.67 Support — — 26.5 6.05
higher perceived levels of stigmatization and symptoms are found to have lower levels of QOL. The evidence presented in this study therefore provides support for our hypotheses. Stigma is found to have the largest indirect effect on all 4 QOL domains, with mastery and social support having mediating effects. Symptoms and social support are also found to have indirect effects on the QOL domains through mastery.
DISCUSSION
The results of this study concur with our hypothetical model, indicating that mastery and social support have direct positive effects on all QOL domains, whereas symptoms and stigma have negative effects on QOL. Mastery has the greatest direct effect on the QOL of patients with schizophrenia, with stigma being found to have the greatest indirect effect. The high correlations between the 4 QOL domains may account for the similarity in the final path models for all 4 QOL domains. Future studies should therefore attempt to examine whether similar patterns occur in other popula-tions of schizophrenia patients. Mastery has been identified as a personal resource in coping with stress (Pearlin and Schooler, 1978;
Pearlin et al., 1981), with the crucial role of mastery in predicting subjective QOL for individuals with mental illness having also been demonstrated in several of the prior studies (Rosenfield, 1992; Zissi et al., 1998; Eklund et al., 2003).
Although it may be suggested that mastery is very much a concept of Western individualism and autonomy, the present study confirms that mastery is also a key factor in enhancing the QOL for patients with schizophrenia in Taiwan, which thereby suggests that the concept of mastery may well have cross-cultural relevance. This may be related to the fact that patients with schizophrenia are a
TABLE 2. Path Analysis for the Initial Model Dependent Variable Independent Variable Standardized Coefficient Regression Coefficient R2 Mastery Age 0.043 0.015 0.361 Gender 0.014 0.101 — Symptoms ⫺0.153* ⫺0.180* — Stigma ⫺0.453* ⫺0.152* — Support 0.241* 0.145* — Support Symptoms 0.015 0.029 0.121 Stigma ⫺0.347* ⫺0.193* — Stigma Symptoms ⫺0.009 ⫺0.031 0.000 QOL domains Physical Age ⫺0.047 ⫺0.012 0.479 Gender 0.036 0.188 — Symptoms ⫺0.151* ⫺0.127* — Stigma ⫺0.178* ⫺0.043* — Mastery 0.450* 0.321* — Support 0.175* 0.075 — Psychological Age 0.019 0.005 0.434 Gender 0.081 0.472 — Symptoms ⫺0.159* ⫺0.180* — Stigma ⫺0.205* ⫺0.147* — Mastery 0.413* 0.323* — Support 0.128* 0.061* — Social Age ⫺0.025 ⫺0.007 0.400 Gender 0.186* 1.143* — Symptoms ⫺0.203* ⫺0.198* — Stigma ⫺0.175* ⫺0.048* — Mastery 0.265* 0.219* — Support 0.260* 0.130* — Environmental Age ⫺0.006 ⫺0.001 0.392 Gender 0.012 0.064 — Symptoms ⫺0.171* ⫺0.143* — Stigma ⫺0.240* ⫺0.057* — Mastery 0.236* 0.168* — Support 0.283* 0.121* — *Significance at p⬍ 0.05.
TABLE 3. Path Analysis for the Final Model Dependent Variable Independent Variable Standardized Coefficient Regression Coefficient R2 Mastery Gender 0.183* 1.128* 0.366 Symptoms ⫺0.152* ⫺0.180* — Stigma ⫺0.454* ⫺0.153* — Support 0.247* 0.150* — Support Stigma ⫺0.347* ⫺0.193* 0.120 QOL domains Physical Symptoms ⫺0.155* ⫺0.180* 0.475 Stigma ⫺0.177* ⫺0.042* — Mastery 0.451* 0.319* — Support 0.168* 0.072* — Psychological Symptoms ⫺0.163* ⫺0.152* 0.433 Stigma ⫺0.206* ⫺0.054* — Mastery 0.416* 0.326* — Support 0.130* 0.062* — Social Symptoms ⫺0.204* ⫺0.199* 0.401 Stigma ⫺0.174* ⫺0.048* — Mastery 0.264* 0.218* — Support 0.256* 0.128* — Environmental Symptoms ⫺0.171* ⫺0.144* 0.394 Stigma ⫺0.239* ⫺0.057* — Mastery 0.236* 0.168* — Support 0.281* 0.121* — *Significance at p⬍ 0.05.
FIGURE 2. Final path model for the 4 quality of life domains.
aPhysical quality of life domain;bPsychological quality of life domain;cSocial quality of life domain;dEnvironmental quality of life domain.
greatly disadvantaged group within society who constantly experi-ence feelings of a lack of control; achieving a sense of mastery may therefore be particularly crucial for these patients.
Patients with schizophrenia who have a higher sense of mastery may be capable of taking charge of their lives and engaging in those things that are important to them; this will, in turn, affect their overall QOL. Patients with schizophrenia have themselves indicated that they do try to engage in protective and proactive strategies to cultivate the acceptance of relationships and environ-ments during their recovery path (Lin et al., 2003; Ma et al., 2005). For example, they may attempt to educate the people around them to facilitate a better understanding of both their illness and their efforts to adapt to living within the community.
Another important contribution of the present study is the interrelationships that are found to exist between symptoms, stigma, mastery, social support, and QOL. As indicated in one particular prior study, although more severe psychiatric symptoms are gener-ally associated with lower mastery among patients with schizophre-nia, it has also been found that, over time, improved access to social contact has a clear association with an increased mastery score (Bengtsson-Tops, 2004). The results of the present study indicate that psychiatric symptoms and overall satisfaction with the level of social support have indirect effects on the QOL of patients with schizophrenia, as mediated through mastery.
Several of the early studies show that among all persons suffering from mental illness, the effects of stigma on overall satisfaction with life are partly mediated through the effects on the concept of self (Rosenfield, 1997; Markowitz, 1998). More recently, a similar model confirmed that a higher level of stigmatization among patients with schizophrenia reduced their overall level of self-efficacy and empowerment, thereby leading to lower QOL levels (Vauth et al., 2007). The final causal models in the present study demonstrate that there are several distinct routes by which stigma may give rise to detrimental effects on QOL. In addition to
the direct effects, perceived stigma has a negative effect on the QOL of patients by affecting their sense of mastery and satisfaction with social support.
It has been reported in several earlier studies undertaken in Hong Kong, China, and Taiwan that patients with schizophrenia and their families have experienced stigmatizing incidences from the general public, employers, neighbors, and even their own relatives (Lin et al., 2002; Phillips et al., 2002; Lee et al., 2005; Lin et al., 2008). Clearly, such stigmatization can easily undermine the self-esteem of such patients (Rosenfield, 1997; Link et al., 2001), leading to negative social interactions (Schulze, 2007), and an overall negative impact on the QOL of those suffering from mental illnesses (Yanos et al., 2001).
Studies undertaken in Taiwan have demonstrated that the majority of mentally ill patients tend to live with their families (Hsu et al., 2005; Lin et al., 2008; Chung et al., 2009). In the present study we have also found that a high proportion of the participants were living with their families and that a similarly high proportion had never been married. This indicates that their immediate family members are entrusted with the responsibility for supporting them. Within the sociocultural context of Chinese communities, given that strong emphasis is placed on family ties and social networks, this clearly makes living with a highly stigmatized disease, such as schizophrenia, extremely difficult not only for such patients, but also for their family members.
Although the experience of schizophrenia tends to create tension between the patients and their families (Struening et al., 2001; Ma et al., 2005), ultimately leading to negative social inter-actions (Ma et al., 2005; Lin et al., 2008), patients with schizophre-nia in Taiwan seem to adopt strategies aimed at concealing their illness and retreating from social contacts to cope with the stigma (Link et al., 1989; Perlick et al., 2001; Lee et al., 2005; Vauth et al., 2007). In the present study, we contribute additional cross-cultural evidence to show that the QOL of patients with schizophrenia is reduced, either directly or indirectly, through their perceived level of stigmatization that hampers their general sense of mastery and satisfaction with the overall level of social support.
The present study further implies that interventions aimed at successfully reducing the level of stigmatization, as perceived by the patients, along with a strengthening of their sense of mastery, may have important contributions to make to the overall QOL of patients with schizophrenia. It has been suggested that more meaningful and satisfying use of time has a positive correlation with mastery (Eklund et al., 2007; Bejerholm et al., 2007), and that any partici-pation in psychiatric services which effectively promotes a sense of mastery could have significant benefits on the overall QOL of patients with schizophrenia (Rosenfield, 1992, 1997). All of these studies suggest that patients with schizophrenia could benefit from treatment programs and occupational engagement in which greater emphasis is placed on the enhancement of mastery.
Effort should also be placed into developing strategies capa-ble of counteracting the negative effects of stigma. Treatment programs aimed at improving the social skills of individuals, along with their ability to cope with the perceived stigma, have been suggested as a means of reducing both stigma and its adverse effects. In addition to interventions at a personal level, professional effort in Taiwan should also try to place much greater emphasis on commu-nity programs aimed at engaging patients with schizophrenia, as well as their families, in the task of developing comprehensive community-based treatment programs.
There are several limitations of the present study which must be taken into consideration. First of all, the study was cross-sectional in nature; thus, any future studies should attempt to validate the model using longitudinal data. Second, the study
TABLE 4. Decomposition of the Final Path Model for the 4 QOL Domains
QOL Domain Bivariate
Relationships Direct Indirect Noncausal Total Physical (Symptoms, QOL) ⫺0.156 ⫺0.068 0.009 ⫺0.215 Stigma ⫺0.177 ⫺0.302 0.002 ⫺0.477 Mastery 0.451 — 0.186 0.637 Support 0.168 0.111 0.129 0.408 Psychological Symptoms ⫺0.163 ⫺0.063 0.007 ⫺0.219 Stigma ⫺0.206 ⫺0.269 0.001 ⫺0.474 Mastery 0.416 — 0.187 0.603 Support 0.130 0.103 0.133 0.366 Social Symptoms ⫺0.204 ⫺0.040 ⫺0.005 ⫺0.249 Gender 0.183 — 0.034 0.217 Stigma ⫺0.174 ⫺0.231 ⫺0.003 ⫺0.408 Mastery 0.264 — 0.234 0.498 Support 0.256 0.065 0.100 0.421 Environmental Symptoms ⫺0.171 ⫺0.036 0.009 ⫺0.198 Stigma ⫺0.239 ⫺0.225 0.001 ⫺0.463 Mastery 0.236 — 0.267 0.503 Support 0.282 0.058 0.116 0.456
sample comprised mainly of females recruited from the outpa-tient clinic of a university hospital, with the majority of these women having higher levels of education and also never having been married. The inclusion of predominantly female patients could well have blurred the cultural context where male Chinese patients tend to receive higher stigma in the workplace, demon-strate a general failure to hold on to gainful employment, and have a tendency to work in low-paid jobs. Thus, any attempt to generalize these results to other populations of patients with schizophrenia should be undertaken with considerable caution.
Third, the variations in the range of symptoms were limited by the low symptom severity of the sample, making it difficult to draw any conclusions with regard to the effects of symptom severity on QOL. Fourthly, the clinical diagnoses carried out in this study were based on semi-structured interviews with 1 psychiatrist, which could well result in diagnostic uncertainty. Finally, other potential factors, such as social competence and the level of social emotional support received from friends and family—factors that are not explored in this study—may also affect the QOL of patients with schizophrenia.
Nevertheless, the significance of this study is its clear delin-eation of the interrelationships existing between schizophrenia symptoms, perceived stigma, social support, mastery, and the QOL of patients with schizophrenia. The crucial roles of mastery and stigma, in terms of their effect on the QOL of the patients, also highlight those components that are of importance in the effective design of intervention programs aimed at enhancing the QOL of patients with schizophrenia.
A longitudinal design should be adopted in future studies to explore the ways in which such stigma is perceived among patients with schizophrenia and the actual circumstances of their stigmati-zation in relation to their QOL over the course of the disease. Further study effort should also be placed into exploring the ways in which the fear and shame experienced by the family—through their asso-ciation with schizophrenia as well as the burden of providing care—limits their capacity to provide the necessary support to such patients, consequently affecting the QOL of both parties. Future studies could attempt to evaluate the effectiveness of multifaceted programs in terms of their promotion of mastery and stigma reduc-tion, and the resultant enhancement of the overall QOL for patients with schizophrenia.
CONCLUSIONS
This study provides cross-cultural evidence on the crucial roles of mastery and stigma in terms of their effects on the QOL of patients with schizophrenia. Our results clearly indicate that enhanc-ing mastery and reducenhanc-ing the associated stigma are of paramount importance in the design of interventions aimed at enhancing the QOL of patients with schizophrenia. Treatment programs optimizing the meaningful use of time could enhance mastery, whereas strate-gies aimed at improving the patients’ ability to cope with perceived stigma at both individual and community levels should help to reduce the adverse effects.
ACKNOWLEDGMENTS
The authors thank Factor-Inwentash Faculty of Social Work at the University of Toronto who hosted the visiting scholarship of the first named author during which this paper was compiled.
REFERENCES
Akvardar Y, Akdede BB, Ozerdem A, Eser E, Topkaya S, Alptekin K (2006) Assessment of quality of life with the WHOQOL-BREF in a group of Turkish psychiatric patients compared with diabetic and healthy subjects. Psychiatry
Clin Neurosci. 60:693– 699.
Awadalla AW, Ohaeri JU, Salih AA, Tawfiq AM (2005) Subjective quality of life
of community living Sudanese psychiatric patients: Comparison with family caregivers’ impressions and control group. Qual Life Res. 14:1855–1867. Bejerholm U, Eklund M, Bejerholm U, Eklund M (2007) Occupational
engage-ment in persons with schizophrenia: Relationships to self-related variables, psychopathology and quality of life. Am J Occup Ther. 61:21–32.
Bengtsson-Tops A (2004) Mastery in patients with schizophrenia living in the community: Relationship to sociodemographic and clinical characteristics, needs for care and support and social network. J Psychiatr Ment Health Nurs. 11:298 –304.
Bengtsson-Tops A, Hansson L (2001) Quantitative and qualitative aspects of the social network in schizophrenic patients living in the community. Relationship to sociodemographic characteristics and clinical factors and subjective quality of life. Int J Soc Psychiatry. 47:67–77.
Chen YL, Hsiung PC, Pan AW (2007) The study of the construct validity of the personal control scale with Rasch measurement model. Paper presented at: The Pacific Rim Objective Measurement Symposium; June 16 –19, Tao-Yuan, Taiwan.
Chung L, Pan AW, Hsiung PC (2009) Quality of life for patients with major depression in Taiwan: A model-based study of predictive factors. Psychiatry
Res. 168:153–162.
Dogan S, Dogan O, Tel H, Coker F, Polatoz O, Dogan FB (2004) Psychosocial approaches in outpatients with schizophrenia. Psychiatr Rehab J. 27:279 –282. Eklund M, Backstrom M (2005) A model of subjective quality of life for outpatients with schizophrenia and other psychoses. Qual Life Res. 14:1157– 1168.
Eklund M, Backstrom M, Hansson L (2003) Personality and self-variables: Important determinants of subjective quality of life in schizophrenia out-patients. Acta Psychiatr Scand. 108:134 –143.
Eklund M, Leufstadius C (2007) Relationships between occupational factors and health and well-being in individuals with persistent mental illness living in the community. Can J Occup Ther. 74:303–313.
Gorna K, Jaracz K, Rybakowski F, Rybakowski J (2008) Determinants of objective and subjective quality of life in first-time-admission schizophrenic patients in Poland: A longitudinal study. Qual Life Res. 17:237–247. Hsu CC, Yao G, Hwu HG, Hsiung PC (2005) The Taiwanese version of the
Lancashire Quality of Life Profile (T-LQOLP): Reliability and validity.
Tai-wanese J Psychiatry. 19:33– 46.
Law CW, Chen EY, Cheung EF, Chan RC, Wong JG, Lam CL, Leung KF, Lo MS (2005) Impact of untreated psychosis on quality of life in patients with first-episode schizophrenia. Qual Life Res. 14:1803–1811.
Lee S, Lee MT, Chiu MY, Kleinman A (2005) Experience of social stigma by people with schizophrenia in Hong Kong. Br J Psychiatry. 186:153–157. Lin CL, Kopelowicz A, Chan CH, Hsiung PC (2008) A qualitative inquiry into the
Taiwanese mentally ill persons’ difficulties living in the community. Arch
Psychiatr Nurs. 22:266 –276.
Lin ML, Hsiung PC, Lin SJ, Hwu HG (2002) The stigma experience of patients with schizophrenia. Tzu Chi Med J. 14:381–388.
Lin ML, Hsiung PC, Lin SJ, Hwu HG (2003) The coping strategies of schizo-phrenic patients in stigmatic experiences. Formosa J Ment Health. 15:49 – 69. Link BG, Cullen FT, Struenting E, Shrout PE, Dohrenwend BP (1989) A modified labeling theory approach to mental disorder: An empirical assessment. Am
Sociol Rev. 54:400 – 423.
Link BG, Struening EL, Neese-Todd S, Asmussen S, Phelan JC (2001) Stigma as a barrier to recovery: The consequence of stigma for the self-esteem of people with mental illness. Psychiatr Serv. 52:1621–1626.
Lysaker PH, Davis LW, Warman DM, Strasburger A, Beattie N (2007) Stigma, social function and symptoms in schizophrenia and schizoaffective disorder: Associations across 6 months. Psychiatry Res. 149:89 –95.
Ma YC, Lin SJ, Hu WH, Hsiung PC (2005) The coping process of patients with schizophrenia: Searching for a place of acceptance. Tzu Chi Med J. 17:247– 256.
Makanjuola AB, Adeponle BA, Obembe OA (2007) A comparison of quality-of-life in schizophrenia and affective disorder patients in a Nigerian tertiary hospital. Transcult Psychiatr. 44:65–78.
Markowitz FE (1998) The effects of stigma on the psychological well-being and life satisfaction of persons with mental illness. J Health Soc Behav. 39:335–347. Pan AW, Chen YL, Hsiung PC, Chung L (2008) The study of the psychometric
qualities of the social support questionnaire. Paper presented at: 8th Occupa-tional Therapy Conference of NaOccupa-tional Taiwan University; April 19; Taipei, Taiwan.
Pan AW, Chung L, Fife BL, Hsiung PC (2007) Evaluation of the psychometrics of the Social Impact Scale: A measure of stigmatization. Int J Rehab Res. 30:235–238.
Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT (1981) The stress process.
J Health Soc Behav. 22:337–356.
Pearlin LI, Nguyen KB, Schieman S, Milkie MA (2007) The life-course origins of mastery among older people. J Health Soc Behav. 48:164 –179.
Pearlin LI, Schooler C (1978) The structure of coping. J Health Soc Behav. 19:2–21.
Pedhazur EJ (1982). Multiple Regression and Behavioral Science. Orlando (FL): Harcourt Brace.
Perlick DA, Rosenheck RA, Clarkin JF, Sirey JA, Salahi J, Struening EL, Link BG (2001) Stigma as a barrier to recovery: Adverse effects of perceived stigma on social adaptation of persons diagnosed with bipolar affective disorder.
Psychiatr Serv. 52:1627–1632.
Phillips MR, Pearson V, Li F, Xu M, Yang L (2002) Stigma and expressed emotion: Study of people with schizophrenia and their family members in China. Br J Psychiatry. 181:488 – 493.
Picardi A, Rucci P, de Girolamo G, Santone G, Borsetti G, Morosini P (2006) The quality of life of the mentally ill living in residential facilities: Findings from a national survey in Italy. Eur Arch Psychiatry Clin Neurosci. 256:372–381.
Rosenfield S (1992) Factors contributing to the subjective quality of life of the chronic mentally ill. J Health Soc Behav. 33:299 –315.
Rosenfield S (1997) Labeling mental illness: The effect of received services and perceived stigma on life satisfaction. Am Sociol Rev. 62:660 – 672.
Sarason IG, Sarason BR, Shearin EN, Pierce GR (1987) A brief measure of social support: Practical and theoretical implications. J Soc Pers Relat. 4:497–510. Schieman S, Turner HA (1998) Age, disability and the sense of mastery. J Health
Soc Behav. 39:169 –186.
Schulze B (2007) Stigma and mental health professionals: A review of the evidence on an intricate relationship. Int Rev Psychiatry. 19:137–155. Shiau SJ (1995) Family Assessment Tools for Families with Schizophrenia:
Instruments Development and Applications in Home Health Care. Taipei
(Taiwan): Department of Health.
Sim K, Chan YH, Chua TH, Mahendran R, Chong SA, McGorry P (2006) Physical comorbidity, insight, quality of life and global functioning in first episode schizophrenia: A 24-month, longitudinal outcome study. Schizophr
Res. 88:82– 89.
Sirey JA, Bruce ML, Alexopoulos GS, Perlick DA, Friedman SJ, Meyers BS
(2001) Perceived stigma and patient-rated severity of illness as predictors of antidepressant drug adherence. Psychiatr Serv. 52:1615–1620.
Skevington SM, Lotfy M, O’Connell KA, Group W (2004) The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHO-QOL group. Qual Life Res. 13:299 –310.
Struening EL, Perlick DA, Link BG, Hellman F, Herman D, Sirey JA (2001) Stigma as a barrier to recovery: The extent to which caregivers believe most people devalue consumers and their families 关comment兴. Psychiatr Serv. 52:1633–1638.
Subhash S (1995). Applied Multivariate Techniques. New York (NY): Springer. Ulas H, Akdede BB, Ozbay D, Alptekin K (2008) Effect of thought disorders on quality of life in patients with schizophrenia. Prog Neuropsychopharmacol Biol
Psychiatry. 32:332–335.
Vauth R, Kleim B, Wirtz M, Corrigan PW (2007) Self-efficacy and empowerment as outcomes of self-stigmatizing and coping in schizophrenia. Psychiatry Res. 150:71– 80.
Wegener S, Redoblado-Hodge MA, Lucas S, Fitzgerald D, Harris A, Brennan J (2005) Relative contributions of psychiatric symptoms and neuropsychological functioning to quality of life in first-episode psychosis. Aust N Z J Psychiatry. 39:487– 492.
Wright ER, Gronfein WP, Owens TJ (2000) Deinstitutionalization, social rejec-tion and the self-esteem of former mental patients. J Health Soc Behav. 41:68 –90.
Yang LH, Kleinman A, Link BG, Phelan JC, Lee S, Good B (2007) Culture and stigma: Adding moral experience to stigma theory. Soc Sci Med. 64:1524 – 1535.
Yanos PT, Rosenfield S, Horwitz AV (2001) Negative and supportive social interactions and quality of life among persons diagnosed with severe mental illness. Community Ment Health J. 37:405– 419.
Yao G, Chung CW, Yu CF, Wang JD (2002) Development and verification of validity and reliability of the WHOQOL-BREF Taiwan version. J Formosa
Med Assoc. 101:342–351.
Yao G, Wu CH (2009) Similarities and differences among the Taiwan, China and Hong-Kong versions of the WHOQOL questionnaire. Soc Indic Res. 91:79 –98. Zissi A, Barry MM, Cochrane R (1998) A mediational model of quality of life for individuals with severe mental health problems. Psychol Med. 28:1221–1230.