案例報告
A Case Report of Hypotension and
Bradycardia Associated
with Immediate-Release Diltiazem Overdose
Li-Yao Lee
1, Chen-Chun Kuo
1, Ying-Hao Lu
1,2*, Yaw-Bin Huang
1,31
Department of Pharmacy, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung, Taiwan
2School of Pharmacy, College of Pharmacy, Kaohsiung Medical University, Kaohsiung, Taiwan 3
Graduate Institute of Clinical Pharmacy, College of Pharmacy, Kaohsiung Medical University, Kaohsiung, Taiwan
ABSTRACT
A 31-year-old female had attempted suicide with 56 diltiazem 30 mg immediate-release (IR) tablets of her father’s prescription and was admitted into emergency department after one hour of ingestion. First vital signs revealed temperature of 36.2℃, blood pressure of 58/27 mmHg and pulse of 71 beats/min. The electrocardiogram showed junctional bradycardia. She was given the following treatment: GI decontamination (activated charcoal, AC 61.5g), antidotes (calcium gluconate 10% 10mL and glucagon 3mg) and supportive care (atropine 1mg, dopamine 800mg, norepinephrine 8mg and normal saline 500mL). After 12 hours of emergency treatment, her blood pressure and heart rate returned to normal (114/70 mmHg and 88 beats/min). Finally, she was subsequently transferred to the intensive care unit for further observation and treatment, and then discharged after 4 days of admission. In calcium channel blockers (CCBs) intoxication, hypotension and bradycardia are the most important clinical features and non- dihydropyridine classes have much effect in suppression cardiac contractility. In this case, copious medication was used to treat 1) hypotension and 2) bradycardia respectively: 1) calcium gluconate, dopamine, norepinephrine and insulin; 2) calcium gluconate, glucagon and atropine. This case successfully treated suicidal diltiazem overdose, and showed that in the management of CCB overdose, attention must be paid to severe fetal side effects of hypotension and bradycardia using various medications with the purpose of maintaining the vital signs.
Key words: hypotension, bradycardia, immediate release, diltiazem overdose, calcium channel blockers 聯 絡 人:呂英豪 通 訊 處:807 高雄市三民區自由一路 100 號 高雄醫學大學 聯絡電話:07-3121101 分機 7174 電子郵件:[email protected] [email protected]
INTRODUCTION
Calcium channel blockers (CCBs) are commonly used in treatment of hypertension and tachyarrhythmias [1]. Diltiazem and verapamil belong to non-dihydropyridine CCB classification that selectively block L-type calcium channel in the myocardium, therefore both myocardial contractility and vascular smooth muscle contractility are affected by them (Table 1) [1,2]. CCB intoxication is one of the leading causes from poisoning associated with significant morbidity and mortality. The American Association of Poison Control Centers Toxic Exposure Surveillance System (TESS) reported over 9,500 cases of CCB intoxication during 2004 [3]. Sixteen percent of all cardiovascular drug exposures resulted from CCBs that also accounted for 38 percent of deaths in this class [3]. Compared to dihydropyridine CCBs, diltiazem and verapamil overdoses are considered to manage not only severe vascular dilation but also critical myocardial depression [4]. To this day, the literature has reported many events concerning diltiazem or verapamil overdoses and their treatment(s) [5,6,7,8], and most occurred in extended-release (ER) or sustained-release (SR) form.
We report a case of hypotension and bradycardia accompanied with intentional immediate-release (IR) diltiazem overdose, and treated with gastrointestinal (GI) decontamination, antidotes (calcium gluconate and glucagon) and supportive care to minimize diltiazem overdose-induced hypotension and bradycardia.
CASE REPORT
A 31-year-old female had attempted suicide with 56 diltiazem 30 mg IR tablets and was admitted into emergency department (ED) after one hour following ingestion. No systemic disease (such as hypertension or diabetes mellitus), alcohol abuse or smoking, but depressive mood had noted. Arrived ED, she maintained clear mental status but felt cold. The first vital signs revealed temperature of 36.2 ℃, blood pressure of 58/27 mmHg and heart rate of 71 beats/min. The electrocardiogram (ECG) showed junctional bradycardia and included PR interval prolongation. The initial laboratory parameters were in normal range except for the fasting blood sugar of 173 mg/dL (normal 70-110 mg/dL).
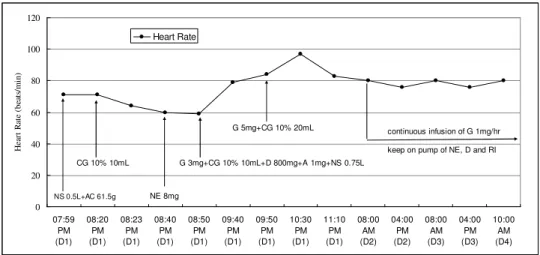
After intubation, 500 mL of normal saline and 61.5 g of activated charcoal (AC) were administered. Ten milliliters of 10% calcium gluconate (1g) was given when blood pressure from 58/27 mmHg fell to 53/22 mmHg without a change in heart rate, and an observed improvement in blood pressure (120/100 mmHg) was immediately shown (Figures 1 and 2). After 7 minutes, norepinephrine 8 mg was administered due to her low blood pressure of 60/38 mmHg. At the same time, glucagon 3mg, 10-mL 10% calcium gluconate (1g), dopamine 800 mg, atropine 1mg and normal saline 750 mL were administered to maintain her vital signs. After one hour of observation, glucagon 3 mg and two of 10-mL 10% calcium gluconate (2g) were then administered. Systolic blood pressure returned to 80-90 mmHg, and heart rate remained within the range of 80-90 beats/min. After 12 hours, blood pressure of 114/70 mmHg and heart rate of 88 beats/min were back to normal. She
was subsequently transferred to the intensive care unit (ICU) for further observation and treatment. Continuous infusion of glucagon 1mg/hr was given and norepinephrine, dopamine and regular insulin (RI) were kept on pump. Finally, she was discharged after 4 days of admission.
Discussion
Treatment of CCB Overdose-Induced Hypotension and Bradycardia
To keep circulation is the major treatment of CCB overdose; therefore hypotension and bradycardia are the most important clinical features in CCB overdose for maximal treatment [9]. Hypotension may be seen in each CCB overdose case, but bradycardia usually is seen only in non-dihydropyridine class CCB (diltiazem and verapamil) overdoses as a result of the effect of more suppression of cardiac contractility (Table 1)[4]. The neuro-protective effect of CCBs, CCB-poisoned patients may maintain a surprisingly clear mental status at the initial period in spite of hypotension. However, the mental status rapidly deteriorated if there is no active treatment [9]. This specific clinical feature was also observed in this case. Hypotension was clearly presented in the variation of systolic and diastolic pressure (Figure 1), but apparently slow heart rate was not observed in Figure 2. Even though heart rate was not apparent, we still positively handled this problem due to junctional bradycardia and included PR interval prolongation as shown in ECG. Table 2 is a summary of the treatment for CCB overdose-induced hypotension and bradycardia in this case.
The Use of Glucagon in CCB overdose
Intravenous glucagon is recommended as an
antidote for CCB overdose. Its mechanism is related to an increase of intracellular cyclic AMP levels in the myocardium resulting in phosphorylation of L-type calcium channels and calcium influx into cells [10], therefore glucagon is effective to increase heart rate in CCB toxicity of human cases [8,11]. The dosing regimen is: 1) bolus therapy to IV of 1-5 mg repeated up to a total of 15 mg; and 2) continuous infusion as determined by bolus amount needed to obtain response [4]. The ER physician followed the above regimen and gained good control of heart rate as shown in Figure 2.
Hyperglycemia and High-Dose Insulin Therapy
CCB overdose results in hyperglycemia, primarily due to the blockade of pancreatic L-type calcium channels to inhibit insulin release [12]. When blood sugar level reaches double the baseline, an initial regular insulin bolus of 0.1 IU/kg should be given to instantly treat CCB overdose-induced hyperglycemia and then a continuous infusion of 0.2-0.5 IU/kg per hour should be started [13]. Initially, the fasting blood sugar of 173 mg/dL (normal 70-110 mg/dL) did not reach double the maximum baseline (220 mg/dL), therefore the physician in our ER did not consider to actively manage CCB overdose-induced hyperglycemia until the patient was transferred to ICU.
Difference Treatments between IR and ER/SR Preparations
CCB medications are both available in IR and ER/SR preparations. The ER/SR medications are in wide clinical use and more reported in CCB intoxication than IR’s [1]. Gastric lavage should be considered in all patients of CCB
overdose within one to two hours of ingestion. Even if patients are asymptomatic, single-dose AC should be administered in IR preparations [5,9]. Due to delayed absorption, more than one dose of AC may be of value with ingestion of ER/SR products [4]. In this case, only one AC was administered to observe the above principle. Whole bowel irrigation (WBI) is another gut decontamination option in ER/SR medications of CCB overdose [4]. As a result of high-protein binding in CCBs, hemodialysis may not be effective to eliminate IR or ER/SR forms. For asymptomatic patients who ingested IR-form CCBs, the ECG should be monitored for the first
8-12 hours following ingestion [4]. For all the patients who ingested ER/SR-form CCBs, the monitoring should be extended to 36 hours or more [4].
No single agent has been consistently effective in the treatment of severe CCBs overdoses, therefore multiple medications are required to stabilize severely poisoned patients. This case successfully treated suicidal IR diltiazem overdose, and showed that in the management of CCB overdose, attention must be paid to severe fetal side effects of bradycardia and hypotension using different medications for the purpose of maintaining vital signs.
REFERENCES
1. Eisenberg MJ, Brox A, Bestawros AN. Calcium channel blockers: An update. Am J Med 2004;116:35-43.
2. Katz AM. Cardiac ion channels. N Engl J Med 1993;328:1244-51.
3. Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2004 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 2005;23:589-666.
4. Salhanick SD, Shannon MW. Management of calcium channel antagonist overdose. Drug Saf 2003;26:65-79.
5. Bologa C, Scripcariu P, Ciuhodaru L, Anton G, Buga C. Cardiodepressive syndrome after diltiazem overdose. TMJ 2006;56:173-5. 6. Cantrell FL, Williams SR. Fatal
unintentional overdose of diltiazem with antemortem and postmortem values. Clin Toxicol 2005;43:587-8.
7. Proano L, Chiang WK, Wang RY. Calcium channel blocker overdose. Am J Emerg Med 1995;13:444-50.
8. Doyon S, Roberts JR. The use of glucagon in a case of calcium channel blocker overdose. Ann Emerg Med 1993; 22:1229-33.
9. Fox E, Crouch BI. Calcium channel blocker toxicity and treatment issues. Toxupdate 1999;1:1-4.
10. Bailey B. Glucagon in beta-blocker and calcium channel blocker overdoses: a systematic review. J Toxicol Clin Toxicol 2003; 41:595.
11. Mahr NC, Valdes A, Lamas G. Use of glucagon for acute intravenous diltiazem toxicity. Am J Cardiol 1997;79:1570. 12. Levine M, Boyer EW, Pozner CN, Geib A-J,
Thomsen T, Mick N, Thomas. Assessment of hyperglycemia after calcium channel blocker overdoses involving diltiazem or verapamil. Crit Care Med 2007;35:2071-5. 13. Shepherd G, Klein-Schwartz W. High-dose
insulin therapy for calcium-channel blocker overdose. Ann Pharmacother 2005; 39:923-30.
Table 1. Relative cardiovascular effect between CCBs
Compound Class Myocardial Contractility Vascular Dilatation Diltiazem Benzothiazepines ↓ ↑ Verapamil Phenylalkylamines ↓↓ ↑ Amlodipine Dihydropyridines ↓/0 ↑↑ Nifedipine Dihydropyridines ↓/0 ↑↑ Note: ↓=decrease; 0= no effect; ↑=increase.
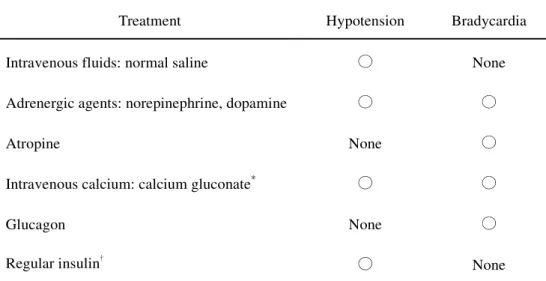
Table 2. Treatment of hypotension and bradycardia for CCB overdose in this case
Treatment Hypotension Bradycardia Intravenous fluids: normal saline ○ None Adrenergic agents: norepinephrine, dopamine ○ ○
Atropine None ○
Intravenous calcium: calcium gluconate* ○ ○
Glucagon None ○
Regular insulin† ○ None
* Intravenous calcium has two slats of calcium chloride and calcium gluconate. † Regular insulin is not only used to treat hypotension but also mainly to improve
0 20 40 60 80 100 120 140 07:59 PM (D1) 08:20 PM (D1) 08:23 PM (D1) 08:40 PM (D1) 08:50 PM (D1) 09:40 PM (D1) 09:50 PM (D1) 10:30 PM (D1) 11:10 PM (D1) 08:00 AM (D2) 04:00 PM (D2) 08:00 AM (D3) 04:00 PM (D3) 10:00 AM (D4) B lo o d P re s s u re ( m m H g ) Systolic Pressure Diastolic Pressure NS 0.5L+AC 61.5gCG 10% 10mL G 5mg+CG 10% 20mL NE 8mg G 3mg+CG 10% 10mL+D 800mg+A 1mg+NS 0.75L continuous infusion of G 1mg/hr keep on pump of NE, D and RI
Figure 1. Effects of treatment on blood pressure. Abbreviation: A=Atropine, AC= Activated Charcoal, CG=Calcium Gluconate, D=Dopamine, G=Glucagon, NE=Norepinephrine, NS=Normal Saline.
0 20 40 60 80 100 120 07:59 PM (D1) 08:20 PM (D1) 08:23 PM (D1) 08:40 PM (D1) 08:50 PM (D1) 09:40 PM (D1) 09:50 PM (D1) 10:30 PM (D1) 11:10 PM (D1) 08:00 AM (D2) 04:00 PM (D2) 08:00 AM (D3) 04:00 PM (D3) 10:00 AM (D4) H ea rt R at e (b ea ts /m in ) Heart Rate NS 0.5L+AC 61.5g CG 10% 10mL G 5mg+CG 10% 20mL NE 8mg G 3mg+CG 10% 10mL+D 800mg+A 1mg+NS 0.75L continuous infusion of G 1mg/hr keep on pump of NE, D and RI