行政院國家科學委員會專題研究計畫成果報告
腦幹與大腦半球梗塞對情緒狀態之影響:長期性追蹤研究 計畫編號: NSC 88-2413-H-002-022 執行期間: 87年 8月 1日至 88年 7月 31 日 計畫主持人:花茂棽 共同主持人:陳獻宗、徐文俊 執行單位:台灣大學 中華民國 88 年 11月 22日Effects of Brainstem and Hemispheric Infarction on Emotional Status: A Longitudinal Study (I)
中文摘要: 第一年研究主要目的是檢驗腦幹中風病人的情緒狀態。總共五組中風病人分別為 左側大腦與右側大腦皮質中風病人、左側與右側皮質下腦部中風病人以及腦幹中 風病人,以及一組正常受試者參與本研究。每位受試者皆接受一組情緒功能的測 驗,這六組受試者在年齡教育程度與性別相互配對。資料分析結果顯示:腦幹病 人有輕微程度情緒功能的改變;憂鬱是主要的症狀。除此以外情緒功能的問題上 包括極輕微到輕微體化型、強迫性意念與行為以及焦慮等症狀,由於目前這些結 果來自有限病人之樣本,因此進一步繼續探討這些問題是否真正存在是有其必要 性的。至於原計畫在第一年欲探討部分有關這些腦幹中風病人情緒功能改變的現 象是否為短暫性質或持久性質的問題,同樣的,在相當有限的追蹤資料情況下, 僅能留待第二年的研究計畫來探討。 關鍵字:憂鬱症、情緒功能狀態、腦幹中風
ABSTRACT
The aim of the first-year study was to examine the emotional status of the patients
with brainstem stroke. An emotional function test battery was administered to five
groups of the adult patients with cerebral hemispheric, subcortical, and brainstem
strokes, and one group of normal control adults. Members of these six groups were
matched in terms of age, educational level, and sex. Comparing the test results
revealed that the patients with brainstem had a mild impairment of emotional function,
mainly depression. In addition, otherwise psychopathological manifestations
including slight to mild somatization, obsessive-compulsive symptom, and anxiety
were also noticed. Since our findings were based on the limited data, further
investigation is necessary. Likewise, only a few patients have received the 6-month
follow-up evaluation of their emotional function in this first-year study. The issue
regarding whether or not emotional changes evident in the patients with brainstem
stroke are transient or persistent, thus, awaits the second-year investigation.
Stroke is a common disease of central nervous system. In Taiwan this disease has
been the second leading cause of death for all ages (Huang, Chiang & Lee, 1997).
Physical disability, and a variety of cognitive impairments, such as aphasia, amnesia,
apraxia, agnosia, aprosodia, dysarthria, attentional problem, neglect, and visuospatial
disorientation are frequent consequences of cerebral hemispheric stroke (Heilman &
Valenstein, 1993; Lezak, 1995; Walsh, 1994). In addition to these deficits, emotional
changes are also a common sequela (Hosking, Marsh & Friedman, 1996). The
disturbances include depression, emotional lability, apathy, irritability, agoraphobia,
social withdrawal, self-neglect, and anxiety (House, Dennis, Mogridge, Warlow,
Hawton & Jones, 1991;Morris, Robinson, & Raphael, 1993; Nelson, Cicchetti, Satz,
Sowa & Mitrushina, 1994).
The implied clinical and economic impacts of these emotional disturbances on the
stroke patients are multifold (Spencer, Tompkins & Schultz, 1997). First, the patients
with emotional problems undertake more negative thinking and stress negative results
(Ingram, Kendall, Smith, Donnell & Ronan, 1987). Consequently, sundry cognitive
function changes in these patients might be exaggerated though cognitive impairments
tend to co-occur with emotional problems (Seibert & Ellis, 1991; Speedie et al., 1990).
Secondly, sundry cognitive function changes, such as depression can be a vital
and their caregivers might be changed tensely by these emotional sequelae (Spencer et
al.,1997). Therefore, in order to offer the patients the supreme opportunity for
treatment profits, a great care for their emotional disturbances is merited.
Depression has generally been considered to be the most common emotional
consequence of cerebral hemispheric stroke (Nelson, 1994; Price, 1990). The
prevalence rate of poststroke depression, however, varies extensively from less than
25% up to more than 60% (Astrom, Adolfsson & Asplund, 1993). Methodological
discrepancies mainly including the selection of patients, the time of evaluation since
the stroke and the duration of the assessment period, as well as diverse diagnostic
criteria and psychopathological measures have a significant contribution to this
variation (Astrom et al., 1993; Hosking et al., 1996). Furthermore, the proportion of
poststroke depression does not keep steady throughout the poststroke period (Astrom
et al., 1993). The manifestations of otherwise emotional problems, such as
agoraphobia, social withdrawal, anxiety, mania, catastrophic reactions, and apathy
recently have also been observed in the patients following cerebral hemispheric stroke
(e.g., House et al., 1991; Morris et al., 1993; Robinson & Starkstein, 1997). The issue
regarding whether or not depression is the most frequent emotional result of cerebral
hemispheric stroke, thus, becomes controversial and awaits further investigation.
though the literature in this area is less extensive than that of cerebral hemispheric
stroke. Generally, depression is significantly related to lesions of left basal ganglia
(Starkstein, Robinson, Berthier & Price, 1988). However, mania, bipolar affective
disorders, and psychosis are highly associated with right subcortical (basal ganglia or
thalamus) lesions (Robinson et al., 1988; Starkstein et al., 1991; Starkstein, Robinson
& Berthier, 1992; Trimle & Cummings, 1981). Anxiety and apathy have a high
frequency of lesions involving the posterior limb of the internal capsule (Robinson &
Starkstein, 1997; Starkstein et al., 1993a) while catastrophic reactions are notably
related to anterior subcortical lesions (Starkstein et al., 1993b).
The dysfunction of the biogenic amine system has been hypothesized to be one of
the mechanisms that may play an important role in the cause of depression (Beatty,
1995; Conn, 1995). Both noradrenergic and serotonergic cell bodies are located in the
locus coeruleus and raphe nucleus of the brainstem, and send ascending projections to
the frontal cortex through the median forebrain bundle. The ascending pathways then
arc posteriorly and travel longitudinally through the deep layers of the cortex,
arborizing and sending terminal projections into the superficial cortical layer
(Morrison, Molliver, & Grzanna, 1979). On the basis of neuroanatomical evidences
and clinical findings, Robinson and his colleagues (1984) proposed that poststroke
due to lesions in either the frontal cortex or basal ganglia. If this is the case,
depressive symptoms should also be evident in the patients with brainstem stroke
involving the rostral pons and caudal mesencephalon which are sites for the
serotonergic raphe nucleus and the noradrenergic locus coeruleus (Lang, 1991).
The literature of emotional disturbances in the patients following brainstem stroke,
however, is very limited. Trimble and Cumminings (1981) reported that
manifestations of suicidal ideation, unstable mood, euphoria, depressive feelings, and
emotional lability were noted in two patients with brainstem stroke. However, the
definite lesioned areas of both patients determined by the CT scan were located in the
thalamus rather than the brainstem. Starkstein, Robinson, Berthier and Price (1988)
found that patients with posterior circulation lesions involving the brainstem and/or
cerebellum had a remarkably low frequency of depression, and a significantly short
duration of depressive symptoms. Unfortunately, since no otherwise
psychopathological measures, with the exception of depression and anxiety tests, were
used in their study, the issue of whether or not other emotional sequelae might also be
manifested in patients following brainstem stroke remains unknown.
The report of emotional disturbances in poststroke patients in Taiwan is lacking.
In order to explore the above unclear issue, and to document the literature in Taiwan,
that is, 5 patient cohorts and 1 group of normal controls will be included. 5 patient
groups consist of 1 group of patients following brainstem stroke, 1 with left and 1
with right cortical stroke, and 1 with left and 1 with right basal ganglion stroke. The
first-year study goal is to complete 1- and 6-monthss poststroke assessment of
emotional function; the second-year study goal is to complete 1-year poststroke
evaluation of emotional status. The specific aims of the study, thus, are to examine the
following questions: 1) Is there an impairment of emotional status in patients with
brainstem stroke? 2) If so, does the deficit only involve depression, as Starkstein et
al’s observation (1988), or also include otherwise emotional function tested? 3) If
depression or/and otherwise emotional changes does/or occur in the patients with
brainstem stroke, is/are the deficit(s) transient or persistent?
METHOD
Par ticipants. Because of a very high dropout rate of the participants, 6 groups with
only 55 volunteer adults were included in the first-year study. There were 37 stroke
patients including 12 with brainstem (Group 1), 3 with left cortical (Group 2), 5 with
left subcoritcal (Group 3), 8 with right cortical (Group 4), and 9 with right subcortical
(Group 5) lesions, and 18 normal control subjects (Group 6). The lesion locations
were verified by MRI, and all of these patients were victims of the first stroke in the
drug treatment), and psychiatric history. The patients were also free of dementia,
confusional state, anosognosia, and moderate or severe comprehension deficits.
The mean differences in age were not significantly different, with the exception of
Groups 4 and 5 and Groups 4 and 6. That is, the mean age of the patients with right
cortical stroke was significantly younger than that of the patients with right
subcortical stroke and of the normal controls (Table 1). The mean differences in
education were also not significantly different. All participants were right-handed in
which hand dominance was ascertained by the history that the participant has always
used his/her right hand preferentially for doing skillful activities, such as writing and
holding chopsticks.
Tests and procedure. After giving informed consent, each participant will receive a
series of neuropsychological tests. They included cognitive function and emotional
status measures. The Temporal Orientation Test (Benton, Hamsher, Varney & Spreen,
1983), the Orientation to Personal Information and Place (Hamsher, 1983), Object
Naming Test (Spreen & Benton, 1969), and Aural Comprehension (Benton &
Hamsher, 1978) were used to rule out the participants suspectable for dementia,
moderately or severely receptive aphasia, confusional state, and anosognosia. The test
battery of emotional status consisted of Symptom Checklist-90-R (Derogatis, 1977),
1987), and a semi-structured Standard Neurobehavioral Interview Inventory
(Hamsher, 1983). In addition, Canadian Neurological Scale and Barthel Index
(Mahoney & Barthel, 1965) were also used to measure the severity of the patient’s
physical disability, and evaluate the degree of his/her independence in basic activities
of daily living respectively. The assessment was administered in an examing room
between 11 AM and 2PM to minimize any possible effects of diurnal mood variation
on interview responses, as Starkstein, Cohen, Fedoroff, Parikh, Price, and Robinson
(1990). All measures were Chinese versions.
In order to obtain reliable and valid ratings of the patient’s emotional status, we
also asked the participant’s significant others, particularly family caregivers of the
patient, to rate the emotional status of the participant. All of the significant informants
of the patients will be free of emotional disturbances, dementia, and psychiatric
history. For the present, our available patients only received the first examination, that
is, they were examined at the poststroke periord of 1 month while a few (2 patients)
received the second examination, that is, 6 months after the onset of stroke.
RESULTS
Since the measures of emotional status are ordinal scales, Kruskal-Wallis one-way
analysis of variance by Ranks (Marascuili and McSweeney, 1977) was used to
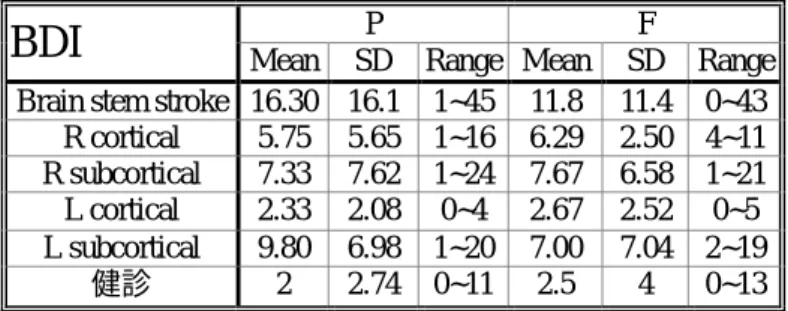
Inventory and SCL-90-R was different from that of the normal control participants.
On the Beck Depression Inventory, the patients with brainstem stroke had the highest
mean rank followed by the patients with left subcortical stroke, the patients with right
subcortical stroke, the patients with right cortical stroke, the patients with left cortical
stroke, and the normal controls. The mean rank differences among the participant
groups did reach a statistical difference (Chi square=17.92, df = 5, p<.05). Nemenyi’s
post-hoc pairwise contrasts with Bonferroni corrections for a control of Type I error
were subsequently used to analyze the data. The results, however, did not reveal any
significant differences between the participant groups (Tables 2 and 3).
Likewise, on the SCL-90-R, the highest mean rank to the lowest on the
Somatization subscale was the patients with brainstem stroke, the patients with left
subcortical stroke, the patients with right cortical stroke, the patients with right
subcortical stroke, the normal controls, and the patients with left cortical stroke. On
the Obsessive-Compulsive subscale, the patients with brainstem stroke had the
highest mean rank followed by the patients with right subcortical and cortical stroke,
the patients with left subcortical and cortical stroke, and the normal controls. On the
Interpersonal Sensitivity subscale, the highest mean rank to the lowest was the
patients with brainstem stroke, with left subcortical stroke, with right subcortical
brainstem stroke had the highest mean rank on the Depression subscale, followed by
the patients with right and left subcortical stroke, with right cortical stroke, the normal
controls, and left cortical stroke. On the Anxiety subscale, the patients with brainstem
stroke had the highest mean rank followed by the patients with right cortical stroke,
with right and left subcortical stroke, the normal controls, and with left cortical stroke.
The highest mean rank on the Hostility subscale was the patients with brainstem
stroke, followed by the patients with left and right subcortical stroke, the normal
controls, and the patients with right and left cortical stroke. On the Phobia subscale,
the highest mean rank to the lowest was the patients with brainstem stroke, with right
cortical stroke, with left and right subcortical stroke, the normal controls, and the
patients with left cortical stroke. The highest mean rank to the lowest on the Paranoid
Ideation subscale was the patients with right cortical stroke followed by the patients
with brainstem stroke, the normal controls, the patients with left and right subcoritcal
stroke, and with left cortical stroke. On the psychoticism subcalse, the highest mean
rank score was the patients with brainstem stroke, followed by the patients with right
cortical stroke, with left subcortical stroke, the normal controls, the patients with right
subcortical stroke, and the patients with left cortical stroke. The differences of the
mean rank over these subcales, however, only involved Somatization (Chi
Global (Chi square=12.15, df =5, p<.04) reached a statistically significant level. No
significant differences were found when Nemenyi’s post-hoc pairwise contrasts with
Bonferroni corrections for controlling Type I error were subsequently performed.
The highest mean rank to the lowest of the significant informants of the
participants on the BDI was the patients with brainstem stroke, followed by the
patients with left and right subcortical stroke, the patients with right and left cortical
stroke, and the normal controls. The mean rank differences, analyzed by
Kruskall-Wallis one-way ANOVA revealed, did reach a statistical significant level (Chi
square=3.74, df=5, p<.007). Nemenyi’s post-hoc pairwise comparisons with
Bonferroni corrections for controlling Type I error were subsequently performed.
However, none reached a statistically significant level.
The rating of the significant informants of the participants on the subscales of the
SCL-90-R was as followed. On the Somatization subscale, the patients with brainstem
stroke had the highest mean rank, followed by the patients with left subcortical stroke,
with right cortical and subcortical stroke, the normal controls, and the patients with
left cortical stroke. The highest mean rank to the lowest on the Obsessive-Compulsive
subscale was the patients with brainstem stroke, followed by the patients with right
subcortical and cortical stroke, with right coritcal and subcortical stroke, with left
Sensitivity subscale, the patients with brainstem stroke had the highest mean rank,
followed by the patients with left subcortical stroke, with right cortical and subcortical
stroke, the normal controls, and the patients with left cortical stroke. The highest
mean rank to the lowest on the Depression subscale was the patients with the patients
with brainstem, followed by the patients with right subcortical and cortical stroke,
with left subcortical and cortical stroke, and the normal controls. On the Anxiety
subscale, the patients with brainstem stroke had the highest mean rank, followed by
the patients with right subcortical stroke, with left cortical stroke, with right cortical
and left subcortical stroke, and the normal controls. On the Hostility subscale, the
patients with brainstem stroke had the highest mean rank, followed by the patients
with right subcortical and cortical stroke, with left subcortical stroke, the normal
controls, and the patients with left cortical stroke. The highest mean rank to the lowest
on the Phobia subcale was the patients with right subcortical and cortical stroke, with
left subcortical stroke, the normal controls, and the patients with left cortical stroke.
On the Paranoid Ideation subscale, the patients with brainstem stroke had the highest
mean rank, followed by the patients with right cortical and left subcortical stroke,
with right subcortical stroke, the normal controls, and the patients with left cortical
stroke. The highest mean rank on the Psychoticism subscale was the patients with
with left subcortical stroke, the normal controls, and the patients with left cortical
stroke.
The data analysis by Kruskall-Wallis one-way ANOVA revealed that the mean
rank differences of Somatization (Chi square= 11.28, df=5, p<.05),
Obsessive-Compulsive (Chi square=12.04, df=5, p<.04), Depression (Chi square=11.80, df=5,
p<.04), Anxiety (Chi square=11.24, df=5, p<.05), and Psychoticism (Chi
square=12.13, df=5, p<.04) subscales among these subject groups reached a
statistically significant level. Subsequent Nemenyi’s post-hoc pairwise contrasts
with Bonferroni corrections for controlling Type I error, however, did not reach a
statistically significant level.
In order to determine whether or not the ratings of the participants and their
significant informants on the BDI and SCL-90-R were different. On the BDI, the
discrepant score between the participant and his/her significant informant for each
subject group was calculated, and then a match-paired t test was used to analyze the
data. The result revealed that the differences did not reach a statistically significant
level. Likewise, for each subject group the ranking differences between the
participant and his/her significant informant on each of the subscales of the SCL-90-R
were not statistically significant.
Is there an impairment of emotional status in the patients with brainstem stroke?
Because of the high dropout of the patients, our results based on the limited data did
not revealed that the patients with brainstem stroke had remarkably emotional
impairments compared with their normal counterparts. For the time being the answer
for our first question, thus, seems to be negative. Meanwhile, our preliminary results
also appear to further support Starkstein and his co-workers’ findings (1988) in which
they noted the patients with brainstem stroke having a significant low frequency of
emotional changes. However, our results also revealed some degree of subtle to mild
emotional changes in these patients with brainstem stroke. The definite conclusion,
thus, awaits the second-year investigation.
If so, does the deficit only involve depression, as Starkstein and his colleagues’
observation (1988), or also include otherwise emotional function tested? Accordingly,
the definite answer for the first question is pending. Thus, it appears to be
appropriate to make some comments on this issue. Our patients with brainstem
stroke not only had mild depression, but also had other emotional changes. These
otherwise emotional problems consisted of somtization, obsessive-compulsive
symptoms, anxiety, hostility, paranoid ideation, and psychoticism.
Most of the literature showed that depression was major emotional changes
1990). Our findings based on the patients with either the left or right cerebral
hemispheric stroke, however, were not consistent with these earlier observations.
Instead, somatization was mainly evident in our patients with right cerebral
hemispheric stroke. In addition, obsessive-compulsive symptom and anxiety were
also evident in the patients with right cerebral hemispheric stroke. These results
seemed to be consistent with the researchers’ observations (e.g., House et al., 1991;
Morris et al., 1993; Robinson & Starkstein, 1997).
Depression has often been seen in the patients with lesions of the subcortical
regions, particularly the areas of left basal ganglia (Starkstein Robinson, Berthier &
Price, 1988). Generally, our results were compatible with these observations.
Nevertheless, we did not note our patients having any remarkably asymmetric
manifestation between the two subcortical hemispheric strokes in terms of this
specific aspect of emotional changes. Robinson and Starkstein (1997), and Starkstein
and his co-workers (1993) reported that the patients with lesions involving the
posterior limb of the internal capsule were often evident of anxiety. We did also
notice our patients with the subcortical stroke having the symptom of anxiety.
However, the lesion area in our patients not only involved the subcortical white
matters, but also the adjacent subcortical gray regions. The findings of mania, bipolar
in the patients with subcortical lesions (e.g., Robinson et al., 1988; Starkstein et al.,
1991; Starkstein, Robinson, & Berthier, 1992; Trimble & Cummings, 1981; Starkstein
et al., 1993). We have not yet observed these emotional changes in our patients with
the subcortical stroke. However, the manifestation of somatization and
obsessive-compulsive symptom was also evident in our patients.
The dysfunction of the biogenic amine system has been hypothesized to be one of
the mechanisms that may play an essential role in the cause of depression (Beatty,
1995; Conn, 1995). Since both noradrenergic and serotonergic cell bodies are located
in the locus coeruleus and raphe nucleus of the brainstem, depressive symptoms
should be evident in the patients with brainstem stroke involving the rostral pons and
caudal mesencephalon which are sites for these two nuclei. In fact, depression was
the cardinal psychopathological symptom in our patients with brainstem stroke.
Accordingly, our results seemed to be accordance with the hypothesis of the
dysfunction of the biogenic amine system. In addition, somatization,
obsessive-compulsive symptoms, and anxiety were also evident in these patients.
In line with this hypothesis and on the basis of neuroanatomical evidences and
clinical findings, Robinson and his co-workers (1984) also claimed that poststroke
depression might be as a result of depletion of norepinephrine and/or serotonin due to
evident in the patients with subcortical stroke seemed to substantiate these
researchers’ proposition.
In summary, our preliminary results seemed to implicate that a slight to mild
impairment of emotional status was evident in the patients with brainstem stroke, and
depression was the cardinal psychopathological symptom though these were not on
the statistical basis. In addition, otherwise slightly to mildly emotional changes
including somatization, obsessive-compulsive symptom, and anxiety were also
noticed in these patients. Since the available data were limited, the proposed questions
require further investigation.
REFERENCES
Astrom, M., Adolfsson, R., & Asplund, K. (1993). Major depression in stroke patients: A 3-year longitudinal study. Stroke, 24, 976-982.
Beatty, J. (1995). Principles of behavioral neuroscience (pp. 492-495). Chicago, ILL: Brown & Benchmark Publishers.
Beck, A. T. (1987). Beck Depression Inventory. San Antonio, TX: The Psychological Corporation.
Benton, A. L., & Hamsher, K. deS. (1978). Multilingual Aphasia Examination. Iowa City: University of Iowa Hospital, Department of Neurology.
Benton, A. L., Hamsher, K. deS., Varney, N. R., & Spreen, O. (1983). Contributions to neuropsychological assessment: A clinical manual. New York: Oxford
University Press.
Conn, P. M. (1995). Neuroscience in Medicine (pp. 409-417). Philadelphia, PA: J. B. Lippincott Company.
Derogatis, L. R. (1977). SCL.90-R (revised) version manual-I. Baltimore: Clinical Psychometrics Research Unit, Johns Hopkins University School of Medicine.
Hamsher, K. deS. (1983). Standard Neurobehavioral Interview Inventory. Milwaukee: Univerisity of Wisconsin Medical School, Department of Neurology.
Hamsher, K. deS. (1983). Orientation to Personal Information and Place. Milwaukee: Univerisity of Wisconsin Medical School, Department of Neurology.
Heilman, K. M., & Valenstein, E. (Eds.). (1995) Clinical neuropsychology (3rd ed.). New York: Oxford University Press.
Hosking, S. G., Marsh, N. V., & Friedman, P. J. (1996). Poststroke depression: Prevalence, course and associated factors. Neuropsychology Review, 6, 107-133.
House, A., Dennis, M., Mogridge, L., Warlow, C., Hawton., & Jones, L. (1991). Mood disorders in the year after first stroke. British Journal of Psychiatry, 158,83-92.
Huang, Z.-S., Chiang, T.-L., & Lee, T.-K. (1997). Stroke prevalence in Taiwan: Finding from the 1994 National Health Interview Survey. Stroke, 28, 1579-1584.
Ingram, R. E., Kendall, R. C., Smith, T. W., Donnell, C., & Ronan, K. (1987). Cognitive specificity in emotional distress. Journal of Personality and Social Psychology, 53,734-742.
Lang, J. (1991). Clinical anatomy of the posterior cranial fossa and its formina. New York: Thieme Medical.
Levin, H. S., High, W. M. Goethe, K. E., et al. (1987). The Neurobehavioral Rating Scale assessment of the behavioral sequelae of head injury by the clinician. Journal of Neurology, Neurosurgery, and Psychiatry, 50, 183-193.
Leazk, M. D. (1995). Neuropsychological assessment (3rd ed.). New York: Oxford University Press.
Mahoney, F., & Barthel, D. (1965). Functional evaluation: The Barthel Index. Mareland State Medical Journal, 14, 61-65.
Morris, P. L. P., Robinson, R. G., & Raphael, B. (1993). Emotional lability after stroke. Australian and New Zealand Journal of Psychiatry, 27, 601-605.
Morrison, J. H., Molliver, M. E., Grzanna, R. (1979). Noradrenergic innervation of the cerebral cortex: Widespread effects of local corticl lesions. Science, 205, 313-316.
Nelson, L. D., Cicchetti, D., Satz, P., Sowa, M., & Mitrushina, M. (1994). Emotional sequelas of stroke: A longitudinal perspective. Journal of Clinical and
Experimental Neuropsychology, 16, 796-806.
2),Ⅱ-12-Ⅱ-13.
Reynolds, C. F. (1992). Treatment of depression in special populations. Journal of Clinical Psychiatry, 53,45-53.
Robinson, R. G., Boston, J. D., Starkstein, S. E., et al.(1988). Comparison of mania with depression following brain injury: Causal factors. American Journal of Psychiatry, 145, 172-178.
Robinson, R. G., Kunbos, K. L., Starr, L. B., et al. (1984). Mood disorders in stroke patients: Importance of location of lesion. Brain, 107, 81-93.
Robinson, R. G., & Starkstein, S. E. (1997). Neuropsychiatric aspects of cerebrovascular disorders. In S. C. Yudofsky & R. E. Hales (Eds.), The
American Psychiatric Press Textbook of Neuropsychiatry (3rd ed.). Washington, DC: American Psychiatric Press, Inc.
Seibert, P. S., & Ellis, H. C. (1991). Irrelevant thoughts, emotional mood states, and cognitive task performance. Memory and Cognition, 19, 507-513.
Speedie, L., O’onnell, W., Rabins, P. Pearlson, G., Poggi, M., & Gonzalez Rothi, L. (1990). Language prefortmance deficits in elderly drpressed patients.
Aphasiology, 4, 197-205.
Spencer, K. A., Tompkins, C.A., & Schulz, R. (1997). Assessment of depression in patients with brain pathology: The case of stroke. Psychological Bulletin , 122, 132-152.
Spreen, O., & Benton, A. L. (1969). Neurosensory Center Comprehensive Examination for Aphasia. Victoria, BC: Neuropsychological Laboratory, Department of Psychology, University of Victoria.
Starkstein, S. E., Cohen, B.S., Fedoroff, P., Parikh, R. M., Price T. R., & Robinson, R.G. (1990). Relationship between anxiety disorders and depressive disorders in patients with cerebrovascular injury. Archives of General Psychiatry , 47, 246-251.
Starkstein, S. E., Fedoroff, J. P., Berthier, M. L., et al. (1991). Manic depressive and pure manic states after brain lesions. Biological Psychiatry, 29, 149-158.
Starkstein, S. E., Fedoroff, J. P., Price, T. R., et al (1993a). Apathy following cerebrovascular lesions. Stroke, 24, 1625-1630.
Starkstein, S. E., Fedoroff, J. P., Price, T. R., et al. (1993b). Catastrophic reaction after cerebrovascular lesion: Frequency, correlates, and validation of a scale. Journal of Neurlogy, Neurosurgery and Psychiatry, 57, 189-194.
Starkstein, S. E., Robinson, R. G., Berthier, M. L., & Price, T. R. (1988). Depressive disorders following posterior circulation as compared with middle cerebral artery infarcts. Brain, 111, 375-387.
Trimble, M. R., & Cummings, J. L. (1981). Neuropsychiatric disturbances following brainstem lesions. British Journal of Psychiatry, 138,56-69.
Walsh, K. (1994). Neuropsychology: A clinical approach. New York: Chruchill Livingstone.
Table 1. Demograpnic Characteristics of Subject Groups
Sex Age Edu TO OPIP ON AC
F : M Mean SD Range Mean SD Range Mean SD Range Mean SD Range Mean SD Range Mean SD Range Brain stem stroke 6 6 62.08 9.57 42~77 3.75 4.88 0~12 1.08 1.62 0~5 11.50 1.24 8~12 15.58 1.44 11~16 14.83 3.74 8~18
R cortical 5 3 55.63 11.93 40~65 6.88 3.83 0~12 1.25 1.28 0~3 10.25 2.25 6~12 15.75 0.71 14~16 14.75 3.11 10~18 R subcortical 4 5 70.11 5.86 61~80 4.67 5.72 0~14 1.56 1.67 0~4 10.56 1.24 9~12 15.44 1.13 13~16 15.44 3.81 6~18
L cortical 0 3 68.67 15.63 52~83 6 6 0~12 2 2 0~4 6.67 6.11 0~12 16 0 16 12.33 6.03 6~18 L subcortical 2 3 67.60 6.19 61~76 2 2.83 0~6 2.40 1.95 0~5 11 0.71 10~12 15.60 0.89 14~16 14.20 3.11 11~18
健診 7 11 68.78 5.95 60~82 4.33 4.24 0~15 0.22 0.55 0~2 12 0 12 16 0 16 18 0 18
Table 2. Performance Scores of the BDI
P F
BDI
Mean SD Range Mean SD RangeBrain stem stroke 16.30 16.1 1~45 11.8 11.4 0~43 R cortical 5.75 5.65 1~16 6.29 2.50 4~11 R subcortical 7.33 7.62 1~24 7.67 6.58 1~21 L cortical 2.33 2.08 0~4 2.67 2.52 0~5 L subcortical 9.80 6.98 1~20 7.00 7.04 2~19
Table 3. Patient’s and Patient’s Significant Informant’s Rating Scores on the SCL-90-R
Brain stem stroke R cortical R subcortical L cortical L subcortical 健診
SCL P F P F P F P F P F P F Mean 0.94 0.87 0.65 0.49 0.56 0.41 0.23 0.37 0.90 0.86 0.42 0.37 SD 0.68 0.64 0.27 0.25 0.44 0.26 0.12 0.31 0.32 0.56 0.52 0.46 Somatization Range 0.2~2.8 0.3~2.3 0.3~1.1 0.1~0.8 0.1~1.3 0~0.8 0.1~0.3 0.1~0.7 0.6~1.4 0.3~1.8 0~2.1 0~1.9 Mean 0.66 0.54 0.44 0.45 0.59 0.46 0.27 0.43 0.40 0.48 0.21 0.16 SD 0.63 0.49 0.36 0.27 0.56 0.51 0.25 0.23 0.29 0.51 0.32 0.26 Obsessive-Compulsive Range 0.1~2 0~1.3 0.1~1.1 0.2~0.9 0~1.6 0~1.5 0~0.5 0.3~0.7 0~0.7 0~1.3 0~1.1 0~1 Mean 0.33 0.23 0.10 0.09 0.07 0.13 0 0.07 0.12 0.36 0.06 0.05 SD 0.66 0.26 0.24 0.10 0.11 0.21 0 0.12 0.08 0.48 0.19 0.11 Interpersonal Sensitivity Range 0~2 0~0.6 0~0.7 0~0.3 0~0.3 0~0.6 0 0~0.2 0~0.2 0~1.2 0~0.8 0~0.4 Mean 0.70 0.60 0.41 0.26 0.52 0.54 0.13 0.13 0.48 0.58 0.18 0.12 SD 0.93 0.52 0.59 0.15 0.63 0.54 0.06 0.06 0.58 0.73 0.26 0.24 Depression Range 0.1~2.9 0~1.5 0~1.8 0~0.5 0~1.9 0~1.6 0.1~0.2 0.1~0.2 0~1.4 0~1.8 0~0.8 0~1 Mean 0.58 0.53 0.39 0.16 0.29 0.23 0.03 0.17 0.28 0.32 0.16 0.12 SD 0.95 0.51 0.74 0.17 0.45 0.28 0.06 0.06 0.48 0.45 0.21 0.20 Anxiety Range 0~3 0~1.5 0~2.2 0~0.5 0~1.3 0~0.9 0~0.1 0.1~0.2 0~1.1 0~1.1 0~0.6 0~0.7 Mean 0.33 0.50 0.10 0.28 0.16 0.34 0.07 0.10 0.28 0.54 0.15 0.17 SD 0.36 0.43 0.19 0.24 0.15 0.44 0.12 0.17 0.31 0.68 0.27 0.25 Hostility Range 0~1 0~1.2 0~0.5 0~0.7 0~0.3 0~1.3 0~0.2 0~0.3 0~0.7 0~1.5 0~1 0~0.7 Mean 0.38 0.18 0.24 0.11 0.17 0.27 0 0 0.22 0.18 0.01 0.02 SD 0.86 0.29 0.56 0.20 0.36 0.45 0 0 0.44 0.40 0.03 0.07 Phobic Anxiety Range 0~2.7 0~0.9 0~1.6 0~0.6 0~1.1 0~1.3 0 0 0~1 0~0.9 0~0.1 0~0.3 Mean 0.19 0.28 0.21 0.25 0.02 0.19 0 0.17 0.04 0.42 0.06 0.05 SD 0.37 0.28 0.36 0.29 0.07 0.26 0 0.29 0.09 0.52 0.18 0.10 Parachnoid Ideation Range 0~1.3 0~0.8 0~1 0~0.7 0~0.2 0~0.7 0 0~0.5 0~0.2 0~1.2 0~0.7 0~0.3 Mean 0.33 0.23 0.04 0.08 0.01 0.21 0 0 0.04 0.24 0.02 0.03 SD 0.53 0.26 0.07 0.09 0.03 0.31 0 0 0.05 0.38 0.04 0.08 Psychoticism Range 0~1.6 0~0.7 0~0.2 0~0.2 0~0.1 0~0.9 0 0 0~0.1 0~0.9 0~0.1 0~0.3 Mean 0.55 0.47 0.34 0.25 0.30 0.32 0.10 0.20 0.38 0.46 0.15 0.13 SD 0.64 0.37 0.33 0.11 0.28 0.32 0.10 0.10 0.30 0.48 0.21 0.20 Global Severity Index
Range 0.1~1.9 0.1~1.1 0.1~1.1 0.1~0.4 0~0.9 0~1 0~0.2 0.1~0.3 0.2~0.9 0.1~1.3 0~0.7 0~0.8 Mean 1.65 1.47 1.56 1.19 1.71 1.70 1.10 1.30 1.72 1.58 1.38 1.39 SD 0.50 0.27 0.40 0.20 0.34 0.90 0.10 0.44 0.31 0.33 0.37 0.46 Positive Symptom Distress Index Range 1.1~2.7 1~1.8 1.2~2.4 1~1.6 1.3~2.2 1.1~4 1~1.2 1~1.8 1.4~2.1 1.2~1.9 1~2.2 1~2.2 Mean 25.91 28.25 17.60 19.40 14.90 19.20 9.33 13.00 18.60 24.60 9.12 8.61 SD 21.82 18.86 12.06 7.65 11.60 16.40 6.03 5.00 12.28 22.88 9.27 11.4 Total