Increased risk of adverse pregnancy outcomes for women with
migraines: a nationwide population-based study
ceph_1935 1..7H-M Chen1,2, S-F Chen2, Y-H Chen3& H-C Lin2
1Department of Internal Medicine, PoJen General Hospital,2School of Health Care Administration and3School of Public Health, Taipei
Medical University, Taipei, Taiwan
Chen H-M, Chen S-F, Chen Y-H & Lin H-C. Increased risk of adverse pregnancy outcomes for women with migraines: a nationwide population-based study. Cephalalgia 2009. London. ISSN 0333-1024
Using a 3-year nationwide population-based database, this study aims to examine the risk of adverse pregnancy outcomes in women with migraines, including low birthweight (LBW), preterm birth, infants born small for gesta-tional age, Caesarean section (CS) and pre-eclampsia. We identified a total of 4911 women with migraines who gave birth from 2001 to 2003, together with 24 555 matched women as a comparison cohort. Multivariate logistic regression analyses showed that after adjusting for potential confounders, the odds ratios were 1.16 [95% confidence intervals (CI) = 1.03–1.31, P = 0.014] for LBW, 1.24 (95% CI = 1.13–1.39, P< 0.001) for preterm births, 1.16 (95% CI = 1.07–1.24,
P< 0.001) for CS and 1.34 (95% CI = 1.02–1.77, P = 0.027) for pre-eclampsia for
women with migraines compared with unaffected mothers. We conclude that women with migraines were at increased risk of having LBW, preterm babies, pre-eclampsia and delivery by CS, compared with unaffected mothers. 䊐Migraine, pregnancy complications, preterm birth, pre-eclampsia
Herng-Ching Lin, School of Health Care Administration, Taipei Medical University, 250 Wu-Hsing Street, Taipei 110, Taiwan. Tel. 886 22736 1661 ext. 3613, fax 886 22378 9788, e-mail [email protected] Received 12 January 2009, accepted 4 May 2009
Introduction
Migraine, a common chronic-intermittent neuro-vascular disorder, strongly predominates in adult females (1) and affects almost a quarter of all women during their childbearing years (2, 3). It often improves during pregnancy, but sometimes occurs then for the first time, and may be worse during the first trimester (4–6). There has long been concern about the relationship between migraine and pregnancy. Some reviews have concluded that although a history of migraines may increase the risk of pre-eclampsia, it has no adverse effect on the outcome of pregnancy (7–9). However, this conclu-sion is based on relatively few studies, most with inadequate sample size.
As far as we know, to date there are only two studies of pregnancy outcomes in pregnant women
with migraines. A Hungarian study reported that severe maternal migraines may increase the occur-rence of pre-eclampsia and severe nausea/vomiting during pregnancy (10), but they are not associated with unfavourable delivery outcomes. Another study by Wainscott et al. was carried out at the Princess Margaret Migraine Clinic, London, between May 1973 and June 1974. Similarly, they did not find any significant difference in pregnancy outcomes when comparing 450 women with migraines and 136 women without (11). However, both studies used survey research to collect the data, a technique that can result in recall bias. In addition, the small sample size used in both studies may fail to detect differences between women with migraines and the normal population.
Therefore, this study aims to examine the risk of adverse pregnancy outcomes in pregnant women
with migraines, using a 3-year nationwide population-based database, taking the characteris-tics of infant, mother and father into consideration. Taiwan initiated a National Health Insurance (NHI) programme in 1995. Its nationwide population-based dataset allows us to trace all medical services used by all enrollees. The database provides a unique opportunity to use unselected national data to determine whether migraines are associated with an increased risk of adverse pregnancy outcomes, including low birthweight (LBW), preterm births, babies small for gestational age (SGA), Caesarean section (CS) and pre-eclampsia.
Methods
Database
We used two nationwide population-based datasets in this study. The first was the National Health Insurance Research Dataset (NHIRD) covering the years 1996–2003. Taiwan inaugurated the NHI programme in March 1995, and Taiwan’s NHI programme, a single-payer system with the govern-ment as the sole insurer, provides universal coverage, comprehensive benefits and access to any medical institution of the patient’s choice. The NHIRD includes a registry and all medical claims data for over 22 million enrollees, representing over 98% of the island’s population. The NHIRD is one of the largest and most comprehensive nationwide population-based datasets currently available in the world.
The second dataset was drawn from the 2001– 2003 Taiwan birth certificate registry published by the Ministry of Interior in Taiwan. Birth certificates include data on birthdates for both infants and their parents, gestational week at birth, infant birth-weight, gender, parity, place of birth, parents’ educational levels, and maternal marital status. Registration of all births is mandatory in Taiwan, so the birth certificate data are very accurate and comprehensive. One study by Lin et al. has verified the completeness and validity of Taiwan’s birth registry (12).
With assistance from the Bureau of NHI in Taiwan, the mothers’ and infants’ unique personal identifi-cation numbers provided links between the NHIRD and birth certificate data. All personal identifiers were encrypted by the NHI before release to the researchers. Confidentiality assurances were addressed by abiding by NHI data regulations. Because the NHIRD consists of de-identified
secondary data released to the public for research purposes, this study was exempt from full review by the Internal Review Board.
Study sample
This study included 473 529 pregnant women with singleton live births in Taiwan between 1 January 2001 and 31 December 2003. Of these women, 16 042 had visited ambulatory care centres for treat-ment of migraines (ICD-9-CM code 346) within 2 years prior to index delivery. We selected only patients who had at least three consensus migraine diagnoses, because coding validity is often disputed for administrative databases. As psychiatric comor-bidity has long been noted in association with migraine (13), patients with mental illnesses were not excluded, in order to have a more representa-tive population of migraineurs. Ultimately, 4911 women with migraines were included in the study cohort.
The comparison cohort was selected from the remaining 457 487 mothers. We excluded those who had been diagnosed with certain chronic diseases (such as systemic lupus erythematosis, rheumatoid arthritis, gout, sarcoidosis or ankylosing spondyli-tis), but we did include those with hypertension (ICD-9-CM code 401.XX~405.XX, 642.0X~642.3X, 642.9X, 760.00), diabetes (ICD-9-CM code 648.0X, 250.XX), hyperlipidaemia (ICD-9-CM code 272.X), and coronary heart disease (CHD, ICD-9-CM code 410.XX~414.XX, 429.2). We randomly extracted 24 555 mothers (five for every one with migraines) matched with the study group in terms of age (<20, 20–24, 25–29, 30–34 and ⱖ35 years), the year of delivery, hypertension, diabetes, hyperlipidaemia and CHD as our comparison cohort.
Variables of interest
In this study, outcome variables were all dichoto-mous, including LBW (<2500 g), preterm gestation (<37 weeks), babies SGA (birthweight below the tenth percentile for gestational age), CS delivery vs. vaginal delivery and pre-eclampsia. The indepen-dent variable of interest was whether a woman had been diagnosed with migraines or not.
Potential confounding factors were adjusted for, including characteristics of the mother (age, highest educational level and marital status), father (age and highest educational level), infant (gender and parity) and family monthly income. Parental age was defined as each parent’s age, in years, at the time of the infant’s birth. Parity was grouped into
the following categories: 1, 2, ⱖ3. Maternal and paternal highest education levels were categorized into four levels: elementary school or lower, junior high school, senior high school, college or above. Family monthly income was grouped into four categories: <NT$15 000, NT15 000–NT30 000, NT30 001–NT50 000, ⱖNT50 001.
Statistical analysis
The SAS statistical package (SAS System for Windows, Version 8.2) was used to perform the analyses. The c 2 tests were carried out to examine
differences in the characteristics of infant, mother and father for women with migraines and unaf-fected women. Conditional logistic regression analyses, which were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyper-lipidaemia and CHD, were then used to investigate the risk of LBW, preterm gestation, SGA, CS and pre-eclampsia for mothers with and without migraines, after adjusting for potential confounders. Adjusted odds ratios (OR) are presented with 95% confidence intervals (CI). A two-sided P-value of <0.05 was considered statistically significant for this study.
Results
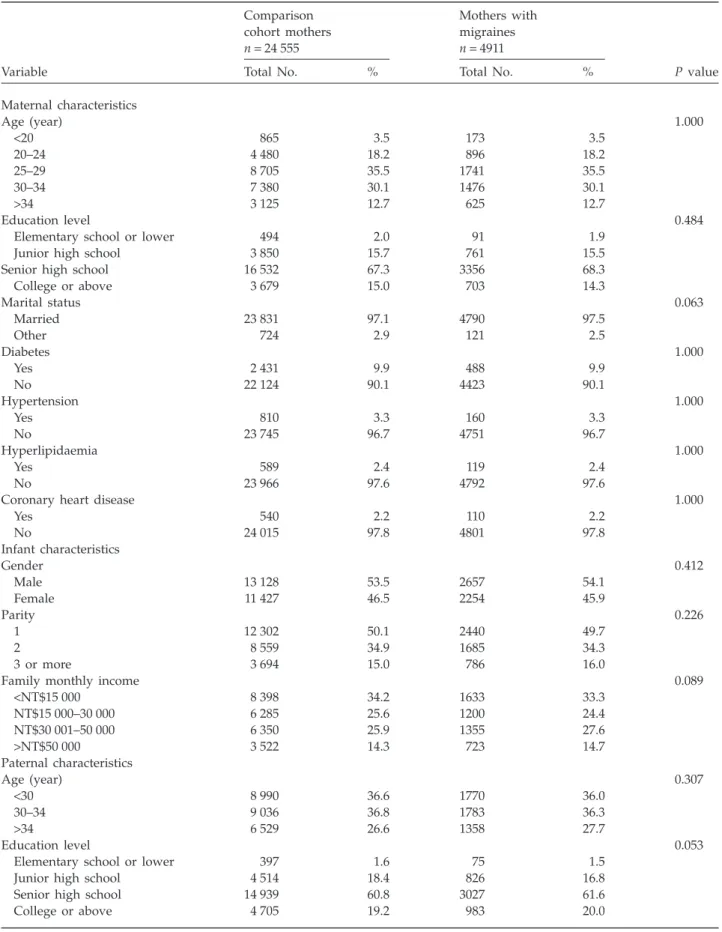
Table 1 illustrates the distribution of characteristics of mothers, infants and fathers, comparing mothers who did and did not have migraines. The mean age of the sampled patients was 28.2 years (standard deviation = 5.2 years) and the majority had finished senior high school. A total of 9.9%, 3.3%, 2.4% and 2.2% experienced diabetes, hypertension, hyperlipi-daemia and CHD, respectively. Pearson c2 tests
show that there was no significant difference between these two cohorts in terms of characteris-tics of mothers, infants and fathers.
Table 2 describes the distributions of LBW, preterm birth, SGA infants, CS and pre-eclampsia between the cohorts. It shows that there were significant differences between mothers with migraines and unaffected mothers in the incidence of LBW (7.5% vs. 6.6%, P = 0.019), preterm birth (9.4% vs. 7.7%, P< 0.001), CS (39.5%% vs. 36.0%,
P< 0.001) and pre-eclampsia (1.4% vs. 1.1%, P = 0.028). However, no significant differences were
observed between the two cohorts in terms of SGA infants (P = 0.125).
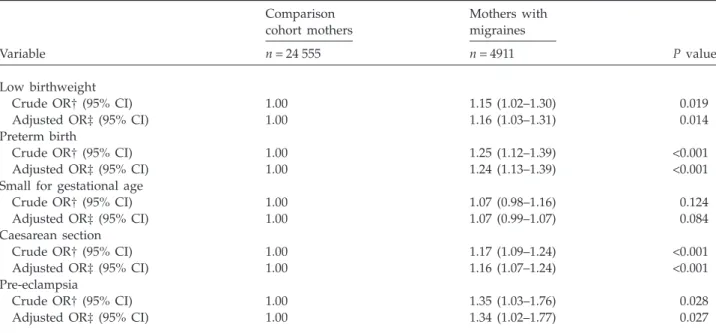
Table 3 describes the crude and adjusted ORs of LBW, preterm birth, SGA infants, CS and pre-eclampsia associated with migraines. After
adjusting for infants’ gender, parity, maternal age, highest maternal education level, parental age dif-ference, mothers’ marital status and family monthly income, as well as hypertension, diabetes, hyper-lipidaemia and coronary heart disease, the ORs were 1.16 (95% CI = 1.03–1.31, P = 0.014) for LBW, 1.24 (95% CI = 1.13–1.39, P< 0.001) for preterm births, 1.16 (95% CI = 1.07–1.24, P< 0.001) for CS and 1.34 (95% CI = 1.02–1.77, P = 0.027) for pre-eclampsia for women with migraines compared with unaffected mothers.
Discussion
This nationwide population-based study clearly demonstrated that maternal migraines were inde-pendently associated with a 1.16- and 1.24-fold increased risk of having LBW and preterm babies, respectively, after adjusting for family income and maternal, paternal and infant characteristics. Women with migraines were also more likely to experience pre-eclampsia and CS, compared with unaffected women.
Our findings are consistent with 9 of 11 published studies conducted in different regions that have documented a positive association between migraines and pre-eclampsia (14). However, most previous methodologically rigorous studies were conducted among North American, Latin American and European women (15–18). This is the first study to evaluate the association between migraines and pre-eclampsia risk among East Asian women. Our findings add to the evidence supporting increased pre-eclampsia risk for women with a history of migraines and also extend the literature to include an East Asian population.
In addition, as far as we know, our study is the first to identify increased risk of LBW, preterm birth babies and CS among mothers with migraines. Although some studies have reported no increased incidence of poor pregnancy outcomes among women with migraines (10, 11), these studies suffer from several limitations that could undermine the strength of their findings. For example, one recent population-based study compared outcomes for 38 151 newborns, 713 of them born to women with severe migraines during pregnancy (10). They found maternal migraines may increase the occur-rence of pre-eclampsia during pregnancy, but are not associated with unfavourable delivery out-comes. Although they used the dataset of newborn infants from the Hungarian Case–Control Surveil-lance System of Congenital Abnormalities, the maternal information was mainly obtained from
Table 1 Comparisons of pregnant women with and without migraines in relation to maternal, paternal and infant characteristics in Taiwan, 2001–2003 (n = 29 466) Variable Comparison cohort mothers n = 24 555 Mothers with migraines n = 4911 P value
Total No. % Total No. %
Maternal characteristics Age (year) 1.000 <20 865 3.5 173 3.5 20–24 4 480 18.2 896 18.2 25–29 8 705 35.5 1741 35.5 30–34 7 380 30.1 1476 30.1 >34 3 125 12.7 625 12.7 Education level 0.484
Elementary school or lower 494 2.0 91 1.9
Junior high school 3 850 15.7 761 15.5
Senior high school 16 532 67.3 3356 68.3
College or above 3 679 15.0 703 14.3 Marital status 0.063 Married 23 831 97.1 4790 97.5 Other 724 2.9 121 2.5 Diabetes 1.000 Yes 2 431 9.9 488 9.9 No 22 124 90.1 4423 90.1 Hypertension 1.000 Yes 810 3.3 160 3.3 No 23 745 96.7 4751 96.7 Hyperlipidaemia 1.000 Yes 589 2.4 119 2.4 No 23 966 97.6 4792 97.6
Coronary heart disease 1.000
Yes 540 2.2 110 2.2 No 24 015 97.8 4801 97.8 Infant characteristics Gender 0.412 Male 13 128 53.5 2657 54.1 Female 11 427 46.5 2254 45.9 Parity 0.226 1 12 302 50.1 2440 49.7 2 8 559 34.9 1685 34.3 3 or more 3 694 15.0 786 16.0
Family monthly income 0.089
<NT$15 000 8 398 34.2 1633 33.3 NT$15 000–30 000 6 285 25.6 1200 24.4 NT$30 001–50 000 6 350 25.9 1355 27.6 >NT$50 000 3 522 14.3 723 14.7 Paternal characteristics Age (year) 0.307 <30 8 990 36.6 1770 36.0 30–34 9 036 36.8 1783 36.3 >34 6 529 26.6 1358 27.7 Education level 0.053
Elementary school or lower 397 1.6 75 1.5
Junior high school 4 514 18.4 826 16.8
Senior high school 14 939 60.8 3027 61.6
Table 2 The distribution of LBW, preterm birth, SGA, CS and pre-eclampsia for mothers with migraines and unaffected mothers, 2001–2003 (n = 29 466) Variable Comparison cohort mothers n = 24 555 Mothers with migraines n = 4911 P value No. % No. % Low birthweight 0.019 Yes 1 610 6.6 367 7.5 No 22 945 93.4 4544 92.5 Preterm birth <0.001 Yes 1 884 7.7 462 9.4 No 22 671 92.3 4449 90.1
Small for gestational age 0.125
Yes 4 114 16.8 867 17.7 No 20 441 83.3 4044 82.4 Cesarean section <0.001 Yes 8 842 36.0 1940 39.5 No 15 713 64.0 2971 60.5 Pre-eclampsia 0.028 Yes 261 1.1 70 1.4 No. 24 294 98.9 4841 98.6
CS, Caesarean section; LBW, low birthweight; SGA, small for gestational age.
Table 3 Crude and adjusted odds ratios (OR) for LBW, preterm birth, SGA, CS and pre-eclampsia among women with
and without migraines during pregnancy, 2001–2003 (n = 29 466)
Variable Comparison cohort mothers Mothers with migraines P value n = 24 555 n = 4911 Low birthweight
Crude OR† (95% CI) 1.00 1.15 (1.02–1.30) 0.019
Adjusted OR‡ (95% CI) 1.00 1.16 (1.03–1.31) 0.014
Preterm birth
Crude OR† (95% CI) 1.00 1.25 (1.12–1.39) <0.001
Adjusted OR‡ (95% CI) 1.00 1.24 (1.13–1.39) <0.001
Small for gestational age
Crude OR† (95% CI) 1.00 1.07 (0.98–1.16) 0.124
Adjusted OR‡ (95% CI) 1.00 1.07 (0.99–1.07) 0.084
Caesarean section
Crude OR† (95% CI) 1.00 1.17 (1.09–1.24) <0.001
Adjusted OR‡ (95% CI) 1.00 1.16 (1.07–1.24) <0.001
Pre-eclampsia
Crude OR† (95% CI) 1.00 1.35 (1.03–1.76) 0.028
Adjusted OR‡ (95% CI) 1.00 1.34 (1.02–1.77) 0.027
*Indicates P< 0.05; ***indicates P < 0.001.
†Crude ORs were calculated using conditional logistic regressions that were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyperlipidaemia and coronary heart disease.
‡Adjusted ORs were calculated by using conditional logistic regressions that were conditioned on maternal age, the year of delivery, hypertension, diabetes, hyperlipidemia and coronary heart disease and adjusted for infant’s gender, parity, highest maternal education level, parental age difference, mothers’ marital status and family monthly income.
prenatal care logbooks and a structured question-naire. Only 68% of migraines were recorded medi-cally in the prenatal logbooks, while the rest were based on patient self-reports. Potential recall bias suggests underestimation of migraines, which clearly undermines the strength of their findings.
Similarly, in 1978, Wainscott and Volans carried out a retrospective survey at the Princess Margaret Migraine Clinic, London, UK (11). They examined pregnancy outcomes for 450 women with migraines compared with 136 controls, and found the inci-dence of miscarriage, toxaemia, congenital anoma-lies and stillbirth was not increased among the migraine sufferers compared with the national aver-ages or the controls. However, selection bias is a possible problem with this study, because the control participation rate was much lower than the case participation rate. In addition, many studies investigating populations with migraines have been limited to small clinical samples and did not use currently accepted diagnostic criteria for migraines and pre-eclampsia; consequently there were signifi-cant methodological shortcomings.
Because the extent to which migraines affect pregnancies is not well established, this report uses a comprehensive dataset in Taiwan that provides a unique opportunity to evaluate the association between migraines and adverse pregnancy out-comes. Similar to those of previous investigations, our results further confirmed the relation between migraines and pre-eclampsia (15–18). However, unlike previous studies (10, 11), our study identi-fied increased risk of preterm delivery and LBW among women with migraines. The mechanisms by which migraines produce adverse pregnancy out-comes are complex and heterogeneous. Unfavour-able foetal outcomes may relate to antiphospholipid antibodies (aPL) (19), channelopathic vasculopathy (20), and use of triptan medications (21). Further, triptans are agonists at the 5-HT1B/1D receptors that cause vasoconstriction and neuronal inhibition and they are frequently prescribed to treat acute attacks of migraine. Exposure to these drugs during pregnancy has been associated with an increased risk of preterm delivery and LBW (22).
This study has several noteworthy strengths. First, the very large sample size used provides ample statistical power to detect differences in risk of adverse birth outcomes between pregnant women with and without migraines. To the best of our knowledge, this is the most complete nation-wide population-based study ever conducted to assess the risk of adverse pregnancy outcomes
among women diagnosed with migraines. Further-more, linking the NHIRD with the national birth registry leaves little room for selection and non-response bias and its robust findings can be gener-alized to the population as a whole. We have also incorporated increasing concern about the effects of paternal characteristics on adverse birth outcomes that may be independent of maternal effects into the study design (23). Lastly, factors such as hyper-tension, diabetes, hyperlipidaemia and CHD might adversely affect maternal pregnancy outcomes. Risks of cardiovascular illnesses and CHD were also associated with patients with migraine (24–26). In our study, the study and comparison cohorts were matched in terms of these conditions to better evaluate independent effects of migraine on preg-nancy outcomes. Future studies need to differenti-ate the impact of migraine from other significant factors affecting birth outcomes.
Despite the above strengths, findings should be interpreted with caution due to the following limi-tations. First, because we identify mothers diag-nosed with migraines by the ICD-9-CM code from the NHIRD released by the Bureau of the NHI, the sample may not accurately represent the population with migraine. Second, the validity of the migraine diagnoses could be a concern. Due to the use of a claims dataset, whether the coded migraine actually represented patients with migraine headache and whether that control did not have migraine could not be independently verified. For a variety of reasons, women may be misclassified. However, in Taiwan, the diagnosis of migraine in clinical set-tings is generally based upon the International Headache Society criteria (27). Further, the NHI Bureau routinely cross-checks a sample of claims from each hospital and clinic with its medical charts. It is generally believed that the NHI’s cross-checks foster accurate coding. Third, with this large sample in our study, overpower might be a concern, for even small differences could be statistically sig-nificant. Indeed, some estimates in our study were small with confidence limits close to one. These results should be interpreted cautiously in terms of the meaningfulness or the clinical significance. Lastly, because the NHIRD does not include com-plete information regarding medications taken during pregnancy, it is not possible for us to assess the confounding role of medications in the relation-ship between migraines and adverse birth out-comes. However, in Taiwan, most women with migraines are reluctant to take medications during pregnancy due to concerns about adverse con-sequences for the developing foetus. Thus, the
association between migraines and birth outcomes found in our study was largely based on women not receiving migraine treatment during pregnancy. Although previous studies have concluded that migraines have no adverse effect on pregnancy outcomes, this study used a large, unselected national dataset to demonstrate that women with migraines were at increased risk for having LBW and preterm babies, and for delivery by CS, com-pared with unaffected mothers. In addition, our results, combined with reports by others, suggest that the risk of pre-eclampsia is increased in women who have a history of migraines. We suggest that clinicians should make women with migraines aware of potential risks before planning a child, coupled with more intensive monitoring and pre-natal care during pregnancy. Future studies are needed to explore the association between adverse birth outcomes and migraine severity, as well as medications taken during pregnancy, to enable more specific interpretation of these findings.
References
1 MacGregor A. Migraine in women. London: Martin Dunitz Ltd, 1999.
2 Lipton RB, Bigal ME. The epidemiology of migraine. Am J Med 2005; 118 (Suppl. 1):S3–S10.
3 Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Head-ache 2001; 41:646–57.
4 Maggioni F, Alessi C, Maggino T, Zanchin G. Headache during pregnancy. Cephalalgia 1997; 17:765–9.
5 Miles CB. Treatment of migraine during pregnancy and lactation. S D J Med 1995; 48:373–7.
6 Silberstein SD. Migraine and pregnancy. Neurol Clin 1997; 15:209–31.
7 Aube M. Migraine in pregnancy. Neurology 1999; 53:S26–8.
8 Matharu MS, Levy MJ, Goadsby PJ. Understanding migraine in women. Practitioner 2002; 246:272–8. 9 Menon R, Bushnell CD. Headache and pregnancy.
Neu-rologist 2008; 14:108–19.
10 Banhidy F, Acs N, Horvath-Puho E, Czeizel AE. Preg-nancy complications and delivery outcomes in pregnant women with severe migraine. Eur J Obstet Gynecol Reprod Biol 2007; 134:157–63.
11 Wainscott G, Sullivan FM, Volans GN, Wilkinson M. The outcome of pregnancy in women suffering from migraine. Postgrad Med J 1978; 54:98–102.
12 Lin CM, Lee PC, Teng SW, Lu TH, Mao IF, Li CY. Validation of the Taiwan Birth Registry using obstetric records. J Formos Med Assoc 2004; 103:297–301.
13 Radat F, Swendsen J. Psychiatric comorbidity in migraine: a review. Cephalalgia 2005; 25:165–78. 14 Allais G, Castagnoli Gabellari I, Airola G, Schiapparelli P,
Terzi MG, Mana O, Benedetto C. Is migraine a risk factor in pregnancy? Neurol Sci 2007; 28 (Suppl. 2):S184–7. 15 Adeney KL, Williams MA, Miller RS, Frederick IO,
Sorensen TK, Luthy DA. Risk of preeclampsia in relation to maternal history of migraine headaches. J Matern Fetal Neonatal Med 2005; 18:167–72.
16 Facchinetti F, Allais G, D’Amico R, Benedetto C, Volpe A. The relationship between headache and preeclampsia: a case-control study. Eur J Obstet Gynecol Reprod Biol 2005; 121:143–8.
17 Marcoux S, Berube S, Brisson J, Fabia J. History of migraine and risk of pregnancy-induced hypertension. Epidemiology 1992; 3:53–6.
18 Sanchez SE, Qiu C, Williams MA, Lam N, Sorensen TK. Headaches and migraines are associated with an increased risk of preeclampsia in Peruvian women. Am J Hypertens 2008; 21:360–4.
19 Spegiorin LC, Galao EA, De Godoy JM, Bagarelli LB, Oliani AH. Antiphospholipid antibodies and growth retardation in intrauterine development. Prague Med Rep 2007; 108:185–90.
20 Clark CA, Spitzer KA, Crowther MA, Nadler JN, Laskin MD, Waks JA, Laskin CA. Incidence of postpartum thrombosis and preterm delivery in women with antiphospholipid antibodies and recurrent pregnancy loss. J Rheumatol 2007; 34:992–6.
21 Garcia-Carrasco M, Galarza C, Gomez-Ponce M, Cervera R, Rojas-Rodriguez J, Espinosa G et al. Antiphospholipid syndrome in Latin American patients: clinical and immu-nologic characteristics and comparison with European patients. Lupus 2007; 16:366–73.
22 Olesen C, Steffensen FH, Sorensen HT, Nielsen GL, Olsen J. Pregnancy outcome following prescription for sumatriptan. Headache 2000; 40:20–4.
23 Chen XK, Wen SW, Krewski D, Fleming N, Yang Q, Walker MC. Paternal age and adverse birth outcomes: teenager or 40+, who is at risk? Hum Reprod 2008; 23:1290–6.
24 Kurth T, Gaziano J, Cook N, Logroscino G, Diener HC, Buring J. Migraine and risk of cardiovascular disease in women. JAMA 2006; 296:283–91.
25 Kurth T, Schurks M, Logroscino G, Gaziano J, Buring J. Migraine, vascular risk, and cardiovascular events in women: prospective cohort study. BMJ 2008; 337:a636. 26 Woodward M. Migraine and the risk of coronary heart
disease and ischemic stroke in women. Womens Health 2009; 5:69–77.
27 Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Headache Classification Committee of the International Headache Society. Cephalalgia 1988; 8 (Suppl. 7):1–96.