Preface
As physicians’ clinical skills cannot be measured solely by written
examination, a National objective structured clinical examination (OSCE)
has been considered necessary as a part of medical licensure examination.
By the end of 2008, about 20 medical centers/ hospitals in Taiwan
announced that OSCE has been a regular clinical examination for their
trainees. However, there is little consensus about how to implement a
high-stake, large scale OSCE.
The Medical Council of Canada (MCC) has administered an OSCE for
the license to practice medicine since 1992. The high stake, large scale
OSCE is to test physicians’ skills of history taking, physical examination,
and communication. The examination results with psychometric evidence
indicate that a full-scale national administration of an OSCE model for
licensure is feasible in Canada.
Professor, Sydney Marla Smee is currently the Manager of MCCQE Part
II, Evaluation Bureau Medical Council of Canada (1990-Present). She is
an internationally recognized expert in implementing a high stake OSCE.
The workshop in Taiwan lead by Dr. Smee is to facilitate the
establishment of a Taiwanese model of high stake OSCE.
Contents
Agenda --- 3
Speaker’s Curriculum Vitae --- 5
Instructor Assistant’s Curriculum Vitae --- 10
Moderator’s Curriculum Vitae --- 12
PowerPoint (Day 1) --- 13
PowerPoint (Day 2) --- 32
Related Articles
The Use of Standardized Patient Assessments for
Certification and Licensure Decisions ---
The Comparison of Physician Examiners and
Trained Assessors in a High-Stakes OSCE Setting ----
Physician Scores on a National Clinical Skills
Examination as Predictors of Complaints to Medical
Regulatory Authorities
--- Participants ---
37
45
49
59
Day1
Agenda
High- Stakes OSCE (I): Administrative Issues and Related Topics
Date: January 7, 2010 (Thursday)
Place:
臺北醫學大學 醫學綜合大樓前棟 4 樓-誠樸廳
台北市信義區 110 吳興街 250 號
Instructor:
Dr. Sydney M. Smee
Instructor Assistant: Dr. Charity T.C. Tsai
Time
Activity
Moderator
08:30-08:45
Registration
08:45-09:00
Opening Remarks
Minister Chaur-Shin Yung 楊朝祥部長
President Wen-Ta Chiu 邱文達校長
Director Chong-Liang Shi 石崇良處長
Prof. Chi-Wan
Lai
賴其萬教授
09:00-09:30
Presentation: Update on Plans for a Taiwan
OSCE
09:30-10:30
Presentation: High Stakes Multi-site OSCE:
Key Processes and Design Issues
10:30-10:45
Break
10:45-12:00
Group Activity: Five Groups- Create an
OSCE Design
12:00-13:00
LUNCH
13:00-14:30
Group Activity: Group Reports & Discussion
14:30-14:45
Break
14:45-15:15
Group Activity: Large Group Exercise-
Examination Day Scheduling
15:15-16:15
Group Activity: Five Groups- Required
Resources - Human and Other
16:15-17:00
Group Activity: Group Reports
Day2
Agenda
High- Stakes OSCE (I): Administrative Issues and Related Topics
Date: January 8, 2010 (Friday)
Place:
臺北醫學大學 醫學綜合大樓前棟 4 樓-誠樸廳
台北市信義區 110 吳興街 250 號
Instructor: Dr. Sydney M. Smee
Instructor Assistant: Dr. Charity T.C. Tsai
Time
Activity
08:30-09:00
Check-in: Questions/Answers
09:00-10:30
Presentation & Exercise: Costing the OSCE
10:30-10:45
Break
10:45-11:15
Presentation: Training Issues- Examiners, SPs and Staff
11:15-12:00
Presentation: Production Timeline-Critical Milestones
12:00-13:00
LUNCH
13:00-14:30
Presentation: Hot Topics: Examiner Qualifications, Incidents,
Re-scores and Appeals
14:30-14:45
Break
14:45-17:00
Wrap-Up - Next Steps
17:00
Closing Remarks 閉幕致詞
Speaker’s Curriculum Vitae
D
D
r
r
.
.
S
S
y
y
d
d
n
n
e
e
y
y
M
M
.
.
S
S
m
m
e
e
e
e
Higher Education
2007
Doctor of Philosophy
University of Ottawa
Major: Education
Minor: Measurement and Evaluation
1994
Master of Education
Ontario Institute of Studies in Education
University of Toronto
Major: Adult Education
1982
Bachelor of Arts
McMaster University
Major: Political Science
Professional Positions
1990-Present
Manager, MCCQE Part II
Evaluation Bureau, Medical Council of Canada
1987 - 1990
Coordinator, Volunteer Services
Casey House Hospice, Toronto
1986-1988
Consultant, Standardized Patient Program Development
University of Massachusetts, University of Toronto, McMaster
University
1984 - 1985
Coordinator, Patient Instructor Program
Editorial Activities
Ad Hoc Reviewer:
Advances in Health Sciences: 2001, 2007
Medical Education: 2001 – 2002, 2005, 2009.
Publications
Boulet, J.R., Smee, S.M., Dillon, G.F., and Gimpel, J.R. (2009).The use of
standardized patient assessments for certification and licensure
decisions. Simulation in Health Care 4:1 Spring.
Smee, SM. (2008). High Stakes OSCE scoring: Station-specific rating scales versus
checklists. Paper presented at the 13
thOttawa Conference on Medical Education:
Melbourne, Australia.
Smee, SM. (2008). Impact of judgmental weights for OSCE checklist items on station
pass marks. Paper presented at the 13
thOttawa Conference on Medical
Education: Melbourne, Australia.
Boursicot, KA, Smee, SM, & Paterson, J. (2008). Ten years of monitoring test
security in graduation level OSCEs. Paper presented at the 13
thOttawa
Conference on Medical Education: Melbourne, Australia.
Wood, TJ & Smee, S. (2008). Does editing an OSCE station after an examination
improve its performance on subsequent examinations? Paper presented at the
2008 annual meeting of the Association of Medical Educators of Europe
(AMEE): Prague, Czech Republic.
Wood, TJ, Smee, SM, Bartman, I, & Blackmore, DE. (2008) Do two different
processes for limiting false positive errors add to the quality of the pass/fail
decision on a high stakes examination? Paper presented to the annual meeting
on Research in Medical Education (RIME): San Antonio, USA.
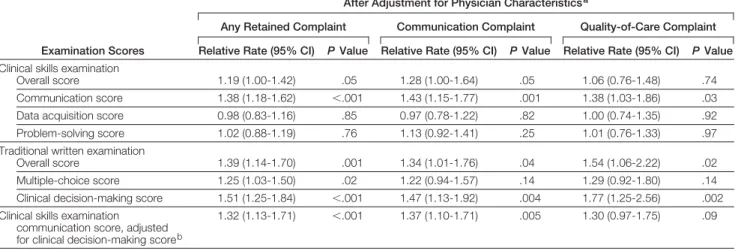
Tamblyn, R, Abrahamowicz, M, Dauphinee, D, Wenghofer, E, Jacques, A, Klass, D,
Smee, S, Blackmore, D, Winslade, N, Girard, N, Du Berger, R, Bartman, I,
Buckeridge, D, & Hanley, J. (2007). Physician Scores on a National Clinical
Skills Examination as Predictors of Complaints to Medical Regulatory
Authorities. Journal of the American Medical Association, 298, 993-1001.
Humphrey-Murto, S, Smee, SM, Touchie, C, Wood, TJ, & Blackmore, DE. (2005). A
comparison of physician examiners and trained assessors in a high-stakes OSCE
setting. Academic Medicine, 80, s59-s62.
Boursicot, KAM & Smee, SM. (2004). Setting standards for a finals Objective
Structured Clinical Examination (OSCE): Comparing the borderline group
method with an Angoff approach. Paper presented at the 10
thOttawa
International Conference on Medical Education, Ottawa, Canada.
Smee, SM. (2003). ABC of learning and teaching in medicine: Skill-based assessment.
British Medical Journal, 326, 703-706.
Smee, SM, Dauphinee, WD, Blackmore, DE, Rothman, AI, Reznick, R, & Des
Marchais, J. (2003). A sequenced OSCE for licensure: Administrative issues,
results and myths. Advances in Health Sciences Education: Theory and Practice,
8, 223-236.
Birtwhistle, R, Blackmore, DE, Smee, SM, & Wood, T. (2002). Does specialty play a
role when physicians are used as examiners in a nationally administered OSCE?
Paper presented at the 9th Ottawa International Conference on Medical
Education Capetown, South Africa.
Blackmore, DE & Smee, SM. (2002). Weighted vs. unweighted OSCE checklists. In
Paper presented at the 9th Ottawa International Conference on Medical
Education Capetown, South Africa.
Smee, SM & Blackmore, DE. (2002). Setting standards for an objective structured
clinical examination: The borderline group method gains ground on Angoff.
Medical Education, 35, 1009-1010.
Smee, SM & Blackmore, DE. (2002). Authors' reply: Setting standards for an
objective structured clinical examination: The borderline group method gains
ground on Angoff. Medical Education, 36, 388-389.
Smee, SM & Blackmore, DE. (2001). Commentary - Setting standards for an
objective structured clinical examination: The borderline group method gains
ground on Angoff. Medical Education, 35, 1009-1010.
Dauphinee, WD, Boulais, AP, Smee, SM, Rothman, AI, Reznick, R, & Blackmore,
DE. (2000). Examination results of the Licentiate of the Medical Council of
Proceedings of the Eighth International Ottawa Conference - Evolving
Assessment: Protecting the Human Dimension (pp. 92-98). Philadelphia:
National Board of Medical Examiners.
Dauphinee, WD, Blackmore, DE, Smee, SM, Rothman, AI, Des Marchais, J, &
Reznick, RK. (2000). Adaptive testing: A report on the results and myths arising
from the use of a sequenced OSCE for national licensure. In D. E. Melnick (Ed.),
Proceedings of the Eighth Ottawa International Conference - Evolving
Assessment: Protecting the Human Dimension (pp. 241-246). Philadelphia:
National Board of Medical Examiners.
Smee, SM, Blackmore, DE, Rothman, AI, Reznick, RK, & Dauphinee, WD. (2000).
Pioneering a sequenced OSCE for the Medical Council of Canada: An
administrative overview. In D. E. Melnick (Ed.), Proceedings of the Eighth
International Ottawa Conference - Evolving Assessment: Protecting the Human
Dimension (pp. 234-240). Philadelphia: National Board of Medical Examiners.
Poldre, P, Smee, SM, Reznick, RK, Blackmore, DE, Birtwhistle, R, Blouin, D,
Chalmers, A, Galway, B, Hodges, B, MacFadyen, J, & Spady, D. (1999). The
experience of thousands: The post-examination OSCE station review process of
the Medical Council of Canada. In D. E. Melnick (Ed.), Evolving assessment:
Protecting the human dimension (CD-ROM) Philadelphia: National Board of
Medical Examiners.
Dauphinee, WD, Blackmore, DE, Smee, SM, Rothman, A. I, & Reznick, RK. (1997).
Using the judgments of physician examiners in setting the standards for a
national multi-center high stakes OSCE. Advances in Health Sciences Education:
Theory and Practice, 2, 201-211.
Dauphinee, WD, Blackmore, DE, Smee, SM, Rothman, AI, & Reznick, RK. (1997).
Optimizing the input of physician examiners in setting standards for a large
scale OSCE: Experience with Part II of the Qualifying Examination of the
Medical Council of Canada. In A. J. J. A. Scherpbier, C. P. M. van der Vleuten,
J. J. Rethans, & A. F. W. van der Steeg (Eds.), Advances in Medical Education:
Proceedings of the Seventh Ottawa International Conference on Medical
Education (pp. 656-658). Dordrecht: Kluwer Academic Publishers.
Medical Education (pp. 458-461). Dordrecht: Kluwer Academic Publishers.
Smee, SM. & Sumawong, V. (1997). Advancing the use of standardized patients: A
workshop for the consortium of Thai medical schools. In AJJA. Scherpbier,
CPM van der Vleuten, JJ Rethans, & AFW van der Steeg (Eds.), Advances in
Medical Education (pp. 714-716). Dordrecht: Kluwer Academic Publishers.
Smee, SM. & Blackmore, DE. (1997). Preparing physician examiners for a high
stakes, multi-site OSCE. In AJJA Scherpbier, CPM. van der Vleuten, JJ Rethans,
& AFW van der Steeg (Eds.), Advances in Medical Education (pp. 462-469).
Dordrecht: Kluwer Academic Publishers.
Reznick, RK, Blackmore, DE, Dauphinee, WD, Rothman, AI, & Smee, SM. (1996).
Large-scale high-stakes testing with an OSCE: Report from the Medical Council
of Canada. Academic Medicine, S71, 19-21.
Smee, SM. (1994). Medical Education Clinic: Using SPs for teaching and evaluation.
Adult Education Quarterly, 6, 9-10.
Reznick, RK, Blackmore, DE, Cohen, R, Baumber, JS, Rothman, AI, Smee, SM,
Chalmers, A, Poldre, P, Birtwhistle, R, Walsh, P, Spady, D, & Bérard, MJ.
(1993). An objective structured clinical examination for the licentiate of the
Medical Council of Canada: From research to reality. Academic Medicine, S68,
4-6.
Reznick, RK, Smee, SM, Baumber, JS, Cohen, R, Rothman, AI, Blackmore, DE, &
Bérard, M. (1993). Guidelines for estimating the real cost of an objective
structured clinical examination. Academic Medicine, 68, 513-517.
Reznick, RK, Smee, SM, Rothman, AI, Chalmers, A, Swanson, DB, Dufresne, L,
Lacombe, G, Baumber, J, Poldre, P, Levasseur, L, Cohen, R, Mendez, J, &
Bérard, M. (1992). An objective structured clinical examination for the licentiate:
Report of the pilot project of the Medical Council of Canada. Academic
Medicine, 48, 487-494.
Stillman, PL, Swanson, DB, Smee, SM, Stillman, AE, & Ebert, TH. (1986).
Assessing the clinical skills of residents with standardized patients. Annals of
Internal Medicine, 105, 762-771.
China Medical University
University of Calgary, MSc in Medical Education
University of Calgary, PhD in Medical Education
Present Academic and Administrative approintment:
Director, Department of Pediatrics, Taipei
Medical University WanFang Hospital
Vice Director, Faculty of Medicine, Taipei
Medical University
Vice Director, Education and Research, Taipei
Medical University WanFang Hospital
Associate professor, Taipei Medical University
Instructor Assistant’s Curriculum Vitae
Charity TC Tsai, MD, PhD
Publication (in recent 5 years)
1.
Tsuen-Chiuan Tsai, Using children as standardized patients for assessing clinical
competence in pediatrics. Arch Dis Child 89 (12): 1117-1120, Dec. 2004
2.
Tsuen-Chiuan Tsai, M.D., Peter H. Harasym, Ph.D., Cheri Nijssen-Jordan, and
Greg Powell, Learning gains derived from a high fidelity simulation in
emergency department J Formos Med Assoc 105 (1):94-98, 2006
3.
JD Tsai, FU Huang, CC Lin, TC Tsai, HC Lee, and JC Sheu. Intermittent
hydronephrosis secondary to ureteropelvic junction obstruction: clinical and
imaging features. Pediatrics. 2006 Jan;117(1):139-46.
4.
Tsai TC, Harasym PH. Challenges of pediatric residency education in Taiwan.
Acta Pediatrica Sinica. 47(1):3-6, 2006
5.
Tsuen-Chiuan Tsai . Psychosocial effects on caregivers for children in Taiwan on
chronic peritoneal dialysis. Kidney Int. 2006 Dec;70(11):1983-7
6.
Tsuen-Chiuan Tsai . University of Washington 家醫科及臨床技能中心參訪. J
Med Education. Jan. 10(1): 86-88, 2006
7.
Tsuen-Chiuan Tsai,
1Pei-Jung Chang,
2Shin-Yuan Fang
,
2Chyi-Her Lin
3.A
Mannequin-based Simulation on Teaching Emergent Crisis Care. J Med
Education, 10(2): 115-125, 2006
8.
Sheu JC, Koh CC, Chang PY, Wang NL, Tsai JD, Tsai TC. Ureteropelvic
junction obstruction in children: 10 years' experience in one institution.
Pediatr Surg Int. 2006 Jun;22(6):519-23
9.
Tsai YC, Tsai TC, Tsaf JD, Huang FY, Lin CC, Sheu JC. Clinical analysis of
chronic peritoneal dialysis related peritonitis in children. Pediatr Neonatol. 2006
Yeh, Jing-Jane Tsai, Yin-Fan Chang. Analysis of OSCE results: experience in
National Cheng Kung University Medical College. J Med Education 10
(4):313-23, 2006
11. Huang DTN, Tsai TC, Huang FY, Tsai JW, Chiu NC, Lin CC. Clinical
differentiation of acute pyelonephritis from lower urinary tract infection in
children. Journal of microbiology, immunology and infection. J Microbiol
Immunol Infect. 2007;40:513-517
12. Tsai TC. Resistance to educational change: management and communication.
Pediatr Neonatol.48:3-6, 2007
13. Tsai TC, Lin CH, Harasym PH, Violato C. Students' perception on medical
professionalism: the psychometric perspective. Med Teach. 2007
Mar;29(2-3):128-34.
14. Peter H. Harasym, Tsuen-Chiuan Tsai, and Payman Hemmati. Current trends in
developing medical students’ critical thinking abilities. Kaohsiung J Med Sci
July 2008. 24 (7) 341-354
15. Tsuen-Chiuan Tsai. The Use of Medical Cognition in Medical Curriculum
Reform in Taiwan. Pediatr Neonatol 2008;49(3):53−57
16. 蔡淳娟、邱文達、王先震、連吉時、粟發滿、郭雲鼎、徐明義.The use of portfolio
in internship clinical education. J of Med Edu 12(1): 8-19.2008.
17. Lee MD, Lin CC, Huang FY, Tsai TC, Huang CT, Tsai JD. Screening young
children with a first febrile urinary tract infection for high-grade vesicoureteral
reflux with renal ultrasound scanning and technetium-99m-labeled
dimercaptosuccinic acid scanning. J Pediatr. 2009 Jun;154(6):797-802.
18. 顏如娟,蔡淳娟,郭耿南,張殷瑞,陳泰宏.台灣醫師人力需求之探討.投稿台灣公
共衛生雜誌 2009/07
19. Tsuen-Chiuan Tsai, Peter H. Harasym, Sylvain Coderre, Kevin McLaughlin, &
Tyrone Donnon. Assessing ethical problem solving by reasoning rather than
decision making. Med Edu 2009: 43: 1188–1197
20. Ju-Chuan Yen,Tsuen-Chiuan Tsai, Min-Huei Hsu, Kung-Jiang Chang, Du-Jian
Tsai, Wei-Hua Lee. The attitudes toward disclosure of medical errors: the
perspectives of Taiwanese with different occupational backgrounds. Submit to
The American Journal of Bioethics (UAJB-2009-0218) 2009/04/14
21. Tsuen-Chiuan Tsai, Peter H. Harasym. An Ethical Reasoning Model:
Contributions to Medical Education. (Submitted to Med Educ in 2009/09)
22. 蔡淳娟,林其和,劉克明. 台灣各界對醫學系學制變革可行性的看法. 投稿醫
Moderator’s Curriculum Vitae
Professor Chao Hsiang Yang (楊朝祥部長)
Present Positions
Minister, Ministry of Examinations
Professor Wen-Ta Chiu (邱文達校長)
Present Positions
Professor and President, Taipei Medical University
Professor Chong-Liang Shi (石崇良處長)
Present Positions
Director of Medical Affairs, Department of Health
Professor Chi-Wan Lai (賴其萬教授)
Present Positions
Executive Secretary, Medical Education Committee, Ministry of Education
CEO, Taiwan Medical Accreditation Council
Date: 07 January, 2010 High- Stakes OSCE (I): Administrative Issues and Related Topics
Sydney M Smee, Ph. D.
Manager, MCCQE Part II
Evaluation Bureau, Medical Council of Canada
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
1
My Background
•
Standardized Patient at McMaster University with Dr.
Howard Barrows and Gayle Gliva-McConvey
•
Coordinator for Patient Instructor Program at University
of Massachusetts for Dr. Paula Stillman
•
Did other things….
•
Standardized Patient Training Coordinator for the pilot
project for the Medical Council of Canada’s new
Qualifying Examination Part II in 1992
•
Now – Manager for the MCCQE Part II
•
Keep this in mind - I am strongly influenced by long time
commitment to standardized patients and OSCEs
2
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
3
What is the Part II?
•
(Part I assesses knowledge and clinical
decision-making at end of medical
school – computer testing / MCQs)
•
Part II is an OSCE that assesses clinical
skills after 12 months of post-graduate
clinical training
•
Multi-site, administered twice per day
•
Timed circuit of 12 stations
•
Patient-based
•
Physician-scored
•
Prerequisite for licensure in Canada
since 1993
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
4
Why do we have the Part II?
•
Requested by the Medical Licensing Authorities
because they were facing:
▫ Increasing number of complaints, often based on a
physician’s communication skills.
▫ Need to be publicly accountable; e.g., reports that not
all trainees were being assessed in a clinical setting.
▫ Obligation to audit the training of all medical
graduates seeking licensure in Canada.
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
5
Content of Part II
•
Multidisciplinary, patient-based cases
▫ Some have a written component based directly on the
patient problem
•
Common or acute presenting problems
▫ Some problems include legal and ethical issues
•
Assesses skills:
▫ History taking
▫ Physical examination skills
▫ Counseling / patient education skills
▫ Patient management ability
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Part II - Fall 2009
•
12 case OSCE with 2 pilot cases
▫ 5+5 minute couplets (patient + written components)
▫ 10 minute case (sometimes there was an oral component)
•
OSCE was run twice per day
•
16 university-based sites (at teaching hospitals)
•
2,644 test takers assessed in two days
•
Most common site model ran two tracks and
administered the OSCE twice in one day – assessed
128 test takers
-▫ 44 clinic rooms
- 50 to 60 standardized patients
▫ 44 physician examiners
- 16 to 20 staff people
Goals for Workshop
•
Provide overview of OSCE processes
•
Set specifications for an OSCE
•
Identify critical tasks and timelines
•
Estimate costs
•
Review training needs
•
Discuss “hot topics”
•
Specify next steps in the process
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
7
Six OSCE Processes for Multi-site Model
•
Initiation
▫ Governance
▫ Terms of Reference ▫ Design and scope
•
Content Development
▫ Create
▫ Edit and Format ▫ Approve
•
Site Development
▫ Determine specifications ▫ Recruit key staff
▫ Provide training
•
Production (pre-OSCE)
▫ Establish supply needs ▫ Create and produce materials ▫ Ship
•
Processing (post-OSCE)
▫ Receive ▫ Enter scores ▫ Analyze data
•
Registration and Reporting
▫ Eligibility criteria▫ Document requirements ▫ Results and appeals
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Initiation
Part II Terms of Reference:
• Collaborative agreement
• Schools provide office space, clinic
space (for OSCE days), equipment, and name the Chief Examiner
• MCC provides funds, OSCE
materials, training and supervision
• Design & Scope
• Part II has changed over time
• Two days / 20 stations / 5 sites
• One day / sequenced / 12 sites
• One day / 14 stations / 15 sites
• One day / 12 stations / 16 sites
• Two days/ 12 stations / 17 sites
• This workshop:
• Design and define an OSCE…
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
9
MCC Part II Governance Model
Content Development
•
MCC content is created centrally
▫ Multidisciplinary committee with members balanced across
• Medical specialty
•
Language (French – English)
• Geography
• Gender
▫ Members are active clinicians with faculty appointments
▫ All have a keen interest in medical education
▫ Faculty from the medical schools work with the committee
to create and review cases
•
MCC staff provide support:
▫ Plan meetings
▫ Psychometric and logistical advice
▫ Edit, format and produce OSCE materials
•
More on case writing at the next workshop….
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Site Development
(It’s all about the people.)
•
Determine site specifications
▫ Clinic Room requirements ▫ Large rooms for orientation ▫ Office space, furniture and computers, telephones, etc. ▫ Exam day staffing needs ▫ Parking and catering•
Recruit key site staff
▫ Site Manager ▫ Chief Examiner ▫ SP Trainer
•
Provide training and
supervision
▫ Job descriptions ▫ Manuals ▫ Central meetings ▫ Telephone support ▫ Site visits▫ Exam day supervision ▫ SP training materials
Case materials Videos
Internet resources Diagrams
Training for Trainers
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
11
Production
•
Establish supply needs
▫ Signage, props, registration materials, incident reporting
▫ Exam sheets
▫ Orientation materials for site staff, examiners, and test takers
Print, video, other? (e.g., booklets and lab values)
▫ Identify security challenges and solutions
•
Create and produce exam materials
▫ What software?
▫ How are you collecting score data?
▫ What about other data? Feedback from examiners?
•
Ship the materials to the site(s)
▫ Shipment deadline is a major milestone
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Processing
•
Receive (after the examination)
▫ Verify return of materials is complete
•
Enter scores
▫ What process depends on software used
▫ Ensure format of data allows for quality assurance and for
score reporting
•
Analyze data
▫ Item analysis of cases
▫ Reliability of OSCE
▫ Review of examiners and exam day reports
▫ Review of results
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
13
Registration and Reporting
•
Eligibility criteria
▫ What are the criteria and how will this be communicated to test takers?
•
Document requirements
▫ How will you verify eligibility?
•
Results
▫ Who has access to the results?
▫ How will they be reported?
•
Appeals
▫ Define conflict of interest and other reasons for appeals
▫ Determine process for appeals
Consider different levels; e.g., rescores and feedback calls
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
....Making many decisions
Presented at Taipei Medical University, WanFang Hospital by the TaiwanAssociation of Medical Education, January 2010
15
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
16 Define performance standard Which clinical skills? Who assesses? What clinical presentations? Length of stations? How many stations?
Define a standard –
MCCQE Part II:
Acceptably competent to enter independent
medical practice in Canada
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
17
Blueprint criteria = Validity
Body Systems Clinical Tasks
History Taking Physical Exam Procedural Patient Education ?? Cardiac Respiratory X Gastrointestinal Reproductive X X ??
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
18
Define the criteria for selecting cases for
each test form
MCCQE Part II Blueprint Criteria
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
19
DOMAIN Counseling/Education 2
History 4 (or 5)
Management / Acute Care 2
Physical exam 4 (or 3)
Combined History / Physical
(2 – if possible)
Patient Interaction Rating scales are integrated within most stations
DISCIPLINE Medicine 3
Ob/Gyn 2
Pediatrics 2
Psychiatry 2
Surgery 3
NOTE Review problems to ensure balance across body systems CLEO content must comprise a minimum of 10% of overall content.
CLEO is integrated into cases with oral questions and patient interaction rating scale items
HISTORY of USE No more than 3 stations with high exposure (as a guide) New cases in each blueprint (no specific numbers assigned)
Item Total Score
Correlation Minimum: 0.20 (AS A GUIDE) GENDER as balanced as possible
AGE GROUPS Elderly / Adult / Adolescent / Young children One or more cases representing each age group
Patient problems are common or critical; each case is linked to the MCC Objectives
Clinical Skills and Presentations
•
Some things are more “OSCE-able” than others
•
Some cases cost more to administer
▫ Multi-patient cases and manikins may be a challenge
•
Large-scale, multi-site OSCE have some limitations
▫ Must have the same resources at all sites
•
Focus on skills and content best assessed by OSCE
▫ Content that can be assessed more cost effectively in
other formats (like multiple choice examinations)
should not be included in an OSCE
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Long versus short cases / Reliability
•
Long cases (>12 minute cases)
▫ Assess complete encounters (e.g., Hx + Physical)
▫ Fewer cases and examiners per test taker
▫ Long testing time required to achieve reliable scores
▫ Can assess performance on more complex problems
•
Short cases (5 -12 minute cases)
▫ Assess samples of performance
Suggests assessment of clinical judgment
▫ More cases and more examiners per test taker
increases reliability
•
Mix of long and short cases
▫ More complex OSCE design (but still do-able)
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
21
What is your preference for an OSCE?
1.
Fewer longer cases
2.
More shorter cases
3.
Mix of short and long cases
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
What do you think the minimum
number of cases is for a valid OSCE?
1.
Six
2.
Eight
3.
Ten
4.
Twelve
5.
Fourteen
6.
Sixteen
7.
Eighteen
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
23
Which of the following do you think
should be assessed in an OSCE?
1.
History taking
2.
Physical examination skills
3.
Patient education ability
4.
Managing acute problems
5.
Managing non-acute problems
6.
Responses to ethical issues
7.
Interpretation of investigations
8.
Procedural skills
9.
Written tasks (e.g., admission orders)
10.
Other
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Group Task for After Break
•
Five Groups – One Reporter for each group
•
Start designing an OSCE for assessing ....
•
Specify the clinical skills you want assessed
▫ Define the range of clinical presentations by
discipline and/or body system (or other criteria)
▫ Determine how many patient cases
▫ Specify the time limit for cases
•
Group reports after lunch…
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
25
Group Reports
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Exam Day Scheduling
•
To cost an OSCE you need a design and an exam
day schedule (to start)
•
Large portion of the costs are people
▫ Need to specify what is expected of the people
•
Once you cost a design, you will likely revise it…
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
27
28
Activity Time Chief Examiner Manager SP Trainer Timers Hall Staff Group Leaders Caterers
Set-up site 6:00
Register SPs /Staff 6:15 Register / Orient Examiners 6:30 Register / Orient AM Test takers 6:45 Move people to stations 7:00
1 Start OSCE 7:15
Break in OSCE? 7:30
2 End OSCE 7:45
Lunch Break? 8:00
Register / Orient PM Test takers 8:15
3 Start OSCE 8:30 Break in OSCE? 8:45 4 End OSCE 9:00 Clean-up Site 9:15 9:30 9:45 10:00 10:15 10:30 10:45 11:00 11:15 11:30 11:45 12:00 12:15 12:30 12:45 13:00 13:15 13:30 13:45 14:00 14:15 14:30 14:45 15:00 15:15
Tasks
•
Central Tasks
▫ Communicate with stakeholders: Test takers, medical faculties, ?? ▫ Establish registration
processes
▫ Create and produce OSCE materials
▫ Develop protocols for training everyone ▫ Visit sites
▫ Run central meetings ▫ Process results ▫ Report results
•
Site Tasks
▫ Plan layout of OSCE stations at the site
▫ Book clinics and orientation rooms
▫ Recruit SPs and examiners ▫ Train SPs
▫ Recruit staff- train them too ▫ Plan out the OSCE day in
great detail ▫ Run the OSCE ▫ Ship everything back
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
29
Production Timeline - Milestones
10. Report Results 9. Complete QA on Scores 8.Exam
Day 7. Ship to site(s) mark sheets6. Print
5. Training meetings 4. Recruit staff at exam site 3. Letter of Agreement with site 2. Finalize case content 1. Finalize OSCE design
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
30
Work backwards……
Production processes overlap with site development
processes…..
2. Finalize case content 1. Finalize OSCE design
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
31
5. Training meetings 4. Recruit site personnel
3. Agreement with sites
3.
Letter of Agreement signed
▫ Funds forwarded
▫ Chief Examiner appointed
4.
Recruit site personnel
▫ Manager and SP Trainer
▫ Examiners and Standardized Patients ▫ Site staff for timing, registration etc.
5.
Training meetings
▫ Centrally – site team(s) and core staff ▫ Not too early and not too late
▫ Balance input from sites with central control….
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
8. Exam Day 7. Ship to site
6. Print mark sheets
6.
Print mark sheets
▫ Significant deadline – no more changes without pain ▫ Production takes careful, detailed planning
▫ Attend to security issues/ inventory tracking etc.
7.
Ship to sites
▫ Central control is “gone” – it’s in the hands of the site team ▫ Increasing focus on support
8.
Exam day
▫ Oversight
▫ Incident reporting
▫ What can go wrong, will go wrong – be prepared to learn
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
33
10. Report Results 9. Complete QA on Scores
9. Complete quality assurance on scores ▫ Verify the scores are accurately recorded ▫ Assess how the cases performed (item analysis)
▫ Assess how the examiners performed (any hawks or doves?) ▫ Assess how the OSCE performed (reliability)
▫ Take into account exam day incident reports
10. Report results ▫ Who gets what? ▫ Scores? Pass/Fail? ▫ Feedback?
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Required Resources
Central Resources
•
Staff Positions
▫ How many? ▫ What qualifications?•
Case Writers
▫ How many?▫ How many meetings?
•
Office(s)
▫ Existing or new?
•
Equipment and software
▫ Existing or new?
Site Resources
•
Staff positions
▫ How many? ▫ What qualifications?•
Office(s)
▫ New or existing?•
SP training room(s)
•
Equipment and software
▫ Existing or new?
•
Challenges?
▫ What else do you need to know?
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
35
Five Groups – Tasks to be assigned
•
Group 1:
•
Group 2:
•
Group 3:
•
Group 4:
•
Group 5:
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Group Reports
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Date: 08 January, 2010 High- Stakes OSCE (I): Administrative Issues and Related Topics
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
38
A large group experiment with an Excel workbook
Training Issues
•
Chief Examiners & Managers
▫ Critical roles in preparing for the OSCE at the site level ▫ At the beginning, these
people can help create
protocols and forms to ensure the OSCE is standardized ▫ Benefit of multi-site OSCE is
working with others, receiving training
▫ Cost of multi-site OSCE is loss of local autonomy
•
Examiners
▫ Orient to the OSCE
▫ Training may be delivered locally by site staff OR centrally via web-based technology
▫ When and how to orient examiners is a compromise between the ideal and practical
▫ Local support and direction to site-specific issues is always needed
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
40
Training Issues
•
Standardized Patients
▫ Longer cases require more training
▫ More complex cases require more training (e.g.,
psychiatric affect, multiple physical symptoms)
▫ Good training involves practicing with someone acting as a candidate and getting feedback
▫ Training should happen close to the OSCE
•
Exam Day Staff
▫ Need to understand the OSCE and why its important
▫ Need to know their specific tasks (e.g. timing, collecting mark sheets, directing people)
▫ Need to know what to do when something goes wrong (and something always does) ▫ Training based on centrally
developed materials and given locally leads to fair testing
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Hot Topics
•
Examiner qualifications
•
Incidents
•
Re-scores and Appeals
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
42
Examiner Qualifications
•
Formal MCC Criteria:
▫ Must have the Licentiate of the Medical Council of Canada
(LMCC).
▫ Should be 3 years post-LMCC.
▫ Should have at least 3 years in independent practice.
▫ Cannot be residents or fellows. Examiners must hold an
unrestricted license and currently be practicing medicine.
▫ Should have the ability and stamina for the task (e.g.,
hearing loss is a serious handicap).
▫ May be community physicians.
•
Informally, Chief Examiners interview any examiners
who are not known
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Incident Reports – What can go wrong?
•
Conflicts of interest
•
Examiner errors
•
Candidate is inappropriate
•
Timing errors
•
Illness (SPs, test takers, examiners)
•
Missing materials
•
Missing SP
•
Missing examiner
•
Flooding toilet, fire alarms, parades,
strikes…
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
44
What can be done?
•
With a pass/fail examination the incidents that
are most critical are those that impact test takers
who are borderline failures
▫ Is incident significant?
▫ Delete the station?
▫ Invalidate the examination?
MCC will not assume a pass standing
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Re-scores and Appeals:
Risk Management
•
Have policies and procedures in place for
answering post-OSCE questions and complaints
▫ Follow-up t0 selected letters and incident reports
▫ Providing feedback in exam reports or by request
▫ Rescores to verify results
▫ Appeal process for complaints
Process for low level issues, more formal for serious
issues
46
Sydney M Smee [email protected] www.mcc.ca
Presented at Taipei Medical University, WanFang Hospital by the Taiwan Association of Medical Education, January 2010
Review Article
The Use of Standardized Patient Assessments for Certification
and Licensure Decisions
John R. Boulet, PhD; Sydney M. Smee, PhD; Gerard F. Dillon, PhD; John R. Gimpel, DO
Although standardized patients have been employed for formative assessment for over 40 years, their use in high-stakes medical licensure examinations has been a relatively recent phenomenon. As part of the medical licensure process in the United States and Canada, the clinical skills of medical students, medical school graduates, and residents are evaluated in a simulated clinical environment. All of the evaluations attempt to provide the public with some assurance that the person who achieves a passing score has the knowledge and/or requisite skills to provide safe and effective medical services. Although the various standardized patient-based licensure examinations differ somewhat in terms of purpose, content, and scope, they share many common-alities. More important, given the extensive research that was conducted to support these testing initiatives, combined with their success in promoting educational activities and in identifying individuals with clinical skills deficiencies, they provide a framework for validating new simulation modalities and extending simulation-based assessment into other areas.
(Sim Healthcare 4:35– 42, 2009)
Key Words: Licensure, Certification, Simulation, Standardized patient, Simulated patient,
OSCE
T
here are many types of simulations that are currently being used to assess healthcare professionals.1– 4 In both Canadaand the United States (US), many of these simulation modal-ities, including multiple choice questions, part-task trainers, and computer-based case simulations, have been used as part of the examination process used to certify and license physi-cians.1,5,6 These simulation-based examinations, which can
vary somewhat in terms of purpose and focus, all attempt to provide the public with some assurance that the person who achieves a passing score has the knowledge and/or requisite skills to provide safe and effective medical services, either independently or under supervision. Here, as with any sim-ulation-based assessment, the structure, content, fidelity, and difficulty of the modeled exercises, combined with the scores, will determine what inferences one can make about the indi-vidual test taker.
From a simulation perspective, the use of standardized patients (SPs) for certification and licensure decisions has been a relatively recent phenomenon.7Historically, SP-based
assessments were implemented as part of formative
evalua-tion activities.8 –10Individuals were trained to portray specific
patient conditions, allowing medical students to practice their clinical skills and receive immediate feedback concern-ing strengths and weaknesses. In the 1980s, with an increased emphasis on evaluating what medical trainees could do, as opposed to what they knew, various organizations started research programs aimed at determining how assessments employing SPs could be structured to make valid skills-based proficiency decisions. Over the next two decades, the end result of these research activities was the implementation of a number of high-stakes assessments all aimed at measuring abilities in key clinical skills domains. Although these re-search efforts required extensive resources, they were suc-cessful in identifying the specific conditions and structures that are needed to produce defensible scores and decisions for multistation, performance-based, simulation activities.11–17
The introduction of SP-based certification and licensure examinations in medicine was a monumental achievement. Although other high-stakes simulation-based assessments have been developed and used in other professions, the logis-tical, economical, and psychometric challenges associated with national multistation clinical skills assessments were staggering.18,19Organizations that built these assessments all
had to address concerns regarding test content (eg, types of scenarios to model), test administration models (eg, fixed versus temporary sites; number, timing and sequencing sta-tions), measurement rubrics (eg, holistic or analytic), eligi-bility requirements, scoring models (eg, compensatory or
From the Foundation for Advancement of International Medical Education and Research (J.R.B.), Philadelphia, PA; Medical Council of Canada (S.M.S.), Ottawa, ON, Canada; National Board of Medical Examiners (G.F.D.), Philadelphia, PA; and National Board of Osteopathic Medical Examiners (J.R.G.), Conshohocken, PA.
Reprints: John R. Boulet, PhD, Foundation for Advancement of International Medical Education and Research, 3624 Market Street, Philadelphia, PA 19104 (e-mail: [email protected]).
clinical skills as part of certification/licensure process,20each
of these organizations was able to produce a high-quality simulation-based assessment that was appropriate for their particular needs. In doing so, many lessons were learned, the most important being that simulation-based summative as-sessment of clinical skills was viable, even with large examinee populations, differing testing purposes, and varying exami-nation administration protocols.
PURPOSE
The purpose of this article was to describe and contrast the Clinical Skills Assessment (CSA) programs that are employed in Canada and the US as part of the certification and licensure process for physicians. These assessments include the Medi-cal Council of Canada (MCC) Qualifying Examination Part II (MCCQE Part II),21the United States Medical Licensing
Examination (USMLE) Step 2 Clinical Skills (USMLE Step 2 CS),22 and the National Board of Osteopathic Medical
Examiners (NBOME) Comprehensive Osteopathic Medical Licensing Examination Level 2-Performance Evaluation (COMLEX-USA Level 2-PE).23 To better understand the
USMLE Step 2 CS, a brief overview of the Educational Com-mission for Foreign Medical Graduates (ECFMG) CSA is also provided.24The CSA was used to assess the clinical skills of
international medical graduates (IMGs) before the introduc-tion of USMLE Step 2 CS. Following this overview, a brief synthesis of the similarities and differences in the assessments and assessment programs is provided. With these distinc-tions in mind, and knowing the success and scope of the individual testing programs, it is possible to envision where summative simulation-based assessment activities could be enhanced, applied in other areas, and used for the evaluation of nonphysician healthcare professionals.
ASSESSMENT OF CLINICAL SKILLS
In general terms, clinical skills refer to information gath-ering and communication skills, applied during the patient encounter, that help to establish an accurate diagnosis and support high-quality treatment. Within the medical educa-tion and practice community, these skills have long been recognized as essential to patient care. Several organizations, including those responsible for the accreditation of under-graduate and under-graduate medical education (GME) programs, have included clinical skills among the competencies deemed important to the education and assessment of practicing phy-sicians.25–27As a result, it is not surprising that considerable
efforts have been made to develop, and subsequently defend, testing methods than can be used to reliably and validly mea-sure these skills.
STANDARDIZED PATIENTS
SPs, often referred to as simulated patients or pro-grammed patients, are people who have been trained to ac-curately portray the role of a patient with a specific medical condition or conditions. The term “standardized” refers to the fact that the person is specifically trained to model the
who interview the same SP with the same presenting com-plaint will receive, on questioning, the same patient history. The physical findings relevant to the case, either real or sim-ulated, need to be stable and, for a given modeled scenario, they must not vary from one SP to another.
LARGE-SCALE SP EXAMINATIONS
Medical Council of Canada Qualifying Examination Part II
Since 1912, the MCC has been setting an examination that is a prerequisite for medical licensure in Canada; the Licenti-ate of the MCC is granted to those who successfully complete it. In 1992, the MCC added the Qualifying Examination Part II (MCCQE Part II) to the assessment sequence. Initially the MCCQE Part II was a 20-station Objective Structured Clini-cal Examination (OSCE).7,28Although the use of OSCEs is
now commonplace throughout the world, implementing a national summative, performance-based, assessment based on a series of SP encounters was, at the time, unprecedented. The impetus for implementing the MCCQE Part II came largely from the licensing authorities. In the late 1980s, be-cause of the number and nature of related complaints that they received each year, members of these authorities began calling for an assessment of clinical and communication skills. The existing paper-and-pencil test of medical knowl-edge and problem solving (MCC Qualifying Examination Part I—MCCQE Part I) was not sufficient to address the emergent belief that candidates for medical licensure should be assessed more broadly.
To qualify for the MCCQE Part II, candidates must have completed successfully 12 months of postgraduate clinical training and passed the MCCQE Part I, currently a computer-adaptive test of knowledge and clinical decision-making. The number of candidates who qualify for the MCCQE Part II continues to grow. In 1992, 401 candidates took the exami-nation. In 2007, 3481 candidates completed this assessment, a more than eightfold increase.
As the measurement qualities of the MCCQE Part II be-came better understood, the number of stations was reduced from 20 to 14, and is now set at 12. This reduction in station length could be attributed to evolving test development pro-cesses, allowing for a more efficient and appropriate targeting of test content to examinee ability. Each station is based on a clinical problem presented by a SP; scoring is completed by physicians who observe from within the room. Checklists and rating scales are used to generate the station scores. At this time, the MCCQE Part II is comprised of eight 10-minute encounters with a SP and six couplet stations that include a 5-minute encounter with a SP followed by a 5-minute written component (Two of the stations in the as-sessment, including one of the couplets, are used for pilot testing purposes). Four domains are assessed based on com-mon presenting problems: history-taking skills, physical ex-amination skills, patient management, and doctor-patient interactions. Patient safety issues and professionalism are also evaluated.
ing poor performance in one station may be compensated by superior performance in another, the overall pass/fail deci-sion is based on a conjunctive standard; candidates must pass both by total score (the sum of their station scores) and by the number of stations passed.
Results from the MCCQE Part II are reported as a stan-dard score (mean ⫽ 500, standard deviation ⫽ 100). The examination is criterion-referenced, with the individual sta-tion pass marks set using the borderline group method.29
Candidates receive a bar graph indicating their performance in each of four domains relative to the mean score for their testing cohort. The four domains are data gathering (from history taking and physical examination tasks), patient inter-action (from rating scale items across stations), problem-solving and decision-making (based on certain stations; eg, acute care of trauma and the written work from the couplet stations), and legal, ethical, and organizational issues (which comprises a minimum of 10% of the total score). More ex-tensive feedback is provided to those candidates who are un-successful; specifically, they are told which stations they failed and are provided with a more extensive description of the four domains.
To balance accessibility and costs, a multisite, fixed test form model with two administrations per year is employed. In the spring, one test form is administered twice over 1 day at 10 university sites across Canada. At most sites, the examina-tion runs in two or more parallel tracks. In the fall, there are two test forms, one for each of 2 days of testing, and the examination runs at 16 sites. In spring, over 500 SPs are trained to simulate the patient problems. Twice that many are recruited for the fall. Ensuring that the SPs present their problems consistently and with sufficient fidelity for valid testing is critical. Each site has its own trainers who recruit and prepare the SPs according to the protocols developed centrally. Training videos, meetings with MCC staff, consul-tation with supervising physicians, along with telephone sup-port are all part of a process aimed at ensuring the SPs are ready for the examination.
Like all large-scale testing programs, there have been some administrative challenges. Developing feasible, psychometri-cally sound cases (simulated scenarios) is an ongoing task and takes considerable time and effort. Because the MCCQE Part II is a national examination, the scoring instruments and the supporting materials for SP training are developed centrally by a multidisciplinary test committee. Cases range from those requiring relatively little simulation (eg, history of diarrhea) to those where the SP must accurately simulate specific pa-tient presentations (eg, shortness of breath, decreased con-sciousness, pain, anxiety).
The MCC is continuously assessing different aspects of the MCCQE Part II. Numerous research studies suggest that both valid and reliable competency decisions are being made.30 –32 Most recently, the predictive validity of the
MCCQE Part II was investigated by looking at the relation-ship between MCCQE Part I and Part II scores and complaint
decision-making component from the MCCQE Part I were predictors for complaints.
Educational Commission for Foreign Medical Graduates Clinical Skills Assessment
Based on several years of extensive research and consulta-tion with the MCC, the ECFMG CSA was instituted in July 1998.34,35This 11 station clinical skills examination was
de-veloped to evaluate whether graduates of international med-ical schools (IMGs) possessed the skills necessary to enter supervised GME programs in the US. Successful completion of this examination became one of the required elements for ECFMG certification. Initially, the assessment was offered at one fixed site in Philadelphia, Pennsylvania. In 2002, in col-laboration with the National Board of Medical Examiners, a second testing site was constructed in Atlanta, Georgia. Be-tween 1998 and 2004, 43,624 IMGs were tested (37,930 first-time takers) in a total of 372,674 simulated clinical encoun-ters. During this time, numerous studies were published, several providing evidence to support the validity of the as-sessment scores.36 –38Of particular note, research was
con-ducted to show that SP and physician evaluations of clinical skills were comparable.39 In 2004, administration of the
ECFMG CSA ceased. Instead, IMGs were required to take and pass USMLE Step 2 CS (described below), a similar sim-ulation-based assessment that was developed to measure the clinical skills of American allopathic medical students and graduates. The USMLE Step 2 CS examination is part of the USMLE sequence (There are three “Steps” to the USMLE. Step 1 is intended to assess whether the examinee under-stands and can apply important concepts of the sciences basic to the practice of medicine. Step 2 focuses on the examinee’s knowledge, skills, and understanding of clinical science es-sential for provision of patient care “under supervision”— typically the point that medical school graduates begin their postgraduate education and experience. Step 3 is intended to assess whether the examinee can apply medical knowledge and understanding of biomedical and clinical science essen-tial for the unsupervised, independent practice of medicine.) To qualify for a medical license to practice in the US, gradu-ates of MD-granting schools in the US and gradugradu-ates of med-ical schools located outside the US must take and pass all components of USMLE.
United States Medical Licensing Examination Step 2 Clinical Skills
From the time that introduction of the USMLE program was first proposed in the late 1980s, it was the intent of the National Board of Medical Examiners and the Federation of State Medical Boards (the organizations that sponsor USMLE) to include clinical skills among the areas assessed as part of the examination program supporting the US medical licensing system. After many years of development, this goal became a reality in June 2004 when USMLE Step 2 CS was administered for the first time.40At this point, the previously
existing Step 2 examination, a 1-day, computer-based multi-ple choice questionnaire test, was renamed the Step 2 Clinical