Use of non-steroidal anti-inflammatory drugs and risk of chronic kidney
disease in subjects with type 2 diabetes mellitus, a nationwide
longitudinal cohort study
Hui-Ju Tsai1,2,3, Yueh-Han Hsu4,5,6, Ya-Wen Huang1, Yu-Kang Chang7, Jia-Sin Liu7,
Chih-Cheng Hsu 7,8
1Division of Biostatistics and Bioinformatics, Institute of Population Health Sciences,
National Health Research Institutes, Zhunan, Taiwan.
2Department of Medical Genetics, College of Medicine, Kaohsiung Medical
University, Kaohsiung, Taiwan.
3Department of Pediatrics, Feinberg School of Medicine, Northwestern University,
Chicago, IL, USA.
4Division of Nephrology, Department of Internal Medicine, Ditmanson Medical
Foundation Chia-Yi Christian Hospital, Chia-Yi City, Taiwan.
5Department of Nursing, Min-Hwei College of Health Care Management, Tainan
City, Taiwan.
6Department of Health Services Administration, China Medical University, Taichung
City, Taiwan.
7Division of Geriatrics and Gerontology, Institute of Population Health Sciences,
National Health Research Institutes, Zhunan, Miaoli County, Taiwan.
8Department of Health Services Administration, China Medical University and
Hospital, Taichuang City, Taiwan.
Correspondence and reprint requests should be addressed to:
Chih-Cheng Hsu, MD, DrPH, Division of Geriatrics and Gerontology, Institute of Population Health Sciences, National Health Research Institutes, 35, Keyan Road, Zhunan Town, Miaoli County 350, Taiwan.
Type of manuscript: Original Article
Running head: NSAIDs and chronic kidney disease
Key words: non-steroidal anti-inflammatory drugs (NSAIDs), chronic kidney
disease, type 2 diabetes mellitus
Word count for abstract: 250 Word count for the text: 2,700
Total (Introduction, Methods, Results, Discussion) Tables: 3
Abstract
Aims: Our understanding about whether the use of non-steroidal anti-inflammatory
drugs (NSAIDs) can cause kidney dysfunction remains inconclusive. We aimed to investigate the temporal relationship between NSAIDs use and the development of chronic kidney disease (CKD) in subjects with type 2 diabetes mellitus (T2DM).
Methods: We conducted a retrospective cohort study and followed up a CKD-free
T2DM sample (n=57,463) using national health insurance claims data in Taiwan. The NSAIDs exposure status in 2007 was measured. A total of 5,002 subjects with incident CKD were identified from 2008 to 2011. Multivariable proportional hazards models were applied to determine the temporal relationship between NSAIDs use and CKD development.
Results: We observed a significant temporal relationship between NSAIDs use and
CKD development in subjects with T2DM. Compared to subjects not taking any NSAIDs in 2007, subjects taking NSAIDs for at least 90 days in 2007 had a higher risk of CKD development (adjusted hazard ratio (AHR)=1.29; 95%CI: 1.20–1.40). In subgroup analyses, subjects (irrespective of age, sex, various comorbidities, and use of antihypertensive drugs, aspirin, or acetaminophen) taking NSAIDs for at least 90 days were more likely to develop CKD than subjects taking NSAIDs for less than 90 days or not taking NSAIDs.
Conclusions: The results suggest that there is a positive temporal relationship
between NSAIDs use and increased risk of CKD in subjects with T2DM. The use of NSAIDs should be based on clinical evaluations of benefits and risks, and should be prescribed with caution, particularly, among subjects at high-risk for CKD.
Introduction
Chronic kidney disease (CKD), which has experienced increased prevalence over the past decade, has become a worldwide public health problem [1–3]. Identification of CKD risk factors is therefore an inevitable research endeavor for the prevention of end-stage renal disease (ESRD). One of frequently recognized risk factors for CKD is the use of non-steroidal anti-inflammatory drugs (NSAIDs). Physiologically, NSAIDs have been shown to inhibit cyclooxygenase function, reduce prostaglandin
production, and change hemodynamics in the kidney, leading to acute renal failure [4–6]. Other short-term NSAID-related adverse renal effects such as sodium retention, GFR (glomerular filtration rate) alteration and blood pressure elevation have also been reported [5,7,8]. However, renal outcomes related to the use of NSAIDs, particularly their long-term effects, in population studies remain inconclusive [9,10].
Previous results from epidemiological studies have indicated that NSAIDs could further deteriorate already impaired renal function [11–13]. For example, it was shown that CKD patients who took non-selective NSAIDs, compared to those who did not, were 56% more likely to develop ESRD requiring dialysis [11]. In addition, it has been documented that high-dose NSAIDs use in the elderly with CKD was a significant risk factor that accelerated their CKD progression [12]. However, the impact of NSAIDs use on CKD development is still a debatable issue. Some studies showed that NSAIDs use was associated with hospitalization due to acute renal failure [12], moderate-severe CKD [14], or ESRD development [9]. To the contrary, the harmful effects of NSAIDs on renal function could not be confirmed in some cross-sectional [15], retrospective or prospective cohort studies [10].
Furthermore, to the best of our knowledge, there have been no studies to
investigate the renal effects of NSAIDs use in patients with type 2 diabetes (T2DM), even though they represent one of the vulnerable populations predisposed to develop
nephropathy [16,17]. In this study, we aimed at delineating the effects of NSAIDs use on CKD development in a longitudinal T2DM cohort.
Patients and methods Data source
The single-payer comprehensive National Health Insurance (NHI) program has been at the core of the health care system in Taiwan since 1995. Over the years, more than 98% of the total Taiwanese population has been enrolled in this program [18]. The National Health Insurance Research Database (NHIRD) derived from the NHI
reimbursement claims was created for research purposes. The data used for this study were obtained from the Longitudinal Health Insurance Database for the year 2005 (LHID2005) that was derived from the NHIRD of 2005. Briefly, LHID2005 was constructed by randomly selecting 1,000,000 enrollees from the Registry for Beneficiaries of the NHI program in 2005. There were no significant differences in the sex or age distributions or in the average insurable income between the random samples selected from the LHID2005 and the enrollees recorded in the original NHIRD. Detailed information on the sampling method representative of the LHID2005 is provided at http://w3.nhri.org.tw/nhird/date_01.html. This study was approved by the Institutional Review Board of the National Health Research Institutes in Taiwan.
Study cohort
From the LHID2005, we selected individuals aged 20 years or older in 2006 who had at least one hospital admission or two outpatient visits for diabetes-related illness (based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) code: 250.xx) within 1 year before 2007 as the T2DM
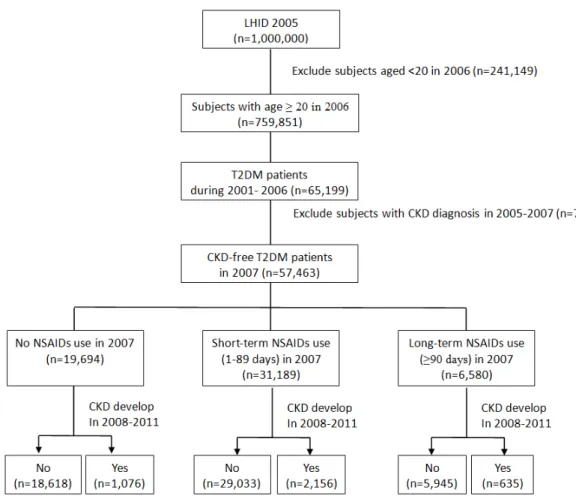
patients. In other words, subjects included in this study were those with diagnosis of DM in 2006, that is, prevalent DM subjects. We did not consider their DM status prior to 2006. From the identified T2DM patients, we excluded those who had at least one CKD diagnosis (ICD–9–CM codes: 250.4, 403–404, 582, 583, 585, or 586) in 2005– 2007. In detail, the study period was from January 1, 2006 to December 31, 2011. The inclusion criteria were described as follows: 1) subjects aged 20 years or older in 2006; 2) subjects who were diagnosed with T2DM (ICD–9–CM code:250.xx) in 2001 to 2006; 3) subjects who were CKD free in 2005–2007; and 4) subjects registered as NHI beneficiaries in 2006. As a result, a total of 57,463 CKD-free T2DM subjects were selected for the study. All study subjects were followed up until December 31, 2011 to record any incident CKD. Figure 1 presents the detailed flow chart regarding subject selection for this longitudinal cohort study.
Definition of exposure to NSAIDs
The NSAIDs investigated in this study included: 1) selective COX-2 inhibitors: celecoxib and etoricoxib; 2) propionic acid derivatives: ibuprofen, ketoprofen, naproxen, flurbiporfen, tiaprofenic acid, fenoprofen, and fenbufen; 3) acetic acid derivatives: ketorolac, indomethacin, tolmetin, sulindac, etodolac, diclofenac, aceclofenac, and acemetacin; 4) fenamic acid derivatives: mefenamic acid; 5) enolic acid derivatives: piroxicam, meloxicam, and tenoxicam; and 6) others (difunisal, nabumetone, nefopam, and nimesulide). The total prescription days of any NSAIDs in 2007 were summed to represent NSAID exposure time. We divided study subjects into three groups based on their NSAID exposure time in 2007: (1) subjects taking NSAIDs ≥ 90 days; (2) subjects taking NSAIDs at least one day, but less than 90 days; and (3) subjects who had not taken any NSAIDs. In subgroup analyses, we calculated the cumulative DDD (defined daily dose) of NSAIDs in 2007, and the
average daily NSAIDs dosage by dividing the cumulative DDD by 365.
Definition of subjects with CKD
The definition for newly diagnosed CKD subjects in this study was determined to be those who had a diagnosis of ICD–9–CM codes: 250.4 (diabetic nephropathy), 403– 404 (hypertensive nephropathy), or 582, 583, 585 and 586 (chronic kidney disease) in inpatient or outpatient medical claims data from 2008–2011.
Statistical analysis
We computed and compared the distributions of the demographic and clinical characteristics of our study subjects across three different NSAIDs exposure groups using chi-square test for categorical variables and F-test for continuous variables, respectively. Specifically, the examined demographic characteristics included age (20–29, 30–45, 46–60, 61–75 and >75 years), gender, enrollee category (I–IV) and geographical area (northern, central, southern and eastern), separately. In addition, we also measured comorbidity using the Charlson comorbidity index (CCI) score (=0, 1– 2 and 3) [19]. Of note, this study used enrollee category (EC) as a proxy measure to represent the study subjects’ socio-economic status (SES). A detailed description of EC classification can be obtained elsewhere [20]. Briefly, the insurance fee for the NHI Program was determined based on enrollees’ wages. Therefore, EC classified enrollees into 4 categories (EC I - EC IV), with EC I indicating those with the highest wages, while EC IV indicating those with the lowest wages. In terms of comorbidity, the list of diseases considered in the CCI score calculation included: myocardial infarction, congestive heart failure, peripheral vascular disease, dementia,
cerebrovascular disease, chronic pulmonary disease, connective tissue disease, peptic ulcer disease, mild liver disease, hemiplegia, moderate or severe renal disease,
diabetes, any tumor, leukemia, lymphoma, moderate or severe liver disease and metastatic solid tumor. Since the primary outcome of interest was incident CKD in patients with T2DM, moderate or severe renal disease and diabetes were not included in the CCI score calculation.
Cox proportional hazard models were performed to examine the association between CKD and various CKD-related risk factors (such as age, sex, hypertension (HT), CVD, stroke, CCI score, and use of insulin, four kinds of anti-HT drugs, statins, aspirin and acetaminophen) in subjects with T2DM. In addition, we applied Cox proportional hazard models to investigate the relationship between the effects of NSAIDs use (including: number of NSAID use days, cumulative DDD of NSAIDs use and average DDD of NSAID use, separately) and the risk of developing CKD, with and without adjustment of covariates. The list of covariates included: age (20– 29, 30–45, 46–60, 61–75 and >75 years), sex, geographical area, EC, hypertension, CVD, stroke, DM duration, CCI score (excluding moderate or severe renal disease and diabetes), and past-year medication use of insulin, four kinds of anti-HT drugs, statins, aspirin and acetaminophen, respectively. Of note, we used the NSAIDs non-exposure group as the reference group.
To examine the NSAIDs effect modified by the demographic and clinical
characteristics of the study subjects, we further performed subgroup analyses with and without covariate adjustment, stratified by age, sex, hypertension, CVD, stroke, CCI score, and past-year medication use of angiotensin converting enzyme
inhibitors/angiotensin II receptor blockers (ACEI/ARB), aspirin and acetaminophen, respectively. In addition, we have also added an interaction term for each examined covariate (including: age, sex, hypertension, CVD and stroke, CCI score, and medication use of ACEI/ARB, aspirin and acetaminophen) and NSAIDs use, and evaluated presence of effect modification, respectively.
All of the analyses were performed using SAS version 8.2 (SAS institute, Cary, NC).
P values less than 0.05 were declared statistically significant.
Results
Demographic and clinical characteristics of study subjects
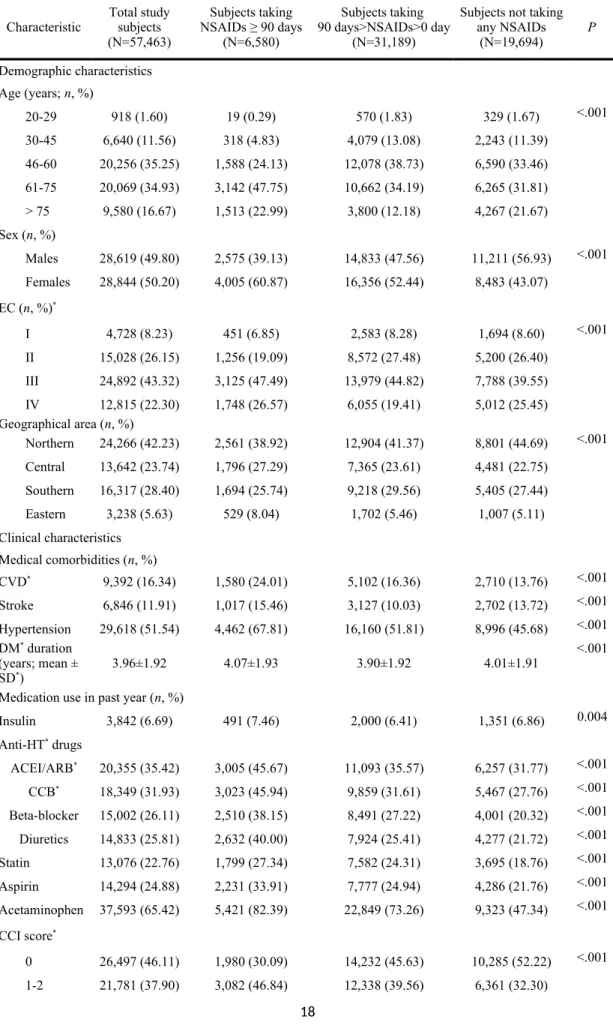
The study cohort included a total of 57,463 subjects with T2DM. Table 1 presents the demographic and clinical characteristics of the study subjects. Generally, the
distributions of age, gender, EC and geographical area were different across the three different NSAIDs exposure groups. In terms of clinical characteristics, the
percentages of hypertension, CVD and stroke were the highest for the group of subjects taking NSAIDs ≥90 days than for the other two groups. Similarly, CCI score and past-year medication use of insulin, anti-HT drug, statins, aspirin and
acetaminophen were higher in the group of subjects taking NSAIDs ≥90 days than in the other two groups.
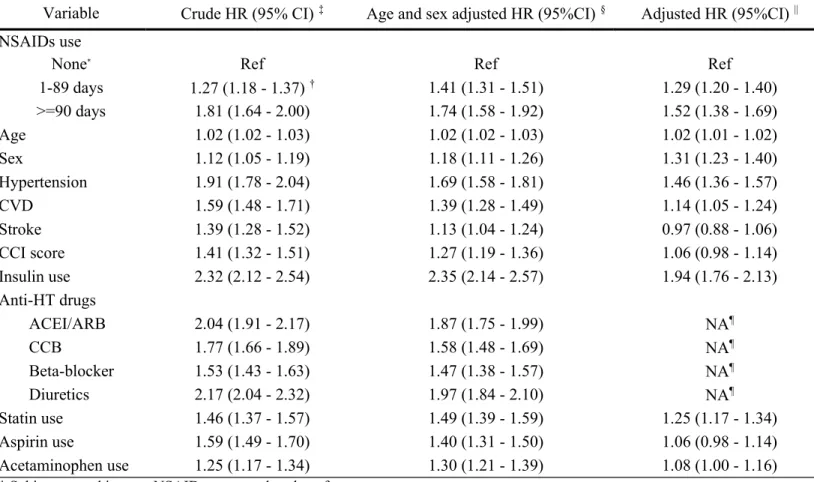
Association between CKD and various CKD-related risk factors
Table 2 presents the association between CKD and various CKD related risk factors such as age, sex, HT, CVD, stroke, CCI score, and use of insulin, four kinds of anti-HT drugs, statins, aspirin and acetaminophen in subjects with T2DM. The results from crude analyses indicated that all of the listed CKD related risk factors were significantly associated with CKD development. In addition to stroke, CCI score, and use of aspirin and acetaminophen, most of the other factors remained statistically significant when all CKD related factors were included in the same model (Table 2).
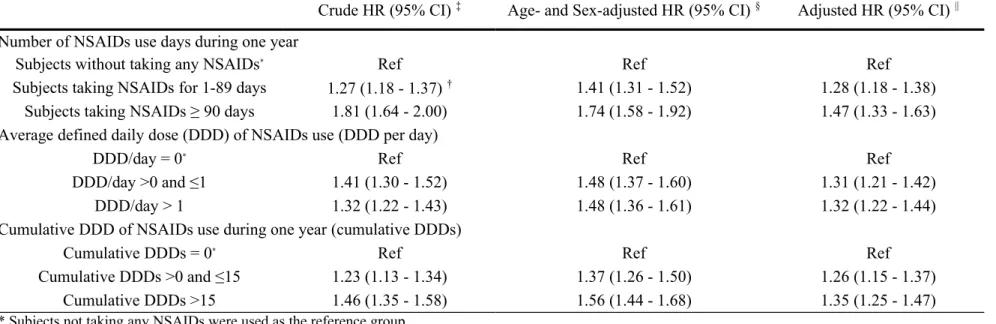
Temporal relationship between NSAIDs use and occurrence of CKD
between NSAIDs use and increased risk of CKD in subjects with T2DM, no matter which way we classified NSAIDs use. Compared to the non-exposure group, the risk of CKD development increased by at least 32% in those who had the highest exposure to NSAIDs in a 4-year follow-up period (AHR=1.47; 95% CI: 1.32–1.62 for NSAIDs use ≥ 90 days; AHR=1.32; 95% CI: 1.21–1.43 for NSAIDs use > 1 DDD per day; AHR=1.35; 95% CI: 1.25–1.46 for cumulative NSAIDs use > 15 DDDs).
Interestingly, we also observed a dose-response relationship between NSAIDs use and the occurrence of CKD in subjects with T2DM (Table 3).
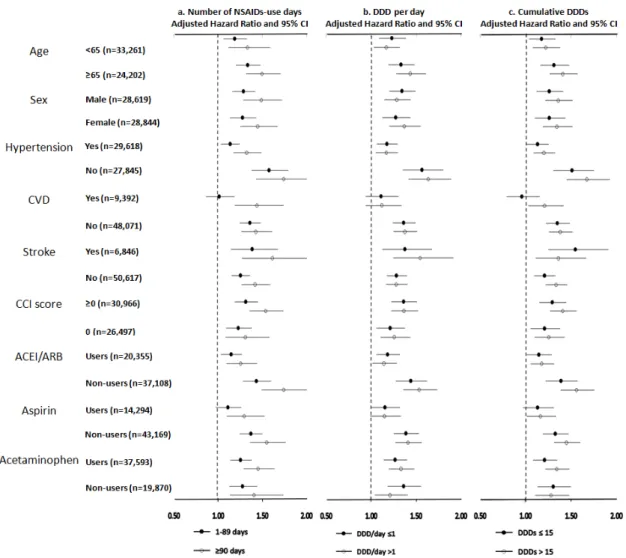
Subgroup analyses of NSAIDs use and CKD
The results of subgroup analyses are presented in Figure 2. Consistent with the findings in Table 3, subjects taking NSAIDs ≥90 days in 2007 had a greater risk of CKD than subjects taking NSAIDs less than 90 days in 2007 in all examined subgroups (stratified by age, sex, hypertension, CVD, stroke, CCI score, and medication use of ACEI/ARB, aspirin and acetaminophen). Likewise, the results in Figure 2 also show that subjects taking NSAIDs over one DDD per day or taking cumulative NSAIDs over 15 DDDs had a greater risk of CKD than their respective counterparts.
Discussion
This study demonstrated a significantly elevated risk of CKD with NSAIDs use in subjects with T2DM. To the best of our knowledge, this is one of the first nationwide longitudinal cohort studies examining the temporal relationship between NSAIDs use and an increased risk of CKD development in T2DM patients, namely, a vulnerable population predisposed to develop nephropathy. Moreover, the results also provided suggestive evidence that there was a dose-response effect of NSAIDs use on an
elevated risk of CKD in subjects with T2DM.
Previous studies have yielded inconclusive results with respect to NSAIDs use and the consequent development of CKD. Our results are in line with several previous studies suggesting the association between NSAIDs use and an increased risk for adverse renal outcomes [9,11,21–23]. For example, Sandler et al. examined the association of regular use of non-aspirin NSAIDs with the risk of CKD, and concluded that there was an elevated risk for CKD with daily use of NSAIDs,
especially for men aged more than 65 years [23]. In addition, Gooch et al. investigated the association between NSAID use and the risk for CKD progression in a
community-based elderly cohort and reported a positive association between high cumulative NSAIDs exposure and CKD progression in the elderly population [13]. Conversely, some other groups have reported a lack of association between NSAIDs use and CKD risk, especially for subjects who took NSAIDs occasionally [10,24]. For example, Rexrode et al. documented that no association was found between intake of acetaminophen, aspirin or other NSAIDs and risk of renal dysfunction in a cohort of initially healthy men [10]. Similarly, Kurth et al. observed that occasional to moderate use of acetaminophen, aspirin or other NSAIDs did not increase the risk of CKD in apparently healthy men [24]. It is likely that such inconsistent conclusions might be attributed to differences in study populations, study designs, case numbers and the set of adjusted confounding factors. Therefore, controversial findings from previous studies have implied that subjects with different health conditions or a different disease status may influence the effects of NSAIDs use on the occurrence of CKD different degrees.
In subgroup analyses, a greater risk of CKD attributable to NSAIDs use was noted among subjects aged 65 years or older than for those < 65 years. This result is in agreement with previous findings in elderly study populations [13,23]. Furthermore,
we found that the effect of NSAIDs use on the risk of CKD development was smaller among subjects with HT and/or taking anti-HT drugs ACEI/ARB than those without HT or not taking any anti-HT drugs ACEI/ARB. One possible explanation may be that T2DM subjects with HT and/or taking anti-HT drugs ACEI/ARB were in a CKD high-risk group and had more CKD-related risk factors than those without HT or not taking any anti-HT drug. It is possible that exposure to NSAIDs may have accounted for a limited degree of increased risk for CKD in these vulnerable T2DM patients. T2DM has been recognized as one of the major causes of CKD [17]. In addition, it has been noted that poor glycemic control in subjects with T2DM is one of the key risk factors leading to the development of CKD [25]. Additionally, a high prevalence of CKD in subjects with T2DM has been observed previously [26]. More importantly, the results in this study provide strong evidence that NSAIDs use significantly
increases the occurrence of CKD in subjects with T2DM. Therefore, it is important to provide clinical guidance when prescribing NSAIDs, particularly to subjects with T2DM, and specifically in terms of the potential adverse effects of NSAIDs on elevated risk for CKD.
Several potential limitations should be considered in this study. First, it was likely that NSAIDs use among the study population might be due to other symptoms that had a direct impact on kidney function or renal disease itself. Even though we adjusted for comorbid medical illnesses by using the CCI score in our analytical models, still, we could not totally exclude potential confounding by indication. Second, poor adherence or discontinuance in two NSAID exposed groups would result potential differential misclassification, consequently reduce the estimated risk. Thus, the findings should be interpreted with caution. Third, due to the fact that no laboratory/biochemical data are available in NHIRD, we had no such information for CKD diagnosis or severity of CKD. Therefore, we were unable to assess the effect of
NSAIDs use on different stages of CKD. In addition, it was likely that some
participants in the study cohort may have developed CKD, but would not have been identified using the ICD–9–CM codes for CKD due to lack of laboratory/biochemical data. However, misclassification of CKD diagnosis might be undifferentiated and would reduce the estimated risk.Fourth, in the present study, some potential
confounding factors that might affect the association between NSAIDs use and CKD such as serum albuminuria and eGFR levels were not available in the NHIRD. It was likely that the observed increased risk might be still partially explained by those
unmeasured confounders. Last, we did not assess whether different kinds of NSAIDs
use might have a different effect on renal dysfunction. It would be of interest to further explore this aspect.
In summary, our results document the temporal relationship between NSAIDs use and increased risk of CKD in subjects with T2DM. These findings underscore that close monitoring of renal function is advisable in T2DM patients at high risk for CKD when taking specified amounts of NSAIDs. More importantly, physicians should take more caution when prescribing NSAIDs to subjects with T2DM or subjects at high risk for CKD. Further investigation would be merited to facilitate a better
understanding of the underlying mechanisms in relation to the effects of NSAIDs use on CKD development in this vulnerable group.
Competing interests
Nothing to declare
Acknowledgements
This study is supported by grants from the National Health Research Institutes, Taiwan (PI: Tsai, PH–099–PP–56, PH–101–SP–14 and PH–102–SP–05) and the National Science Council, Taiwan (PI: Hsu, NSC 101–2314–B–400–002). We thank Tami R. Bartell at Lurie Children’s Research Center of Chicago for English editing. This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance of the Department of Health, Taiwan, and managed by the National Health Research Institutes, Taiwan (Registered numbers: 99081, 99136, 99287, 100007). The interpretation and
conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
References
1. Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United States. JAMA 2007; 298: 2038–2047. 2. Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, Ishani A, et al. US
Renal Data System 2010 Annual Data Report. Am J Kidney Dis 2011; 57: A8, e1–526.
3. Stevens PE, O'Donoghue DJ, de Lusignan S, Van Vlymen J, Klebe B, Middleton R, et al. Chronic kidney disease management in the United Kingdom:
NEOERICA project results. Kidney Int 2007; 72: 92–99.
4. Simon LS, Mills JA. Nonsteroidal antiinflammatory drugs (second of two parts). N Engl J Med 1980; 302: 1237–1243.
5. Garella S, Matarese RA. Renal effects of prostaglandins and clinical adverse effects of nonsteroidal anti-inflammatory agents. Medicine (Baltimore) 1984; 63: 165–181.
6. Sedor JR, Davidson EW, Dunn MJ. Effects of nonsteroidal anti-inflammatory drugs in healthy subjects. Am J Med 1986; 81: 58–70.
7. Clive DM, Stoff JS. Renal syndromes associated with nonsteroidal antiinflammatory drugs. N Engl J Med 1984; 310: 563–572.
8. Lafrance JP, Miller DR. Selective and non-selective non-steroidal anti-inflammatory drugs and the risk of acute kidney injury. Pharmacoepidemiol Drug Saf 2009; 18: 923–931.
9. Perneger TV, Whelton PK, Klag MJ. Risk of kidney failure associated with the use of acetaminophen, aspirin, and nonsteroidal antiinflammatory drugs. N Engl J Med 1994; 331: 1675–1679.
10. Rexrode KM, Buring JE, Glynn RJ, Stampfer MJ, Youngman LD, Gaziano JM. Analgesic use and renal function in men. JAMA 2001; 286: 315–321.
11. Kuo HW, Tsai SS, Tiao MM, Liu YC, Lee IM, Yang CY. Analgesic use and the risk for progression of chronic kidney disease. Pharmacoepidemiol Drug Saf 2010; 19: 745–751.
12. Schneider V, Levesque LE, Zhang B, Hutchinson T, Brophy JM. Association of selective and conventional nonsteroidal antiinflammatory drugs with acute renal failure: A population-based, nested case-control analysis. Am J Epidemiol 2006; 164: 881–889.
13. Gooch K, Culleton BF, Manns BJ, Zhang J, Alfonso H, Tonelli M, et al. NSAID use and progression of chronic kidney disease. Am J Med 2007; 120: 280 e1–7. 14. Hippisley-Cox J, Coupland C. Predicting the risk of chronic Kidney Disease in
men and women in England and Wales: prospective derivation and external validation of the QKidney Scores. BMC Fam Pract 2010; 11: 49.
15. Agodoa LY, Francis ME, Eggers PW. Association of analgesic use with prevalence of albuminuria and reduced GFR in US adults. Am J Kidney Dis 2008; 51: 573–583.
16. Yokoyama H, Sone H, Oishi M, Kawai K, Fukumoto Y, Kobayashi M.
Prevalence of albuminuria and renal insufficiency and associated clinical factors in type 2 diabetes: the Japan Diabetes Clinical Data Management study
(JDDM15). Nephrol Dial Transplant 2009; 24: 1212–1219.
17. Rodriguez-Poncelas A, Garre-Olmo J, Franch-Nadal J, Diez-Espino J, Mundet-Tuduri X, Barrot-De la Puente J, et al. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol 2013; 14: 46.
18. Chen CY, Liu CY, Su WC, Huang SL, Lin KM. Factors associated with the diagnosis of neurodevelopmental disorders: a population-based longitudinal study. Pediatrics 2007; 119: e435–443.
19. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373–383.
20. Chen CY, Liu CY, Su WC, Huang SL, Lin KM. Urbanicity-related variation in help-seeking and services utilization among preschool-age children with autism in Taiwan. J Autism Dev Disord 2008; 38: 489–497.
21. Adams DH, Howie AJ, Michael J, McConkey B, Bacon PA, Adu D. Non-steroidal anti-inflammatory drugs and renal failure. Lancet 1986; 1: 57–60. 22. Pommer W, Bronder E, Greiser E, Helmert U, Jesdinsky HJ, Klimpel A, et al.
Regular analgesic intake and the risk of end-stage renal failure. Am J Nephrol 1989; 9: 403–412.
23. Sandler DP, Burr FR, Weinberg CR. Nonsteroidal anti-inflammatory drugs and the risk for chronic renal disease. Ann Intern Med 1991; 115: 165–172.
24. Kurth T, Glynn RJ, Walker AM, Rexrode KM, Buring JE, Stampfer MJ, et al. Analgesic use and change in kidney function in apparently healthy men. Am J Kidney Dis 2003; 42: 234–244.
25. Detournay B, Simon D, Guillausseau PJ, Joly D, Verges B, Attali C, et al. Chronic kidney disease in type 2 diabetes patients in France: prevalence, influence of glycaemic control and implications for the pharmacological management of diabetes. Diabetes Metab 2012; 38: 102–112.
26. van der Meer V, Wielders HP, Grootendorst DC, de Kanter JS, Sijpkens YW, Assendelft WJ, et al. Chronic kidney disease in patients with diabetes mellitus type 2 or hypertension in general practice. Br J Gen Pract 2010; 60: 884–890.
Table 1. Demographic and clinical characteristics of NSAIDs* use in T2DM study
subjects
Characteristic Total studysubjects (N=57,463) Subjects taking NSAIDs ≥ 90 days (N=6,580) Subjects taking 90 days>NSAIDs>0 day (N=31,189)
Subjects not taking any NSAIDs (N=19,694) P Demographic characteristics Age (years; n, %) 20-29 918 (1.60) 19 (0.29) 570 (1.83) 329 (1.67) <.001 30-45 6,640 (11.56) 318 (4.83) 4,079 (13.08) 2,243 (11.39) 46-60 20,256 (35.25) 1,588 (24.13) 12,078 (38.73) 6,590 (33.46) 61-75 20,069 (34.93) 3,142 (47.75) 10,662 (34.19) 6,265 (31.81) > 75 9,580 (16.67) 1,513 (22.99) 3,800 (12.18) 4,267 (21.67) Sex (n, %) Males 28,619 (49.80) 2,575 (39.13) 14,833 (47.56) 11,211 (56.93) <.001 Females 28,844 (50.20) 4,005 (60.87) 16,356 (52.44) 8,483 (43.07) EC (n, %)* I 4,728 (8.23) 451 (6.85) 2,583 (8.28) 1,694 (8.60) <.001 II 15,028 (26.15) 1,256 (19.09) 8,572 (27.48) 5,200 (26.40) III 24,892 (43.32) 3,125 (47.49) 13,979 (44.82) 7,788 (39.55) IV 12,815 (22.30) 1,748 (26.57) 6,055 (19.41) 5,012 (25.45) Geographical area (n, %) Northern 24,266 (42.23) 2,561 (38.92) 12,904 (41.37) 8,801 (44.69) <.001 Central 13,642 (23.74) 1,796 (27.29) 7,365 (23.61) 4,481 (22.75) Southern 16,317 (28.40) 1,694 (25.74) 9,218 (29.56) 5,405 (27.44) Eastern 3,238 (5.63) 529 (8.04) 1,702 (5.46) 1,007 (5.11) Clinical characteristics Medical comorbidities (n, %) CVD* 9,392 (16.34) 1,580 (24.01) 5,102 (16.36) 2,710 (13.76) <.001 Stroke 6,846 (11.91) 1,017 (15.46) 3,127 (10.03) 2,702 (13.72) <.001 Hypertension 29,618 (51.54) 4,462 (67.81) 16,160 (51.81) 8,996 (45.68) <.001 DM* duration (years; mean ± SD*) 3.96±1.92 4.07±1.93 3.90±1.92 4.01±1.91 <.001
Medication use in past year (n, %)
Insulin 3,842 (6.69) 491 (7.46) 2,000 (6.41) 1,351 (6.86) 0.004 Anti-HT* drugs ACEI/ARB* 20,355 (35.42) 3,005 (45.67) 11,093 (35.57) 6,257 (31.77) <.001 CCB* 18,349 (31.93) 3,023 (45.94) 9,859 (31.61) 5,467 (27.76) <.001 Beta-blocker 15,002 (26.11) 2,510 (38.15) 8,491 (27.22) 4,001 (20.32) <.001 Diuretics 14,833 (25.81) 2,632 (40.00) 7,924 (25.41) 4,277 (21.72) <.001 Statin 13,076 (22.76) 1,799 (27.34) 7,582 (24.31) 3,695 (18.76) <.001 Aspirin 14,294 (24.88) 2,231 (33.91) 7,777 (24.94) 4,286 (21.76) <.001 Acetaminophen 37,593 (65.42) 5,421 (82.39) 22,849 (73.26) 9,323 (47.34) <.001 CCI score* 0 26,497 (46.11) 1,980 (30.09) 14,232 (45.63) 10,285 (52.22) <.001
≥ 3 9,185 (15.98) 1,518 (23.07) 4,619 (14.81) 3,048 (15.48) Mean ± SD* 1.19±1.66 1.61±1.73 1.13±1.54 1.14±1.80 <.001 CKD* development in 2008-2011 (n, %) 3,867 (6.73) 635 (9.65) 2,156 (6.91) 1,076 (5.46) <.001 Observed person-year 166,451 18,727 90,297 57,427 CKD Incidence density per 1,000 (95% CI) 23.23 ( 22.50-23.96 ) 33.91 ( 31.27-36.55 ) 23.88 ( 22.87-24.88 ) 18.74 ( 17.62-19.86 )
Abbreviations: NSAIDs, nonsteroidal anti-inflammatory drugs; EC, enrollee category; CVD, cerebrovascular disease; T2DM, type 2 diabetes mellitus; HT, hypertension; ACEI/ARB, angiotensin-converting-enzyme inhibitor/angiotensin II receptor blockers; CCB, Calcium channel blockers; CCI, Charlson comorbidity index; SD, standard deviation; CKD, chronic kidney disease.
Table 2. Association between chronic kidney disease (CKD) and various CKD-related risk factors in subjects with T2DM Variable Crude HR (95% CI) ‡ Age and sex adjusted HR (95%CI) § Adjusted HR (95%CI) ||
NSAIDs use
None* Ref Ref Ref
1-89 days 1.27 (1.18 - 1.37) † 1.41 (1.31 - 1.51) 1.29 (1.20 - 1.40) >=90 days 1.81 (1.64 - 2.00) 1.74 (1.58 - 1.92) 1.52 (1.38 - 1.69) Age 1.02 (1.02 - 1.03) 1.02 (1.02 - 1.03) 1.02 (1.01 - 1.02) Sex 1.12 (1.05 - 1.19) 1.18 (1.11 - 1.26) 1.31 (1.23 - 1.40) Hypertension 1.91 (1.78 - 2.04) 1.69 (1.58 - 1.81) 1.46 (1.36 - 1.57) CVD 1.59 (1.48 - 1.71) 1.39 (1.28 - 1.49) 1.14 (1.05 - 1.24) Stroke 1.39 (1.28 - 1.52) 1.13 (1.04 - 1.24) 0.97 (0.88 - 1.06) CCI score 1.41 (1.32 - 1.51) 1.27 (1.19 - 1.36) 1.06 (0.98 - 1.14) Insulin use 2.32 (2.12 - 2.54) 2.35 (2.14 - 2.57) 1.94 (1.76 - 2.13) Anti-HT drugs ACEI/ARB 2.04 (1.91 - 2.17) 1.87 (1.75 - 1.99) NA¶ CCB 1.77 (1.66 - 1.89) 1.58 (1.48 - 1.69) NA¶ Beta-blocker 1.53 (1.43 - 1.63) 1.47 (1.38 - 1.57) NA¶ Diuretics 2.17 (2.04 - 2.32) 1.97 (1.84 - 2.10) NA¶ Statin use 1.46 (1.37 - 1.57) 1.49 (1.39 - 1.59) 1.25 (1.17 - 1.34) Aspirin use 1.59 (1.49 - 1.70) 1.40 (1.31 - 1.50) 1.06 (0.98 - 1.14) Acetaminophen use 1.25 (1.17 - 1.34) 1.30 (1.21 - 1.39) 1.08 (1.00 - 1.16)
* Subjects not taking any NSAIDs were used as the reference group. † p value < 0.05 is bold.
‡ Crude hazard ratio.
§ Only adjusted for age and gender.
|| Variables included in the multivariate proportional regression hazards model: NSAIDs use, age, sex, geographical area, EC, hypertension, CVD, stroke, T2DM duration, CCI score (excluding moderate or severe renal disease and diabetes), and use of insulin, statin, aspirin or acetaminophen.
Table 3. Risk of chronic kidney disease with use of NSAIDs in subjects with T2DM
Crude HR (95% CI) ‡ Age- and Sex-adjusted HR (95% CI) § Adjusted HR (95% CI) ||
Number of NSAIDs use days during one year
Subjects without taking any NSAIDs* Ref Ref Ref
Subjects taking NSAIDs for 1-89 days 1.27 (1.18 - 1.37) † 1.41 (1.31 - 1.52) 1.28 (1.18 - 1.38)
Subjects taking NSAIDs ≥ 90 days 1.81 (1.64 - 2.00) 1.74 (1.58 - 1.92) 1.47 (1.33 - 1.63) Average defined daily dose (DDD) of NSAIDs use (DDD per day)
DDD/day = 0* Ref Ref Ref
DDD/day >0 and ≤1 1.41 (1.30 - 1.52) 1.48 (1.37 - 1.60) 1.31 (1.21 - 1.42) DDD/day > 1 1.32 (1.22 - 1.43) 1.48 (1.36 - 1.61) 1.32 (1.22 - 1.44) Cumulative DDD of NSAIDs use during one year (cumulative DDDs)
Cumulative DDDs = 0* Ref Ref Ref
Cumulative DDDs >0 and ≤15 1.23 (1.13 - 1.34) 1.37 (1.26 - 1.50) 1.26 (1.15 - 1.37) Cumulative DDDs >15 1.46 (1.35 - 1.58) 1.56 (1.44 - 1.68) 1.35 (1.25 - 1.47)
* Subjects not taking any NSAIDs were used as the reference group. † p value < 0.05 is bold.
‡ Crude hazard ratio.
§ Only adjusted for age and gender.
|| Adjusted covariates include: age, sex, geographical area, EC, hypertension, CVD, stroke, T2DM duration, CCI score (excluding moderate or severe renal disease and diabetes), anti-HT drugs, and use of insulin, statin, aspirin or acetaminophen.
Figure 2. Risk of chronic kidney disease with NSAIDs use in subjects with T2DM, stratified by age, sex, hypertension, CVD and stroke, CCI score, and medication use of ACEI/ARB, aspirin and acetaminophen, respectively.
Abbreviations: NSAIDs, nonsteroidal anti-inflammatory drugs; CVD, cerebrovascular disease; DM, diabetes mellitus; CCI, Charlson comorbidity index; ACEI/ARB, angiotensin-converting-enzyme inhibitor/angiotensin II receptor blockers. NSAIDs use was classified by: a) number of NSAIDs-use days during one year; b) average defined daily dose (DDD) of NSAIDs use (DDD per day); and c) cumulative DDD of NSAIDs use during one year (cumulative DDDs). Adjusted covariates include: age, sex, geographical area, EC, hypertension, CVD, stroke, T2DM duration, CCI score (excluding moderate or severe renal disease and diabetes), insulin use, anti-HT drug, and use of insulin, statin, aspirin or acetaminophen.