行政院國家科學委員會專題研究計畫 成果報告
裝置體外膜氧合之病人其細胞激素與預後之關係
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-002-239- 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院外科 計畫主持人: 柯文哲 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 92 年 10 月 7 日
Prognostic Predictors in Extracorporeal Membrane Oxygenation
Treatment
Wen-Je Ko, MD, Yih-Sharng Chen, MD, Robert J. Chen, MD, MPH, Ching-Yuang
Lin, MD*
From the Department of Surgery, National Taiwan University Hospital; and the
Department of Pediatrics, Taipei Veteran General Hospital*, Taipei, Taiwan
Running title: prognostic predictors in ECMO treatment
This study is funded by grant NSC 90-2314-B-002-428 from Taiwan National Science
Council
Address for reprints: Ching-Yuan Lin, MD, Department of Pediatrics, Taipei Veteran
General Hospital, Taipei, Taiwan
Corresponding author: Wen-Je Ko, MD, Department of Surgery, National Taiwan
Tel: 886-2-23123456 ext 3098
Abstract
Objective: The outcome of extracorporeal membrane oxygenation (ECMO) treatment
is always unpredictable when it is not indicated for neonatal respiratory diseases. A
prospective study was conducted to collect clinical, biochemical, immunological
parameters at variable times during an ECMO course to determine which factors
influenced ECMO outcome.
Methods: The patients’ demography, pre-ECMO conditions, biochemistry,
hematology, and arterial blood gas analysis during ECMO treatment, were recorded
along with the duration, outcome and complications of the treatment. Blood was
collected on the 3rd and 6th days after initiation of ECMO for cytokines study.
Results: Fifty patients who were receiving ECMO for acute cardio/pulmonary failure
were studied; 32 were male, and 18 were female. Their ages ranged from 20 days to
84 years; their body weights ranged from 2.4 kg to 95 kg. ECMO was set up in
operation rooms (n=20), intensive care units (n=18), cardiac catheterization rooms
(n=3), emergency rooms (n=3), and outside hospitals (n=6). The indications of
ECMO treatment included postcardiotomy cardiogenic shock (n=27), acute
myocarditis (n=5), myocardial infarction that required resuscitation (n=7),
cardiomyopathy with cardiogenic shock (n=2), acute respiratory distress syndrome
ECMO. The etiologies of mortality included extremely poor heart function (n=5),
severe shock damage (n=5), and uncontrollable bleeding (n=1). Three patients died of
brain death due to ECMO mechanical failure (n=1) or intracranial hemorrhage while
on the ECMO (n=2). Sixteen patients underwent a successful ECMO treatment, but
three of them died suddenly months later. Only 2 of 16 successful ECMO patients
needed ECMO support for more than five days. The ECMO treatment of 20 patients
failed and the patients died of multiple organs failure whether or not they were
weaned off ECMO. Comparing instances of successful ECMO with those of failed
ECMO by multiple logistic regression, revealed that three independent factors, acute
renal failure at the time of ECMO set-up, sepsis during ECMO, lower IL-12 serum
level on the 3rd day, predicted a failed ECMO treatment.
Conclusion: ECMO is an ideal rescue treatment for acute cardio/pulmonary failure,
but a successful ECMO treatment requires the following: 1. Acute cardiopulmonary
failure treated by ECMO must be rapidly reversible. ECMO is not intended for
prolonged treatment. 2. No severe shock damage must have occurred due to
underlying diseases before ECMO support is begun. 3. No complications can occur
during ECMO.
Key word: extracorporeal membrane oxygenation, prognosis, acute renal failure,
Ultramini-abstract
Extracorporeal membrane oxygenation (ECMO) provides an ideal rescue
treatment for acute cardio/pulmonary failure in critical patients. However, extremely
poor heart function, very severe shock damage, and uncontrollable bleeding are
contraindications of ECMO treatment. In those patients expected to benefit from
ECMO treatment, acute renal failure at the time of ECMO set-up, sepsis during
ECMO, and lower IL-12 serum level on the 3rd day predict the failure of ECMO
Although extracorporeal membrane oxygenation (ECMO) treatment has been
primarily used for neonatal respiratory disease, 1 the number of patients undergoing
such treatment has recently decreased because of new developments in surfactant
therapy, NO inhalation, high frequency oscillatory ventilation, etc. 2 However, ECMO
has become an ideal rescue treatment for acute cardiopulmonary failure in critical
patients due to newly designed ECMO, including an improved vascular cannula,
centrifugal pumps, microporous membrane oxygenators, heparin bound Carmeda
bioactive surface and other developments. In fact, the use of ECMO in patients with
circulatory collapse is increasing. 1
Under current constraints on increasing medical costs, the cost of any expensive
treatment must be justified. However, the outcome of ECMO treatment is always
unpredictable especially when it is applied to critical patients. This prospective study
evaluates the outcome of ECMO treatment of acute cardiopulmonary failure with
different etiologies and collects clinical, biochemical, and immunological parameters
at various times during ECMO treatment to determine which factors influenced
ECMO outcome. More thoroughly understanding prognostic predictors of ECMO
treatment can improve the success rate of ECMO treatment and make ECMO
Patients and methods
All patients who received ECMO support at the surgical department of National
Taiwan University Hospital from October 2000 to September 2001 were prospectively
enrolled in this study. ECMO has been employed for different extended indications in
this hospital, including temporary support of non-heart-beating donors, 3 rescuing
patient from acute massive pulmonary embolism, 4 replacing a cardiopulmonary
bypass required in some operations of lung transplantations 5 and giant intracranial
aneurysm 6. After these extended ECMO indications had been excluded, 50 patients
were included in this study.
The ECMO used was CB2505 (for patients with body weight ≧12 kg) or
CB2503 (for pediatric patients with body weight < 12kg), both from Medtronic Inc.,
Anaheim, CA, USA. The ECMO was composed of a centrifugal pump, and a
microporous membrane oxygenator with an integrated heater. The entire ECMO
system, including cannula, had a heparin bound Carmeda bioactive surface. A
reflectance photometer (MX-2, Medtronic Inc., Anaheim, CA) was attached to the
pre- and post-oxygenator circuit to monitor continuously blood oxygen saturation and
hematocrit. ECMO priming, the cannulation technique, anticoagulation protocol,
intensive care protocol, and ECMO weaning are described elsewhere. 7
ECMO, pre-ECMO inotrope equivalent (IE, see note in Table 2), pre-ECMO blood
lactate level, CPR before/during ECMO set-up, location of and route through which
ECMO was established, ECMO duration, sepsis before ECMO set-up, sepsis during
ECMO or within one week after the patient was weaned off ECMO (definition of
sepsis: positive microorganism culture present in theoretically sterile area, for
example, blood, pericardial cavity, pleural cavity; fever >38.5℃, blood WBC count >
15,000/mm3 with shift to left in the differential count; clinical diagnosis of pneumonia
or severe wound infection), acute renal failure requiring dialysis at ECMO set-up or
later in the course, and the outcome and any complications of ECMO treatment.
Arterial blood gas, hematology, serum biochemistry, including CK, CK-MB, AST, Bil,
lactate, BUN, and Cr, were checked at least daily during ECMO treatment. Our
previous study showed that ECMO survival patients could usually be weaned off
ECMO after 4 to 6 days of ECMO support. 7 This study aimed to find which
immunological factors on the 3rd day following initiation of ECMO predicted
successful ECMO treatment, and which immunological factors on the 6th day were
associated with ECMO treatment failure. Ten mL of blood were taken on the 3rd and
6th days to measure both the serum levels of proinflammatory cytokines, including
IL-6, IL-8, IL-12, IL-17, IL-18, TNF-α, INF-γ, RANTES, MCP-1, and the total
IL-18 was measured by Sandwich ELISA test (Hayashibara Biochemical Labs.,
Inc) and IL-6, IL-8, IL-12, IL-17, RANTES, MCP-1, TNF-α, INF-γwere measured
by Sandwich ELISA test (R & D System Inc, MN, USA). The concentrations of the
total serum nitrite and nitrate were measured by colorimetric method (OXIS
International Inc, OR, USA) to reveal nitride oxide production. This study was
reviewed and funded by the Taiwan National Science Council.
Statistical analysis:
Numerical variables were tested by the Mann-Whitney U test, and categorical
variables were tested by Fisher’s exact test. Results at P<0.05 were considered
Results
ECMO treatment for different diseases:Thirty-two (64%) patients were male, and 18 were female. Their ages ranged
from 20 days to 83.9 years with a median of 21.6 years. Their body weights ranged
from 2.4 kg to 95.0 kg with a median of 50.0 kg. ECMO was set up in operation
rooms for 20 patients, in intensive care units for 18, in cardiac catherization rooms for
3, in emergency service rooms for 3, and in outside hospitals for 6.
For those 6 patients at outside hospitals, we sent a team to the outside hospitals and
set up ECMO there, and then transferred the patients under ECMO support to our
hospital. Fifteen patients (30%) underwent ECMO for extracorporeal
cardiopulmonary resuscitation (ECPR) while cardiac massage and epinephrine
injection were being performed. Six of these 15 patients were weaned off ECMO and
one was bridged to a centrifugal pump left ventricular assist device (VAD), but only 3
patients survived to discharge from hospital. After ECPR, brain death was noted in 3
patients; and a mild neurological defect was noted in 1 patient who, however,
recovered later. Two ARDS patients received only VV-ECMO. Two ARDS patients
received VA-ECMO initially, and were then shifted to VV-ECMO after the
hemodynamics became stable. All other 46 patients in this study received only
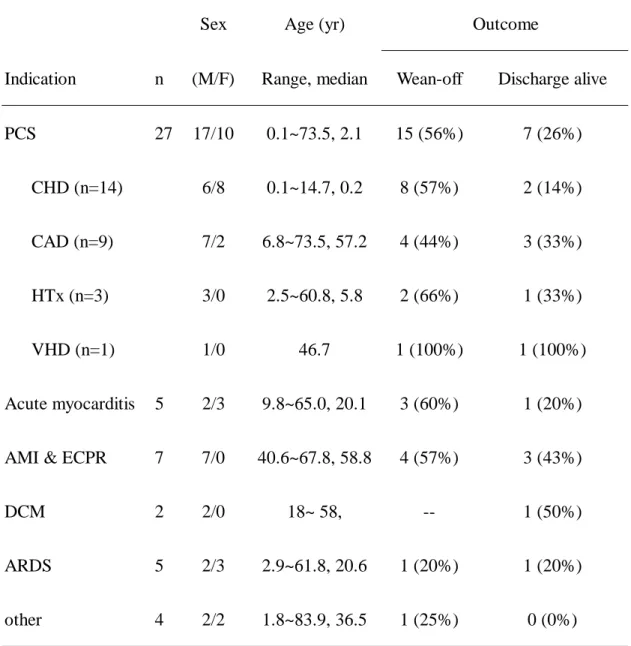
Table 2 shows indications and outcomes of ECMO treatment. Postcardiotomy cardiogenic shock (PCS) was the most common indication of ECMO support. Two cases of PCS also involved respiratory failure, and ECMO was used to support both heart and lung. Fourteen patients required ECMO for PCS following operations for congenital heart defects, 8 of them could be weaned off ECMO but only 2 survived to hospital discharge. Six patients weaned off ECMO but died in the hospital due to sepsis (n=2), intracranial hemorrhage complicated by brain death (n=1), and sudden death (n=3, 39, 79, 115 days after ECMO wean-off).
Five patients received ECMO for acute myocarditis. One of them had
mycoplasma myocarditis and encephalitis, and the other 4 patients had viral
myocarditis. Brain death was noted in two patients following ECPR by ECMO, and in
one patient following CPR due to ECMO mechanical failure. One patient was
successfully weaned off ECMO but died of acute cholecystitis and uncontrolled sepsis
28 days after ECMO was removed.
Seven patients suffered acute myocardial infarction complicated with cardiogenic
shock, and all of them received ECMO for ECPR. Two of them received percutaneous
transcoronary angioplasty under ECMO support. One was weaned off ECMO but
none survived to hospital discharge. Five received an emergent coronary artery bypass
grafting under ECMO support. Three were weaned off ECMO and survived to
hospital discharge.
Two patients received ECMO for circulatory collapse due to dilated
cardiomyopathy. One was bridged to HeartMate left VAD and finally underwent heart
other patient required ECMO for ECPR, and hypoxic encephalopathy and acute renal
failure were found after resuscitation. Although the patient was bridged to a
centrifugal pump left VAD, he later died of multiple organ failure (MOF).
Five patients underwent ECMO for acute respiratory failure. The only case of
survival was a kyphoscoliosis patient with pneumonia alone. Four other patients who
died, had systemic diseases other than pneumonia alone. A patient with Wegener’s
granulomatosis suffered acute renal failure and lung hemorrhage complicated with
pneumonia. A liver transplant recipient had pneumonia soon after transplantation.
Two patients had pneumococcal pneumonia with septic shock.
Four patients received ECMO for various indications. The indications included a
pulmonary hypertension crisis in a liver transplant recipient who had undergone an
elective operation for chronic parasinusitis, acute occlusion of a modified
Blalock-Taussig shunt in a patient with Tetralogy of Fallot; circulatory collapse due to
choking, and lung hemorrhage as an operative complication in a patient with a large
chest wall tumor.
Outcome of ECMO treatment:
Eleven patients (22%) died on ECMO support within 48 hours following initiation of ECMO. Five patients presented extremely poor cardiac function. The combined cardiac output of patients’ native hearts and ECMO were not enough to support patients, and the patients died of circulatory
insufficiency. Five patients suffered brain death, anuria or oliguria, disseminated intravascular coagulation, and other problems, due to CPR before/during ECMO set-up, and soon died of severe shock damage. One patient died of uncontrollable lung hemorrhage due to an operative complication. This study noted brain death in at least 10 patients. Etiologies of brain death included ECPR (n=3), ECMO mechanical failure (n=1), intracranial hemorrhage (n=2), and pre-ECMO CPR (n=4).
Thirty-nine patients survived ≧ 3 days following initiation of ECMO support. A
case of acute myocarditis had a complication of ECMO mechanical failure. Brain
death was noted after the event, and might have been caused by a thromboembolism
from the circuits or CPR itself during emergent ECMO change. Two patients suffered
intracranial hemorrhage and brain death while on the ECMO support for PCS. One
was a one-month-old, 2.5 kg male infant, and the other was a three-month-old, 4.1 kg
female infant. ECMO was terminated and the patients died. These three patients died
of direct complication of ECMO treatment, and they were therefore not included in
the biochemistry and cytokine study.
Thirteen patients were weaned off ECMO support and survived to hospital
discharge. Another three patients were weaned off ECMO and presented no evidence
of MOF at the time of ECMO removal. However, the patients showed symptoms of
congestive heart failure, and sudden cardiac death occurred 39, 79,and 115 days after
ECMO removal. Mortality was unrelated to the ECMO event, and so ECMO
treatment was successful in these 3 patients. The above 16 patients were considered to
ECMO support for more than 5 days. One was a heart transplant recipient, who had
primary graft dysfunction manifest in the right heart failure and required ECMO
support for 221 hours. The other patient was a case of ARDS, and required ECMO for
594 hours.
Nine patients were weaned off ECMO support but showed evidence of MOF at
the time of ECMO removal. They died of MOF 17±14 days following removal of
ECMO. Eleven patients could be not weaned from ECMO and died of MOF while on
ECMO support. These 20 patients were considered to be “failed ECMO patients”. We
compared demography, pre-ECMO condition, biochemistry and some clinical data
between the successful ECMO patients and failed ECMO patients in Table 2.
Prognostic predictors of ECMO outcome:
An attempt was made to identify the indicators of shock damage that predicted the
outcome of ECMO treatment. However, pre-ECMO IE, pre-ECMO blood lactate
levels, CPR, peak CK, CK-MB, and AST levels in the first 3 days, and peak Bil,
maximum WBC count, minimum platelet count in the first week, were not different
between the successful ECMO patients and failed ECMO patients. Only the variable
“acute renal failure at the time of ECMO set-up” showed a significant difference
and mortality. Variables CK, CK-MB, blood lactate levels on the 3rd day, and CK,
CK-MB, AST levels on the 6th day, differed between the two groups. These variables
indicated persistent damage during ECMO treatment and higher values were
associated with ECMO treatment failure.
Figure 1 shows that the failed ECMO patients had significantly higher serum
levels of IL-18, IL-17, IL-6, IL-8, MCP-1 on the 3rd day, and significantly higher
serum levels of IL-17, Il-6, IL-8, TNF-α on the 6th day than their successful ECMO
counterparts. Persistent elevation of proinflammatory cytokines levels, including
IL-18, IL-17, IL-6, IL-8, TNF-α, and MCP-1, contributed to MOF and subsequent
mortality. Notably, the failed ECMO patients had significantly lower IL-12 serum
levels on the 3rd day than the successful ECMO patients, but higher IL-12 serum level
on the 6th day. This “early-low, late-high” pattern in the IL-12 blood level was
associated with mortality in ECMO patients. To build a model to predict ECMO
outcome, we combined all variables in Table 2 and Figure 1 to perform a logistic
regression analysis. Significant predictors (p<0.2) from simple logistic regression
analyses were selected. With colinearity eliminated, multiple logistic regression was
conducted by backward stepwise selection method. The significant predictors in the
final model were acute renal failure at the time of ECMO set-up (odds ratio=28, 95%
following ECMO removal (odds ratio=5.30, 1.14~24.54, p=0.033), and IL-12 serum
level on the 3rd day (odds ratio=0.95, 0.896~0.999, p=0.049). These results imply that
the presence of acute renal failure at ECMO set-up, sepsis during ECMO, and lower
Discussion
Advantages of use of ECMO in critical patients:ECMO could be applied in different patients with very different ages and body weights. Other forms of mechanical circulatory support like the intra-aortic balloon pump and VAD have limited use in smaller patients. ECMO has two modes. VV-ECMO can replace only lung function. VV-ECMO is enough, if a patient has respiratory failure but has good heart function. VA-ECMO can support both heart and lungs. ECMO support could be applied for acute cardiopulmonary failure due to diverse etiologies. In comparison, VAD can provide only circulatory support. The ECMO design that included a microporous membrane oxygenator and a centrifugal pump enabled rapid priming. Less than 30 min was required to establish the ECMO support in our hospital. Cannulation of peripheral vessels enabled ECMO to be used as a bedside procedure under local anesthesia. In our hospital, all instruments and ECMO parts required for ECMO set-up are packed and put on a cart. When ECMO support was required, a team was sent to the site with the ECMO cart and ECMO was set up there. We could provide emergent ECMO support to patients in operation rooms, intensive care units, cardiac catheterization rooms, emergence service rooms, and even in other hospitals. After ECMO had been set-up, the patient was transported to a special ICU for further care. All these advantages made ECMO an ideal rescue treatment for cardiopulmonary failure in critical patients, and ECPR was made possible by ECMO.
ECMO can stabilize critical patients, and thus allow a physician reasonable time
to decide the next step, which may involve waiting for recovery, heart/lung
transplantation, coronary artery bypass grafting, bridging to more permanent devices
like VAD, or giving-up. This study noted brain death in at least 10 patients, and more
patients were noted to have suffered severe shock damage that made long-term
survival impossible. Further aggressive treatment was omitted in these patients.
unpredictably critical patients.
Limitation of ECMO treatment:
ECMO is not intended for long-term support. Only 2 survival patients in this
study required ECMO support for more than 5 days; one was an ARDS patient, and
the other was a heart transplant recipient. As expected, recovery of the ARDS needed
a longer time. Primary graft dysfunction with the right heart failure has been reported
to need longer ECMO support than ordinary PCS. 8 For other patients, either heart
function recovered, or complications supervened and prevented recovery. Therefore, a
definite treatment plan should be decided early during ECMO.
Eleven patients (22%) died under 48 hours after ECMO support was initiated.
Smedira reported a similar 24% 3-day mortality rate in adult patients who received
ECMO support for heart failure. 9 ECMO can provide only partial circulatory support,
and the combined output of a patient’s native heart and ECMO must suffice to support
that patient. Our previous report showed that ECMO provided 2.53±0.84 L/min blood
flow in adult patients. 7 This amount flow is not enough for an adult patient with a
motionless heart. The patient’s heart must contribute some required cardiac output.
ECMO alone cannot provide full circulatory support, especially in adult patients.
ECMO support. The complications of severe shock damage such as brain death
precluded survival. Although these complications could not be foreseen before
ECMO, their existence led to a poor prognosis and should preclude further aggressive
treatment. ECMO itself, of course, cannot treat uncontrollable bleeding. In a word,
extremely poor heart function, very severe shock damage, and uncontrollable bleeding
are contraindications of ECMO support. Patients with these problems were not good
candidates for ECMO support, because they did not benefit from ECMO treatment. In
fact, a most important complication of ECMO was its abuse or misuse.
Factors that influence ECMO outcome:
In this study, 3 children were successfully weaned off ECMO, but months later
died suddenly. The children presented no evidence of other organ damage except
persistent heart failure post-ECMO. The same finding has been reported in adult
patients who received ECMO support for PCS. 7 Persistent heart failure predicts risk
of sudden death in ECMO-weaned patients. For these patients, arrhythmia
prophylaxis is necessary or early heart transplantation is indicated.
Monocyte/macrophage-derived cytokines such as IL-6, IL-8 and TNF-α appear
to play a pivotal role in local immunological activation, leading to tissue destruction.
10-12 IL-17, secreted only by CD4+
endothelial cells to generate IL-6, IL-8, MCP-1, PGE2, NO and granulocyte-CSF. 13 Additionally, IL-17 sustains the maturation CD34-hematopoietic progenitors into
neutrophils, 11, 12, 14 suggesting that IL-17 plays some role in innate response. 14 IL-18
is a member of the IL-1 cytokine family, and it is produced by macrophages, Kupffer
cells, keratinocytes, fibroblasts, chondrocytes, and osteoblasts. IL-18 directly induces
both IFN-γ production by NK cells and NK cytotoxicity. 15 IL-18 induces cytokine
and chemokine release from neutrophils; upregulates CD11b expression; induces
granule release; and enhances the respiratory burst following exposure to fMLP. 15
Consequently, IL-18 promotes an innate immune response and a Th1 response. 16
These data indicate that IL-18 is important in developing and sustaining inflammatory
pathogenic states. This study found that high levels of serum proinflammatory
cytokines including IL-18, IL-17, IL-6, IL-8 and MCP-1 on the 3rd day increasing to
the 6th day might be associated with a poor prognosis. This indicates that
over-activation of innate immunity may lead to a fatal outcome. IL-12, defined as Th1
cytokines, contributes to inflammation. In an experiment with baboons given an E.
coli injection, a lower peak level of IL-12 was noted in the baboons that received a
lethal E. coli injection than in the baboons that were injected with sublethal amount.
This finding sharply contrasted with higher levels of other cytokines, such as TNF-α,
IL-12 on the 3rd day and a high level of IL-12 on the 6th day were associated with a
fatal outcome of ECMO treatment.
Clinical data, biochemistry tests, and serum cytokines were analyzed in these
patients who were expected to benefit from ECMO. Three independent factors were
found to predict failure of ECMO treatment. These 3 factors were acute renal failure
at the time of ECMO set-up, sepsis during ECMO, and lower IL-12 blood level on the
3rd day following initiation of ECMO. Acute renal failure at ECMO set-up implies
that severe shock damage had occurred before ECMO treatment was begun and this
factor was a good indictor of shock damage to predict a failed ECMO outcome.
Sepsis during ECMO course increased the risk of MOF and thereby reduced the
likelihood of survival. Without ECMO, the patients would have died before the 6th day,
and the increased level of IL-12 on the 6th day might represent a desperate response to
impending death. Therefore, Il-12 blood levels on the 3rd day were more clinically
meaningful. ECMO mortality patients had lower IL-12 but higher levels of other
proinflammatory cytokines on the 3rd day than did their surviving counterparts. In
short, shock damage, sepsis, and immunological dysregulation reduced the likelihood
of successful ECMO treatment in patients with acute cardiopulmonary failure.
Successful ECMO treatment requires the following: 1. Acute cardiopulmonary
failure treated by ECMO must be soon reversible. ECMO is not intended for
prolonged treatment, and it serves only as a temporary partial cardiopulmonary
support until recovery or bridging to other more permanent treatment. 2. No severe
shock damage due to the underlying diseases can have occurred before ECMO
support is initiated. 3. No complications such as mechanical failure, sepsis, or others,
can have occurred during ECMO treatment. An initially low level of IL-12 on the 3rd
day, rebounding to a high level on the 6th day, accompanied with a high level of serum
proinflammatory cytokines including IL-18, IL-17, IL-6, IL-8 and MCP-1 on the 3rd
day increasing to the 6th day may be associated with a poor prognosis. Therefore,
improving the success rate of ECMO treatment requires the following: 1. Good case
selection. 2. Sufficiently early initiation of ECMO support. 3. Intensive ECMO care
Acknowledgements
The authors would like to thank the Taiwan National Science Council for
References
1. ECLS registry report. international summary. Extracorporeal Life Support
Organization 2002 Jan.
2. Hintz SR, Suttner DM, Sheehan AM, Rhine WD, Van Meurs KP. Decreased use
of neonatal extracorporeal membrane oxygenation (ECMO): how new treatment
modalities have affected ECMO utilization. Pediatrics 2000;106:1339-43.
3. Ko WJ, Chen YS, Tsai PR, Lee PH. Extracorporeal membrane oxygenation
support of donor abdominal organs in non-heart-beating donors. Clin Transplant
2000;14:152-6.
4. Hsieh PC, Wang SS, Ko WJ, Han YY, Chu SH. Successful resuscitation of acute
massive pulmonary embolism with extracorporeal membrane oxygenation and open
embolectomy. Ann Thorac Surg 2001;72:266-7.
5. Ko WJ, Chen YS, Lee YC. Replacing cardiopulmonary bypass with
extracorporeal membrane oxygenation in lung transplantation operations. Artif
Organs 2001;25:607-12.
6. Chen YS, Ko WJ, Lin FY, Huang SC, Wang SS, Tu YK. New application of
heparin-bounded extracorporeal membrane oxygenation in difficult neurosurgery.
Artif Organs 2001;25:627-32.
membrane oxygenation support for adult post-cardiotomy cardiogenic shock. Ann
Thorac Surg 2002;73:538-45.
8. Fiser SM, Tribble CG, Kaza AK, Long SM, Zacour RK, Kern JA, et al. When to
discontinue extracorporeal membrane oxygenation for postcardiotomy support. Ann
Thorac Surg 2001;71:210-4.
9. Smedira NG, Moazami N, Golding CM, McCarthy PM, Apperson-Hansen C,
Blackstone HE, et al. Clinical experience with 202 adults receiving extracorporeal
membrane oxygenation for cardiac failure: Survival at five years. J Thorac
Cardiovasc Surg 2001;122:92-102.
10. Hsieh HG, Loong CC, Lui WY, Chen A, Lin CY. IL-17 expression as a possible
predictive paramedter for subclinical renal allograft rejection. Transpl Int
2001;14:287-98.
11. Fossiez F, Djossou O, Chomarat P, Flores-Romo L, Ait-Yahia S, Maat C, et al.
T-cell interleukin-17 induces stromal cells to produce proinflammatory and
hematopoietic cytokines. J Exp Med 1996;183:2593-603.
12. Albanesi C, Cavani A, Girolomoni G. IL-17 is produced by nickel-specific T
lymphocytes and regulates ICAM-1 expression and chemokine production in human
keratinocytes:synergistic or antagonist effects with IFN-γ and TNF-α. J Immunol
13. Antonysamy MA, Fanslow WC, Fu F, Li W, Qian S, Troutt AB, et al. Evidence
for a role of IL-17 in organ allograft rejection: IL-17 promotes the functional
differentiation of dendritic cell prognitors. J Immunol 1999;162:577-84.
14. Witowski J, Pawlaczyk K, Breborowicz A, Scheuren A, Kuzlan-Pawlaczyk M,
Wisniewska J, et al. IL-17 stimulates intraperitoneal neutrophil infiltration through the
release of GROα chemokine from mesothelial cells. J Immunol 2000;165:5814-21.
15. Leung BP, Culshaw S, Gracie JA, Hunter D, Canetti CA, Campbell C, et al. A
role for IL-18 in neutrophil activation. J Immunol 2001;167:2879-86.
16. Xu D, Trajkovic V, Hunter D, Leung BP, Schulz K, Gracie JA, et al. IL-18
induces the differentiation of Th1 or Th2 cells depending upon cytokine milieu and
genetic background. J Immunol 2000;30:3147-56.
17. Jansen PM, van der Pouw Kraan TC, de Jong IW, van Mierlo G, Wijdenes J,
Chang AA, et al. Release of interleukin-12 in experimental Escherichia coli septic
shock in baboons: relation to plasma levels of interleukin-10 and interferon-gamma.
Figure Legend
Figure 1. Comparison of plasma cytokines levels between successful ECMO patients
and failed ECMO patients on the 3rd and 6th days following initiation of ECMO
treatment. Bars represent ± standard error around the mean.
Table 1: indication and outcome of ECMO treatment
Sex Age (yr) Outcome
Indication n (M/F) Range, median Wean-off Discharge alive
PCS 27 17/10 0.1~73.5, 2.1 15 (56%) 7 (26%) CHD (n=14) 6/8 0.1~14.7, 0.2 8 (57%) 2 (14%) CAD (n=9) 7/2 6.8~73.5, 57.2 4 (44%) 3 (33%) HTx (n=3) 3/0 2.5~60.8, 5.8 2 (66%) 1 (33%) VHD (n=1) 1/0 46.7 1 (100%) 1 (100%) Acute myocarditis 5 2/3 9.8~65.0, 20.1 3 (60%) 1 (20%)
AMI & ECPR 7 7/0 40.6~67.8, 58.8 4 (57%) 3 (43%)
DCM 2 2/0 18~ 58, -- 1 (50%)
ARDS 5 2/3 2.9~61.8, 20.6 1 (20%) 1 (20%)
other 4 2/2 1.8~83.9, 36.5 1 (25%) 0 (0%)
AMI: acute myocardial infarction, ARDS: acute respiratory distress syndrome, CAD:
coronary artery disease, CHD: congenital heart disease, DCM: dilated
cardiomyopathy, ECMO: extracorporeal membrane oxygenation, ECPR: extracororeal
cardiopulmonary resuscitation, HTx: heart transplantation, PCS: post-cardiotomy
cardiogenic shock, VHD: valvular heart disease
Successful ECMO (n=16) Failed ECMO (n=20) P Sex (M/F) 12/4 13/7 0.517 Age (yr) 31.6 ±27.3 28.1 ±28.7 0.787 Body weight (kg) 43.7 ±32.2 41.7 ±31.4 0.975 ECMO duration (hr) 116.6 ±135.7 188.9 ±133.5 0.011* Pre-ECMO condition: I.E. 30.3 ±15.0 38.4 ±32.9 0.942
Blood lactate (m mole/L) 10.6 ±5.8 11.9 ±6.2 0.512
CPR (+/-) 6/10 13/7 0.101
ARF at ECMO set-up (+/-) 2/14 16/4 0.000*
Sepsis at ECMO set-up (+/-) 1/15 5/15 0.134
Sepsis during/after ECMO (+/-) 3/13 11/9 0.027*
Peak CK (U/L) 2661 ±2090 26229 ±41483 0.114
Peak AST (U/L) 542 ±828 1731 ±2790 0.279
Peak Bil (mg/dL) 3.7 ±3.0 6.8 ±6.5 0.272
Max WBC count (x103/mm3 ) 15.6 ±6.2 21.3 ±1.1 0.111
Min platelet count (x103/mm3 ) 30.9 ±15.5 23.2 ±13.8 0.107
3rd day after ECMO initiation:
CK-MB (U/L) 65.4 ±73.6 626.0 ±1130.3 0.010*
AST (U/L) 158 ±131 1140 ±2088 0.280
Bil (mg/dL) 2.4 ±1.6 4.7 ±4.2 0.144
Blood lactate (mmole/L) 2.6 ±1.8 5.5 ±4.5 0.011*
Platelet count (x103/mm3 ) 50.5 ±37.3 48.3 ±25.0 0.726
PaO2/FiO2 233 ±133 306 ±180 0.226
6th day after ECMO initiation:
CK (U/L) 942 ±940 12394 ±20146 0.049*
CK-MB (U/L) 23.6 ±12.9 238.7 ±273.4 0.000*
AST (U/L) 160 ±237 394 ±456 0.049*
Bil (mg/dL) 3.6 ±2.6 8.4 ±7.2 0.121
Blood lactate (mmole/L) 2.0 ±1.2 3.4 ±2.7 0.198
Platelet count (x103/mm3 ) 60.3 ±22.6 46.2 ±30.6 0.104
PaO2/FiO2 243 ±149 240 ±200 0.275
ARF: acute renal failure (requiring dialysis), AST: aspartate aminotransferase, Bil: bilrubin,
CK: creatinie kinase, CK-MB: creatine kinase MB fraction, CPR: cardiopulmonary
resuscitation, ECMO: extracorporeal membrane oxygenation, IE: inotrope equivalent
(dosages of dopamine + dobutamine (in mcg/kg/min) + (dosages of epinephrine +
mcg/kg/min) x 15)
Peak CK, Peak AST: the highest value in the first 3 days after initiation of ECMO
treatment
Peak Bil, Max WBC, Min Platelet: the highest and lowest value in the first week after
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 IF N -γ ( pg/ m l) 0 2 4 6 8 1 0 1 2 1 4 1 6 1 8 * TN F-α (p g /m l) F aile d E C M O 0 50 0 10 0 0 15 0 0 20 0 0 25 0 0 30 0 0 35 0 0 40 0 0 45 0 0 * RA NTE S ( p g /ml ) 0 1 0 2 0 3 0 4 0 5 0 * ** IL -17 ( p g /m l) 0 20 0 40 0 60 0 80 0 10 0 0 12 0 0 14 0 0 3rd 6th day * * IL -8 (p g /m l) 0 10 0 20 0 30 0 40 0 50 0 60 0 70 0 80 0 90 0 * IL -1 8 (p g /m l) 0 1 00 2 00 3 00 4 00 5 00 6 00 7 00 * * IL -6 ( p g /m l) 0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 * IL -12 ( pg/ m l) S uccess ful E C M O 0 5 1 0 1 5 2 0 2 5 3rd 6th day NO ( n mo le /m l) 0 50 0 10 0 0 15 0 0 20 0 0 25 0 0 30 0 0 35 0 0 * M C P -1 ( pg/ m l) fig 1.