Open Access
Research article
Influence of social support on cognitive function in the elderly
Shu-Chuan Jennifer Yeh*
1,2
and Yea-Ying Liu
1,3
Address: 1Institute of Human Resource Management, National Sun Yat-sen University, Kaohsiung, Taiwan, 2Institute of Health Care Management, National Sun Yat-sen University, Kaohsiung, Taiwan and 3College of Nursing, Kaohsiung Medical University, Kaohsiung, Taiwan
Email: Shu-Chuan Jennifer Yeh* - [email protected]; Yea-Ying Liu - [email protected] * Corresponding author
social supportelderlycognitionfunctional statusSPMSQ
Abstract
Background: Social support is important in daily activities of the elderly. This study tests the
hypothesis that there is an association between social support and cognitive function among the elderly in a community setting.
Methods: Face-to-face interviews were conducted in a cross-sectional stratified random sample
of 4,993 elderly (≥65 years) city residents. Using multiple regression analysis, we investigated the influence of social support on cognitive function.
Results: 12% were over 80 years old. 53.28% were men. 67.14% were married. Higher Short
Portable Mental Status Questionnaire (SPMSQ) scores (higher score means better cognitive function) were associated with strong social support, as measured by marital status and perceived positive support from friends. Lower cognitive function was associated with older and with female respondents. Only instrumental activities of daily living (IADL) were statistically and negatively related to SPMSQ. Lower functional status was associated with lower cognitive function. Elders with grade school educations had lower SPMSQ scores than did elders with high school educations.
Conclusions: In Taiwan, higher cognitive function in community-living elderly was associated with
increased social support. Life-style management should provide social activities for the elderly to promote a better quality of life.
Background
Social support is important in daily activities for the eld-erly living in community settings, and several studies have provided evidence of an association between social sup-port and cognitive function. A socially engaging lifestyle is correlated with higher cognition scores in both communi-ty and nursing home settings [1,2]. Because social activi-ties provide the challenge of effective communication and participation in complex interpersonal exchanges, social support has been thought to inhibit cognitive decline in the elderly [3].
A longitudinal study from Bassuk & colleagues (1999) found that elderly persons who had no social ties were at increased risk for cognitive decline, compared with those who had five or six social ties [4]. Using frequency of con-tact with friends and colleagues as an indicator for social support, Boult & colleagues found that social support was associated with a reduced risk of developing disability up to 4 years later [5]. Research has also shown that social role involvement and personal control were factors not only in slowing age-related decline in physical health, but also in reducing levels of ADL disability [6]. In a prospec-tive cohort study that followed 1,203 non-demented aged
Published: 30 May 2003
BMC Health Services Research 2003, 3:9
Received: 22 October 2002 Accepted: 30 May 2003 This article is available from: http://www.biomedcentral.com/1472-6963/3/9
© 2003 Yeh and Liu; licensee BioMed Central Ltd. This is an Open Access article: verbatim copying and redistribution of this article are permitted in all media for any purpose, provided this notice is preserved along with the article's original URL.
75 and over for 3 years, Fratiglioni and colleagues (2000) found that a social network reduced the incidence of de-mentia [7].
Except for Fratiglioni et al.'s study, research regarding the cognitive status of the elderly and social support generally has been limited by sample size and by the absence of ad-justment for potential confounders, such as education or health status. Because respondents were usually self-re-ferred, selection bias in data collection has also been present.
The concept of social support has been difficult to meas-ure. Several studies have used proxy indicators such as oc-cupational status to make inferences about the effect of social activities on cognition [8,9]. Some have treated pri-or favpri-orable socioeconomic status as synonymous with social activity in old age [10,11], while others have used composite activity scales as proxies for social engagement [1,4].
Loneliness has also been used to predict mental status, in-cluding depression [12]. However, loneliness is subjective and not synonymous with objective social isolation. A person may live alone with few social contacts and not feel lonely. In contrast, an individual surrounded by oth-ers may report a long-standing sense of loneliness. With respect to the elderly, a discrepancy between the social network and the need for social contact may cause loneli-ness [13–16]. Social contacts and perceived social support from family members, friends and acquaintances are im-portant for fulfillment of different social needs. Although one study indicated that ADL functions were associated with emotional and social loneliness [17], it did not ex-amine the relationship between loneliness and cognitive function.
We examine the effect of social support on cognitive func-tion in a large sample selected to represent a cross-secfunc-tion of the elderly population in Taiwan. By controlling for in-dividual characteristics such as age, gender and health sta-tus, we investigated the association between social support and cognitive function in the elderly.
Methods
Study sample
In October 2000, we used stratified random sampling to collect data from all 11 districts in Kaohsiung City, south-ern Taiwan. An equal interval method randomly selected respondents from each district. Lists of residents ≥ 65 years old were obtained from Resident Registries, which contain the names, addresses, sex and ages of all city resi-dents. The study was approved by the Research Ethics Committee of the Health Department of Kaohsiung City.
All elderly residents ≥ 65 years old living in the Kaohsiung area were included unless they were vegetative, stuporous, semi-comatose, suffering from dementia or other serious psychiatric diseases or had a serious spinal cord injury. In-dividuals with an unknown address or proxy respondents were excluded from final analysis.
Of 106,697 persons listed, a total of 6,367 questionnaires were sent out and from these 4,993 face-to-face interviews were completed successfully by trained registered nurses. The interviewers' training involved both a general intro-duction to survey interviewing and fieldwork techniques and procedures, and a review of the specific aspects of the study for which interviewers were responsible. Inter-rater reliability was measured by intraclass correlation coeffi-cient (ICC) during the training stage. Correlation among raters was 0.827.
82 subjects were represented by proxy interviews with a close acquaintance or family member. Proxy respondents were not asked about self-perceived memory and were re-moved from the final analysis. Forty-six elders with seri-ous psychiatric diseases were excluded. Forty-two elders died prior to the interview, and 742 were never contacted due to a change in residence or an unknown address. Four respondents were diagnosed with dementia during the study period. Seventy-six refused to participate. Over half of the data was missing for 386 respondents. These sub-jects were excluded from the final analysis. Final study sample contained 4,989 respondents with aged ≥ 65 years.
Around 12 percent of the elderly were over 80 years old, 53.28% were men, 67.14% were married, and 18.9% had at least a high school education. These percentages were representative of the overall elderly population in Kaohsi-ung [18]. Although distributions of gender (χ2 = 3.43, p =
.148) and education (χ2 = 5.955, p = .062) in our study
were similar to those of the entire elderly population in Taiwan, marital status (χ2 = 48.432, p < .05) and age
(t-value = 15.26, p < .05) were not.
Measures
Dependent variable
The dependent variable was cognitive status measured by the 10-item Short Portable Mental Status Questionnaire (SPMSQ). The SPMSQ was developed by Pfeiffer to assess mental status of the elderly. We chose SPMSQ to measure cognitive status because its brevity permitted assessment without taxing the endurance and capabilities of the least cognitively fit. Although public health nurses were pre-trained for conducting interviews, their formal neurologic training was not evaluated. However, Welch & West (1999) found that SPMSQ could be accurately applied by persons without formal neurologic training [19]. For all of
these reasons, we chose SPMSQ, even though MMSE has better sensitivity and specificity [20]. MMSE scores are also more easily affected by education, intelligence, age, CVA and social class.
The validity of SPMSQ in a Taiwanese population and in patients with organic brain syndrome has been estab-lished [21–24]. SPMSQ can assess the total range of per-formance from intact functioning despite severe impairment. Respondents were asked the questions and not allowed access to information or objects that might stimulate their memories. This test included 10 questions dealing with orientation, personal history, remote memo-ry and calculations. Correct answers received 1 point each. A summary score was constructed by summing the 10 items, yielding a range from 0 to 10. Internal consistency of SPMSQ scale for this study was 0.98.
Missing items from cognitive tests are generally informa-tive in the measurement of cogniinforma-tive performance [25], and a "don't know" response is generally considered in-correct [11,26]. In this study, missing values in the SPM-SQ were always considered incorrect answers.
Independent variables
Four measures of social support that reflected objective and subjective dimensions were examined. Marital status, measured by one dichotomous variable (married vs. non-married) was chosen because a spouse can be an impor-tant source of emotional and tangible support [27]. Per-ceived positive support from friends was measured by asking the respondent whether he had a good friend with whom to talk. Living alone was measured by one categor-ical variable (yes vs. no). Loneliness was measured by ask-ing respondents to rank this feelask-ing on a 3-point scale: 1 = strong, 2 = some and 3 = little.
Control variables
Social support might be related to SPMSQ because of its association with other factors known to be involved in the aging process. To reduce the possibility of spurious asso-ciations, we selected a set of control variables that have been empirically evaluated with respect to social relation-ships and SPMSQ [28–30].
Socio-economic status
Five socio-demographic variables were used. Age was the difference between date of birth and date of interview. Gender was defined as a dummy variable, with male cod-ed as 0 and female as 1. Religion was categorizcod-ed into 4 dummy variables: Traditional, Christian, Catholic and other, with Buddhist as the reference group. Occupation was classified into 5 dummy variables: blue collar, farmer, professional-administrator, retired and housewife, with white collar as the reference group. Education was
catego-rized into 2 dummy variables: grade school or below and college or above, with high school as the reference.
Functional status
Physical health status might affect social networks and so-cial support, particularly if the interviewee considered dis-ease, disability and self-rated health stressful [31]. Functional status was the ability to perform activities of daily living (ADL) and instrumental activities of daily liv-ing (IADL). Katz index of ADL was used to assess personal self-maintenance (bathing, dressing, toileting, transfer-ring, continence and feeding) on a four-point scale: 0 = in-dependent, 1 = semi-independent on devices (needs assistance by using devices), 2 = semi-independent on persons (needs assistance from persons) and 3 = totally dependent. Total score was produced by summing the scored items, yielding a range from 0 to 18. Internal con-sistency was α = 0.95.
IADL are complex tasks such as traveling, shopping, pre-paring meals, doing housework and handling personal fi-nances [32]. Unlike ADL, which is largely concerned with basic bodily maintenance, IADL deals with the execution of more complicated tasks that have a broad impact in linking social competency and independent living [33,34]. Therefore, IADL might be more useful than ADL in detecting disabilities in an elderly population [32]. Lower functional status has been assumed to limit oppor-tunities for social contact by reducing interactions with family and friends outside the home [35] and by limiting social activities [36].
The self-reported functional status measure asked re-spondents if they were able to perform each IADL on their own: preparing meals, shopping, taking medicine, traveling out of walking distance, managing money or us-ing the telephone. We used a three-point scale to measure the above six items: 0 = independent, 1 = semi-independ-ent on devices (needs assistance by using devices), 2 = semi-independent on persons (needs assistance from per-sons) and 3 = totally dependent. Total score was produced by summing the scored items, yielding a range of 0 to 18. Internal consistency was α = 0.91.
Reported health conditions
An interrelation among health condition variables (Par-kinson's disease, heart disease, hypertension, chronic lung diseases, diabetes and stroke) and psychometric tests, such as SPMSQ, has been suggested. However, research re-garding this interrelation has yielded inconclusive results [37–39]. We included several health conditions as dum-my variables (1 = yes and 0 = no): hypertension, diabetes, vision, hearing, cancer and depression. We did not in-clude dementia as a health condition because of its strong
association with the dependent variable and because of its exclusion from the final analysis.
Analytic plan
Descriptive analyses were conducted to understand the study sample. Differences in SPMSQ were examined with respect to demographic variables. We also investigated the association between SPMSQ scores and all two-level de-mographic and health-related variables by using chi-square test. For multiple groups of demographic variables, one-way analysis of variances (ANOVA) was used to de-tect any differences in variance among groups. Once dif-ferences were confirmed, post-hoc analysis (Scheffe's test) was applied to evaluate specific group differences. Multiple regression was used to regress SPMSQ scores on independent variables (social support) and all covariates to find significant indicators (used α level at 0.05 and 0.01). Initial analyses included age, gender, religion, occu-pation and health-condition variables (e.g., diabetes and hypertension) as covariates to determine the relationship between individual characteristics, functional status, so-cial support and SPMSQ. All analyses used SAS 8e statisti-cal software.
Results
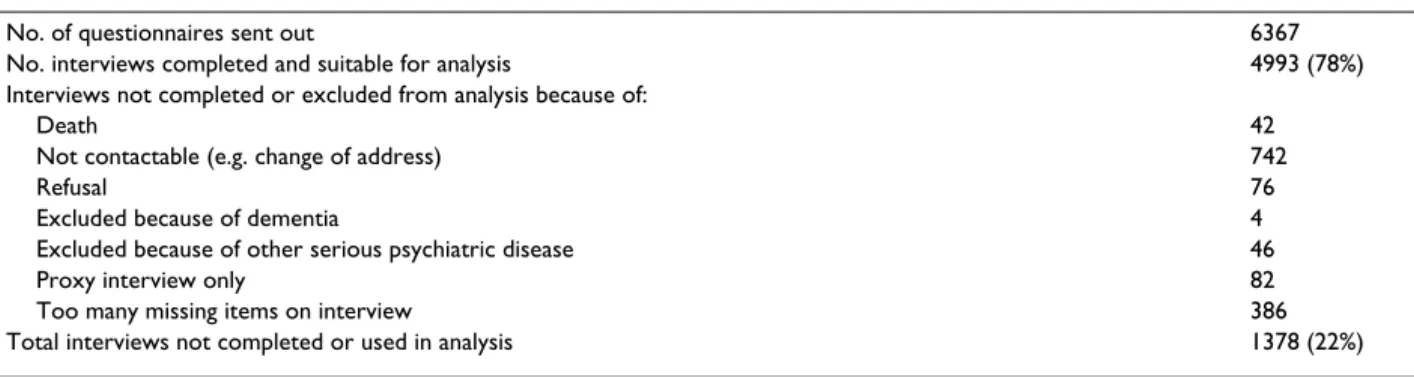
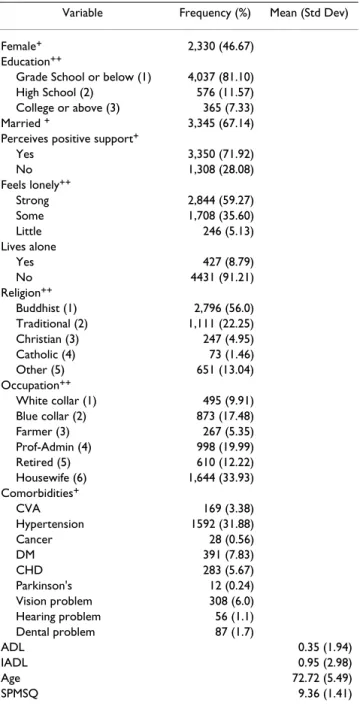
Table 1 describes the response rates of the study sample. We sent out 6,367 questionnaires. 4,993 interviews were valid, and 1,378 were invalid. Response rate was 78%. Summary statistics for the study variables are displayed in Table 2. Mean age of participants was 73 years ± 5.49. Most subjects were married, perceived positive support from friends and felt lonely. 56% were Buddhists (56%). 33.93% were housewives. Around 20% were professional administrators. About 32 percent had hypertension and 0.6% had cancer. Average ADL and IADL scores (range 0– 18) were 0.35 and 0.95, respectively. Mean SPMSQ score was 9.36 (± 1.41), range 0–10.
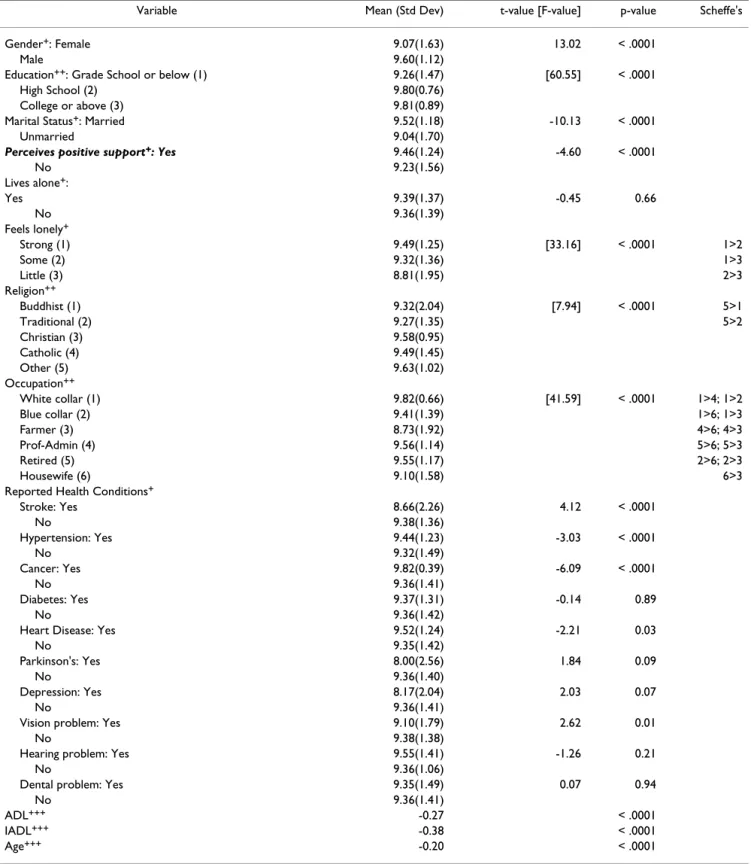
SPMSQ scores were used to measure cognitive function (Table 3). Cognitive function in females was lower than in males. Unmarried elders had lower cognitive function than did married elders. Elderly who perceived positive support from friends had higher SPMSQ scores than those without such a perception. Most covariates showed differ-ences in SPMSQ scores except for the following: living alone, diabetes, Parkinson's disease, depression, hearing and dental problems. Correlations between SPMSQ scores and 3 continuous variables (ADL, IADL and age) were statistically significant.
Regression results showed that higher SPMSQ scores were clearly associated with two groups: married elders (β = 0.13, p = 0.005) and those who perceived positive support from friends (β = 0.11, p = 0.005). Older (β = -0.03, p < .0001) or female (β = -0.38, p < .0001) respondents were more likely to have cognition problems as indicated by lower SPMSQ scores. Cognitive function of respondents who had a grade school education was lower in comparison with those who had a high school education (β = -0.22, p < .001). Compared with white-collar workers, both farmers and blue-collar workers were negatively associated with SPMSQ scores (β = 0.61, p < .0001; β = -0.19, p = .016, respectively). IADL (β = -0.14, p < .0001) was statistically and negatively related to SPMSQ. The as-sociation of ADL with cognitive function was not statisti-cally significant. Two reported health conditions, depression (β = -0.79, p = 0.031) and vision problems (β = -0.19, p = 0.017), were associated with lower cognitive function (lower SPMSQ score). Other factors were not sta-tistically significant. Overall model fit statistic (adjusted R2) was 0.2019 (F = 40.33; p < .0001). Table 4 lists results
for the full regression model.
Discussion
Our study examined primary data collected on an elderly population in Kaohsiung, Taiwan. The relationship between social support and cognitive function indicated that two out of the four measures of social support,
mari-Table 1: Description of sample response rates
No. of questionnaires sent out 6367
No. interviews completed and suitable for analysis 4993 (78%) Interviews not completed or excluded from analysis because of:
Death 42
Not contactable (e.g. change of address) 742
Refusal 76
Excluded because of dementia 4
Excluded because of other serious psychiatric disease 46
Proxy interview only 82
Too many missing items on interview 386
tal status and perceived positive support from friends, were statistically significant. These findings support our hypothesis that social support is an indicator of cognitive function in community-dwelling older adults. We suggest that interventions or activities that enhance social support would improve cognitive functions in the elderly. Living alone and loneliness were not significantly associ-ated with the SPMSQ scores. Our result regarding living
alone is similar to another study that used ADLs, IADLs, cognition and nursing home utilization as outcome indi-cators to investigate whether living alone influenced these outcomes [40]. It was determined that patients living alone after hospitalization were less likely to improve in physical function; however, no relationship with cogni-tive function was found.
Research on the association between loneliness and cog-nitive function is limited. Our results indicate that loneli-ness did not have a statistically significant influence on cognitive function. However, post-hoc analyses using Scheffe's method (Table 3) revealed that elders who felt very alone had higher SPMSQ scores than those who felt less lonely. Studies have indicated that there is a negative relationship between loneliness and social support [17,41,42]. Therefore, we believe that although loneliness can be associated with social support, it cannot predict all perspectives of mental status, including cognitive function.
Cognitive function was correlated with functional status in ways consistent with available knowledge. Because physical function may confound the association of social support and cognitive status, we controlled for ADL and IADL in the model. We found that functional status, par-ticularly IADL, may have substantial impact on cognitive function (with partial R-square = 0.14, F-value = 699.48, p-value < .0001).
In summary, this study used data from a representative elderly community sample of substantial size in Taiwan. Respondents were not self-referred, thereby reducing re-ferral bias. Our results confirm the findings of two earlier studies that found a positive association between social support and cognitive function [1,3]. In our study, mar-riage and perceived positive support from friends were sig-nificantly and positively associated with cognitive function. Loneliness and living alone were not significant-ly associated with cognitive function.
Limitations
This and other similar studies are limited because the SPMSQ score (the only cognitive measure available for this analysis) may provide only attenuated information on memory and does not optimally detect mild cognitive deficits [29]. Some respondents who seemed cognitively intact may have been suffering from early-stage dementia [4]. Perhaps a more sophisticated neuropsychological test would be better measure for evaluating the relationship between cognition function and social support.
Although our study has a substantial representative sam-ple, it is not a longitudinal study. Variables measured at a single point in time tend to be related more than those
Table 2: Descriptive analyses for Kaohsiung elderly (n = 4,993) Variable Frequency (%) Mean (Std Dev)
Female+ 2,330 (46.67)
Education++
Grade School or below (1) 4,037 (81.10) High School (2) 576 (11.57) College or above (3) 365 (7.33) Married + 3,345 (67.14)
Perceives positive support+
Yes 3,350 (71.92) No 1,308 (28.08) Feels lonely++ Strong 2,844 (59.27) Some 1,708 (35.60) Little 246 (5.13) Lives alone Yes 427 (8.79) No 4431 (91.21) Religion++ Buddhist (1) 2,796 (56.0) Traditional (2) 1,111 (22.25) Christian (3) 247 (4.95) Catholic (4) 73 (1.46) Other (5) 651 (13.04) Occupation++ White collar (1) 495 (9.91) Blue collar (2) 873 (17.48) Farmer (3) 267 (5.35) Prof-Admin (4) 998 (19.99) Retired (5) 610 (12.22) Housewife (6) 1,644 (33.93) Comorbidities+ CVA 169 (3.38) Hypertension 1592 (31.88) Cancer 28 (0.56) DM 391 (7.83) CHD 283 (5.67) Parkinson's 12 (0.24) Vision problem 308 (6.0) Hearing problem 56 (1.1) Dental problem 87 (1.7) ADL 0.35 (1.94) IADL 0.95 (2.98) Age 72.72 (5.49) SPMSQ 9.36 (1.41)
Table 3: Descriptive analyses for Kaohsiung elderly (n = 4,993)
Variable Mean (Std Dev) t-value [F-value] p-value Scheffe's
Gender+: Female 9.07(1.63) 13.02 < .0001
Male 9.60(1.12)
Education++: Grade School or below (1) 9.26(1.47) [60.55] < .0001
High School (2) 9.80(0.76)
College or above (3) 9.81(0.89)
Marital Status+: Married 9.52(1.18) -10.13 < .0001
Unmarried 9.04(1.70)
Perceives positive support+: Yes 9.46(1.24) -4.60 < .0001
No 9.23(1.56) Lives alone+: Yes 9.39(1.37) -0.45 0.66 No 9.36(1.39) Feels lonely+ Strong (1) 9.49(1.25) [33.16] < .0001 1>2 Some (2) 9.32(1.36) 1>3 Little (3) 8.81(1.95) 2>3 Religion++ Buddhist (1) 9.32(2.04) [7.94] < .0001 5>1 Traditional (2) 9.27(1.35) 5>2 Christian (3) 9.58(0.95) Catholic (4) 9.49(1.45) Other (5) 9.63(1.02) Occupation++ White collar (1) 9.82(0.66) [41.59] < .0001 1>4; 1>2 Blue collar (2) 9.41(1.39) 1>6; 1>3 Farmer (3) 8.73(1.92) 4>6; 4>3 Prof-Admin (4) 9.56(1.14) 5>6; 5>3 Retired (5) 9.55(1.17) 2>6; 2>3 Housewife (6) 9.10(1.58) 6>3
Reported Health Conditions+
Stroke: Yes 8.66(2.26) 4.12 < .0001 No 9.38(1.36) Hypertension: Yes 9.44(1.23) -3.03 < .0001 No 9.32(1.49) Cancer: Yes 9.82(0.39) -6.09 < .0001 No 9.36(1.41) Diabetes: Yes 9.37(1.31) -0.14 0.89 No 9.36(1.42)
Heart Disease: Yes 9.52(1.24) -2.21 0.03
No 9.35(1.42)
Parkinson's: Yes 8.00(2.56) 1.84 0.09
No 9.36(1.40)
Depression: Yes 8.17(2.04) 2.03 0.07
No 9.36(1.41)
Vision problem: Yes 9.10(1.79) 2.62 0.01
No 9.38(1.38)
Hearing problem: Yes 9.55(1.41) -1.26 0.21
No 9.36(1.06)
Dental problem: Yes 9.35(1.49) 0.07 0.94
No 9.36(1.41)
ADL+++ -0.27 < .0001
IADL+++ -0.38 < .0001
Age+++ -0.20 < .0001
1. Higher ADL or IADL scores indicate more functional dependence. 2. +t-statistic used to compare mean SPMSQ scores in 2 groups defined by
dichotomous covariates. 3. ++ANOVA used to test the differences in variance of SPMSQ scores among multiple groups. 4. +++Correlation analysis
measured at different points. Cross-sectional studies can-not establish the direction of an association (cause and ef-fect) [44,45]. Therefore, future research needs to test the causality between social support and cognition function in the elderly by using longitudinal design.
Mean ADL and IADL scores tended to be lower, which meant most of the elders were more independent. Since we lacked the information on ADL and IADL status for the total elderly population in Taiwan, we could not deter-mine whether any difference in functional status existed between our study sample and national data.
We used specifically defined indicators (marital status, liv-ing alone, loneliness or perceived positive support from friends) to make inferences about the effects of social
sup-port on cognition. Although we did not examine in detail the nature of the social interactions, two of our simple measures showed significant associations with cognitive function. Social interactions require varying levels of cog-nitive effort. An earlier study found that active behaviors represented more robust associations with cognition than did passive behaviors [43]. Future research may employ different social-activity constructs to examine these issues. Perceived positive support from friends have been used proxies for social support in USA [46]; however, it has not been validated in Taiwan elderly population. In addition, a 3-point scale for loneliness may not be discriminatory enough to measure loneliness. For future study, the re-vised UCLA loneliness scale may be a better choice. This scale contains 20 questions, each with a 4-point
Likert-Table 4: Multiple regression of SPMSQ scores, social support and characteristics
Variable Coefficients (s.e.) T value P-value
Intercept 12.30(0.29) 42.97 < .0001
Social Support
Married 0.13(0.04) 2.81 0.005
Perceives positive support 0.11(0.04) 2.79 0.005
Feels lonely -0.03(0.03) -1.09 0.276
Lives alone 0.09(0.07) 1.25 0.210
Age -0.03(0.00) -9.40 < .0001
Female vs. male -0.38(0.06) -6.57 < .0001
Education
Grade School vs. High School -0.22(0.05) -4.37 < .0001
College vs. High School -0.05(0.09) -0.58 0.564
Religion
Christian vs. Buddhist 0.16(0.08) 2.01 0.078
Catholic vs. Buddhist 0.04(0.15) 0.26 0.793
Occupation
Farmer vs. white collar -0.61(0.10) -5.88 < .0001
Blue collar vs. white collar -0.18(0.07) -2.40 0.016
Prof-Admin vs. white collar -0.08(0.07) -1.19 0.233
Housewife vs. white collar -0.09(0.09) -1.12 0.264
Retirement vs. white collar -0.11(0.08) -1.37 0.172
ADL -0.01(0.01) -0.56 0.578
IADL -0.14(0.01) -15.35 < .0001
Reported Health Conditions
CVA -0.02(0.11) -0.21 0.835 Hypertension 0.07(0.04) 1.56 0.118 DM 0.02(0.07) 0.26 0.796 CHD 0.11(0.08) 1.30 0.195 Cancer 0.40(0.26) 1.56 0.118 Parkinson's -0.52(0.35) -1.49 0.136 Depression -0.79(0.37) -2.14 0.031 Vision problem -0.24(0.08) -3.16 0.017 Hearing problem 0.23(0.19) 1.21 0.227 Dental problem 0.16(0.15) 1.06 0.287 Adjusted R-square 0.2019 F-value 40.33 < .0001
type answer ranging from never to often. Although this questionnaire was not specifically designed for use with the elderly, its reliability and validity have been reported to have a Cronbach's alpha of 0.96. Factor analysis has in-dicated that it measures emotional as well as social lone-liness. Thus, validation of the suitability of applying the revised UCLA loneliness scale in Taiwan's elderly popula-tion is a subject worthy of future research.
Authors' Contributions
SCY participated in the design of the study, carried out the study, performed the statistical analysis and drafted the manuscript. YYL participated in the design of the study and literature review.
Competing interests
None declared
Acknowledgements
This work was supported by a grant of the National Science Council of Tai-wan, R.O.C.
References
1. Christensen H, Korten A, Jorm AF, Henderson AS, Scott R and Mackinnon AJ Activity levels and cognitive functioning in an
elderly community sample Age Ageing 1996, 25:72-80
2. Langer EJ, Rodin J, Beck P, Weinman C and Spitzer L Environmental
determinants of memory improvement in late adulthood J
Pers Soc Psychol 1997, 37:2003-2013
3. Berkman LF Which influences cognitive function: Living alone
or being alone? Lancet 2000, 355:1291-1292
4. Bassuk SS, Glass TA and Berkman LF Social engagement and
in-cident cognitive decline in community – dwelling elderly persons Ann Intern Med 1999, 131:165-173
5. Boult C, Kane RL, Louis TA, Boult L and McCaffrey D Chronic
con-ditions that lead to functional limitation in the elderly J
Gerontol 1994, 49:M28-M36
6. Mendes de Leon CF, Glass TA, Beckett LA, Seeman TE, Evans DA and Berkman LF Social networks and disability transitions across
eight intervals of yearly data in the New Haven EPESE J
Ger-ontol B Psychol Sci Soc Sci 1999, 54B:S162-S171
7. Fratiglioni L, Wang HX, Ericsson K, Maytan M and Winblad B
Influ-ence of social network on occurrInflu-ence of dementia: a com-munity-based longitudinal study Lancet 2000, 355:1315-1319
8. Beard CM, Kokmen E, Offord KP and Kurland LT Lack of
associa-tion between Alzheimer's disease and educaassocia-tion, occupa-tion, marital status, or living arrangement Neurology 1992, 42:2063-2068
9. Fabrigoule C, Letenneur L, Dartigues JF, Zarrouk M, Commenges D and Barberger-Gateau P Social and leisure activities and risk of
dementia: A prospective longitudinal study J Am Geriatr Soc
1995, 43:485-490
10. Gribbin K, Schaie KW and Parham IA Complexity of life style and
maintenance of intellectual abilities Journal of Social Issues 1980, 36:47-61
11. Zunzunegui MV, Gutierrez P Cuadra, Beland F, Del Ser T and Wolf-son C Development of simple cognitive function measures in
a community dwelling population of elderly in Spain Int J
Ger-iatr PsychGer-iatry 2000, 15:130-140
12. Prince MJ, Harwood RH, Blizard RA, Thomas A and Mann AH Social
support deficits, loneliness and life events as risk factors for depression in old age. The Gospel Oak Project VI Psychol Med
1997, 27:323-332
13. Andersson L Loneliness and perceived responsibility and
con-trol in elderly community residents J Soc Behav Pers 1992,
3:431-443
14. Cutrona CE, Russel DW and Rose J Social support and
adapta-tion to stress by the elderly J Psychol Aging 1986, 1:47-54
15. Jones WH and Moore TL Loneliness and social support IN Lone-liness: Theory, research, and applications (Edited by: Hojat H, Crandall R) Newbury Park, CA: Sage 1986, 145-157
16. Weiss RS Reflections on the present state of loneliness
re-search In Loneliness: Theory, rere-search, and applications (Edited by: Hojat
M, Crandall R) Newbury Park, CA: Sage 1989, 116
17. Bondevik M and Skogstad A The oldest old, ADL, social
net-work, and loneliness West J Nurs Res 1998, 20:325-343
18. Ministry of Interiors 2003, [http://www.moi.gov.tw/W3/stat/topic/
topic403.htm]
19. Welch DC and West RL The Short Portable Mental Status
Questionnaire: assessing cognitive ability in nursing home residents Nursing Research 1999, 48:329-32
20. MacKenzie DM, Copp P, Shaw RJ and Goodwin GM A Comparison
of the Mini-Mental State Examination (MMSE), Abbreviated Mental Test (AMT) and Mental Status Questionnaire (MSQ)
Psychological Medicine 1996, 26:427-430
21. Chen HT Functional assessment: a holistic view of the elderly
care Annual meeting of Taiwan Medical Association, Kaohsiung, Taiwan
1999, 44-45:S3-S4
22. Hsiao SH, Chiu HC and Liu HW A Replication of
Multidimen-sionality of Activities of Daily Living (ADL): on the Elderly in
Southern Taiwan. 1994, 10:449-457
23. Lee MB and Lee YJ A cross-sectional epidemiological study of
psychiatric comorbidity in hospitalized medically ill Chinese
Psychiatry 1990, 4:10-26
24. Lee MB, Lee YJ and Hsu CC Psychiatric disorders in medical
in-patients: prevalence, psychiatric referrals, and risk factors
Chinese Psychiatry 1989, 3:112-123
25. Herzog AR and Wallace RB Measures of cognitive functioning in
the AHEAD study J Gerontol B Psychol Sci Soc Sci 1997, 52:37-48
26. Brayne C, Gill C, Huppert FA, Barkley C, Gehlhaar E, Girling DM, O'Connor DW and Paykel ES Incidence of clinically diagnosed
subtypes of dementia in an elderly population. Cambridge Project for Later Life Br J Psychiatry 1995, 167:255-262
27. Seeman TE and Berkman LF Structural characteristics of social
networks and their relationship with social support in the elderly: Who provides support? Soc Sci Med 1988, 26:737-749
28. Oxman TE and Hull JG Social support, depression, and
activi-ties of daily living in older heart surgery patients J Gerontol B
Psychol Sci Soc Sci 1997, 52B:1-14
29. Pfeiffer E A short portable mental status questionnaire for the
assessment of organic brain deficit in elderly patients J Am
Geriatr Soc 1975, 23:433-441
30. Litwin H Social network type and morale in old age The Gerontol 2001, 41:516-524
31. Sugisawa H, Liang J and Liu X Social networks, social support,
and mortality among older people in Japan J Gerontol 1994, 49:S3-13
32. Sonn U and Asberg KH Assessment of activities of daily living in
the elderly Scand J Rehabil Med 1991, 23:193-202
33. Fillenbaum GG Screening the elderly: A brief instrumental
ac-tivities of daily living measure J Am Geriatr Soc 1985, 33:698-706
34. Hokoishi K, Ikeda M, Maki N, Nomura M, Torikawa S, Fujimoto N, Fukuhara R, Komori K and Tanabe H Interrater reliability of the
physical self-maintenance scale and the instrumental activi-ties of daily living scale in a variety of health professional representatives Aging Ment Health 2001, 5:38-40
35. Bergeman CS, Plomin R, Pedersen NL and McClearn GE Genetic
mediation of the relationship between social support and psychological well-being Psychol Aging 1991, 6:640-646
36. Thompson MG and Heller K Facets of support related to
well-being: Quantitative social isolation and perceived family sup-port in a sample of elderly women Psychol Aging 1990, 5:535-544
37. Woo J, Ho SC, Lau S, Lau J and Yuen YK Prevalence of cognitive
impairment and associated factors among elderly Hong Kong Chinese aged 70 years and over Neuroepidemiology 1994, 13:50-58
38. Scherr PA, Hebert LE, Smith LA and Evans DA Relation of blood
pressure to cognitive function in the elderly Am J Epidemiol
1991, 134:1303-1315
39. Skoog L, Lernfelt B, Landahl S, Palmertz B, Andreasson LA, Nilsson L, Persson G, Oden A and Svanborg A 15-year longitudinal study of
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK Your research papers will be:
available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral 40. Mahoney JE, Eisner J, Havighurst T, Gray S and Palta M Problems of
older adults living alone after hospitalization J Gen Intern Med
2000, 15:611-619
41. Sarason IG, Sarason BR and Sherion EN Social support as an
indi-vidual difference variable: Its stability, origins, and relational aspects J Pers Soc Psychol 1986, 50:845-855
42. Stokes JP and Levin I Gender differences in predicting loneliness
from social network characteristics J Pers Soc Psychol 1986, 51:1069-1074
43. Hultsch DF, Hammer M and Small BJ Age differences in cognitive
performance in later life: Relationships to self-reported health and activity life style J Gerontol 1993, 48:1-11
44. Bowling A Research methods in health: investigating health
and health services Open University Press, Buckingham, Philadelphia
1997,
45. Grady KE and Wallston BS Research in health care settings. Thousand Oaks, California: Sage Publications 1988,
46. Potts MK Social Support and Depression among Older Adults
Living Alone: The Importance of Friends Within and Out-side of a Retirement Community Social Work 1997, 42:348-362
Pre-publication history
The pre-publication history for this paper can be accessed here: