行政院國家科學委員會專題研究計畫 期中進度報告
早產兒早期給予 Dexamethasone 學齡年齡之追蹤評估(1/2)
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-039-036-執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 中國醫藥學院醫學系 計畫主持人: 葉純甫 計畫參與人員: 林毓志、林其和、陳永榮、黃朝慶 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中
華
民
國 92 年 5 月 22 日
行政院國家科學委員會補助專題研究計畫期中進度報
告
School-Age Outcome in Childr en with Ear ly
Postnatal Dexamethasone (D) Ther apy for Pr evention
of CLD of Pr ematur ity
計畫類別:■個別型計畫
□整合型計畫
計畫編號:NSC91-2314-B-039-036
執行期間:91 年 8 月 1 日至 92 年 7 月 31 日(第一年)
計畫主持人:葉純甫
共同主持人:林毓志、林其和、陳永榮、黃朝慶
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:中國醫藥大學 醫學系
中華民國 九十二 年 五 月 三十一 日
I行政院國家科學委員會專題研究計劃期中進度報告
School-Age Outcome in Childr en with Ear ly Postnatal
Dexamethasone (D) Ther apy for Pr evention of CLD of
Pr ematur ity
計劃編號: NSC 89-2314-B006-056
執行期限: 91 年 8 月 1 日至 92 年 7 月 31 日(第一年)
主持人: 葉純甫 中國醫藥大學 醫學系
中文摘要 早產生後投于 Dexamethasone 的治療,沒有長期追蹤的研究,本研究利用早 期研究計劃(Double-blind study of early dexamethasone therapy for prevention of CLD in premature infants)來做學年齡的追蹤研究。 在 158 位小孩中,我們能追蹤到 136 位(87%)─70 位為對照組,66 位為治療 組。他們之間,在週產期間沒有顯著差別(體重 1.35±0.33 vs 1.39±0.36 kg,懷孕 週數 29.3±2.3 vs 30.6±2.4 wks,Apgar score,呼吸器及 RDS 之嚴重度)。治療組 身高較低(122.1±9.3 vs 125.9±6.4 cm P<0.07);頭圍小一些(49.2±3.9 vs 50.6±1.6 cm P<0.08)。治療組的小孩,在身高、體重<3% tile 之比例,比對照組高(25/66 vs 5/70, P<0.05; 21/66 vs 6/70 P<0.05)。治療組有較高的神經運動的問題,他們的 ABC movement score 比對照組高(total impairment score 18.9±13.8 vs 11.9±10.0 P<0.02; Ball skill 4.9±3.9 vs 3.1±2.9, P<0.05, Balance 7.0±6.0 vs 3.8±5.4 P<0.02)。治療組的 智商似乎都比較低 (77±14 vs 85±12)。學校成績二組差不多。我們的結論是,早 期投于 Dexamethasone 來預防早產兒 CLD,可能有不良影響,此種治療方法, 不宜再用。英文摘要
Background: Postnatal D therapy has been used for years. The long-term outcome up to school age has not been completely studied.
Objectives: To study the outcome at school age of infants who were enrolled in a double-blind trial of early (<12hrs) D therapy for prevention of CLD.
Design/methods: Of the 158 children who lived to school age, 136 (86%) were studied (70 control C, 66 D). C and D had comparable birth wt. (mean±SD, 1.35±0.33 vs 1.39±0.36 Kg), gest age (29.3±2.3 vs 30.6±2.4 wks), gender, Apgar score at 1 and 5 min, severity of RDS and initial neonatal outcome (IVH≧GrⅡ: 10 vs 8, CLD 15 vs 8 ). In the D group, 0.25mg Kg q.12.h for 1 wk and then tapered off in 3wk were given. The following variables were assessed at school age (8.22±0.68 vs 8.21±0.63 yrs): physical growth, neuro. exam. movement ABC, cognitive WISC-Ⅲ, school performance (mathematics, language, adaptive behavior), speech, visual and auditory function. II
Results: The D gr. tends to have lower height(122.1±9.3 vs 125.9±6.4cm P=0.07 ), lower head circ. (49.2±3.9 vs 50.6±1.6cm P=0.08) than C gr. More children in D than in C gr. had their height and wt. <3% tile. (25/66 vs 5/70 P<0.01, 21/66 vs 6/70 P<0.05). 20 D and 16 C had sign. neurological abnormalities with motor dysfunction. D gr. had sign. higher movement ABC score (total impairment score 18.9±13.8 vs 11.9±10.0, P<0.02; Ball skill 4.9±3.9 vs 3.1±2.9, 9<0.05; balance 7.0±6.0 vs 3.8±4.5, P<0.02 ) and poorer visual perception than C gr. Cognition WISC-Ⅲ were lower in D than in C gr. in full scale (77±14 vs 85±12 P<0.05) and in performance scale (76±16 vs 84±13 P<0.05). School performance were comparable between the grs. Significant handicap (neuromotor dysfunction + WISC-Ⅲ full scale ≦3% tile ) were seen in 26 D and 19 C.
Conclusion: Postn D therapy may be associated with adverse effects on somatic growth, neuromotor and cognitive function at school age.
Keywords: School-age outcome, Early postnatal dexamethasone therapy, Chronic lung disease
INTRODUCTION
Dexamethasone has been used for years in infants with established BPD. It has recently been used for possible prevention of BPD when the drug was administered very early shortly after birth. In both therapeutic regimens, several immediate side effects including hyperglycemia, hypertension, adrenal suppression, growth delay and alteration of cardiac function have been reported.
The two years follow up studies from ours and these from others suggested a possible neuromotor dysfunction associated with dexamethasone therapy. However. these infants were very sick and had multiple problems at birth, it is impossible to prove this correlation. Furthermore two year follow-up results can not always predict the school age outcome.
There have been no long-term follow up studies up to school age reported in literature. The pervious double-blind study (DOH83-HR-217) (prevention of Chronic Lung Disease of BPD in premature with RDS by early dexamethasone therapy) undertaken in our unit provides a good model for long term follow. The preliminary results of our study suggest that Dexamethasone improve pulmonary ventilation and reduce the lung injuries and incidence of BPD. Based on our therapeutic regimen, the immediate side effects appeared to be less then what have been previously reported. However, since Dexamethasone may cause central nervous system and growth toxicities in various animals, there has been concerns about the long term effect on growth, development and school performance. The purpose of the present study was to investigate the long term
effects of Dexamethasone on physical growth and motor and mental development, and school performance.
Respiratory Distress Syndrome (RDS) continuously to be the most common cause of morbidity and mortality in premature infants and BPD is the most common and significant pulmonary complication in infants surviving from RDS. It has been estimates that about 20-40% of infants with RDS would have certain degree of lung injuries during O2 therapy and mechanical ventilation early in the course of RDS. These infants might eventually develop various degree of BPD. This chronic lung disease of BPD may persist for months or even years. During the course of BPD, the infant may subject to multiple problems, e.g.: frequent respiratory tract infection, under nutrition, growth and developmental delay, right heart failure and cor-pulmonale, sudden infant death etc. However, unlike the chronic Obstructive Pulmonary Disease (COPD) in adult, the lungs in small infant continue to grow and to regenerate so that by certain time in early childhood, the disease of BPD may be completely recovered. It has been estimated that about 7000 new cases of BPD would develop each year in U.S.A. The direct cost for BPD infant, both for the initial and later care each year would be U.S.$. 42 billion. There has been no solid date available on incidence of BPD in Taiwan. Based on a study in a local geographic area in Tainan, we estimate that about 500 BPD infants will be seen each year in the whole Taiwan area; the yearly cost will be about NT$ 500 million. This figure is surely underestimated because it does not include the indirect costs from various sources, not even mention about the
emotional and psychological burden to the family. Thus, prevention or minimizing BPD is essential. The previously study from the principle investigator and studies from others on infants with established BPD strongly indicated that Dexamethasone decreased lung injuries and improved lung function. However, because of various immediate side effects and the possible long-term sequelae, dexamethasone was not generally recommended. Our previous double-blind study supported by National Health Research Institute, indicates that, by modifying the therapeutic regimen, the immediate side effects are much less and yet the dexamethasone effect on the lung is not affected. However, we still don’t know the long term effect with this therapeutic regimen. If we could demonstrate that there is no significant long term adverse effect by using our therapeutic regimen, then we can recommend their routine use for prevention of BPD. This finding is certainly a great contribution to neonatal therapeutics.
A long-term follow-up study up to school age is desperately needed.
METHOD AND MATERIAL
Between July 2002 and June 2004, all infants who were enrolled in a multicenter double-blind controlled study and who survived were included for the follow-up study. All these infants had birth weight < 2000 gm and had RDS and required mechanical ventilation shortly after birth. They were randomized based on a double-blind fashion into two groups: the Dexamethasone treated group and placebo (normal saline) group. In the solution containing Dexamethasone sodium phosphate,
the dosage was:
Day 1-7 0.25 mg /kg/ dose q 12 h Day 8-14 0.125 mg /kg/ dose q 12 h Day 14-21 0.05 mg /kg/ dose q 12 h Day 22-28 0.025 mg /kg/ dose q 12 h
The first does was administered within 12 hour after birth. A standard protocol for the management of infant with RDS was followed by all infants. The protocol emphasized the criteria for initiation and weaning of mechanical ventilation. The fluid intake was adjusted to 80 ml / kg / day in the first postnatal day and increased daily to 150 ml/kg/day and on ward. If the infant was receiving phototherapy, an additional 20% of calculated fluid intake had been given to compensate for the increased insensible water loss. Feeding via nasogastric tube was usually not been attempted during the first week. If adequate caloric in take caned not otherwise be achieved, a free amino acid solution had been administered to make up the deficit. All infants were weighed daily and their intake and urine output were precisely measured. Infants who survived were followed and evaluated at about 7 year of corrected postnatal age and / or at 8 or 9 years of postnatal age for the followings:
1) A Complete Interim Health History and Family History: a complete health history and family history, educational levels, marital status and socioeconomic status, were obtained.
2) A complete physical examination and neurological assessment. At each visit, a complete physical examination was performed, emphasized on weight, occipitofrontal head circumference, and spine crown-heel length measurement was recorded. Each examination was accompanied by
neurological assessment of mental status, motor development (including coordination, general reflex, muscle one), and cranial nerves by a pediatric neurologist. A standard bipolar EEG was obtained that include visual flicker, and stimulation. Auditory and visual evoke potentials will also be measured.
3) Psychometric Evaluation and School Performance. The psychometric testing of the Children include assessments of neuropsychological abilities and academic achievements. These include cognitive abilities (Kaufman assessment). Language, Psychomotor skill for fine, gross and visual motor, memory and attention skill, Academic achievement evaluation include reading, spelling and arithmetic abilities, rating on school performance, rating of behavior, rating of attention problems, adaptive- behavior interview and rating of social skill.
4)Statistical Analysis. We compared the two groups of Children with regard to outcome at early school age. The outcome measures were standardized for age before analysis. Overall differences between groups in continuous measures of outcome were examined by an analysis of variance or a multivariate analysis of variance. The alpha level was set at 0.05 for each domain and Bonferroni adjustment in the alpha level was used in making univariate comparison within multiple-measure domains. Logistic regression was used to assess associations of social and neonatal risk factors with major developmental outcome among the two groups.
RESULTS
As shown in table I. The total number of children included for this follow-up study
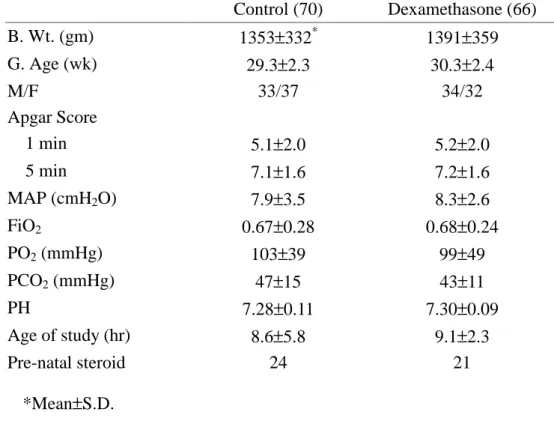
was 136, (87% of the survivals): 70 were in the control group and 66 in the dexamethasone group. The clinical characteristics in the perinatal period are shown in table II. The two groups were comparable is birth caught, gest. age, gender and Apgar score. The two groups were also comparable in mean airway pressure for ventilation, blood gases and acid-base balance. The first dose of dexamethasone was given at a mean postnatal age of 9.1 hours.
The two groups were comparable in socio-economic background in maternal age, education, family income, and marital status of the parents. (Table III) The mean postnatal age at time of follow-up was 8.2 years in the control groups and 8.3 years in dexamethasone group. Birth groups were comparable in incidence of URI/year and blood pressures. (Table IV)
The body weight and height of individual boys and girls were shown in Fig 1 and Fig 2. Dexamethasone groups had significantly smaller mean head circumference than control group (47.9 vs 50.6 cm P<0.05). This is particularly noted in boys (49.7 vs 50.8 cm P<0.05).
The neurological outcome and motor movement assessment are shown in table V. More proportion of children in dexamethasone group had motor and visual motor integration problem. The audiovisual evacuations are shown in table VI. The two groups were reparable.
The genitive functions between the groups are shown in table VII. Children in the dexamethasone group had significantly between IQ than control group in full scale and performance scale.
The school performances are shown in
table VIII. There is no significant difference between the groups.
The incidence of disabilities was higher (P<0.05) in dexamethasone groups (27/66 or 41%) than the control groups (16/70 or 23%) (Fig. 3)
SUMMARY AND CONCLUSION
1) Early postnatal dexamethasone therapy (<12 hours) for one week, taper off in
3 weeks, was associated with significant adverse effects on somatic growth, motor and cognitive function, and with increases of disabilities at school age. This therapeutic regimen should not be recommended.
2) We suggest any therapeutic modality of postnatal use of steroid should be carefully evaluated for their long term side-effects.
Table I.
Control (130) Dexamethasone (132) Died in neonatal period 39 44
Died before school age 13 10 Couldn’t be located 8 12 Number follow-up 70 66 ≤1999 gm IMV <12 hrs 5
Table II. Clinical and Biochemical Char acter istics in the Per inatal Per iod Control (70) Dexamethasone (66) B. Wt. (gm) 1353±332* 1391±359 G. Age (wk) 29.3±2.3 30.3±2.4 M/F 33/37 34/32 Apgar Score 1 min 5.1±2.0 5.2±2.0 5 min 7.1±1.6 7.2±1.6 MAP (cmH2O) 7.9±3.5 8.3±2.6 FiO2 0.67±0.28 0.68±0.24 PO2 (mmHg) 103±39 99±49 PCO2 (mmHg) 47±15 43±11 PH 7.28±0.11 7.30±0.09 Age of study (hr) 8.6±5.8 9.1±2.3 Pre-natal steroid 24 21 *Mean±S.D. 6
Table III. Mater nal Education and Social-Economic Background
Control (70) Dexamethasone (66) Maternal age (yr) 32.8±4.5* 33.2±6.2 Maternal education
Not high school graduate 20 21 High school graduate 36 32
Some college 7 8
College graduate 7 5 Family income (US dollars/y)
<10000 9 9 10000-15000 29 28 15001-30000 22 21 30001-50000 7 7 >50000 3 2 Marital status Married 66 64 Single 0 0 Divorced 4 2 *Mean±S.D. 7
Table IV. Medical Histor y and Physical Examination at School Age Control (70) Dexamethasone (66) Postn-age (yrs) 8.2±0.7* 8.3±0.6 Frequency of URI/yr 6±5 6±6 Blood pressure (mmHg) Systolic 104±8 106±9 Diastolic 61±7 59±8 *Mean±S.D. 8
Table V.
Control (70)
Dexamethasone (66) Gross Neuromotor Dysfunction 14 20 Movement ABC
Manual Dexterity 4.9±3.9* 6.9±4.9 P<0.05 Ball skill 3.1±3.0 4.9±4.0 P<0.02 Balance 3.8±4.0 7.0±6.1 P<0.01 Total impairment score 11.8±10.0 18.9±14.0 P<0.01 <5% tile 13 32 P<0.001 Visual-motor integration Score <75 (<5% tile) 5 15 P<0.02 *Mean±S.D. 9
Table VI. Audiovisual Assessment Control (70) Dexamethasone (66) Vision Normal 39 34 Abnormal 31 32 Ÿ Visual acuity
(≤20/200 at least in one eye)
5 8
Ÿ Blindness 2 1
Hearing impairment
(↓20db at least in one ear)
9 14
Table VII. Cognitive Function (WISC-III) Control Dexamethasone P Full scales 84.4±12.1 78.1±14.0 <0.05 Verbal scales 88.3±12.6 83.8±13.1 Performance scales 84.4±13.2 76.4±15.7 <0.05 11
Table VIII. Academic Per for mance
Control (70) Dexamethasone (66) Special school 8 (11.4%) 10 (15.1%) Reading and Spelling (<5% tile) 4 (5.7%) 6 (9.0%) Arithmetics (<5% tile) 8 (11.4%) 13 (19.6%) Adaptive behavior
Below average 9 (12.8%) 5 (7.6%) Poor 1 (1.4%) 2 (3.0%)
PEFERENCES
1. Alkalay AL, Pomerance JJ, Puri AR, et al. Hypothalamic. pituitary-adrenal axis function in very low birth weight infants treated with dexamethasone. Pediatrics. 1990; 86:2004-210
2. Avery GB, Fletcher AB, Kaplan, M, Brudno DS. Controlled trial of dexamethasone in respirator-dependent infants with bronchopulmonary dysplasia. Pediatrics. 1985;75:106-111
3. Blanco LN, Massaro GD, Massaro D. Alveolar dimensions and number: developmental and hormonal regulatin. Am J Physiol (Lung Cell Mol Physiol). 1989; 257L240-L247
4. Cotterell M, Balazs R. Johnson AL > Effects of corticosteroids on the biochemical maturation of rat brain; postnatal ecll formation. J Neurochem. 1972;19:2151-2167
5. Cummings JJ, d’Eugenio DB, Gross SJ. A controlled trial of dexamethasone in preterm infants at high risk for bronchopulmonary dysplasia. N Eng1 J Med. 1989;3201505-1510
6. Dobbing J, Sands J. Quantitative growth and development of human brain. Arch Dis Child. 1973; 48:757-767
7. Ditzhardinge PM, Eisen A, Lejtenyi c, Metrakos K, Ramsay M. sequelad of early steroid administration to the newborn infant. Pediatrics. 1974;53:877-883
8. Fitzhardinge PM, Page k, Arstikatis M, et al: Mechanical ventilation of infants of less thant 1501 gms birth weight: Health growth and neurological sequelae. J Pediatr 1976;88:531-540
9. Frank L, Groseclose EE. Oxygen toxicity
in newborns: the adverse effects of undernutrition. J Appl Physiol. 1982;53:1248-1255
10. Halpern P, Teitelman U, Lanir A. Effects of methylpredisolone on normobaric pulmonary oxygen toxicity inrats. Respiration. 1985;48:153-158.
11. Hislop AA, Wigglesworth JS, Desal, R, Aber V. The effects of preterm delivery and mechanical ventilation on human lung growth. Early Hum Deve. 1987;15:147-164
12. Howard E, Granoff DM. Increased voluntary running and decreased motor coordination in mice aftr neonatal corticosterone implantation. Exp Neurol. 1968;22:661-673
13. Kazzi NJ, Brans YW, Poland RL. Dexamethasone effects on the hospital course of infants with bronchopulmonary dysplasia who are dependent on artifical ventilation. Pediatrics. 1990;86:72-722 14. Newman JH, Fulkerson WJ, Kobayashi T,
English D, Meyrick B, Brigham KL.Effects of methylprednisolone on lung oxygen tocixity in awake sheep. J Appl Physiol.1986;60:1386-1392
15. Noble-Jamieson CM, Regev R, Silverman M. Dexamethasone in neonatal chronic lung disease: pulmonary effects and intracranial complications. Eur J Pediatr. 1989;148:365-367
16. O’Brodovich HM, Mellins RB. Bronchopulmonary dysplasia:unresolved neonatal actue lung jnjury. Am Rev Respir Dis. 1985:132:694-709
17. Ohtsu N, Ariagno RL, Sweeney TE, et al. The effects of dexamethasone on chronic pulmonary oxygen toxicity in infant mice.
Pediatr Res. 1989;25:353-359
18. Shaffer SG, O’Neil D, Bradt SK, Thibeatult DW. Cronic vascular pulmonary dysplasia associated with neonatal hyperoxia exposure in the rat. Pediate Res. 1987;21:14-20
19. Sobonya RE, Logvinoff MM, Taussig LM, Theriault A. Morphometric analysis of the lung in prolonged bronchopulmonary dysplasia. Pediatr Res. 1983;16:969-972 20. Simth LJ, Brody JS. Influence of
methylprednisolone on mouse alveolar type 2 cell response to actue lung injury. Am Rev Respir Dis. 1981;123:459-464 21. Ulrich R, Yurwiler A, Geller E. Effects
ofhydrocortisone on biogenic amine levels in the hypothalamus. Neuroendocrinology. 1975;19:259-268 22. Weichse ME Jr. The therapeutic use of
glucocorticoid hormones in the perinatal period: potential neurological hazareds. Ann Neurol. 1977;2:364-366
23. Weichsel ME Jr. Glucocorticoid effect upon thymidine kinase in the developing cerebellum. Pediatr Res. 1974;19:2151-2167
24. Yeh TF, Goldbarg H, Pildes RS: Follow-up of premature infants treated with indomethacin. J Pediatri 1981;99:336
Fig.1 Fig. 2 0 10 20 30 40 50 60 70 80 6 7 8 9 10 11 12 13 14 15 (Mean ±S.D.) <10% tile C 3/70 D 11/66 p<0.05 3 10 25 50 75 90 97 Male (6-15 years) Control Dexamethasone 24.7±5.2 kg 23.4 ±5.6 kg (% ti le ) B o d y W t (kg ) Age (year) 1 0 5 1 1 5 1 2 5 1 3 5 1 4 5 1 5 5 1 6 5 1 7 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 1 5 <10% tile C 3/70 D 11/66 p<0.05 Male (6-15 year s) Contr ol Dexamethasone 126.5±6.3 cm 123.3 ±11.6 cm (Mean ±S.D.) P<0.05 H ei g h t ( c m ) (% t il e) 3 10 25 75 50 90 97 Bod y W t (k g ) Age (year) ti le ( % ) H ei g ht ( cm ) Age (year) ti le ( % ) (% t il e) B od y W t (k g) Bod y W t (kg ) tile (%) H e ig ht (cm ) ti le (%) 1516
Fig.3 0 20 40 60 80 100 Control Dexamethasone No disability Disability 54 16 39 23% 41% 27 17