and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
Contents lists available atSciVerse ScienceDirect
European Journal of Radiology
j o u r n a l h o m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / e j r a d
Review
Clinical value of FDG PET or PET/CT in urinary bladder cancer: A systemic review
and meta-analysis
夽
Yu-Yu Lu
a,1, Jin-Hua Chen
b, Ji-An Liang
c,d, Hsin-Yi Wang
a, Cheng-Chieh Lin
d,e, Wan-Yu Lin
a,d,1,
Chia-Hung Kao
d,f,∗aDepartment of Nuclear Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
bBiostatistics Center and Graduate Institute of Biostatistics, China Medical University, Taichung, Taiwan cDepartment of Radiation Oncology, China Medical University Hospital, Taichung, Taiwan
dSchool of Medicine, China Medical University, Taichung, Taiwan
eDepartment of Community Medicine and Health Examination Center, China Medical University Hospital, Taichung, Taiwan fDepartment of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan
a r t i c l e
i n f o
Article history: Received 2 July 2011 Accepted 26 July 2011 Keywords:
Urinary bladder cancer FDG PET
PET/CT Systemic review Meta-analysis
a b s t r a c t
Aim: The purpose of the current study was to conduct a systemic review and meta-analysis of the published literature to evaluate the diagnostic accuracy of FDG PET or PET/CT in urinary bladder cancer. Materials and methods: The authors conducted a systematic MEDLINE search of articles published between January 2000 and December 2010. Two reviewers independently assessed the methodological quality of each study. We conducted a meta-analysis of pooled sensitivity and specificity in detecting primary and metastatic lesions of bladder cancer.
Results: Six studies met the inclusion criteria. The pooled sensitivity and specificity of PET/CT for primary lesion detection of bladder cancer were 0.90 (95% CI: 0.70–0.99) and 1.00 (95% CI: 0.74–1.00), respectively. The pooled sensitivity and specificity of FDG PET or PET/CT for staging or restaging (metastatic lesions) of bladder cancer were 0.82 (95% CI: 0.72–0.89) and 0.89 (95% CI: 0.81–0.95), respectively.
Conclusion: The diagnostic accuracy of FDG PET or PET/CT is good in metastatic lesions of urinary bladder cancer. Due to the small number of patients and limited number of studies analyzed, the diagnostic capability of FDG PET or PET/CT in detection of primary bladder wall lesions could not be assessed.
© 2011 Elsevier Ireland Ltd. All rights reserved.
Bladder carcinoma is the most frequent type of tumor of the uri-nary tract and is most prevalent in the fifth to seventh decade of life
[1]. More than 90% of bladder cancers are transitional cell (urothe-lial) carcinomas, 5% are squamous cell carcinomas, and less than 2% are adenocarcinomas. Approximately 70% of bladder cancers present as superficial tumors, which tend to recur, and 30% present
夽 Grant sponsor: The grant supported by the study projects (DMR-98-052 and DMR-98-087) of China Medical University Hospital and Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH100-TD-B-111-004) and Taiwan Department of Health Cancer Research Center for Excellence (DOH100-TD-C-111-005).
∗ Corresponding author at: Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Road, Taichung 404, Taiwan. Tel.: +886 4 22052121x7412; fax: +886 4 22336174.
E-mail addresses:[email protected](Y.-Y. Lu),
[email protected](J.-H. Chen),[email protected](J.-A. Liang),
[email protected](H.-Y. Wang),[email protected](C.-C. Lin),
[email protected](W.-Y. Lin),[email protected](C.-H. Kao). 1 W.Y. Lin and Y.Y. Lu contributed equally to this work.
as muscle-invasive disease associated with a high risk of death from distant metastases[2]. Optimal therapy planning is depen-dent on accurate staging of the bladder tumor. For idepen-dentification of patients with metastatic disease, current imaging techniques including sonography, computed tomography (CT) and magnetic resonance imaging (MRI) have not proven to be highly accurate
[3–5].
Fluorine-18 2-fluoro-2-deoxy-D-glucose (F-18 FDG) positron emission tomography (PET) has become an important noninva-sive imaging modality for many malignancies because of its unique capability to image metabolically active lesions[6–9].
However, there have been a limited number of reports on the utilization of FDG PET to image bladder cancer, mainly because the urinary excretion of FDG interferes with visualization of the primary bladder tumor and regional nodes. Furthermore, only a rel-atively small population of bladder cancer patients can be obtained for study. Thus, the purpose of the current study was to conduct a meta-analysis of the published literature to evaluate the diagnostic accuracy of FDG PET in urinary bladder cancer.
0720-048X/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2011.07.018
2412 Y.-Y. Lu et al. / European Journal of Radiology 81 (2012) 2411–2416
Table 1
Criteria list used to assess the methodological quality of the studies.
Criteria of validity Positive score
Internal validity
Valid reference test Pathology from biopsy or surgery
Blind measurement of FDG PET without knowledge of reference test Blind measurement of reference test without knowledge of FDG PET
Avoidance of verification bias Assessment by reference test independent of FDG PET results FDG PET interpreted independently of all clinical information Mentioned in publication
Prospective study Mentioned in publication
External validity
Spectrum of disease All stage of disease
Demographic information Age and sex information given
Inclusion criteria Mentioned in publication
Exclusion criteria Mentioned in publication
Avoidance of selection bias Consecutive series of patients
Standard execution of FDG PET Type of camera, dose FDG, time interval, reconstruction FDG: F-18-fluorodeoxyglucose; and PET: positron emission tomography.
1. Materials and methods
1.1. Data search
A comprehensive computer search for relevant articles was conducted using the PubMed/MEDLINE and EBM Review search engines. The search strategy was based on the combination of the terms (1) PET, positron emission tomography; (2) FDG, fluo-rodeoxyglucose; and (3) bladder cancer. Searches were limited to the period between January 2000 and December 2010. Although no language restrictions were used initially, the full-text review and final analysis was limited to articles published in the English language. A manual search of additional studies was conducted using the references of the retrieved articles. Unpublished data and conference proceedings were not included. A total of 126 studies were retrieved from these searches for potential inclusion in the meta-analysis.
1.2. Data selection
Studies were eligible for inclusion based on the following crite-ria: (1) they evaluated bladder cancer for local detection/recurrence and/or staging/restaging and used (2) FDG PET and/or PET/CT imag-ing. Studies were excluded based on the following criteria: (1) included other types of urological cancer, (2) totals of true posi-tives, false posiposi-tives, true negaposi-tives, and false negatives were not provided, and (3) no data from a sub-analysis were provided. Unpublished data and conference proceedings were not included. Based on these criteria, 6 studies were eligible for inclusion in this meta-analysis.
1.3. Data extraction
Two reviewers independently assessed the methodological quality of the eligible studies. The criteria list recommended by the Cochrane Methods Working Group on Systematic Review of Screening and Diagnostic Tests was used[10]. Some items on the list were modified for this specific review. The complete criteria list used is presented inTable 1. Internal validity criteria (IV) were scored as “positive” (adequate methods), “negative” (inadequate methods, potential bias), or “unclear” if insufficient information had been provided on a specific item. External validity criteria (EV) were assessed to evaluate generalizability. Standard performance of FDG PET or PET/CT was scored as positive when the type of PET or PET/CT camera, the dose of FDG, the time between injection and scanning, and the method of reconstruction were described. The criteria for external validity were scored as positive if sufficient information was provided to judge generalizability of findings.
After the consensus meeting, we decided to score unclear scores as negative. Disagreements were resolved by consensus. Quality scores were expressed as a percentage of the maximum score. Subtotals were calculated for internal (maximum 6) and external (maximum 6) validity separately.
1.4. Statistical analysis
Data on sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of FDG PET or PET/CT in the detecting and/or staging/restaging of urinary bladder cancer were calculated from the original numbers given in the publications. We calculated the pooled and individual sensitivity, the specificity, and the 95% confidence interval for pooled estimators in forest plots. The pooled sensitivity and specificity estimators were weighted average in which the weight of each study is individual sample size. The sources of heterogeneity were included the pattern of observed study results and variation introduced by diagnostic threshold. If there is any evidence which was the diagnostic threshold varies between the studies, we should consider the summary receiver operating characteristic (SROC) curve. Testing of diagnostic thresh-old was Spearman’s correlation test. In this study, the threshthresh-old effect did not exist but we also showed the SROC curve in fig-ures which included values of Q* index and AUC. There were two main areas of meta-analysis: detecting bladder cancer and stag-ing/restaging of bladder cancer. However, there were not enough studies about detection of bladder cancer to make a meta-analysis. We report this result for reference only. The meta-analysis was conducted using free software Meta-DiSc (version 1.4).
2. Results
2.1. Literature search
A total of 126 studies about primary tumor detection, staging, tumor recurrence or restaging of bladder cancer with FDG PET or PET/CT were identified. After reviewing the titles and abstracts, 119 studies were excluded based on the criteria listed in Section1.2. Of the remaining 7 studies, one was excluded after a full review because of differentiation from other types of urological tumor and bladder cancer[11]. Six studies met the inclusion criteria[12–17]. The characteristics of the included studies are presented inTable 2. 2.2. Methodological quality assessment
Methodological quality was assessed by 12 items for each of the 6 selected studies. The scores for internal and external validity of the 6 selected studies are presented inTable 3. All studies included
Table 2 Clinical characteristics for selected studies. Study Year No. of patients Sex (M/F) Age Histology No of excluded patients Patient selection (detecting or staging/restaging) PET or PET/CT Lasix Image time Reference test Note Drieskens et al. [12] 2005 55 47/8 Mean: 63.7 33–82 years TCC 15 Staging
PET (Siemens- CTI)
20 mg iv 10 min after FDG inj 60 min after FDG PA or FU Anjos et al. [13] 2007 17 15/2 Mean: 68 49–83 years TCC – Detecting + restaging PET/CT (Siemens) Additional pelvic Images
1 h after iv lasix Duralphase:1 h after FDG, 1 h after lasix PA or FU Jadvar et al. [14] 2008 35 25/10 39–86 years TCC – Restaging
PET (Siemens 953/A) PET/CT (Siemens Biograph)
-6 0 min after FDG PA or FU Oral contrast Kibel et al. [15] 2009 43 32/11 Mean: 70 32–87 years Squamous or glandular differenti- ation
1 Detecting + staging PET/CT (Siemens) 20 mg iv 20 min after FDG inj 60 min after FDG PA Foley Harkirat et al. [16] 2010 29 – – TCC 7 Detecting PET/CT (Siemens) Delayed Image 60–90 min after iv 0.5 mg/kg lasix Dural phase: 1h , 150–180 min After FDG inj PA or FU Apolo et al. [17] 2010 57 38/19 Mean: 76 54–91 years TCC SCC/adenocarcinoma/neuroendocrine 10 Staging/restaging PET/CT (Siemens) -60–90 min after FDG PA or FU
Diluted oral contrast
FDG: F-18-fluorodeoxyglucose; PET: positron emission tomography; CT: computed tomography; PA: pathology; and FU: follow-up.
2414 Y.-Y. Lu et al. / European Journal of Radiology 81 (2012) 2411–2416 Table 3 Quality assessment of the selected studies. Study Year IV EV Total IV score Total EV score % o f maximum score IV1 IV2 IV3 IV4 IV5 IV6 EV1 EV2 EV3 EV4 EV5 EV6 Drieskens et al. [12] 2005 + + −− + + + +++++4 6 8 3 Anjos et al. [13] 2007 + −− + −−− ++ − ++2 4 5 0 Jadvar et al. [14] 2008 + + + −−− ++ −− ++3 4 5 8 Kibel et al. [15] 2009 + − ++ − + − +++ − +4 4 6 7 Harkirat et al. [16] 2010 + + + −−− + −−− ++3 3 5 0 Apolo et al. [17] 2010 + + −−− ++ + −− ++3 4 5 8 Note : IV1–IV6, six criteria for internal validity (IV; see Table 1 ); and EV1–EV6, six criteria for external validity (EV, see Table 1 ).
a valid reference test, but 3 studies did not describe whether the reference test was interpreted without the knowledge of the FDG PET findings (IV3). The readers were blinded to the results of the reference standard in 4 of the 6 studies (IV2). In 2 of the 6 stud-ies, verification bias was avoided because patients were selected for assessment by the reference test independently of the FDG PET results (IV4). Among the 6 eligible studies, 3 were performed prospectively.
In 4 of the selected studies, all staging of disease was included. In 3 studies, the inclusion criteria were described and in 2 studies the exclusion criteria were described. In 5 studies, patients entered the study consecutively. The type of camera, the FDG dosage, the uptake period, the time interval and reconstruction were reported in all of the studies (EV6). The total score for the combined internal and external validity, expressed as a fraction of the maximum score, ranged from 50% to 83%.
2.3. Diagnostic accuracy of FDG PET or PET/CT
Fig. 1shows the forest plot of sensitivity and specificity of FDG
PET/CT for primary lesion detection of bladder cancer. The chi-square values of sensitivity and specificity were 1.43 (p = 0.2320, >.05) and 1.00 (p = 1.0000, >.05), respectively. The pooled sensitiv-ity and specificsensitiv-ity with 95% confidence interval (CI) for PET/CT were 0.90 (0.70–0.99) and 1.00 (0.74–1.00), respectively.Fig. 2shows the forest plot of sensitivity and specificity of FDG PET or PET/CT for staging or restaging (metastatic lesions) of bladder cancer. The chi-square values of sensitivity and specificity were 19.64 (p = 0.0006, <.05) and 11.62 (p = 0.0204, <.05), respectively. The pooled sensi-tivity and specificity with 95% CI for FDG PET or PET/CT were 0.82 (0.72–0.89) and 0.89 (0.81–0.95), respectively.
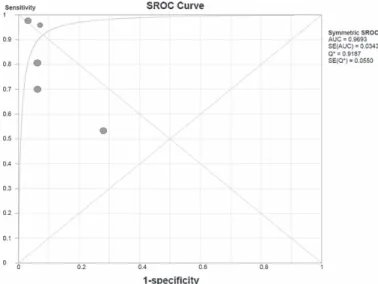
The SROC curve represents a global test performance and the trade-off between sensitivity and specificity. The Q* index repre-sents maximum joint sensitivity and specificity, calculated as a global measure of diagnostic accuracy.Fig. 3shows the SROC curves for FDG PET or PET/CT for staging or restaging (metastatic lesions) of bladder cancer. The Q* index was 0.9187.
3. Discussion
Circulating F-18 FDG is largely excreted in the urine. The pooled activity in the urinary bladder makes the evaluation of bladder wall lesions difficult. This limitation has disappointed many investiga-tors of bladder cancer imaging. According to our meta-analysis, only two studies[13,16]have investigated the value of PET scan with F-18 FDG in detecting primary lesions of urinary bladder can-cer. Both Anjos et al.[13]and Harkirat et al.[16]used delayed pelvic images after diuretic administration and oral hydration with F-18 FDG PET/CT. Anjos et al.[13]investigated 11 patients with inva-sive bladder cancer, and reported the sensitivity and the specificity for the detection of bladder wall lesions were both 100%. Harki-rat et al.[16]evaluated 22 patients with invasive bladder cancer who had not undergone cystectomy and found the sensitivity and the specificity for primary bladder lesions were 86.7% and 100%, respectively. In our meta-analysis, the summary (pooled) sensi-tivity was 90% and the summary (pooled) specificity was 100%
(Fig. 1). There were only two studies about detection of bladder
cancer, therefore the SROCs for detecting bladder cancer could not be calculated.
Among the studies with patient-based data of bladder cancer in staging or restaging (metastatic lesions) by FDG PET or PET/CT, the summary (pooled) sensitivity was 82% and the summary (pooled) specificity was 89% (Fig. 2). The global measure of diagnostic accu-racy was 0.9187. The results of this meta-analysis suggest that FDG PET or PET/CT provides good diagnostic accuracy of lymph node
Fig. 1. Forest plots of the sensitivity and the specificity of FDG PET and PET/CT for detection of primary tumor bladder cancer.
staging and distant metastasis of bladder cancer. The data points in the SROC curve in the study by Drieskens et al.[12]show the worst results (Fig. 3). They examined preoperative nodal involvement and other distant metastasis by FDG PET scan rather than FDG PET/CT scan. A limitation of PET is the lack of an anatomic reference frame.
It is widely accepted that the addition of CT images to PET provides precise anatomic information, which can improve the diagnostic ability for bladder cancer. Therefore, the fact that Drieskens et al.
[12]used FDG PET scan rather than FDG PET/CT scan reduced the diagnostic performance of the scan.
2416 Y.-Y. Lu et al. / European Journal of Radiology 81 (2012) 2411–2416
Fig. 3. The summary receiver operating characteristic (SROC) curves and the Q*
index for FDG PET and PET/CT in staging or restaging (metastatic lesions) of bladder cancer.
The application of FDG PET or PET/CT in bladder cancer is hampered by the urinary excretion. Several interventions such as adequate hydration, bladder irrigation, and forced diuresis with furosemide have been used to overcome this handicap[13,18–22]. Among the 6 eligible studies, four studies used intravenous injec-tion of furosemide[12,13,15,16]. In two of the selected studies
[13,16], additional delayed pelvic images were acquired. Both Anjos
et al. [13] and Harkirat et al. [16] used delayed pelvic images after diuretic administration and oral hydration with F-18 FDG PET/CT in detecting bladder wall lesions. Their results showed good sensitivity and specificity of FDG PET/CT. We believe that the use of FDG PET/CT along with novel interventions will overcome the problem of urinary excretion in detection of urinary bladder cancer.
Our meta-analysis had several potential limitations, because only 6 selected studies were analyzed. First, the presence of clinical heterogeneity in the patient population, imaging techniques, study design, and quality in these selected studies affects the generaliz-ability of the results. The retrospective design in three studies, as well as the interpretation of FDG PET with other available clinical information, further decreased the methodological quality. There was verification bias in four studies. This is because the reference test was assessed on patients selected by the index test results, which can lead to overestimation of the sensitivity. Second, there were only two studies about detection of primary tumor of bladder cancer, and therefore the SROCs for detecting bladder cancer could not be calculated. Large prospective studies are needed in order to evaluate primary tumor detection with FDG PET/CT scan. Despite these drawbacks, this meta-analysis demonstrates the diagnostic performance of FDG PET or PET/CT in bladder cancer over the last decade.
The results from this meta-analysis suggest that the diagnos-tic accuracy of FDG PET or PET/CT is good in staging or restaging (metastatic lesions) of urinary bladder cancer. Due to the small number of patients and limited number of studies analyzed, the diagnostic capability of FDG PET or PET/CT in detection of primary bladder wall lesions could not be assessed. We believe the use of FDG PET/CT along with novel interventions will overcome the prob-lem of urinary excretion in detection of urinary bladder cancer. We suppose that only a few studies that used FDG PET or PET/CT in
detection of urinary bladder cancer can be found, which means that our meta-analysis is still valuable. Further prospective ran-domized, controlled studies with larger case numbers are needed to confirm the value of FDG PET (PET/CT) in detection of primary urinary bladder cancer.
Conflicts of interest
No potential conflicts of interest were disclosed.
References
[1] Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71–96.
[2] Kaufman DS, Shipley WU, Feldman AS. Bladder cancer. Lancet 2009;374(18):239–49.
[3] Paik ML, Scolieri MJ, Brown SL, Spirnak JP, Resnick MI. Limitations of computer-ized tomography in staging invasive bladder cancer before radical cystectomy. J Urol 2000;163:1693–6.
[4] Voges GE, Tauschke E, Stockle M, Alken P, Hohenfellner R. Computerized tomography: an unreliable method for accurate staging of bladder tumors in patients who are candidates for radical cystectomy. J Urol 1989;142:972–4. [5] Yaman O, Baltaci S, Arikan N, Yilmaz E, Gogus O. Staging with computed
tomography, transrectal ultrasonography and transurethral resection of blad-der tumour: comparison with final pathological stage in invasive bladblad-der carcinoma. Br J Urol 1996;78:197–200.
[6] Antoch G, Saoudi N, Kuehl H, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-d-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: com-parison with CT and PET. J Clin Oncol 2004;22:4357–68.
[7] Bar-Shalom R, Yefremov N, Guralnik L, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med 2003;44:1200–9.
[8] Schoder H, Larson SM, Yeung HW. PET/CT in oncology: integration into clinical management of lymphoma, melanoma, and gastrointestinal malignancies. J Nucl Med 2004;45(Suppl. 1):72S–81S.
[9] Cohade C, Osman M, Leal J, Wahl RL. Direct comparison of (18)F-FDG PET and PET/CT in patients with colorectal carcinoma. J Nucl Med 2003;44:1797–803. [10] Cochrane Methods Working Group on Systematic Review
of Screening and Diagnostic Tests: Recommended Methods.
http://www.cochrane.org/cochrane/sadtdoc1.htm. Updated June 6, 1996 [accessed April 8, 2010].
[11] Liu IJ, Lai YH, Espiritu JI, et al. Evaluation of fluorodeoxyglucose positron emis-sion tomography imaging in metastatic transitional cell carcinoma with and without prior chemotherapy. Urol Int 2006;77:69–75.
[12] Drieskens O, Oyen R, Van Poppel H, Vankan Y, Flamen P, Mortelmans L. FDG-PET for preoperative staging of bladder cancer. Eur J Nucl Med Mol Imaging 2005;32:1412–7.
[13] Anjos DA, Etchebehere EC, Ramos CD, Santos AO, Albertotti C, Camargo EE. 18F-FDG PET/CT delayed images after diuretic for restaging invasive bladder cancer. J Nucl Med 2007;48:764–70.
[14] Jadvar H, Quan V, Henderson RW, Conti PS. [F-18]-fluorodeoxyglucose PET and PET-CT in diagnostic imaging evaluation of locally recurrent and metastatic bladder transitional cell carcinoma. Int J Clin Oncol 2008;13:42–7.
[15] Kibel AS, Dehdashti F, Katz MD, et al. Prospective study of [18F]fluorodeoxyglucose positron emission tomography/computed tomog-raphy for staging of muscle-invasive bladder carcinoma. J Clin Oncol 2009;27:4314–20.
[16] Harkirat S, Anand S, Jacob M. Forced diuresis and dual-phase F-fluorodeoxyglucose-PET/CT scan for restaging of urinary bladder cancers. Indian J Radiol Imaging 2010;20:13–9.
[17] Apolo AB, Riches J, Schoder H, et al. Clinical value of fluorine-18 2-fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography in bladder cancer. J Clin Oncol 2010;28:3973–8.
[18] Kosuda S, Kison PV, Greenough R, Grossman HB, Wahl RL. Preliminary assess-ment of fluorine-18 fluorodeoxyglucose positron emission tomography in patients with bladder cancer. Eur J Nucl Med 1997;24:615–20.
[19] Ahlstrom H, Malmstrom PU, Letocha H, Andersson J, Langstrom B, Nilsson S. Positron emission tomography in the diagnosis and staging of urinary bladder cancer. Acta Radiol 1996;37:180–5.
[20] de Jong IJ, Pruim J, Elsinga PH, Jongen MM, Mensink HJ, Vaalburg W. Visualisa-tion of bladder cancer using (11)C-choline PET: first clinical experience. Eur J Nucl Med Mol Imaging 2002;29:1283–8.
[21] Koyama K, Okamura T, Kawabe J, et al. Evaluation of 18F-FDG PET with bladder irrigation in patients with uterine and ovarian tumors. J Nucl Med 2003;44:353–8.
[22] Sugawara Y, Eisbruch A, Kosuda S, Recker BE, Kison PV, Wahl RL. Evaluation of FDG PET in patients with cervical cancer. J Nucl Med 1999;40:1125–31.