Title: Germline copy number variation in complement component C4A is associated with Graves' ophthalmopathy in the Taiwan Chinese population
Authors: Yu-Huei Liu1, 2, Lei Wan1, 3, 4,Chwen-Tzuei Chang5, 6, Wen-Ling Liao1, Wen-Chi Chen2, Yuhsin Tsai3, Chang-Hai Tsai7, 8, Fuu-Jen Tsai1, 3, 7, 9, 10, 11
1
Department of Medical Genetics and Medical Research, China Medical University Hospital, Taichung, Taiwan; 2 Graduate Institute of Integrated Medicine, China Medical University, Taichung, Taiwan; 3 School of Chinese Medicine, China Medical University, Taichung, Taiwan; 4Department of Health and Nutrition Biotechnology, Asia University, Taichung, Taiwan; 5Division of Endocrinology and Metabolism, Department of Medicine, China Medical University Hospital, Taichung, Taiwan; 6 Department of Endocrinology and Metabolism, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 7Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan; 8 Department of Biotechnology, Asia University, Taichung, Taiwan; 9School of Post-Baccalaureate Chinese Medicine, China Medical University, Taichung, Taiwan; 10Department of Biotechnology, Asia University, Taichung, Taiwan, 11Department of Biotechnology and Bioinformatics, Asia University, Taichung, Taiwan.
Address for reprints:
Fuu-Jen Tsai, MD, PhD.
Department of Medical Genetics and Medical Research, China Medical University Hospital
No.2 Yuh-Der Road, 404 Taichung, Taiwan
Telephone: 886-4-22062121 Ext 2041; Fax: 886-4-22033295
E-mail: [email protected]
E-mail address:
Wan L: [email protected] Chang CT: [email protected] Liao WL: [email protected] Chen WC: [email protected] Tsai Y: [email protected] Tsai CH: [email protected] Tsai FJ: [email protected]
Abstract
Background: Gene copy number of complement component C4, which varies
among individuals, may determine the intrinsic strength of the classical
complement pathway. Presuming a major role of complement as an effecter in peptide-mediated inflammation and phagocytosis, we hypothesized that C4 genetic diversity may partially explain the variation in Graves’ disease (GD) outcomes.
Methods: A case-control study including a total of 624 Taiwan Chinese
patients with GD, including 227 with Graves’ ophthalmopathy (GO) and 397 without, were enrolled. CNV of total C4, C4 isotypes (C4A and C4B) genes were performed by quantitative real-time polymerase chain reaction analysis.
Main Outcome Measures: Statistical comparison and identification of CNV of
total C4 and C4 isotypes (C4A and C4B) genes between GD patients with or without GO and other outcomes.
Results: The risk of susceptibility to GO was significantly reduced among GD
patients with <2 copies of C4A (p = 0.014) but not C4B (p = 0.187). In addition, different C4 polymorphisms may correlated with GO susceptibility (p = 0.050). Moreover, although no CNV of C4A or C4B was significantly associated with goiter or nodular hyperplasia, having <2 copies of C4A resulted in a higher risk of vitiligo and myxedema (p = 0.001, OR = 2.646, 95% CI: 1.543–4.504 for vitiligo and p = 0.008, OR = 2.236, 95% CI: 1.270–3.936 for myxedema, respectively).
Conclusions: CNV of C4A may play an important role in the pathogenesis of
Background
Graves' disease (GD) is an organ-specific autoimmune thyroid disease. Graves' ophthalmopathy (GO), characterized by inflammation and fat deposition in the eye muscles and the connective tissue surrounding the eye, is the most common
extrathyroid manifestation of GD and affects 25%–50% of GD patients [1]. It has been known that multiple factors, including the host's genetic factors as well as environmental factors, contribute to the etiology and severity of GD [2,3]. However, other forms of variation that might affect gene expression should also be considered.
A new paradigm in human genetics is high frequencies of interindividual
variation in the copy number (CN) of specific genomic DNA segments. Copy number variation (CNV) loci often contain genes engaged in host-environment interactions, including those involved in immune functions, which results in susceptibility or resistance to autoimmune diseases [4-7], however, no significant association has been found between CNV and GD or GO [6].
Complement component C4 (C4), located on chromosome 6q21.3, is encoded by 2 separate loci in the major histocompatibility complex class III region and derives 2 functionally distinct C4A and C4B isoforms [8]. The complement system is the main element of innate immunity and is regarded as the first line of defense against intrinsic and extrinsic antigens, leading to peptide-mediated inflammation, opsonization
leading phagocytosis, or the direct lysis of antigens [9]. Presuming a major role of complement as an effector in peptide-mediated inflammation and phagocytosis, we hypothesized that C4 genetic diversity may partially explain the variation in GD outcomes. Here we investigated the polymorphic variants of C4 that correlate with predisposition to this disease in the Taiwan Chinese population.
Methods
Patients
diagnosis of GD from China Medical University Hospital in Taiwan were enrolled and actively followed. All individuals provided informed consent as approved by the ethics committee of China Medical University Hospital. Diagnosis of GD and GO was followed the criteria set previously [10]. Full medical record abstraction was conducted to obtain demographics (age and gender); treatment and clinical features are summarized in Table 1.
Genomic DNA extraction and quantification gene dosage of C4A and C4B
Genomic DNA was extracted from peripheral blood following the manufactory's suggestions (Qiagen). C4 gene dosage was assessed by quantitative real-time
TaqMan® PCR analysis (Applied Biosystems) as described in the previously published protocols with some modification [11]. Real-time PCR analysis was performed in 96-well optical plates on a 7900HT real-time PCR system (Applied Biosystems). Primers and probes specific for C4A, and C4B (common C4A and C4B forward primer “C4F”: 5’-GCA GGA GAC ATC TAA CTG GCT TCT-3’; common
C4A and C4B reverse primer “C4R”: 5’-CCG CAC CTG CAT GCT CCT-3’; probe “C4A”: FAM-ACC CCT GTC CAG TGT TAG; probe “C4B”: FAM-ACC TCT CTC CAG TGA TAC. TaqMan® Universal PCR Master Mix, No AmpErase® uracil-DNA glycosylase (ABI catalog number 4326614), VIC-conjugated TaqMan® RNase P control reagents (ABI catalog number 4316844), 250 nM of the respective
FAM-conjugated TaqMan® probes (C4A or C4B), the particular primers (300 nM
C4A or C4B) in distilled water was contained in each of the distinct PCR batches. Appropriately prediluted genomic DNA (threshold cycle [CT] values for RNase P between 24 and 30) was added before start. CN of each target gene in each sample was determined from three separated experiments. Thermal cycler conditions were adjusted as follows: initial denaturation step for 10 minutes at 95°C; 40 cycles including denaturation for 15 seconds at 95 °C; and annealing/extension for 1 minute for 60°C. The data were analyzed using SDS 2.3 software (Applied Biosystems).
the formula nRAWC4X= 2 (CTRNase P)-(CTC4X)+1, where C4X referred to C4A or C4B . Raw
gene dosages of positive controls selected from the reference panel were plotted versus the actual gene dosages, and the resulting calibration curve served for
determination of the actual copy number of unknown samples of this particular run.
Statistical analysis
Statistical analysis was performed using the statistical package PASW for Windows (version 18.0; SPSS Inc.). Differences in the incidence of subjects with C4 gene CNs above and below the median or C4A-C4B polymorphisms between patients with or without GO were evaluated using Fisher’s exact test. Two-tailed p values were estimated by 100,000 Monte Carlo simulations with 99% confidence intervals (CI). Odds ratios (ORs) and 95% CIs were estimated from logistic regression models. A p value of 0.05 with adjusted with Bonferroni was considered statistically significant for each test.
Results
CNV of C4A, but not C4B, is associated with susceptibility to GO
The distribution of copy number for total C4 as well as C4 isotypes according to the presence of GO is shown in Figure 1. The variation in C4 CN showed a pattern close to a normal distribution, and the majority of patients (50.3%) had 4 copies of the
C4 gene. No GD patient had a full deficiency of C4 alleles. The relationship between C4 CNV status and GO was not significant (p = 0.396). The distribution of C4A and
C4B among GD patients with and without GO were further investigated. The median CNs of C4A and C4B in the study population were 2 and 2, respectively. Although the CNV of C4B was not significantly associated with GO (p = 0.186), an unexpected finding was that GD patients with <2 copies (0 or 1) of the C4A gene were less susceptible to GO (p = 0.014, OR = 0.447, 95% CI: 0.255-0.785). The significance remained after applying the Bonferroni correction (p < 0.05/3). These results indicate that <2 copies of C4A, but not C4B, may be a protective factor against the
Polymorphism analysis of C4 genes
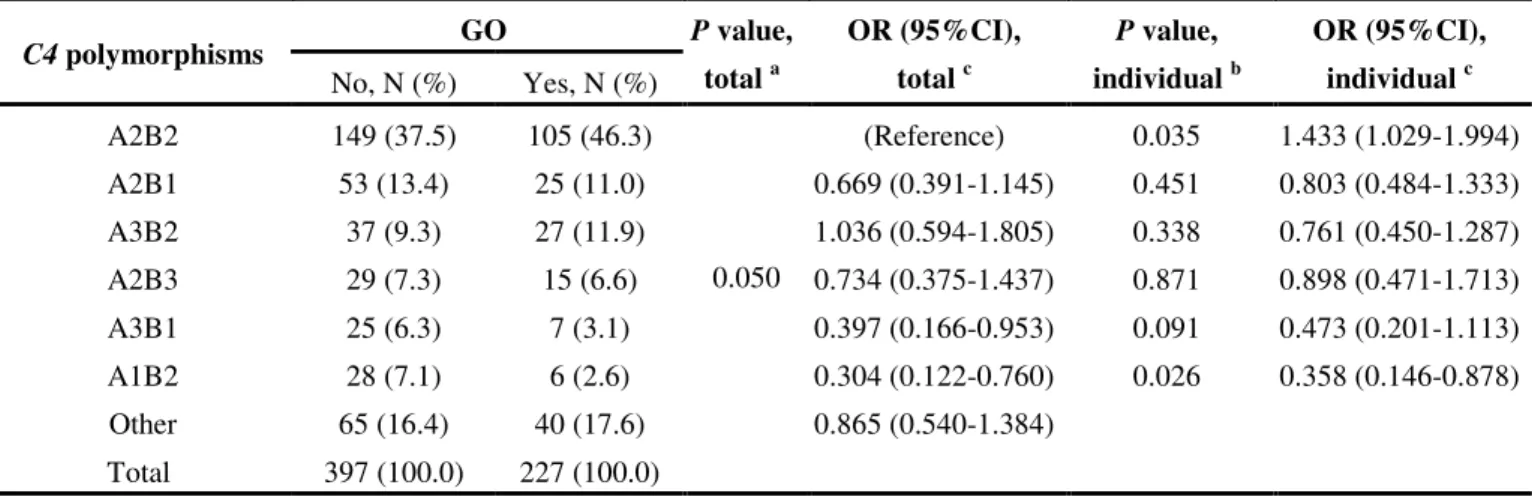
The C4 polymorphism was estimated from the CNs for C4A and C4B. The polymorphisms with a frequency >5% are summarized in Table 2 according to the presence of GO. The significance of polymorphism remained, although did not meet the Bonferroni correction. The GD patients with the most common polymorphism (40.7%), A2B2, with 1.433-fold risk toward GO (p = 0.035, OR = 1.433, 95% CI: 1.029-1.994) as compared to those without. When compared to those with A2B2, those with A3B1 or A1B2 polymorphisms had 60.3% and 69.6% less susceptibility to GO, respectively (p = 0.05, OR = 0.397, 95% CI: 0.166–0.953 for A3B1; p = 0.05, OR = 0.304, 95% CI: 0.122–0.760, p = 0.033 for A1B2). These results suggest the C4 polymorphisms may associate with GO development in the GD patients.
Correlation between C4 CNV and other clinical features of GD
To extend our finding, we also investigated the linkage among C4 CNV and clinical features in patients with GD. Although C4 CNV was not significantly
associated with goiter or nodular hyperplasia (p = 0.103 and p = 0.504, respectively), patients with <4 copies of C4 had a 1.747-fold increased risk of vitiligo (p = 0.002, OR = 1.747, 95% CI: 1.091–2.830) and a 1.877-fold increased risk of myxedema (p = 4.9 × 10-4, OR = 1.877, 95% CI: 1.143–3.082). Only C4A, but not C4B, contributed to the effect (p = 0.001, OR = 2.646, 95% CI: 1.543–4.504 for vitiligo; p = 0.002, OR = 2.646, 95% CI: 1.543–4.504 for myxedema). The significance remained after
applying the Bonferroni correction (p < 0.05/3) (Table 3). No C4 polymorphism was significantly associated with the clinical features of GD (data not shown). These results indicate that <4 copies of C4, especially <2 copies of C4A, may increase the risk for vitiligo and myxedema in patients with GD.
Discussion
Several functionally relevant single nucleotide polymorphisms are characteristic of GD and GO [12,13], but no relevant CNV has been reported [14]. In the present study, we found that GD patients with <2 copies of C4A had a significantly lower
prevalence of GO but higher prevalence of vitiligo and myxedema. In addition, while polymorphism A2B2 may confer higher risk of GO, A3B1 and A1B2 may confer lower risk of GO. To the best of our knowledge, this is the first study to report that CNV in C4 genes is associated with the protection of GO in Taiwan’s Chinese population. Our results provide new insights into the prediction of and target therapeutics for GO.
Indeed, low level of C4 complements in sera have been found in several autoimmune diseases [15-18]. In addition, the presence of C4A and C4B null alleles that result in partial C4 deficiency have shown to be associated with systemic lupus erythematosus (SLE).[7] In the patients with SLE, complement deficiency may promote the accumulation of immune complex in the glomerulus of the kidney. Our results also revealed that deficiency of C4A, may enhance the development of vitiligo and myxedema in GD patients. This may due to activated complement exacerbated inflammation-driven tissue injury, immunocomplex clearance and autoreactive B cells deletion. However, it may play a different regulatory role in organ-specific
autoimmune diseases such as GO. One possibility is that a deficiency of complement may lead to defective processing of immune complexes, impairment of B-cell
memory, and help reduce tissue injury [19]. Unfortunately, the mechanisms by which
C4 abnormality contributes to the protection of organ-specific autoimmunity are poorly understood. Nevertheless, whether a potential gene-gene or gene-environment interaction is involved in susceptibility to GO needs to be further investigated [20]. However, this study provides a substantial amount of data that can help to clarify the role of C4 genes in this disorder. It is only through investigations of diverse
populations that researchers can expect to dissect the complex genetics involved. In addition, functional studies of susceptibility genes using appropriate animal models could allow for an assessment of their role in the disease process.
What is interesting is that although we explored the relationship of C4 CNV to GD as well as other GD clinical features, only the lower copies of C4A, but not C4B, were associated with higher risk of vitiligo and myxedema. Because it appears that
C4A binds to amino group-containing antigens such as immune complex, whereas C4B binds to hydroxyl group-containing antigens such as bacteria, this result may provide another view to support the hypotheses that the pathogenesis of vitiligo and myxedema may be more relevant to the existence of the immune complex than the pathogen. In addition, although there is no evidence related to gene polymorphism in myxedema, recent studies have identified that the risk locus within the major
histocompatibility complex region on chromosome 6q may be associated with vitiligo in both Chinese Han population and American population [21,22]. It may be
interesting to investigate the gene-gene interaction between C4 polymorphism and the vitiligo risky locus in associated with the GD clinical features. Moreover, although confirmation of these results in larger samples is warranted, it would be interesting to further investigate the role of C4A in the development of vitiligo and myxedema.
Conclusion
This study provides evidence that the CNV of C4 genes is associated with risk of the development and progression of GO and the GD-related clinical features. These results might aid in diagnosis during the early stage of the disease and may be
valuable in the development of therapeutic agents for the Taiwan Chinese population.
List of abbreviations
(GD): Graves’ disease; (GO): Graves’ ophthalmopathy; (CNV)” copy number variation; (CN): copy number; (SLE): systemic lupus erythematosus.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
Author Liu YH designed the study, managed the literature searches, undertook the statistical analysis, and wrote the draft of the manuscript. Author Wan L designed and
performed the experiments. Author Chang CT and Chen WC recruited and maintained the clinical information of participants. Author Liao WL and Tsai Y undertook the statistical analysis. Author Tsai CH and Tsai FJ directed the study and reviewed the results. All authors contributed to and have approved the final manuscript.
Acknowledgements
We thank Hsin-Hui Chen for the technical assistance in preparation of DNA and analyzing the variations. This study was supported by grants from the National Science Council (96-2628-B-039-002-MY3 and 98-2320-B-039-008-MY3), Taipei, Taiwan, and grants from the China Medical University Hospital (DMR-100-162), Taichung, Taiwan.
References
1. Mishra A. and Mishra S.K. Multicentre study of thyroid nodules in patients with Graves' disease (Br J Surg 2000; 87: 1111-13). Br J Surg 88(2):313, 2001. 2. Tomer Y. and Huber A. The etiology of autoimmune thyroid disease: a story of
genes and environment. J Autoimmun 32(3-4):231-239, 2009.
3. McGrogan A., Seaman H.E., Wright J.W. and de Vries C.S. The incidence of autoimmune thyroid disease: a systematic review of the literature. Clin Endocrinol (Oxf) 69(5):687-696, 2008.
4. Fanciulli M., Petretto E. and Aitman T.J. Gene copy number variation and common human disease. Clin Genet 77(3):201-213.
5. Schaschl H., Aitman T.J. and Vyse T.J. Copy number variation in the human genome and its implication in autoimmunity. Clin Exp Immunol 156(1):12-16, 2009.
6. Fanciulli M., Norsworthy P.J., Petretto E., Dong R., Harper L., Kamesh L., Heward J.M., Gough S.C.L., de Smith A., Blakemore A.I.F., Owen C.J.,
Pearce S.H.S., Teixeira L., Guillevin L., Graham D.S.C., Pusey C.D., Cook H.T., Vyse T.J. and Aitman T.J. FCGR3B copy number variation is associated with susceptibility to systemic, but not organ-specific, autoimmunity. Nature Genetics 39(6):721-723, 2007.
7. Yang Y., Chung E.K., Wu Y.L., Savelli S.L., Nagaraja H.N., Zhou B., Hebert M., Jones K.N., Shu Y., Kitzmiller K., Blanchong C.A., McBride K.L., Higgins G.C., Rennebohm R.M., Rice R.R., Hackshaw K.V., Roubey R.A., Grossman J.M., Tsao B.P., Birmingham D.J., Rovin B.H., Hebert L.A. and Yu C.Y. Gene copy-number variation and associated polymorphisms of
complement component C4 in human systemic lupus erythematosus (SLE): low copy number is a risk factor for and high copy number is a protective factor against SLE susceptibility in European Americans. Am J Hum Genet 80(6):1037-1054, 2007.
8. Yu C.Y. and Whitacre C.C. Sex, MHC and complement C4 in autoimmune diseases. Trends Immunol 25(12):694-699, 2004.
9. Carroll M.C. The role of complement and complement receptors in induction and regulation of immunity. Annu Rev Immunol 16:545-568, 1998.
10. Liu Y.H., Chen R.H., Chen W.C., Tsai Y., Wan L. and Tsai F.J. Disease association of the CD103 polymorphisms in Taiwan Chinese Graves' ophthalmopathy patients. Ophthalmology 117(8):1645-1651.
11. Szilagyi A., Blasko B., Szilassy D., Fust G., Sasvari-Szekely M. and Ronai Z. Real-time PCR quantification of human complement C4A and C4B genes. BMC Genet 7:1, 2006.
12. Zeitlin A.A., Simmonds M.J. and Gough S.C. Genetic developments in autoimmune thyroid disease: an evolutionary process. Clin Endocrinol (Oxf) 68(5):671-682, 2008.
13. Jacobson E.M. and Tomer Y. The genetic basis of thyroid autoimmunity. Thyroid 17(10):949-961, 2007.
Heward J.M., Gough S.C., de Smith A., Blakemore A.I., Froguel P., Owen C.J., Pearce S.H., Teixeira L., Guillevin L., Graham D.S., Pusey C.D., Cook H.T., Vyse T.J. and Aitman T.J. FCGR3B copy number variation is associated with susceptibility to systemic, but not organ-specific, autoimmunity. Nat Genet 39(6):721-723, 2007.
15. Lachmann P.J. Complement deficiency and the pathogenesis of autoimmune immune complex disease. Chem Immunol 49:245-263, 1990.
16. Beurskens F.J., van Dijk H. and Robins D.M. Does complement component C4A protect from autoimmune disease? Immunol Today 18(4):199, 1997. 17. Seelen M.A. and Daha M.R. The role of complement in autoimmune renal
disease. Autoimmunity 39(5):411-415, 2006.
18. Chen M., Daha M.R. and Kallenberg C.G. The complement system in systemic autoimmune disease. J Autoimmun 34(3):J276-286.
19. Markiewski M.M. and Lambris J.D. The role of complement in inflammatory diseases from behind the scenes into the spotlight. Am J Pathol
171(3):715-727, 2007.
20. Davies E.J., Steers G., Ollier W.E., Grennan D.M., Cooper R.G., Hay E.M. and Hillarby M.C. Relative contributions of HLA-DQA and complement C4A loci in determining susceptibility to systemic lupus erythematosus. Br J Rheumatol 34(3):221-225, 1995.
21. Jin Y., Birlea S.A., Fain P.R., Gowan K., Riccardi S.L., Holland P.J., Bennett D.C., Herbstman D.M., Wallace M.R., McCormack W.T., Kemp E.H., Gawkrodger D.J., Weetman A.P., Picardo M., Leone G., Taieb A., Jouary T., Ezzedine K., van Geel N., Lambert J., Overbeck A. and Spritz R.A.
Genome-Wide Analysis Identifies a Quantitative Trait Locus in the MHC Class II Region Associated with Generalized Vitiligo Age of Onset. J Invest Dermatol.
22. Quan C., Ren Y.Q., Xiang L.H., Sun L.D., Xu A.E., Gao X.H., Chen H.D., Pu X.M., Wu R.N., Liang C.Z., Li J.B., Gao T.W., Zhang J.Z., Wang X.L., Wang
J., Yang R.Y., Liang L., Yu J.B., Zuo X.B., Zhang S.Q., Zhang S.M., Chen G., Zheng X.D., Li P., Zhu J., Li Y.W., Wei X.D., Hong W.S., Ye Y., Zhang Y., Wu W.S., Cheng H., Dong P.L., Hu D.Y., Li Y., Li M., Zhang X., Tang H.Y., Tang X.F., Xu S.X., He S.M., Lv Y.M., Shen M., Jiang H.Q., Wang Y., Li K., Kang X.J., Liu Y.Q., Sun L., Liu Z.F., Xie S.Q., Zhu C.Y., Xu Q., Gao J.P., Hu W.L., Ni C., Pan T.M., Yao S., He C.F., Liu Y.S., Yu Z.Y., Yin X.Y., Zhang F.Y., Yang S., Zhou Y. and Zhang X.J. Genome-wide association study for vitiligo identifies susceptibility loci at 6q27 and the MHC. Nat Genet 42(7):614-618.
Figure legends
Figure 1. C4 copy numbers in Graves’ disease (GD) patients with or without Graves’ ophthalmopathy (GO). (A) left panel, C4 gene copy
numberhealthy; middle panel, C4A gene copy number; right panel, C4B copy number. Fisher’s exact test was used to assess the distribution of C4 genes between groups. Two-tailed p values for significance were estimated by 100,000 Monte Carlo
simulations with 99% confidence intervals. N, number of subjects in each group. (B) Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by applying unconditional logistic regression between GD patients with or without GO.
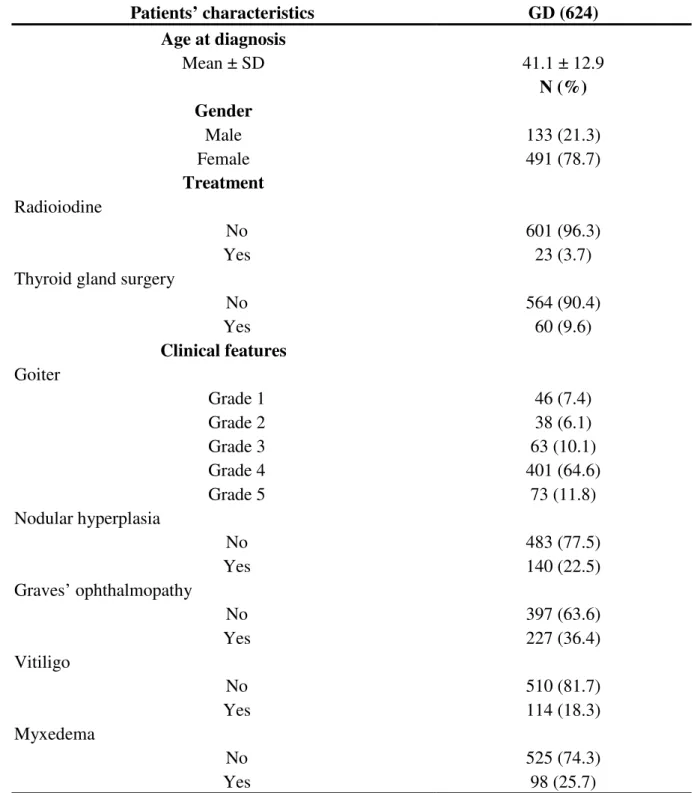
Table 1. Background and demographic characteristics of patients with Graves’ disease. Patients’ characteristics GD (624) Age at diagnosis Mean ± SD 41.1 ± 12.9 N (%) Gender Male 133 (21.3) Female 491 (78.7) Treatment Radioiodine No 601 (96.3) Yes 23 (3.7)
Thyroid gland surgery
No 564 (90.4) Yes 60 (9.6) Clinical features Goiter Grade 1 46 (7.4) Grade 2 38 (6.1) Grade 3 63 (10.1) Grade 4 401 (64.6) Grade 5 73 (11.8) Nodular hyperplasia No 483 (77.5) Yes 140 (22.5) Graves’ ophthalmopathy No 397 (63.6) Yes 227 (36.4) Vitiligo No 510 (81.7) Yes 114 (18.3) Myxedema No 525 (74.3) Yes 98 (25.7)
Abbreviations: GD, Graves, disease; GO, Graves’ ophthalmopathy; SD, standard deviation; N, number.
Table 2. Distribution of C4 polymorphisms in Graves’ disease with or without ophthalmopathy. GO C4 polymorphisms No, N (%) Yes, N (%) P value, total a OR (95%CI), total c P value, individual b OR (95%CI), individual c A2B2 149 (37.5) 105 (46.3) (Reference) 0.035 1.433 (1.029-1.994) A2B1 53 (13.4) 25 (11.0) 0.669 (0.391-1.145) 0.451 0.803 (0.484-1.333) A3B2 37 (9.3) 27 (11.9) 1.036 (0.594-1.805) 0.338 0.761 (0.450-1.287) A2B3 29 (7.3) 15 (6.6) 0.734 (0.375-1.437) 0.871 0.898 (0.471-1.713) A3B1 25 (6.3) 7 (3.1) 0.397 (0.166-0.953) 0.091 0.473 (0.201-1.113) A1B2 28 (7.1) 6 (2.6) 0.304 (0.122-0.760) 0.026 0.358 (0.146-0.878) Other 65 (16.4) 40 (17.6) 0.050 0.865 (0.540-1.384) Total 397 (100.0) 227 (100.0)
Abbreviations: GO, Graves’ ophthalmology; CNV, copy number variation; OR, odds ratio; CI, confidence interval; N, number.
a
C4 polymorphisms between GD patients with or without GO were evaluated by Fisher’s exact test using 7 × 2 contingency tables.
b
Individual C4 polymorphism between those with or without GO were evaluated by Fisher’s exact test using 2 × 2 contingency tables.
c
Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by applying unconditional logistic regression between GD patients with or without GO.
16
Table 3. Distribution of C4 copy numbers in patients with Graves’ disease with or without vitiligo/myxedema. Vitiligo Myxedema CNV No, N (%) Yes, N (%) P value a OR (95%CI) b No, N (%) Yes, N (%) P value a OR (95%CI) b C4 =4 258 (50.6) 56 (49.1) 0.002 (Reference) 265 (50.5) 48 (49.0) (Reference) <4 97 (19.0) 37 (32.5) 1.747 (1.091-2.830) 100 (19.0) 34 (34.7) 4.900 × 10-4 1.877 (1.143-3.082) >4 155 (30.4) 21 (18.4) 0.624 (0.364-1.071) 160 (30.5) 16 (16.3) 0.552 (0.303-1.005) Total 510 (100.0) 114 (100.0) 525 (100.0) 98 (100.0) C4A = 2 330 (64.7) 65 (57.0) (Reference) 336 (64.0) 58 (59.2) (Reference) <2 52 (10.2) 27 (23.7) 0.001 2.646 (1.543-4.504) 57 (10.9) 22 (22.5) 0.008 2.236 (1.270-3.936) >2 128 (25.1) 22 (19.3) 0.873 (0.516-1.475) 132 (25.1) 18 (18.4) 0.790 (0.449-1.391) Total 510 (100.0) 114 (100.0) 525 (100.0) 98 (100.0) C4B = 2 310 (60.8) 67 (58.8) (Reference) 317 (60.4) 59 (60.2) (Reference) <2 112 (22.0) 31 (27.2) 0.414 1.281 (0.794-2.064) 115 (21.9) 28 (28.6) 0.168 1.308 (0.795-2.152) >2 88 (17.3) 16 (14.0) 0.841 (0.464-1.524) 93 (17.7) 11 (11.2) 0.636 (0.321-1.259) Total 510 (100.0) 114 (100.0) 525 (100.0) 98 (100.0)
Abbreviations: GO, Graves’ ophthalmology; CNV, copy number variation; OR, odds ratio; CI, confidence interval; N, number.
a
Copy numbers between patients and controls were evaluated by Fisher’s exact test using 3 × 2 contingency tables.
b
Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by applying unconditional logistic regression between GD patients with or without vitiligo or myxedema.