Lipoprotein(a) and Cardiovascular
Disease in Ethnic Chinese: The Chin-Shan
Community Cardiovascular Cohort Study
Kuo-Liong Chien,1,2*Hsiu-Ching Hsu,2Ta-Chen Su,2Fung-Chang Sung,3Ming-Fong Chen,2 and Yuan-Teh Lee2,4*
BACKGROUND: Little is known about lipoprotein(a)
[Lp(a)] as a predictor of vascular events among ethnic Chinese. We prospectively investigated the association of Lp(a) with cardiovascular disease and all-cause death in a community-based cohort.
METHODS: We conducted a community-based
prospec-tive cohort study of 3484 participants (53% women; age range, 35–97 years) who had complete lipid mea-surements and were free of a cardiovascular disease his-tory at the time of recruitment. Over a median fol-low-up of 13.8-years, we documented 210 cases of stroke, 122 cases of coronary heart disease (CHD), and 781 deaths.
RESULTS: The incidences for each event increased
ap-preciably with Lp(a) quartile for stroke and all-cause death, but not for CHD. Baseline Lp(a) concentration by quartile was not significantly associated with stroke, all-cause death, and CHD in multivariate analyses. The multivariate relative risk was significant for stroke at the 90th and 95th percentiles and for total death at the 95th and 99th percentiles.
CONCLUSIONS: Our findings suggest a threshold
rela-tionship with little gradient of risk across lower Lp(a) values for stroke and all-cause death in Chinese adults. © 2007 American Association for Clinical Chemistry
Lipoprotein(a) [Lp(a)]5 is a low-density lipoprotein particle in which apolipoprotein B-100 is linked by a single disulfide bridge to apolipoprotein(a), which is structurally similar to plasminogen (1, 2 ). The dual ef-fects of atherogenicity and thrombogenesis from Lp(a) particles make it plausible to investigate the role of
Lp(a) in atherosclerosis in a population; however, al-though many cross-sectional studies of hospital-based populations have consistently shown that Lp(a) is re-lated to various vascular diseases (3– 6 ), the evidence provided by many prospective cohort studies has been equivocal. In addition, previous large-scale prospective cohorts were restricted to women (7 ), to men (8 ), or to an older population (9, 10 ). Moreover, most studies have specified only one vascular outcome, either coro-nary heart disease (CHD) or stroke, whereas some studies have combined both outcomes into just one endpoint (9 ). Furthermore, the risk of Lp(a) with re-spect to cardiovascular events has varied according to ethnicity (11 ). Few prospective studies have investi-gated the role of Lp(a) among ethnic Chinese, who have cardiovascular disease patterns distinct from those of Caucasians and African Americans. Therefore, we prospectively investigated the association of plasma Lp(a) concentration with cardiovascular disease and all-cause death among ethnic Chinese in Taiwan. Materials and Methods
STUDY DESIGN AND STUDY PARTICIPANTS
The participants were enrolled in the Chin-Shan Community Cardiovascular Study, a prospective com-munity-based study of risk factors and cardiovascular consequences in men and women 35 years of age or older sponsored by the National Science Council, Tai-wan. The study was started in 1990 with an initial co-hort of 3602 participants, who were recruited on the basis of official registrations. The institutional review boards of the National Taiwan University approved the study. These participants were noninstitutionalized persons who gave oral informed consent to enter and
1Institute of Preventive Medicine, College of Public Health, National Taiwan
University, Taipei, Taiwan;2Department of Internal Medicine, National Taiwan
University Hospital, Taipei, Taiwan;3Institute of Environmental Health, College
of Public Health, China Medical University, Taichung, Taiwan;4Ming-Sheng
Healthcare, Taoyuang, Taiwan.
* Address correspondence to these authors at: Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan, 100. e-mail ytlee@ ha.mc.ntu.edu.tw.
Received April 27, 2007; accepted November 15, 2007. Previously published online at DOI: 10.1373/clinchem.2007.090969
5Nonstandard abbreviations: Lp(a), lipoprotein(a); CHD, coronary heart disease;
HDL-C, HDL cholesterol; LDL-C, LDL cholesterol; RR, relative risk; CI, confidence interval.
Clinical Chemistry 54:2 285–291 (2008)
ment process have been published elsewhere (12, 13 ). In brief, the study collected information regarding medical history, the results of a physical examination and laboratory tests, and an assessment of health status that included any evidence of cardiovascular disease in 1990 and 1991 and the follow-up periods (14 –16 ). We also collected detailed information about lifestyle fac-tors, including alcohol intake, smoking, and regular exercise, as well as data regarding socioeconomic sta-tus, including marital stasta-tus, educational level, and family history of CHD. We defined the cardiovascular disease at baseline according to the responses in the questionnaire about the history of stroke and CHD events. With regard to the follow-up schedule, we gathered information about cardiovascular events and deaths through monthly collections of official death certificate documents, by annual questionnaires, and by house-to-house visits.
ASCERTAINMENT OF EVENTS
The study outcomes were stroke, CHD, and all-cause death. Stroke was defined as a sudden neurologic defi-cit of vascular origin that lasted longer than 24 h that was supported by evidence from an imaging study. Transient ischemic attacks were not included in this definition. Incident CHD cases were defined as non-fatal myocardial infarction, non-fatal CHD, and hospital-ization for percutaneous coronary intervention and coronary artery bypass surgery. Fatal CHD was con-sidered to have occurred if fatal myocardial infarction was confirmed by hospital records, if CHD was listed as the cause of death on the death certificate or was the underlying and most plausible cause of death, or if evidence of previous CHD was available. Deaths from any cause were identified from official certificate doc-uments and further verified by house-to-house visits.
MEASUREMENTS OF BIOCHEMICAL VARIABLES
The procedures of blood sampling have been reported elsewhere (15, 17 ). In brief, all venous blood samples drawn after a 12-h overnight fast were immediately refrigerated and transported within 6 h to the Na-tional Taiwan University Hospital. Serum samples were then stored at⫺70 °C before batch assay of total cholesterol, triglycerides, and HDL cholesterol (HDL-C). Standard enzymatic tests for serum cholesterol and triglycerides were used (Merck 14354 and 14366, respectively). HDL-C concentrations were measured in supernatants after precipitation with magnesium chloride/phosphotungstate reagents (Merck 14993). The LDL cholesterol (LDL-C) concentration was cal-culated as the total cholesterol concentration minus the
were measured by turbidimetric immunoassay (19 ) with commercially available kits (Sigma-Aldrich). The concentration of non-HDL cholesterol was calculated by subtracting the HDL-C concentration from the con-centration of total cholesterol. Lp(a) was measured by isoform-independent ELISA (Organon). The CV for Lp(a) measurements was 5%. In this study, we in-cluded 3484 participants who had complete Lp(a) measurements and were free from cardiovascular dis-ease at baseline.
STATISTICAL ANALYSIS
Participants were classified by quartile of Lp(a) con-centration, and continuous variables were presented as the mean (SD) or the median; categorical data were presented in contingency tables. ANOVA and the 2 test were used to test differences between quartiles. Re-lationships between baseline Lp(a) concentrations and other obesity and lipid markers were evaluated with age- and sex-adjusted Spearman partial correlation coefficients.
Incidence rates for stroke, CHD, and all-cause death were calculated for each Lp(a) quartile by divid-ing the number of cases by the number of person-years of follow-up. The relative risk (RR) of an event was calculated by dividing the incidence rate for each quartile by the rate in the first quartile. We used Cox proportional hazards models to adjust for potential confounding variables. We specified 5 models for esti-mating the RRs of events in higher Lp(a) quartiles rel-ative to the lowest quartile. In model 1, we estimated the univariate RR of Lp(a) concentration with the first quartile as the reference. In model 2, we adjusted for age group (35– 44, 45–54, 55– 64, 65–74, orⱖ75 years) and sex variables. In model 3, we additionally adjusted for body mass index (⬍18, 18–20.9, 21–22.9, 23–24.9, orⱖ25 kg/m2), lifestyle factors [including alcohol in-take (nondrinker/current), smoking, (yes/no) and ex-ercise (yes/no)], and socioeconomic status [including marital status (single, married, or divorced/separated), educational level (⬍9 years/ⱖ9 years), occupation (no work, manual work, or professional), and family his-tory of CHD (yes/no)]. In model 4, we adjusted for the presence/absence of hypertension and diabetes at baseline along with adjustments for the variables in model 3. In model 5, we included the continuous vari-ables of HDL-C and LDL-C concentrations. In all anal-yses, we modeled Lp(a) concentrations as quartiles to avoid the assumption of linearity and to reduce the effects of outliers. Furthermore, we used median Lp(a) concentrations for the categories to test for linear trends across quartiles. We categorized the data
ac-cording to the 90th, 95th, and 99th percentiles and per-formed threshold analyses. We also used the test of Hosmer and Lemeshow to evaluate the goodness of fit of the data to the models (20 ).
All statistical tests were 2-tailed with a type I error of 0.05, and P values ⬍0.05 were considered statisti-cally significant. Analyses were performed with SAS software (version 9.1; SAS Institute) and Stata software (version 9.1; Stata Corporation).
Results
The participants in the highest Lp(a) quartile were less likely to drink alcohol and more likely to be in less professional jobs, compared with participants in the lower quartiles (Table 1). Participants had similar dis-tributions across quartiles for female sex, the presence of smoking, regular exercise, marital status, and edu-cational level. In addition, the participants had similar rates across Lp(a) quartiles for hypertension and dia-betes at baseline and for a family history of CHD. A higher Lp(a) concentration was associated with an older age and higher total cholesterol, LDL-C, and non-HDL cholesterol concentrations but was associ-ated with a lower body mass index and a lower tri-glyceride concentration. We found no statistically significant differences in mean values for HDL-C, apolipoprotein A-I, or apolipoprotein B across Lp(a) quartiles.
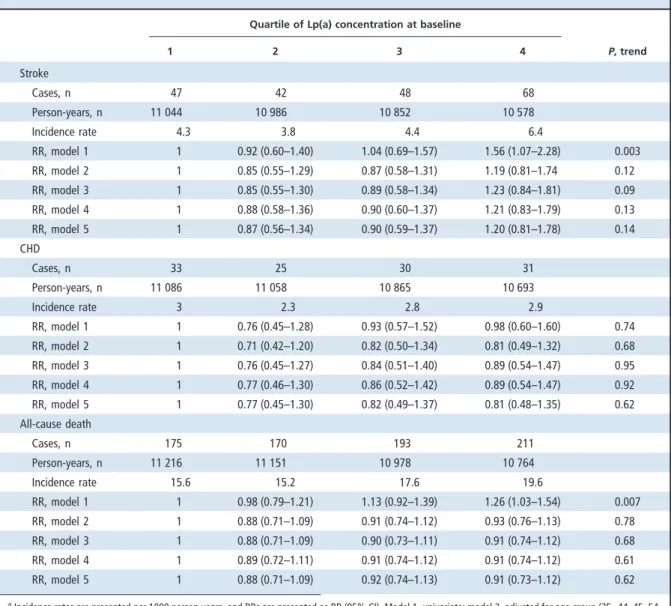
Over a median follow-up of 13.8 years (interquar-tile range, 13.5–14.6 years) for the 3484 participants, we documented 210 cases of stroke (including 184 nonhemorrhagic and 26 hemorrhagic strokes), 122 cases of CHD, and 781 deaths (including 165 car-diovascular deaths). The incidence rates for each event increased appreciably with Lp(a) quartile for stroke and all-cause death, and the rates were approximately the same across quartiles for CHD (Table 2). The RRs for individuals in the highest quartile of Lp(a) con-centration compared with those in the lowest quartile were 1.56 [95% confidence interval (CI), 1.07–2.28;
P for trend⫽ 0.003] for stroke and 1.26 (95% CI, 1.03–
1.54; P for trend⫽ 0.007) for all-cause death. In multi-variate analyses adjusted for potential confounding variables, baseline Lp(a) quartile values were not sig-nificantly associated with stroke, all-cause death, or CHD; however, in an evaluation of the risks of Lp(a) concentrations greater than or equal to the 90th, 95th, and 99th percentiles (i.e., cutoff concentrations of 0.3443 g/L, 0.4708 g/L, and 0.6930 g/L, respectively), the multivariate RR increased with the cutoff value and was statistically significant for stroke at the 90th and 95th percentiles and for all-cause deaths at the 95th
and 99th percentiles (Table 3). However, the RRs for CHD showed a statistically nonsignificant increasing trend, with little power.
To address the possibility that the associated risks of Lp(a) concentration vary by sex and age group, we performed stratified analyses according to par-ticipant sex and age and found no modification of the relationship between Lp(a) concentration and stroke after adjusting for these variables (all inter-action P values ⬎0.1; data not shown). Among par-ticipants older than 65 years, the association between Lp(a) concentration and stroke remained marginally significant after we adjusted for multivariate risk fac-tors, with the RR increasing from the second through the fourth quartiles (RRs, 1.05, 1.24, and 1.59, respec-tively; P for trend⫽ 0.055); however, these patterns were not apparent among participants younger than 65 years.
Discussion
Our data suggest a threshold relationship, with little gradient of risk for stroke and all-cause death across Lp(a) values among Chinese individuals. We found a marginally significant association between Lp(a) con-centration and stroke only in men 65 years of age and older. Moreover, the strength of the association of Lp(a) with stroke was attributable to the ischemic sub-type of stroke.
Different observational studies have provided conflicting evidence about the role that Lp(a) concen-tration plays in stroke. Rigal and colleagues conducted a case-control study of young adults (18 –55 years) consisting of 100 cases of ischemic stroke and 100 matched controls and found that the relationship of Lp(a) concentration with stroke remained significant in men (odds ratio, 3.55; 95% CI, 1.33–9.48, for the comparison of the highest and lowest tertiles) but not in women (odds ratio, 0.42; 95% CI, 0.14 –1.26) (21 ). In another case-control study of Japanese individuals, a high Lp(a) concentration was associated with isch-emic stroke (22 ). The weakness of these studies, however, is that the small sample sizes and the few ad-justments for confounding variables may have invali-dated the results. Nested case-control studies that ret-rospectively measured Lp(a) concentrations in stored samples, which may have been unstable, still did not prove a significant association with further stroke
(8, 23 ). Among the 198 incident stroke cases and 198
controls from 7.5 years of follow-up of a cohort of nearly 15 000 healthy male physicians, Ridker and col-leagues found no association between Lp(a) concentra-tion and the incidence of stroke (8 ).
Results based on prospective cohort studies are still inconsistent with respect to the relationship be-tween Lp(a) concentration and cardiovascular events. Ariyo and colleagues tracked cardiovascular and death events for 3972 older Caucasian adults 65 years and older during 7.4 years of follow-up. These investigators found that Lp(a) concentration remained a significant
predictor of stroke in men but found no relationship with CHD (9 ). Furthermore, they found no significant association between Lp(a) concentration and cardio-vascular outcomes among older women. In 3.2 years of follow-up of a cohort of 5732 elderly Caucasian men and women who had received statin treatment, Gaw and colleagues found no statistically significant
associ-P 1 2 3 4 (nⴝ 871) (nⴝ 871) (nⴝ 871) (nⴝ 871) Sex, % 0.67 Men 48.1 47.1 45.8 45.5 Women 51.9 52.9 54.2 54.5
Current smoker (yes), % 37.8 34.2 35.9 35.9 0.49
Alcohol drinking (yes), % 34.3 28.1 27.6 29.3 0.008
Marital status, % 0.10
Single 2.8 3.6 2.4 2.4
Living with spouse 88.0 85.5 85.8 84.1
Divorced or separated 9.2 10.9 11.8 13.5 Educational level, % 0.14 ⬍9 years 93.3 93.2 95.2 95.1 ⱖ9 years 6.7 6.8 4.8 4.9 Job status, % ⬍0.0001 No job 46.2 49.6 51.9 53.3 Manual labor 33.8 33.1 34.6 34.8 Professional 20.1 17.3 13.6 11.9
Regular exercise (yes), % 14.6 13.7 17.3 14.5 0.15
Family history of CHD, % 11.1 9.8 8.2 9.6 0.22
Hypertension, % 30.8 28.4 29.7 32.2 0.37
Diabetes, % 15.1 12.0 12.3 13.9 0.19
Age, yearsa 53.2 (11.5) 54.2 (12.5) 55.6 (12.2) 56.6 (12.8) ⬍0.0001
Body mass index, kg/m2a
24.0 (3.6) 23.5 (3.4) 23.2 (3.3) 23.2 (3.3) ⬍0.0001 TCb, mmol/La 4.95 (1.11) 5.04 (1.16) 5.15 (1.18) 5.32 (1.21) ⬍0.0001 Triglycerides, mmol/La 1.65 (1.315) 1.46 (1.144) 1.32 (0.931) 1.28 (0.802) ⬍0.0001 HDL-C, mmol/La 1.22 (0.36) 1.22 (0.32) 1.23 (0.31) 1.24 (0.31) 0.3 LDL-C, mmol/La 3.39 (1.09) 3.49 (1.12) 3.61 (1.15) 3.76 (1.19) ⬍0.0001 Non–HDL-C, mmol/La 3.72 (1.13) 3.82 (1.17) 3.92 (1.18) 4.07 (1.22) ⬍0.0001 TC/HDL-Ca 4.39 (1.62) 4.40 (1.52) 4.42 (1.42) 4.53 (1.50) 0.2 Apo A-I, g/La 1.360 (0.544) 1.323 (0.285) 1.338 (0.264) 1.327 (0.263) 0.1 Apo B, g/La 0.953 (0.465) 0.941 (0.316) 0.978 (0.454) 0.969 (0.665) 0.4 Apo B/Apo A-Ia 0.73 (0.40) 0.73 (0.25) 0.75 (0.34) 0.75 (0.52) 0.6
aData are expressed as the mean (SD). bTC, total cholesterol; Apo, apolipoprotein.
ation of log-transformed Lp(a) concentration with stroke and coronary events in a univariate analysis
(10 ). Among 27 791 healthy, mostly Caucasian women
in the Women’s Health Study who were followed for 10 years, a clear threshold effect was seen for Lp(a) con-centration (7 ); that is, the association of Lp(a) with total cardiovascular events remained significant only at extremely high Lp(a) concentrations. Virtually no risk gradient was seen among these women at the lower Lp(a) quintiles. Ohira and colleagues examined the
as-sociation between Lp(a) concentration and ischemic stroke in a biracial population of 14 221 middle-aged adults followed up for 13.5 years and found an appre-ciable association in African Americans and Caucasian women, but not in Caucasian men (11 ). Our data sug-gest a threshold effect for stroke: the risks of stroke above the 90th and 95th Lp(a) percentiles were signif-icant, implying that atherosclerotic burdens increased appreciably among individuals with extremely high Lp(a) concentrations.
Table 2. Incidence cases, person-years, incidence rates, and RRs for stroke, CHD, and all-cause death outcomes during a median follow-up of 13.6 years, according to quartile of Lp(a) concentration at baseline (1990 –1991) in
the Chin-Shan Community Cardiovascular Study.a Quartile of Lp(a) concentration at baseline
P, trend 1 2 3 4 Stroke Cases, n 47 42 48 68 Person-years, n 11 044 10 986 10 852 10 578 Incidence rate 4.3 3.8 4.4 6.4 RR, model 1 1 0.92 (0.60–1.40) 1.04 (0.69–1.57) 1.56 (1.07–2.28) 0.003 RR, model 2 1 0.85 (0.55–1.29) 0.87 (0.58–1.31) 1.19 (0.81–1.74 0.12 RR, model 3 1 0.85 (0.55–1.30) 0.89 (0.58–1.34) 1.23 (0.84–1.81) 0.09 RR, model 4 1 0.88 (0.58–1.36) 0.90 (0.60–1.37) 1.21 (0.83–1.79) 0.13 RR, model 5 1 0.87 (0.56–1.34) 0.90 (0.59–1.37) 1.20 (0.81–1.78) 0.14 CHD Cases, n 33 25 30 31 Person-years, n 11 086 11 058 10 865 10 693 Incidence rate 3 2.3 2.8 2.9 RR, model 1 1 0.76 (0.45–1.28) 0.93 (0.57–1.52) 0.98 (0.60–1.60) 0.74 RR, model 2 1 0.71 (0.42–1.20) 0.82 (0.50–1.34) 0.81 (0.49–1.32) 0.68 RR, model 3 1 0.76 (0.45–1.27) 0.84 (0.51–1.40) 0.89 (0.54–1.47) 0.95 RR, model 4 1 0.77 (0.46–1.30) 0.86 (0.52–1.42) 0.89 (0.54–1.47) 0.92 RR, model 5 1 0.77 (0.45–1.30) 0.82 (0.49–1.37) 0.81 (0.48–1.35) 0.62 All-cause death Cases, n 175 170 193 211 Person-years, n 11 216 11 151 10 978 10 764 Incidence rate 15.6 15.2 17.6 19.6 RR, model 1 1 0.98 (0.79–1.21) 1.13 (0.92–1.39) 1.26 (1.03–1.54) 0.007 RR, model 2 1 0.88 (0.71–1.09) 0.91 (0.74–1.12) 0.93 (0.76–1.13) 0.78 RR, model 3 1 0.88 (0.71–1.09) 0.90 (0.73–1.11) 0.91 (0.74–1.12) 0.68 RR, model 4 1 0.89 (0.72–1.11) 0.91 (0.74–1.12) 0.91 (0.74–1.12) 0.61 RR, model 5 1 0.88 (0.71–1.09) 0.92 (0.74–1.13) 0.91 (0.73–1.12) 0.62
aIncidence rates are presented per 1000 person-years, and RRs are presented as RR (95% CI). Model 1, univariate; model 2, adjusted for age group (35– 44, 45–54,
55– 64, 65–74,ⱖ75 years) and sex; model 3, model 2 plus body mass index (⬍18, 18–20.9, 21–22.9, 23–24.9, or ⱖ25 kg/m2), smoking (yes/no or abstinence),
current alcohol drinking (regular/no), marital status (single, married and living with spouse, or divorced/separated), educational level (⬍9 years/ⱖ9 years), occupation (no work, manual labor, or official/business), regular exercise (yes/no), and family history of CHD (yes/no); model 4, model 3 plus hypertension (yes/no) and diabetes mellitus (yes/no); model 5, model 4 plus HDL-C and LDL-C concentrations.
Our negative results with respect to the relation-ship of Lp(a) concentration to CHD are comparable with those of previous cohort studies of Caucasian and African American populations (9, 10 ) but are not consistent with the positive association reported in the nested case-control study (24 ). Rifai and colleagues conducted a nested case-control study and collected Lp(a) and apolipoprotein(a) data from 195 men who developed severe coronary atherosclerosis during a 5-year follow-up and 195 matched controls in the Physicians’ Health Study (24 ). Although 2 metaanaly-ses indicated a significant association between Lp(a) concentration and the risk for CHD, the results may not be valid for different populations because of het-erogeneity in participant characteristics and the study
(25, 26 ).
The inconsistency of the findings among these different studies is troublesome and begs explanation
(27 ). One proposed explanation has been that Lp(a)
interacts with age with respect to further cardiovas-cular events. Sex, a younger or older age, and the presence of high LDL-C and triglyceride
concentra-tionship among older Chinese men that is compatible with the findings of the Cardiovascular Health Study
(9 ). A specific high-risk population that includes type 2
diabetes and hypercholesterolemia may provide new evidence for the role of Lp(a) in cardiovascular disease
(28 ).
To our knowledge, this investigation is the first extensive study of Lp(a) and the risks of stroke, CHD, and all-cause death among ethnic Chinese. Because of the prospective cohort design, the baseline mea-surements of all cohort members were unlikely to have been affected by storage and laboratory issues that might be raised in some nested case-control studies. The use of a homogeneous community-based population may have reduced the possibility of selec-tion bias. We also included important socioeconomic status and lifestyle factors in the models to control for potential confounding factors. Finally, because few of the participants (⬍1%) reported taking cholesterol-lowering medications, our results were minimally af-fected by statins and other cholesterol-lowering drugs.
Our study had several potential limitations. First, the incident cases of stroke and CHD were relatively few, even with a median follow-up of 13.8 years, and this fact would reduce the power to detect subtle dif-ferences in effects between Lp(a) concentrations and make RR estimation unstable. Second, because Lp(a) concentrations were measured only once, our results might be attenuated by intraindividual variations.
In conclusion, our data do not support the hy-pothesis that an increase in Lp(a) concentration, over most of its range, is significantly associated with stroke, CHD, or all-cause death among ethnic Chinese adults. Only a small proportion of people with ex-tremely high Lp(a) concentrations were at excess risk. These findings limit the use of Lp(a) as a bio-marker for the comprehensive evaluation of risk for cardiovascular disease in Chinese populations; how-ever, a single measure of Lp(a) concentration to iden-tify the small subgroup with extreme values may have some utility.
Grant/funding Support: This study was supported by a grant from the National Science Council in Taiwan (NSC 96-2314-B-002-155).
Financial Disclosures: None declared.
Acknowledgments: We thank the participants in the Chin-Shan community and the cardiologists at Na-tional Taiwan University Hospital for their assistance in this study.
percentiles of Lp(a) concentration at baseline (1990 –1991) in the Chin-Shan Community
Cardiovascular Study.a RR (95% CI) P Stroke ⱖ90th/⬍90th percentile 1.50 (1.01–2.22) 0.045 ⱖ95th/⬍95th percentile 1.75 (1.04–2.93) 0.035 ⱖ99th/⬍99th percentile 0.60 (0.08–4.34) 0.62 CHD ⱖ90th/⬍90th percentile 1.24 (0.73–2.13) 0.43 ⱖ95th/⬍95th percentile 1.71 (0.89–3.30) 0.11 ⱖ99th/⬍99th percentile 2.11 (0.51–8.73) 0.30 All-cause death ⱖ90th/⬍90th percentile 1.17 (0.93–1.45) 0.18 ⱖ95th/⬍95th percentile 1.39 (1.04–1.86) 0.025 ⱖ99th/⬍99th percentile 1.96 (1.10–3.49) 0.022
aAdjusted variables included age group (35– 44, 45–54, 55– 64, 65–74, or
ⱖ75 years), sex, body mass index (⬍18, 18–20.9, 21–22.9, 23–24.9, or ⱖ25 kg/m2), smoking (yes/no or abstinence), current alcohol drinking
(regular/no), marital status (single, married and living with spouse, or divorced/separated), educational level (⬍9 years/ⱖ9 years), occupation (no work, manual labor, or official/business), regular exercise (yes/no), family history of CHD (yes/no), hypertension (yes/no), diabetes mellitus (yes/no), and HDL-C and LDL-C concentrations.
References
1. Loscalzo J. Lipoprotein(a). A unique risk factor for
atherothrombotic disease. Arteriosclerosis 1990; 10:672–9.
2. Gaubatz JW, Heideman C, Gotto AM Jr, Morrisett
JD, Dahlen GH. Human plasma lipoprotein [a]. Structural properties. J Biol Chem 1983;258: 4582–9.
3. Frohlich J, Dobia´sova´ M, Adler L, Francis M.
Gender differences in plasma levels of lipoprotein (a) in patients with angiographically proven cor-onary artery disease. Physiol Res 2004;53:481– 6.
4. Jovicic A, Ivanisevic V, Ivanovic I. Lipoprotein(a)
in patients with carotid atherosclerosis and isch-emic cerebrovascular disorders. Atherosclerosis 1993;98:59 – 65.
5. Pantoni L, Sarti C, Pracucci G, Di CA, Vanni P,
Inzitari D. Lipoprotein(a) serum levels and vascu-lar diseases in an older Caucasian population cohort. Italian Longitudinal Study on Aging (ILSA). J Am Geriatr Soc 2001;49:117–25.
6. Jones GT, van Rij AM, Cole J, Williams MJ,
Bate-man EH, Marcovina SM, et al. Plasma lipopro-tein(a) indicates risk for 4 distinct forms of vas-cular disease. Clin Chem 2007;53:679 – 85.
7. Suk Danik J, Rifai N, Buring JE, Ridker PM.
Li-poprotein(a), measured with an assay indepen-dent of apolipoprotein(a) isoform size, and risk of future cardiovascular events among initially healthy women. JAMA 2006;296:1363–70.
8. Ridker PM, Stampfer MJ, Hennekens CH. Plasma
concentration of lipoprotein(a) and the risk of future stroke. JAMA 1995;273:1269 –73.
9. Ariyo AA, Thach C, Tracy R, for the Cardiovascular
Health Study investigators. Lp(a) lipoprotein, vas-cular disease, and mortality in the elderly. N Engl J Med 2003;349:2108 –15.
10. Gaw A, Murray HM, Brown EA, the PROSPER
study group. Plasma lipoprotein(a) [Lp(a)] con-centrations and cardiovascular events in the elderly: evidence from the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER). Ath-erosclerosis 2005;180:381– 8.
11. Ohira T, Schreiner PJ, Morrisett JD, Chambless LE,
Rosamond WD, Folsom AR. Lipoprotein(a) and incident ischemic stroke: the Atherosclerosis Risk in Communities (ARIC) study. Stroke 2006;37: 1407–12.
12. Lee YT, Lin RS, Sung FC, Yang CY, Chien KL, Chen
WJ, et al. Chin-Shan Community Cardiovascular Cohort in Taiwan: baseline data and five-year follow-up morbidity and mortality. J Clin Epide-miol 2000;53:836 – 46.
13. Chien KL, Lee YT, Sung FC, Su TC, Hsu HC, Lin RS.
Lipoprotein (a) level in the population in Taiwan: relationship to sociodemographic and atheroscle-rotic risk factors. Atherosclerosis 1999;143:267– 73.
14. Chien KL, Hsu HC, Sung FC, Su TC, Chen MF, Lee
YT. Metabolic syndrome as a risk factor for cor-onary heart disease and stroke: an 11-year pro-spective cohort in Taiwan community. Athero-sclerosis 2007;194:214 –21.
15. Chien KL, Sung FC, Hsu HC, Su TC, Chang WD,
Lee YT. Relative importance of atherosclerotic risk factors for coronary heart disease in Tai-wan. Eur J Cardiovasc Prev Rehabil 2005;12: 95–101.
16. Chien KL, Sung FC, Hsu HC, Su TC, Lin RS, Lee YT.
Apolipoprotein A-I and B and stroke events in a community-based cohort in Taiwan: report of Chin-Shan Community Cardiovascular Study. Stroke 2002;33:39 – 44.
17. Chien KL, Lee YT, Sung FC, Hsu HC, Su TC, Lin RS.
Hyperinsulinemia and related atherosclerotic risk factors in the population at cardiovascular risk: a community-based study. Clin Chem 1999;45: 838 – 46.
18. Wieland H, Seidel D. A simple specific method for
precipitation of low density lipoproteins. J Lipid Res 1983;24:904 –9.
19. Siedel J, Schiefer S, Rosseneu M, Bergeaud R, De
Keersgieter W, Pautz B, et al. Immunoturbidimet-ric method for routine determinations of apoli-poproteins A-I, A-II, and B in normo- and
hyper-lipemic sera compared with immunonephelo-metry. Clin Chem 1988;34:1821–5.
20. Hosmer DW Jr, Lemeshow S. Applied logistic
regression. New York: John Wiley & Sons, 1989: 25–37.
21. Rigal M, Ruidavets JB, Viguier A, Petit R, Perret B,
Ferrieres J, Larrue V. Lipoprotein (a) and risk of ischemic stroke in young adults. J Neurol Sci 2007;252:39 – 44.
22. Nagayama M, Shinohara Y, Nagayama T.
Li-poprotein (a) and ischemic cerebrovascular dis-ease in young adults. Stroke 1994;25:74 – 8.
23. Glader CA, Stegmayr B, Boman J, Stenlund H,
Weinehall L, Hallmans G, Dahlen GH.Chlamydia pneumoniae antibodies and high lipoprotein(a) levels do not predict ischemic cerebral infarctions. Results from a nested case-control study in Northern Sweden. Stroke 1999;30:2013– 8.
24. Rifai N, Ma J, Sacks FM, Ridker PM, Hernandez
WJ, Stampfer MJ, Marcovina SM. Apolipopro-tein(a) size and lipoproApolipopro-tein(a) concentration and future risk of angina pectoris with evidence of severe coronary atherosclerosis in men: the Phy-sicians’ Health Study. Clin Chem 2004;50:1364 – 71.
25. Craig WY, Neveux LM, Palomaki GE, Cleveland
MM, Haddow JE. Lipoprotein(a) as a risk factor for ischemic heart disease: metaanalysis of pro-spective studies. Clin Chem 1998;44:2301– 6.
26. Danesh J, Collins R, Peto R. Lipoprotein(a) and
coronary heart disease. Meta-analysis of prospec-tive studies. Circulation 2000;102:1082–5.
27. Berglund L, Ramakrishnan R. Lipoprotein(a): an
elusive cardiovascular risk factor. Arterioscler Thromb Vasc Biol 2004;24:2219 –26.
28. Shai I, Schulze MB, Manson JE, Stampfer MJ, Rifai
N, Hu FB. A prospective study of lipoprotein(a) and risk of coronary heart disease among women with type 2 diabetes. Diabetologia 2005;48: 1469 –76.