Occupational Exposure to Wood, Formaldehyde, and Solvents and Risk
of Nasopharyngeal Carcinoma
Allan Hildesheim,1
Mustafa Dosemeci,
Chang-Chuan Chan, Chien-Jen Chen, Yu-Juen Cheng, Mow-Ming Hsu, I-How Chen,2
Beth F. Mittl, Brenda Sun, Paul H. Levine,3
Jen-Yang Chen,4
Louise A. Brinton, and Czau-Siung Yang
Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, Maryland 20892 [A. H., M. D., P. H. L., L. A. B.]; Graduate Institute of Occupational Medicine and Industrial Hygiene, College of Public Health [C-C. C.], Institute of Epidemiology, College of Public Health [C-J. C., Y-J. C.], Department of Otolaryngology [M-M. H.], and Department of Microbiology, College of Medicine [J.-Y. C., C-S. Y.], National Taiwan University, Taipei, Taiwan; Department of Otolaryngology, MacKay Memorial Hospital, Taipei, Taiwan [I-H. C.]; and Westat, Inc., Rockville, Maryland [B. F. M., B. S.]
Abstract
Our objective was to evaluate the link between
occupational exposures to wood dust, formaldehyde, and solvents and the development of nasopharyngeal carcinoma (NPC). A case-control study was conducted among 375 newly diagnosed cases of NPC in Taipei, Taiwan, and 325 community controls matched to cases on sex, age, and geographical residence (99 and 87% response rates, respectively). Most cases (>90%) were diagnosed with WHO Types 2 or 3 (nonkeratinizing and undifferentiated carcinomas), whereas the remaining cases were diagnosed with WHO Type 1 (squamous cell carcinomas). A complete occupational history was obtained via a personal interview and blindly assessed by an industrial hygienist for intensity and probability of exposure to wood dust, formaldehyde, and solvents. Information on socio-demographic characteristics, cigarette smoking, dietary consumption of nitrosamines, and other potential confounding factors was obtained via a personal interview. Blood specimens were tested for human leukocyte antigen class I/II genotypes,
polymorphisms in cytochrome P450 2E1 genotype, and various anti-EBV antibodies known to be associated with NPC. Analysis was performed using logistic regression; relative risk (RR) estimates and 95% confidence intervals (CI) were calculated. Individuals exposed to wood dust
had an adjusted RR of 1.7 (95% CIⴝ 1.0–3.0). Those exposed to wood dust for>10 years had an adjusted RR of 2.4 (95% CIⴝ 1.1–5.0; ptrendⴝ 0.02). Risk was
strongest for those first exposed before the age of 25 years and those seropositive to EBV. Individuals exposed to formaldehyde were at a more modest and
nonsignificant increased risk of NPC (RRⴝ 1.4; 95% CIⴝ 0.93–2.2). Those exposed to formaldehyde for >10 years had an adjusted RR of 1.6 (95% CIⴝ 0.91–2.9). The association between formaldehyde and NPC was stronger in analyses restricted to EBV seropositive individuals (RRⴝ 2.7; 95% CI ⴝ 1.2–5.9). However, no dose response was observed with increasing duration or cumulative use. No association was observed between solvent exposure and NPC (RRⴝ 1.2; 95% CI ⴝ 0.86– 1.7). Occupational exposure to wood dust is likely to be involved in the development of NPC, a finding that is consistent with the known link between wood exposure and nasal adenocarcinomas. Formaldehyde exposure is less clearly linked to NPC, whereas exposure to solvents is unlikely to be involved in NPC pathogenesis.
Introduction NPC5
is rare in most parts of the world but is endemic in some regions, particularly Southeastern Asia (1). The histological distribution of NPC varies in different regions. In areas with high rates of disease, nonkeratinizing and undifferentiated car-cinomas predominate (WHO Types 2 and 3), whereas in low risk regions, squamous cell carcinomas (WHO Type 1) are predominant (1). The most prominent risk factor for all histo-logical types of NPC is infection with the EBV. Whereas EBV is ubiquitous and establishes lifelong infections in humans, only a very small fraction of individuals infected with the virus develop NPC. Those that do typically present with an altered profile of antibodies against EBV, sometimes years preceding diagnosis of the disease (1, 2). Although EBV is believed by many to be a necessary cause of NPC, it is unlikely to be sufficient for the development of the disease. Other factors, both exogenous (diet and smoking) and host factors (HLA and CYP2E1) have been shown to be associated with the develop-ment of this tumor (3). Recent data suggest that risk factors for NPC other than EBV may vary by histology (4, 5).
The link between occupational exposures and the devel-opment of NPC is poorly understood. With a few notable exceptions (5–10), most studies that have examined occupa-tional factors and NPC risk have suffered from small numbers of cases or have had incomplete assessment of occupational exposures (11–27). Mixed findings have been reported in the
Received 2/9/01; revised 8/7/01; accepted 9/5/01.
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1To whom requests for reprints should be addressed, at Environmental Epide-miology Branch, Division of Cancer EpideEpide-miology and Genetics, National Can-cer Institute, 6120 Executive Boulevard, Room 7062, Bethesda, MD 20892. E-mail: [email protected].
2Present address: Department of Otolaryngology, Chang-Gung Memorial Hos-pital, Lin-Ko, Taiwan.
3Present address: School of Public Health and Health Services, George Wash-ington University, WashWash-ington, DC.
4Present address: National Health Research Institute, Taipei, Taiwan.
5The abbreviations used are: NPC, nasopharyngeal carcinoma; CI, confidence interval; CYP2E1, cytochrome P450 2E1; HLA, human leukocyte antigen; RR, relative risk.
literature, but available evidence points to a possible role of wood dust and formaldehyde exposure in the development of NPC (5, 6, 11). A meta-analysis conducted in 1993 suggested that formaldehyde is associated with a doubling in the risk of NPC (95% CI⫽ 1.4–2.9), but results were based on 36 ex-posed cases, and confounding by other exogenous and/or host factors could not be taken into account (11). In a case-control study conducted in the Philippines (104 cases and 205 con-trols), formaldehyde and wood dust/exhaust exposures were associated with risk of NPC. Risk was particularly high among those exposed early in life and those with extended intervals since first exposure (6). In a United States-based case-control study (196 cases and 244 controls), formaldehyde was associ-ated with NPC risk, but wood dust exposure was not (5). In this study, the association between formaldehyde and NPC was restricted to those diagnosed with squamous cell carci-nomas (5).
A recent review (28) by the IARC concluded that: (a) wood dust is a human carcinogen (supported largely by studies demonstrating a consistent association between wood dust posure and nasal adenocarcinomas); and (b) formaldehyde ex-posure is a probable human carcinogen (based largely on strong animal data combined with limited evidence in humans). Whereas the link between wood dust exposure and nasal ade-nocarcinomas is irrefutable, the association observed between wood dust exposure and nasal and nasopharyngeal squamous carcinomas has been weaker and less consistent across studies (29). In addition to wood dust and formaldehyde, solvents have been suggested to be linked to the development of NPC in at least one study in China (30), although a subsequent study in the Philippines failed to confirm this association (6).
To evaluate the role of wood, formaldehyde, and solvent exposure in the development of NPC, we conducted a case-control study in Taiwan, a country with intermediate rates of NPC (31). Complete occupational histories were obtained from a group of 700 individuals (375 cases and 325 controls) and evaluated for their link to disease.
Materials and Methods
Cases. Details of our case-control study methods have been described previously (31, 32). In brief, incident NPC cases were identified through two tertiary care hospitals in Taipei, Taiwan between July 15, 1991 and December 31, 1994. To be eligible, cases were required to have newly diagnosed, histologically confirmed NPC, to be⬍75 years of age, and to be residents of Taipei city or county for at least 6 months. Of the 378 eligible cases identified, 375 (99%) agreed to participate in our study. Controls. Controls were individually matched to NPC cases at a 1:1 ratio on age (within 5 years), sex, and district/township of residence. Matching was accomplished by use of listings avail-able through the National Household Registration System. To match on residence, each control subject was selected by vis-iting the registry office located in the district (if in Taipei city) or township (if in Taipei county) in which the case subject resided. Within these large geographical units, a random Li (communities of 1000 –1500 households within each district/ township) was selected. From within the selected Li, a random Lin (neighborhoods of 50 –100 households) was selected. In-dividuals within the selected Lin were then enumerated, and a control who matched the eligible NPC case subject on age and sex was randomly selected. Controls were required to have been residents of Taipei city or county forⱖ6 months and to have no history of NPC before identification for our study. Ineligible controls were replaced, but those who refused
par-ticipation were not. Controls (327; 87% of those eligible) agreed to participate.
Risk Factor Questionnaire. An extensive in-person risk fac-tor questionnaire was administered to all study participants by a trained nurse interviewer. For cases, interviews were con-ducted at the time of biopsy for histological confirmation of NPC and always before treatment. The questionnaire elicited information on socio-demographic characteristics, adult and childhood diet, cigarette smoking and betel quid chewing, al-cohol consumption, residential history, and medical history. A complete occupational history was also obtained from partici-pants. Study subjects were asked to report all jobs held forⱖ1 year since the age of 16. Information on jobs held for a year or longer before the age of 16 was also recorded if they were for half-time or greater (⬎20 h/week). For each job held for a year or longer, participants were asked to specify their job title, type of business or industry, job activities, and duties and to list specific tools and/or materials used on the job. Living mothers of cases and controls were also interviewed to obtain informa-tion on dietary patterns of their children during childhood and weaning. Mother interviews were successfully obtained for 96 case mothers (47.3% of eligibles) and 120 control mothers (63.2% of eligibles; Ref. 33).
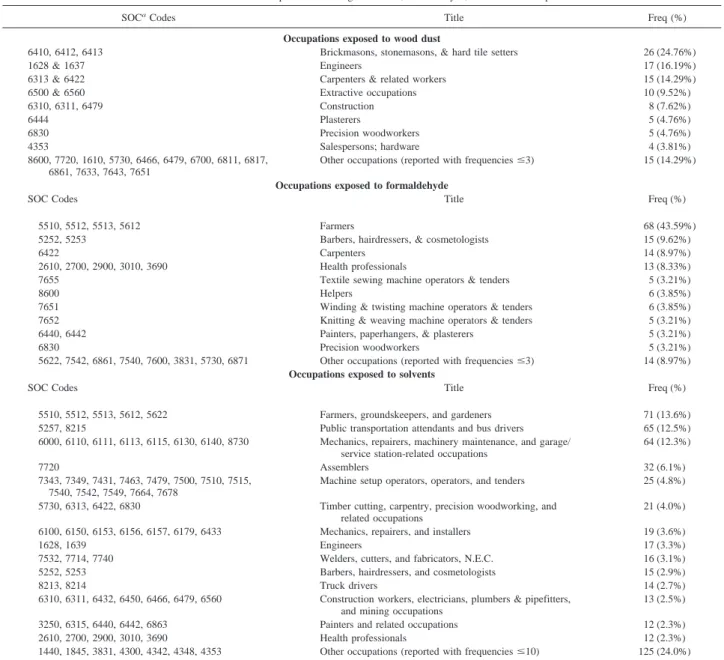
Exposure Assessment. Occupational history data were re-viewed (blinded to case-control status) by the study industrial hygienist (M. D.). Standard Industry Classification and Standard Occupational Classification codes were assigned to each occupa-tion (34, 35). Each Standard Industry Classificaoccupa-tion/Standard Occupational Classification code was evaluated separately for probability and intensity of exposure to formaldehyde, wood, and organic solvents, as described previously (36, 37). Occupations were classified separately on a scale of 0 (not exposed) to 9 (strong) on both the probability and intensity of each of these three exposures. For each subject, this information was combined with duration data to estimate the following: (a) years of exposure; (b) average intensity of exposure [defined as兺 (intensity index for each job ⫻ duration of employment)/兺 years of exposure]; (c) average probability of exposure [similarly defined as兺 (prob-ability index for each job⫻ duration of employment)/兺 years of exposure]; (d) cumulative exposure (defined as intensity years of exposure, i.e., duration of exposure,⫻ average intensity); (e) age at first exposure; and (f) years since first exposure. In addition, duration of exposure was recalculated after exclusion of exposures occurring in the 10 years preceding diagnosis (cases) or interview (controls). Jobs involving wood exposure were classified based on whether exposure was likely to be to hardwood alone, softwood alone, or both. This was done based on potential use of wood type for each reported occupation. We also attempted to classify jobs with respect to whether they involved the use of treated or un-treated wood. However, the lack of participants with occupational exposure to exclusively untreated wood (one case and zero con-trols) precluded examination of this issue. For analysis purposes, probability and intensity of exposure were considered low if they were ⬍4 and high if they were ⱖ4. Occupational data were available for all 375 NPC cases (100%) and 325 of the 327 controls (99.4%). A total of 2034 jobs (1069 from cases and 965 from controls) were reported by the 700 subjects in our study (median⫽ 3; range ⫽ 0–10). Of these, 105 occupations (5.2%) were classified by the industrial hygienist as involving exposure to wood dust; 156 occupations (7.7%) were classified by the indus-trial hygienist as involving exposure to formaldehyde; 521 were classified by the industrial hygienist as involving exposure to solvents (25.6%). The distribution of occupations with wood dust, formaldehyde, and/or solvent exposure is presented in Table 1.
Biological Specimen Collection and Testing. Peripheral blood specimens were collected from 369 cases and 320 con-trols, processed, and stored, as described previously (32). Se-rum was used to test for various anti-EBV antibodies known to be associated with NPC, including viral capsid antigen IgA, EBV nuclear antigen 1 IgA, early antigen IgA, DNA binding protein IgG, and anti-DNase IgG (38 – 41). Individuals positive for any of these EBV markers were considered seropositive, and those negative to all were classified as seronegative. DNA extracted from peripheral blood mononuclear cells was tested for CYP2E1 RSAI polymorphism and classified as homozy-gous for the wild-type allele, heterozyhomozy-gous, or homozyhomozy-gous for the variant allele, as described previously (32). DNA was also used for HLA class I and II antigen testing using a novel strip-based, sequence-specific oligonucleotide probe method (42– 44). For purposes of the present analysis, subjects positive
for any of the following HLA alleles found to be positively associated with NPC risk in our study were classified as pos-itive for “at-risk” alleles (HLA A*0207, A*3303, B*4601, B*5801, DRB1*0301, and DPB1*0401), and the remaining participants were classified as negative for “at-risk” alleles. Statistical Analysis. The RR, as estimated by the odds ratio, was used to assess associations between risk factors and dis-ease. Statistical significance was determined by use of the 95% CI. Logistic regression was used to assess the association be-tween exposures of interest and disease, while controlling for age, sex, and other potential confounding factors. Conditional logistic regression was not chosen to avoid loss of information from cases and controls without a matched pair. Relationships that appeared to increase with increasing levels of exposure were evaluated for significance of the trend by entering the Table 1 Distribution of occupations involving wood dust, formaldehyde, and/or solvent exposure
SOCaCodes Title Freq (%)
Occupations exposed to wood dust
6410, 6412, 6413 Brickmasons, stonemasons, & hard tile setters 26 (24.76%)
1628 & 1637 Engineers 17 (16.19%)
6313 & 6422 Carpenters & related workers 15 (14.29%)
6500 & 6560 Extractive occupations 10 (9.52%)
6310, 6311, 6479 Construction 8 (7.62%) 6444 Plasterers 5 (4.76%) 6830 Precision woodworkers 5 (4.76%) 4353 Salespersons; hardware 4 (3.81%) 8600, 7720, 1610, 5730, 6466, 6479, 6700, 6811, 6817, 6861, 7633, 7643, 7651
Other occupations (reported with frequenciesⱕ3) 15 (14.29%)
Occupations exposed to formaldehyde
SOC Codes Title Freq (%)
5510, 5512, 5513, 5612 Farmers 68 (43.59%)
5252, 5253 Barbers, hairdressers, & cosmetologists 15 (9.62%)
6422 Carpenters 14 (8.97%)
2610, 2700, 2900, 3010, 3690 Health professionals 13 (8.33%)
7655 Textile sewing machine operators & tenders 5 (3.21%)
8600 Helpers 6 (3.85%)
7651 Winding & twisting machine operators & tenders 6 (3.85%)
7652 Knitting & weaving machine operators & tenders 5 (3.21%)
6440, 6442 Painters, paperhangers, & plasterers 5 (3.21%)
6830 Precision woodworkers 5 (3.21%)
5622, 7542, 6861, 7540, 7600, 3831, 5730, 6871 Other occupations (reported with frequenciesⱕ3) 14 (8.97%)
Occupations exposed to solvents
SOC Codes Title Freq (%)
5510, 5512, 5513, 5612, 5622 Farmers, groundskeepers, and gardeners 71 (13.6%)
5257, 8215 Public transportation attendants and bus drivers 65 (12.5%)
6000, 6110, 6111, 6113, 6115, 6130, 6140, 8730 Mechanics, repairers, machinery maintenance, and garage/ service station-related occupations
64 (12.3%)
7720 Assemblers 32 (6.1%)
7343, 7349, 7431, 7463, 7479, 7500, 7510, 7515, 7540, 7542, 7549, 7664, 7678
Machine setup operators, operators, and tenders 25 (4.8%) 5730, 6313, 6422, 6830 Timber cutting, carpentry, precision woodworking, and
related occupations
21 (4.0%) 6100, 6150, 6153, 6156, 6157, 6179, 6433 Mechanics, repairers, and installers 19 (3.6%)
1628, 1639 Engineers 17 (3.3%)
7532, 7714, 7740 Welders, cutters, and fabricators, N.E.C. 16 (3.1%)
5252, 5253 Barbers, hairdressers, and cosmetologists 15 (2.9%)
8213, 8214 Truck drivers 14 (2.7%)
6310, 6311, 6432, 6450, 6466, 6479, 6560 Construction workers, electricians, plumbers & pipefitters, and mining occupations
13 (2.5%) 3250, 6315, 6440, 6442, 6863 Painters and related occupations 12 (2.3%)
2610, 2700, 2900, 3010, 3690 Health professionals 12 (2.3%)
1440, 1845, 3831, 4300, 4342, 4348, 4353 Other occupations (reported with frequenciesⱕ10) 125 (24.0%)
categorical variable as continuous in the logistic model and assessing whether the coefficient departed from 0. The cor-relation between exposures was assessed by means of the Spearman correlation coefficient. Crude distribution and ad-justed RR estimates are presented in the text and tables. RR estimates were adjusted for age, sex, education, ethnicity, and presence of at-risk HLA alleles (for wood exposure only; see first paragraph of “Results” below). Additional adjustment for family history of NPC, cigarette smoking, CYP2E1 RSAI gen-otype, dietary nitrosamine consumption during childhood (at age 10), and presence of at-risk HLA alleles (for formaldehyde and solvents) did not materially affect risk estimates (data not shown). Because ⬎95% of NPC cases were seropositive for one or more of the anti-EBV antibodies measured, and because EBV is considered by many to be a necessary risk factor for the development of NPC, the effect of EBV seropositivity on risk associated with occupational exposures was assessed through stratification (rather than statistical adjustment). Stratified anal-yses were also conducted to examine effects among histological subgroups of NPC.
Results
The median age of both cases and controls was 45 (range: 15–74). Cases (69.3%) and 68.6% of controls were male. Cases (98.6%) compared with 29.6% of controls were seropositive for at least one of the anti-EBV antibodies measured in our study (RR⫽ 170; 95% CI ⫽ 70–440). Cases (82.1%) were Fuk-kienese; 12.8% were of Guangdong, Hakka, or Aboriginal
origin; and the remaining 5.1% of cases were of other Han descent. Among controls, the ethnic distribution was 72.8% Fukkienese, 10.8% Guangdong/Hakka/Aboriginal, and 16.4% other Han. Compared with individuals of Fukkiene descent, those of Guangdong/Hakka/Aboriginal descent had a RR of NPC of 1.0 (95% CI ⫽ 0.65–1.7), and those of other Han descent had a RR of 0.27 (95% CI⫽ 0.16–0.48). Education was inversely associated with disease. Participants reporting more than a high school education had a RR⫽ 0.46 (95% CI ⫽ 0.30 – 0.70) compared with those with less than a middle school education. Other factors associated with NPC in our study and considered as potential confounders in our analyses include ⱖ25 years of cigarette smoking (RR ⫽ 1.7; 95% CI ⫽ 1.1–2.9), dietary nitrosamine consumption at age 10 as reported by the participant’s mother (RR⫽ 2.2 for highest quartile compared with lowest quartile; 95% CI⫽ 0.8–5.6), being homozygous for the CYP2E1 RSAI variant allele (RR ⫽ 2.6; 95% CI ⫽ 1.2–5.7), and having at least one at-risk HLA allele (RR⫽ 2.0; 95% CI⫽ 1.5–2.8; Refs. 31–33).
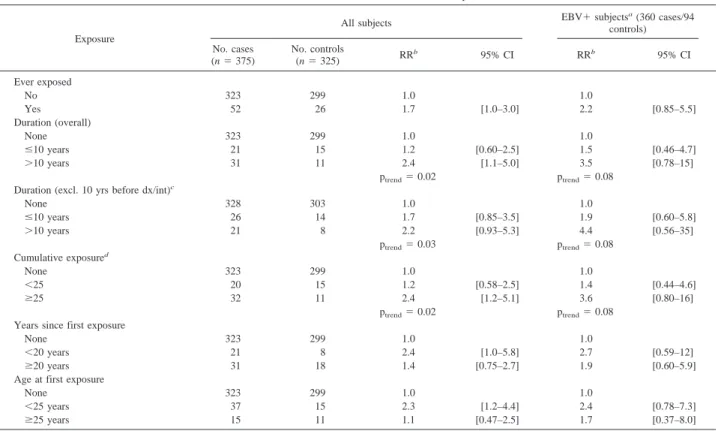
The associations between occupational exposures to wood dust and NPC risk are presented in Table 2. After control for confounding factors, individuals exposed to wood had a RR of 1.7 (95% CI⫽ 1.0–3.0). Those exposed for ⬎10 years had a RR of 2.4 (95% CI⫽ 1.1–5.0; ptrend⫽ 0.02). After excluding
exposures in the 10 years preceding diagnosis/interview, the comparable RR was 2.2 (95% CI⫽ 0.93–5.3; ptrend⫽ 0.03).
Those withⱖ25 intensity years of exposure (i.e., cumulative exposure) had a RR of 2.4 (95% CI⫽ 1.2–5.1; ptrend⫽ 0.02).
Table 2 Distribution and risk associated with wood exposure
Exposure
All subjects EBV⫹ subjects
a(360 cases/94 controls) No. cases (n⫽ 375) No. controls (n⫽ 325) RR b 95% CI RRb 95% CI Ever exposed No 323 299 1.0 1.0 Yes 52 26 1.7 [1.0–3.0] 2.2 [0.85–5.5] Duration (overall) None 323 299 1.0 1.0 ⱕ10 years 21 15 1.2 [0.60–2.5] 1.5 [0.46–4.7] ⬎10 years 31 11 2.4 [1.1–5.0] 3.5 [0.78–15] ptrend⫽ 0.02 ptrend⫽ 0.08 Duration (excl. 10 yrs before dx/int)c
None 328 303 1.0 1.0 ⱕ10 years 26 14 1.7 [0.85–3.5] 1.9 [0.60–5.8] ⬎10 years 21 8 2.2 [0.93–5.3] 4.4 [0.56–35] ptrend⫽ 0.03 ptrend⫽ 0.08 Cumulative exposured None 323 299 1.0 1.0 ⬍25 20 15 1.2 [0.58–2.5] 1.4 [0.44–4.6] ⱖ25 32 11 2.4 [1.2–5.1] 3.6 [0.80–16] ptrend⫽ 0.02 ptrend⫽ 0.08 Years since first exposure
None 323 299 1.0 1.0
⬍20 years 21 8 2.4 [1.0–5.8] 2.7 [0.59–12]
ⱖ20 years 31 18 1.4 [0.75–2.7] 1.9 [0.60–5.9]
Age at first exposure
None 323 299 1.0 1.0
⬍25 years 37 15 2.3 [1.2–4.4] 2.4 [0.78–7.3]
ⱖ25 years 15 11 1.1 [0.47–2.5] 1.7 [0.37–8.0]
aEBV seropositives defined as positive for one of the following anti-EBV antibodies known to be associated with NPC; viral capsid antigen IgA, EBV nuclear antigen
1 IgA, early antigen IgA, DNA binding protein IgG and anti-DNase IgG (see also description in “Materials and Methods”).
bAdjusted for age, sex, education, ethnicity, and HLA.
cDx/int⫽ date of diagnosis (for case) and date of interview (for controls). dDefined as intensity⫻ duration as specified in “Materials and Methods.”
Individuals with⬍20 years since their first exposure had a RR of 2.4 (95% CI⫽ 1.0–5.8), and those with ⱖ20 years since first exposure had a RR of 1.4 (95% CI⫽ 0.75–2.7). The effect of occupational exposure to wood on NPC risk was confined to individuals first exposed before the age of 25 years (RR⫽ 2.3; 95% CI ⫽ 1.2–4.4). Compared with unexposed individuals, those exposed for⬎10 years who were first exposed before the age of 25 years had a RR of 2.8 (95% CI ⫽ 1.2–6.9). The observed associations were not materially affected by addi-tional adjustment for formaldehyde or solvent exposure.
A stronger duration effect was seen in analyses where only those individuals with a high average intensity or probability of exposure were compared against unexposed individuals (i.e., excluding those individuals with low average intensity or prob-ability of exposure); the RR for⬎10 years of exposure was 3.4 (95% CI⫽ 1.2–9.4; ptrend⫽ 0.01) among individuals with high
average intensity of exposure and 2.9 (95% CI⫽ 1.1–7.4; ptrend
⫽ 0.01) among individuals with high average probability of exposure. The patterns observed were similar in analyses re-stricted to the 360 cases and 94 controls seropositive for anti-bodies against EBV, but the magnitude of the observed effects was stronger. We were able to determine whether exposure was to hardwood, softwood, or both for 79.5% of individuals em-ployed in jobs involving wood exposure. Among this subgroup, we observed that individuals exposed to hardwood only (11 cases and 8 controls) were not at excess risk of NPC (RR⫽ 1.3; 95% CI⫽ 0.50–3.4), whereas those exposed to softwood (with or without exposure to hardwood; 33 cases and 10 controls) were at a significant excess risk of NPC (RR⫽ 2.7; 95% CI ⫽ 1.3–5.8).
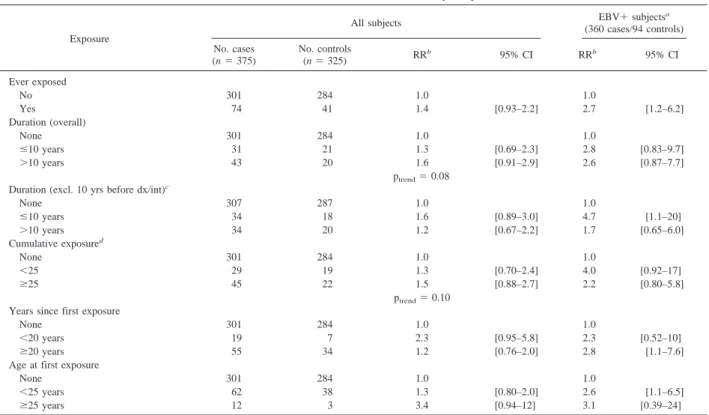
The associations between occupational formaldehyde ex-posures and NPC risk are presented in Table 3. After control for confounding factors, individuals ever exposed to formaldehyde had a RR of 1.4 (95% CI ⫽ 0.93–2.2). There was some evidence of increasing risk of NPC with increasing years of exposure to formaldehyde (RR⫽ 1.3 and 1.6, for ⱕ10 years and ⬎10 years of exposure, respectively), but the observed trend did not achieve statistical significance (ptrend ⫽ 0.08).
Compared with unexposed individuals, those exposed for⬎20 years had a RR of 1.7 (95% CI ⫽ 0.77–3.5), but the trend observed when these more refined duration categories (no ex-posure,ⱕ10, ⬎10–20, and ⬎20 years of exposure) were ex-amined still did not reach statistical significance (ptrend⫽ 0.09).
There was little evidence of increasing risk with increasing duration of exposure after exclusion of exposures in the 10 years preceding diagnosis/interview or with cumulative expo-sure (RR⫽ 1.2 and 1.5 for ⬎10 years of exposure and ⱖ25 intensity years of exposure, respectively). Stronger effects were seen in analyses of individuals with a high average intensity or probability of exposure (i.e., excluding individuals with low average intensity or probability of exposure), but no clear dose response relationships were observed. In individuals with a high average intensity of exposure, the RR estimates associated with ⱕ10 and ⬎10 years of exposure (compared with those unexposed) were 2.1 (95% CI⫽ 0.94–4.8) and 2.1 (95% CI ⫽ 1.0 – 4.2), respectively. Similarly, individuals with a high aver-age probability of exposure, the RR estimates associated with ⱕ10 and ⬎10 years of exposure were 2.6 (95% CI ⫽ 1.1–6.3) and 1.4 (95% CI ⫽ 0.75–3.0), respectively. Stronger effects were also observed in analyses restricted to the 360 cases and Table 3 Distribution and risk associated with formaldehyde exposure
Exposure
All subjects EBV⫹ subjects
a (360 cases/94 controls) No. cases (n⫽ 375) No. controls (n⫽ 325) RR b 95% CI RRb 95% CI Ever exposed No 301 284 1.0 1.0 Yes 74 41 1.4 [0.93–2.2] 2.7 [1.2–6.2] Duration (overall) None 301 284 1.0 1.0 ⱕ10 years 31 21 1.3 [0.69–2.3] 2.8 [0.83–9.7] ⬎10 years 43 20 1.6 [0.91–2.9] 2.6 [0.87–7.7] ptrend⫽ 0.08 Duration (excl. 10 yrs before dx/int)c
None 307 287 1.0 1.0 ⱕ10 years 34 18 1.6 [0.89–3.0] 4.7 [1.1–20] ⬎10 years 34 20 1.2 [0.67–2.2] 1.7 [0.65–6.0] Cumulative exposured None 301 284 1.0 1.0 ⬍25 29 19 1.3 [0.70–2.4] 4.0 [0.92–17] ⱖ25 45 22 1.5 [0.88–2.7] 2.2 [0.80–5.8] ptrend⫽ 0.10 Years since first exposure
None 301 284 1.0 1.0
⬍20 years 19 7 2.3 [0.95–5.8] 2.3 [0.52–10]
ⱖ20 years 55 34 1.2 [0.76–2.0] 2.8 [1.1–7.6]
Age at first exposure
None 301 284 1.0 1.0
⬍25 years 62 38 1.3 [0.80–2.0] 2.6 [1.1–6.5]
ⱖ25 years 12 3 3.4 [0.94–12] 3.1 [0.39–24]
aEBV seropositives defined as positive for one of the following anti-EBV antibodies known to be associated with NPC: viral capsid antigen IgA, EBV nuclear antigen1
IgA, early antigen IgA, DNA binding protein IgG, and anti-DNase IgG (see also description in “Materials and Methods”).
bAdjusted for age, sex, education, and ethnicity.
cDx/int⫽ date of diagnosis (for case) and date of interview (for controls). dDefined as intensity⫻ duration as specified in “Materials and Methods.”
94 controls seropositive for antibodies against EBV. Whereas a significant increase in risk was observed among those ever exposed to formaldehyde (RR⫽ 2.7; 95% CI ⫽ 1.2–6.2), no clear dose response patterns were observed with increased duration or cumulative exposure. No striking patterns were observed when years since first exposure and age at first ex-posure were examined. The observed associations were not materially affected by additional adjustment for wood dust or solvent exposure.
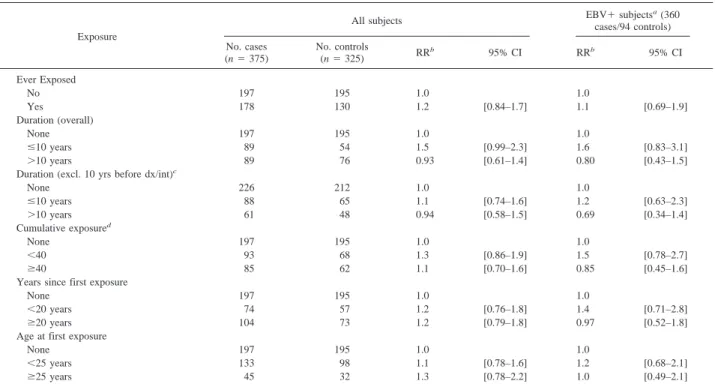
Findings from the analyses that examined the association between occupational exposure to solvents and NPC are sum-marized in Table 4. Individuals exposed to solvents for ⬎10 years had a RR of 0.93 (95% CI⫽ 0.61–1.4), and those with a cumulative exposure ofⱖ40 intensity years had a RR of 1.1 (95% CI ⫽ 0.70–1.6). Analyses of individuals with a high average intensity or probability of exposure also failed to sup-port an association between solvents and NPC (data not shown). No excess risk of disease was observed for individuals with⬎20 years since first exposure to occupational solvents or for those first exposed before the age of 25. No positive asso-ciations between solvent exposure and NPC were seen in anal-yses restricted to EBV seropositive individuals.
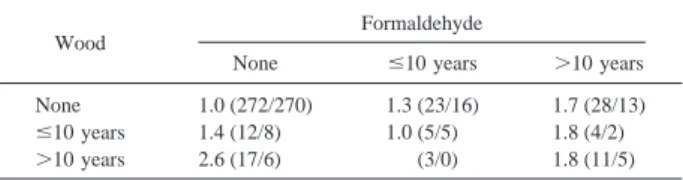
The correlation between wood and formaldehyde exposure in our control population ranged from 0.26 to 0.35, depending on the measure of exposure examined. The combined effect of wood and formaldehyde exposure is presented in Table 5. Among individuals with no occupational exposure to formal-dehyde, risk of NPC increased with increasing years of expo-sure to wood (ptrend⫽ 0.04). A nonsignificant increase in risk
with increasing years of formaldehyde exposure was seen in the absence of exposure to wood (ptrend⫽ 0.09). Similar results
were obtained when the combined effect of cumulative expo-sure to wood dust and formaldehyde was examined (data not shown).
Analyses were also performed separately for individuals ⬍45 years and ⱖ45 years and for males and females (data not shown). For wood dust and solvents, results from these strati-fied analyses were consistent with the overall findings pre-sented above. The one exception was that the small number of females exposed to wood (n⫽ 5) precluded detailed analyses within this subgroup. For formaldehyde, no consistent differ-ential patterns were observed when age-stratified analyses were performed. However, in analyses stratified by gender, effects tended to be restricted to men. Compared with men who were not exposed to formaldehyde, men ever exposed to formalde-hyde had a RR of 1.6 (95% CI⫽ 0.91–2.7), and those exposed for⬎10 years had a RR of 1.7 (95% CI ⫽ 0.86–3.3; ptrend⫽
0.10). The respective RRs for women were 1.1 (95% CI ⫽ 0.50 –2.3) and 1.0 (95% CI⫽ 0.30–3.7; ptrend⫽ 0.88).
Anal-yses restricted to cases diagnosed with nonkeratinizing or un-differentiated carcinomas (91% of our cases) yielded similar results to that observed in the overall analyses. The small number of cases diagnosed with squamous cell carcinomas (9% of our cases) precluded separate analyses among this histolog-ical subgroup.
Discussion
Limitation of the present study should be discussed up front. First, exposure was assessed based on job history information obtained from participants. No direct exposure measurements were made. Whereas this is an improvement over many previ-Table 4 Distribution and risk associated with solvent exposure
Exposure
All subjects EBV⫹ subjects
a(360 cases/94 controls) No. cases (n⫽ 375) No. controls (n⫽ 325) RR b 95% CI RRb 95% CI Ever Exposed No 197 195 1.0 1.0 Yes 178 130 1.2 [0.84–1.7] 1.1 [0.69–1.9] Duration (overall) None 197 195 1.0 1.0 ⱕ10 years 89 54 1.5 [0.99–2.3] 1.6 [0.83–3.1] ⬎10 years 89 76 0.93 [0.61–1.4] 0.80 [0.43–1.5]
Duration (excl. 10 yrs before dx/int)c
None 226 212 1.0 1.0 ⱕ10 years 88 65 1.1 [0.74–1.6] 1.2 [0.63–2.3] ⬎10 years 61 48 0.94 [0.58–1.5] 0.69 [0.34–1.4] Cumulative exposured None 197 195 1.0 1.0 ⬍40 93 68 1.3 [0.86–1.9] 1.5 [0.78–2.7] ⱖ40 85 62 1.1 [0.70–1.6] 0.85 [0.45–1.6]
Years since first exposure
None 197 195 1.0 1.0
⬍20 years 74 57 1.2 [0.76–1.8] 1.4 [0.71–2.8]
ⱖ20 years 104 73 1.2 [0.79–1.8] 0.97 [0.52–1.8]
Age at first exposure
None 197 195 1.0 1.0
⬍25 years 133 98 1.1 [0.78–1.6] 1.2 [0.68–2.1]
ⱖ25 years 45 32 1.3 [0.78–2.2] 1.0 [0.49–2.1]
aEBV seropositives defined as positive for one of the following anti-EBV antibodies known to be associated with NPC: viral capsid antigen IgA, EBV nuclear antigen1
IgA, early antigen IgA, DNA binding protein IgG, and anti-DNase IgG (see also description in “Materials and Methods”).
bAdjusted for age, sex, education, and ethnicity.
cDx/int⫽ date of diagnosis (for case) and date of interview (for controls). dDefined as intensity⫻ duration as specified in “Materials and Methods.”
ous efforts to evaluate occupational factors in NPC develop-ment, the potential for misclassification remains. In particular, if the degree of misclassification is higher for formaldehyde and solvent exposure compared with wood dust exposure, this could explain our inability to demonstrate a clear association between formaldehyde and solvent use and NPC. Also, given that clas-sification of exposure to hardwood versus softwood was made based on job histories alone, it is likely that this assessment is prone to misclassification, and our findings regarding hard-wood versus softhard-wood should therefore be viewed with caution. Finally, the cases in our study were hospital based, whereas controls were recruited from the population. To partially con-trol for referral patterns, we required both cases and concon-trols to be residents of the Taipei metropolitan area (i.e., cases from other regions sent to one of our participating hospitals for diagnosis/treatment were not included) and additionally matched our controls to cases on the area of residence. Also, data from the Taiwan tumor registry between 1991 and 1994 suggest that the 378 cases ascertained for our study correspond to⬃35% of all NPC cases diagnosed in the Taipei metropolitan area during the study period. Thus, while hospital based, our cases represent a large fraction of all cases diagnosed in the area during the study period. This should alleviate concerns over referral bias.
Despite the limitations discussed above, the present inves-tigation is the largest case-control study to date to systemati-cally evaluate the role of occupational exposures in the devel-opment of NPC. Complete and detailed occupational history information was collected from 700 study participants (re-sponse rates ⬎85% for cases and controls combined). This information was reviewed in a blinded fashion by an experi-enced industrial hygienist. Results from the study suggest a consistent association between exposure to wood dust and NPC. Risk increased with increasing duration of exposure, was strongest among individuals with a high average intensity of exposure, and was restricted to those whose first occupational exposure to wood occurred at a relatively young age (⬍25 years). Our data were also suggestive of a stronger effect for softwood exposure.
The observation that risk is highest for individuals ex-posed to wood early in life is consistent with our understanding of the natural history of NPC. Compared with most other cancers, NPC occurs at a relatively young age (median age at diagnosis is in the mid-40s in most countries), and other expo-sures at young ages (particularly dietary expoexpo-sures) have been found previously to be important risk factors for NPC (3).
A strength of our study was the ability to test for various anti-EBV antibodies known to be associated with NPC. EBV is widely believed to be a necessary (but not sufficient) cause of NPC. Whereas EBV is ubiquitous and most individuals are infected with the virus in the first 2 decades of life, only a
subset of individuals develop the anti-EBV antibody pattern characteristically seen among NPC cases. In our study, sero-positivity to one or more of five anti-EBV antibodies known to be associated with NPC was associated with a 170-fold in-creased risk of disease. Wood dust analyses stratified by EBV seropositivity indicated stronger effects among individuals pos-itive for at least one of these markers. This suggests that our observations are not attributable to confounding by EBV, add-ing credence to our findadd-ing that occupational exposure to wood is associated with NPC.
Our results with respect to occupational exposure to wood are consistent with those from a case-control study conducted in the Philippines and with the well-established link between wood exposure and nasal adenocarcinomas (6, 28). In contrast, a study by Vaughan et al. (5) failed to observe an association between wood dust exposure and NPC. The study by Vaughan
et al. was comprised largely of NPC cases diagnosed with
squamous cell carcinomas (WHO Type 1), whereas ours con-sisted almost exclusively of cases diagnosed with nonkeratiniz-ing and undifferentiated carcinomas (WHO Types 2 and 3), additionally supporting previous suggestions that risk factors for NPC other than EBV vary by histology (4, 5).
Whereas nasal adenocarcinomas have been shown to be most strongly associated with hardwood exposure (28), possi-bly because of the smaller particle size generated from hard-woods compared with softhard-woods, our data suggest that NPC (a squamous cell tumor) is more tightly linked to occupational exposure to softwoods. This observation is consistent with some studies that have observed an association between soft-wood exposure and nasal squamous cell tumors (21, 28). The biological rationale for such a finding is unclear. One possible explanation is that chemically treated softwoods absorb higher amounts of chemicals than similarly treated hardwoods. If the association between wood and NPC is attributable to specific chemicals used in the wood industry to preserve wood (e.g., chlorophenols), as suggested by some (17, 45), this may explain the stronger effects we observe for softwood exposure. Con-sistent with this explanation, our population was almost exclu-sively exposed to treated and/or mixed treated and untreated woods. Caution should be exercised, however, in interpreting the differences seen between hardwood and softwood expo-sures in our study, given the modest number of individuals in this subgroup analysis and the potential for misclassification of exposure discussed above.
Formaldehyde is known to cause tumors in animals, in-cluding carcinomas of the nasal cavities, after formaldehyde inhalation (28). There has therefore been great interest in de-termining whether this known animal carcinogen causes tumors in humans. Results from human studies, however, have been mixed (28). A meta-analysis of available studies suggested that formaldehyde exposure was associated with a 2-fold increase in risk of NPC (11). Subsequently, two case-control studies con-ducted in the Philippines and the United States confirmed the association between formaldehyde exposure and NPC risk (5, 6). In our study, a modest and nonsignificant association was observed between duration of formaldehyde exposure and risk of NPC, an effect that appeared to be restricted to men. When elevated risks were observed (e.g., in analyses restricted to EBV seropositives), the strongest effects were seen in those individuals exposed for shorter periods (ⱕ10 years). In a pre-vious case-control study conducted in the Philippines, we also observed a stronger association with NPC in individuals ex-posed for⬍15 years (RR ⫽ 2.7; 95% CI ⫽ 1.1–6.6) compared with those exposed for ⱖ15 years (RR ⫽ 1.2; 95% CI ⫽ 0.48 –3.2; Ref. 6). However, in this previous study, exclusion of Table 5 Joint effect of occupational formaldehyde and wood exposure on risk
of NPCa
Wood
Formaldehyde
None ⱕ10 years ⬎10 years
None 1.0 (272/270) 1.3 (23/16) 1.7 (28/13)
ⱕ10 years 1.4 (12/8) 1.0 (5/5) 1.8 (4/2)
⬎10 years 2.6 (17/6) (3/0) 1.8 (11/5)
aNumbers presented are RR estimates adjusted for age, sex, education, ethnicity,
and HLA. Numbers in parentheses correspond to the number of cases/controls. 95% CI for all individual RR estimates overlap 1. ptrendfor wood in the absence of formaldehyde⫽ 0.04 and for formaldehyde in the absence of wood ⫽ 0.09.
exposures which occurred in the 10 years preceding cancer diagnosis (or interview in the case of the controls) revealed a dose response of increasing risk with increasing duration of use. In the present study, lagging exposures by 10 years did not clarify our findings.
Finally, to follow up on a preliminary suggestion from a large cohort in China that exposure to solvents may be linked to NPC development (30), we evaluated the possible associa-tion between solvents and NPC in our populaassocia-tion. No evidence of an association was observed. Results from our previous study in the Philippines are consistent with these findings (6). It should be noted, however, that the study in China (30) focused on benzene exposure, whereas our Taiwan and Philip-pine (6) studies examined solvents more broadly. This may partially explain the differences observed between studies.
In summary, we observed a consistent association between wood dust exposure and risk of NPC in our case-control study of 375 NPC cases and 325 controls. The association was strong-est for individuals exposed before the age of 25 and those positive for anti-EBV antibodies known to be associated with NPC. A less consistent association was observed between form-aldehyde exposure and NPC risk. No association was observed between solvent exposure and NPC risk.
References
1. Yu, M. C., and Henderson, B. E. Nasopharyngeal cancer. In: D. Schottenfeld and J. F. Fraumeni (eds.), Cancer Epidemiology and Prevention, Ed. 2, pp. 603– 618. New York: Oxford University Press, 1996.
2. Mueller, N., Evans, A., and London, W. T. Viruses. In: D. Schottenfeld and J. F. Fraumeni, Jr. (eds.), Cancer Epidemiology and Prevention, Ed. 2, pp. 503– 602. 1996.
3. Hildesheim, A., and Levine, P. H. Etiology of nasopharyngeal carcinoma: a review. Epidemiol. Rev., 15: 466 – 485, 1993.
4. Vaughan, T. L., Shapiro, J. A., Burt, R. D., Swanson, G. M., Berwick, M., Lynch, C. F., and Lyon, J. L. Nasopharyngeal cancer in a low-risk population: defining risk factors by histological type. Cancer Epidemiol. Biomarkers Prev., 5: 587–593, 1996.
5. Vaughan, T. L., Stewart, P. A., Teschke, K., Lynch, C. F., Swanson, G. M., Lyon, J. L., and Berwick, M. Occupational exposure to formaldehyde and wood dust and nasopharyngeal carcinoma. Occup. Environ. Med., 57: 376 –384, 2000. 6. West, S., Hildesheim, A., and Dosemeci, M. Non-viral risk factor for naso-pharyngeal carcinoma in The Philippines: results from a case-control study. Int. J. Cancer, 55: 1– 6, 1993.
7. Roush, G. C., Walrath, J., Stayner, L. T., Kaplan, S. A., Flannery, J. T., and Blair, A. Nasopharyngeal cancer, Sinonasal cancer, and occupations related to formaldehyde: a case-control study. J. Natl. Cancer Inst. (Bethesda), 79: 1221– 1224, 1987.
8. Olsen, J. H., Jensen, S. P., Hink, M., faurbo, K., Oluf Breum, N., and Jensen, O. M. Occupational formaldehyde exposure and increased nasal cancer risk in man. Int. J. Cancer, 34: 639 – 644, 1984.
9. Armstrong, R. W., Armstrong, M. J., Yu, M. C., and Henderson, B. E. Salted fish and inhalants as risk factors for nasopharyngeal carcinoma in Malaysian Chinese. Cancer Res., 43: 2967–2970, 1983.
10. Yu, M. C., Garabrant, D. H., Huang, T. B., and Henderson, B. E. Occupa-tional and other non-dietary risk factors for nasopharyngeal carcinoma in Guang-zhou, China. Int. J. Cancer, 45: 1033–1039, 1990.
11. Partanen, T. Formaldehyde exposure and respiratory cancer: a meta-analysis of the epidemiologic evidence. Scand. J. Work Environ. Health, 19: 8 –15, 1993. 12. Lynge, E., Anttila, A., and Hemminki, K. Organic solvents and cancer. Cancer Causes Control, 8: 406 – 419, 1997.
13. Hayes, R. B., Blair, A., Stewart, P. A., Herrick, R. F., and Mahar, H. Mortality of U. S. embalmers and funeral directors. Am. J. Prev. Med., 18: 641– 652, 1990.
14. Vaughan, T. L., Strader, C., Davis, S., and Daling, J. R. Formaldehyde and cancers of the pharnyx, sinus and nasal cavity: I. Occupational exposures. Int. J. Cancer, 38: 677– 683, 1986.
15. Blair, A., Stewart, P. A., Hoover, R. N., Fraumeni, J. F., Walwrath, J., O’Berg, M., and Gaffey, W. Cancers of the nasopharynx and oropharynx and formaldehyde exposure. J. Natl. Cancer Inst. (Bethesda), 78: 191–193, 1987.
16. Bond, G. G., McLaren, E. A., Lipps, T. E., and Cook, R. R. Update of mortality among chemical workers with potential exposure to the higher chlori-nated dioxins. J. Occup. Med., 31: 121–123, 1989.
17. Hardell, L., Johansson, B., and Axelson, O. Epidemiological study of nasal and nasopharyngeal cancer and their relation to phenoxy acid chlorophenol exposure. Am. J. Prev. Med., 3: 247–257, 1982.
18. Ng, T. P. A case-referent study of cancer of the nasal cavity and sinuses in Hong Kong. Int. J. Epidemiol., 15: 171–175, 1986.
19. Voss, R., Stenersen, T., Oppedal, B. R., and Boysen, M. Sinonasal cancer and exposure to softwood. Acta Oto-Laryngol., 99: 172–178, 1985.
20. Reif, J., Pearce, N., Kawachi, I., and Fraser, J. Soft-tissue sarcoma, non-Hodgkin’s lymphoma and other cancers in New Zealand forestry workers. Int. J. Cancer, 43: 49 –54, 1989.
21. Vaughan, T. L., and Davis, S. Wood dust exposure and squamous cell cancers of the upper respiratory tract. Am. J. Epidemiol., 133: 560 –564, 1991. 22. Kawachi, I., Pearce, N., and Fraser, J. A New Zealand cancer registry-based study of cancer in wood workers. Cancer (Phila.), 64: 2609 –2613, 1989. 23. Barthel, E., and Dietrich, M. Retrospective cohort study of cancer morbidity in furniture makers exposed to wood dust. Z gesamte Hyg, 35: 270 –272, 1989. 24. Vaughan, T. L. Occupation and squamous cell cancers of the pharynx and sinonasal cavity. Am. J. Prev. Med., 16: 493–510, 1989.
25. Malker, H. S. R., McLaughlin, J. K., Weiner, J. A., Blot, W. J., Ericsson, J. L., and Fraumeni, J. F. Occupational risk factors for nasopharyngeal cancer in Sweden. Br. J. Ind. Med., 47: 213–214, 1990.
26. Hertzman, C., Teschke, K., Ostry, A., Hershler, R., Dimich-Ward, H., Kelly, S., Spinelli, J. J., Gallagher, R. P., McBride, M., and Marion, S. A. Mortality and cancer incidence among sawmill workers exposed to chlorophenate wood pre-servatives. Am. J. Public Health, 87: 71–79, 1997.
27. Zheng, W., McLaughlin, J. K., Gao, Y. T., Gao, R. N., and Blot, W. J. Occupational risks for nasopharyngeal cancer in Shanghai. J. Occup. Med., 34: 1004 –1007, 1992.
28. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Wood Dust and Formaldehyde. IARC Scientific Publ. No. 62. Lyon, France: IARC, 1995.
29. Demers, P. A., Kogevinas, M., Boffetta, P., Leclerc, A., Luce, D., Gerin, M., Battista, G., Belli, S., Bolm-Audorf, U., and Brinton, L. A. Wood dust and sino-nasal cancer: pooled reanalysis of twelve case-control studies. Am. J. Ind. Med., 28: 151–166, 1995.
30. Hayes, R. B., Yin, S. N., Dosemeci, M., Li, G. L., Wacholder, S., Chow, W. H., Rothman, N., Wang, Y. Z., Dai, T. R., Chao, X. J., Jiang, Z. L., Ye, P. Z., Zhao, H. B., Kou, Q. R., Zhang, W. Y., Meng, J. F., Zho, J. S., Lin, X. F., Ding, C. Y., Li, C. Y., Zhang, Z. N., Li, D. G., Travis, L. B., Blot, W. J., and Linet, M. S. Mortality among benzene-exposed workers in China. Environ. Health Perspect.,
104: 1349 –1352, 1996.
31. Cheng, Y. J., Hildesheim, A., Hsu, M. M., Chen, I. H., Brinton, L. A., Levine, P. H., Chen, C. J., and Yang, C. S. Cigarette smoking, alcohol consumption and risk of nasopharyngeal carcinoma in Taiwan. Cancer Causes Control, 10: 201– 207, 1999.
32. Hildesheim, A., Anderson, L. M., Chen, C. J., Cheng, Y. J., Brinton, L. A., Daly, A. K., Reed, C. D., Chen, I. H., Caporaso, N. E., Hsu, M. M., Chen, J. Y., Idle, J. R., Hoover, R. N., Yang, C. S., and Chhabra, S. K. CYP2E1 genetic polymorphisms and risk of nasopharyngeal carcinoma in Taiwan. J. Natl. Cancer Inst. (Bethesda), 89: 1207–1212, 1997.
33. Ward, M. H., Pan, W. H., Cheng, Y. J., Lin, F. H., Brinton, L. A., Chen, C. J., Hsu, M. M., Chen, I. H., Levine, P. H., Yang, C. S., and Hildesheim, A. Dietary exposure to nitrite and nitrosamines and risk of nasopharygeal carcinoma in Taiwan. Int. J. Cancer, 86: 603– 609, 2000.
34. Executive office of the President. Standard industrial classification manual, 1987.
35. US Printing Office. Standard occupational classification manual, 1980. 36. Dosemeci, M., Cocco, P., Gomez, M., Stewart, P. A., and Heineman, E. F. Effects of three features of a job-exposure matrix on risk estimates. Epidemiol-ogy, 5: 124 –127, 1994.
37. Gomez, M. R., Cocco, P., Dosemeci, M., and Stewart, P. A. Occupational exposure to chlorinated aliphatic hydrocarbons: job-exposure matrix. Am. J. Ind. Med., 26: 171–183, 1994.
38. Henle, G., and Henle, W. Epstein-Barr virus-specific IgA serum antibodies as an outstanding feature of nasopharyngeal carcinoma. Int. J. Cancer, 17: 1–7, 1976.
39. Chow, K. C., Ma, J., Lin, L. S., Chi, K. H., Yen, S. H., Liu, S. M., Liu, W. T., Chen, W. K., Chang, T. H., and Chen, K. Y. Serum responses to the combination of epstein-barr virus antigens from both latent and acute phases in nasopharyngeal
carcinoma: complementary test of EBNA-1 with EA-D. Cancer Epidemiol. Bi-omarkers Prev., 6: 363–368, 1997.
40. Liu, M. Y., Chang, Y. L., Ma, J., Yang, H. L., Hsu, M. M., Chen, C. J., Chen, J. Y., and Yang, C-S. Evaluation of multiple antibodies to epstein-barr virus as markers for detecting patients with nasopharyngeal carcinoma. J. Med. Virol., 52: 262–269, 1997.
41. Chen, J. Y., Chen, C. J., Liu, M. Y., Cho, S. M., Hsu, M. M., Kuo, S. L., Lynn, T. C., Shieh, T., Tu, S. M., Lee, H. H., Lai, M. Y., Hseih, C. Y., Hu, C. P., and Yang, C. S. Antibodies to Epstein-Barr virus-specific DNase in patients with nasopharyngeal carcinoma and control groups. J. Med. Virol.,
23: 11–21, 1987.
42. Erlich, H., Bugawan, T., Begovich, A., and Scharf, S. Analysis of HLA class II polymorphism using polymerase chain reaction. Arch. Pathol. Lab. Med., 117: 482– 485, 1993.
43. Bugawan, T. L., and Erlich, H. A. Rapid typing of HLA-DQB1 DNA polymorphism using nonradioactive oligonucleotide probes and amplified DNA. Immunogenetics, 33: 163–170, 1991.
44. Scharf, S. J., Griffith, R. L., and Erlich, H. A. Rapid typing of DNA sequence polymorphism at the HLA-DRB1 locus using the polymerase chain reaction and nonradioactive oligonucleotide probes. Hum. Immunol., 30: 190 –201, 1991. 45. Hardell, L., Axelson, O., and Rappe, C. Nasal cancer and chlorophenols. Lancet, 1: 1167, 1983.